
Diagnostic Performance and Clinical Utility of Conventional PCR Assay in Early Diagnosis of COVID-19 Associated Rhino-Orbito-Cerebral Mucormycosis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
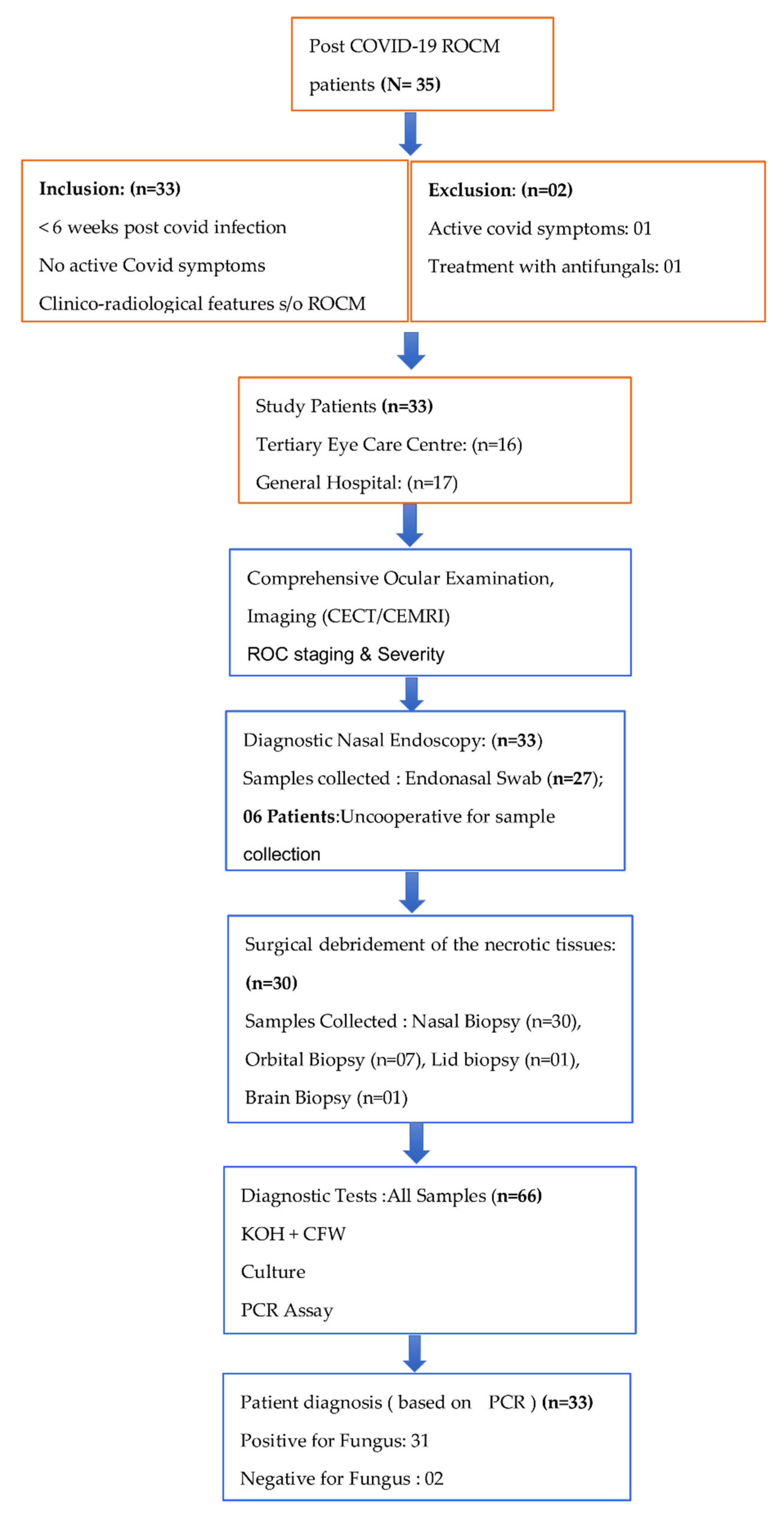
2.1. Study Design
2.2. Clinical Data of Patients and Staging
2.3. Surgical Intervention and Sample Collection
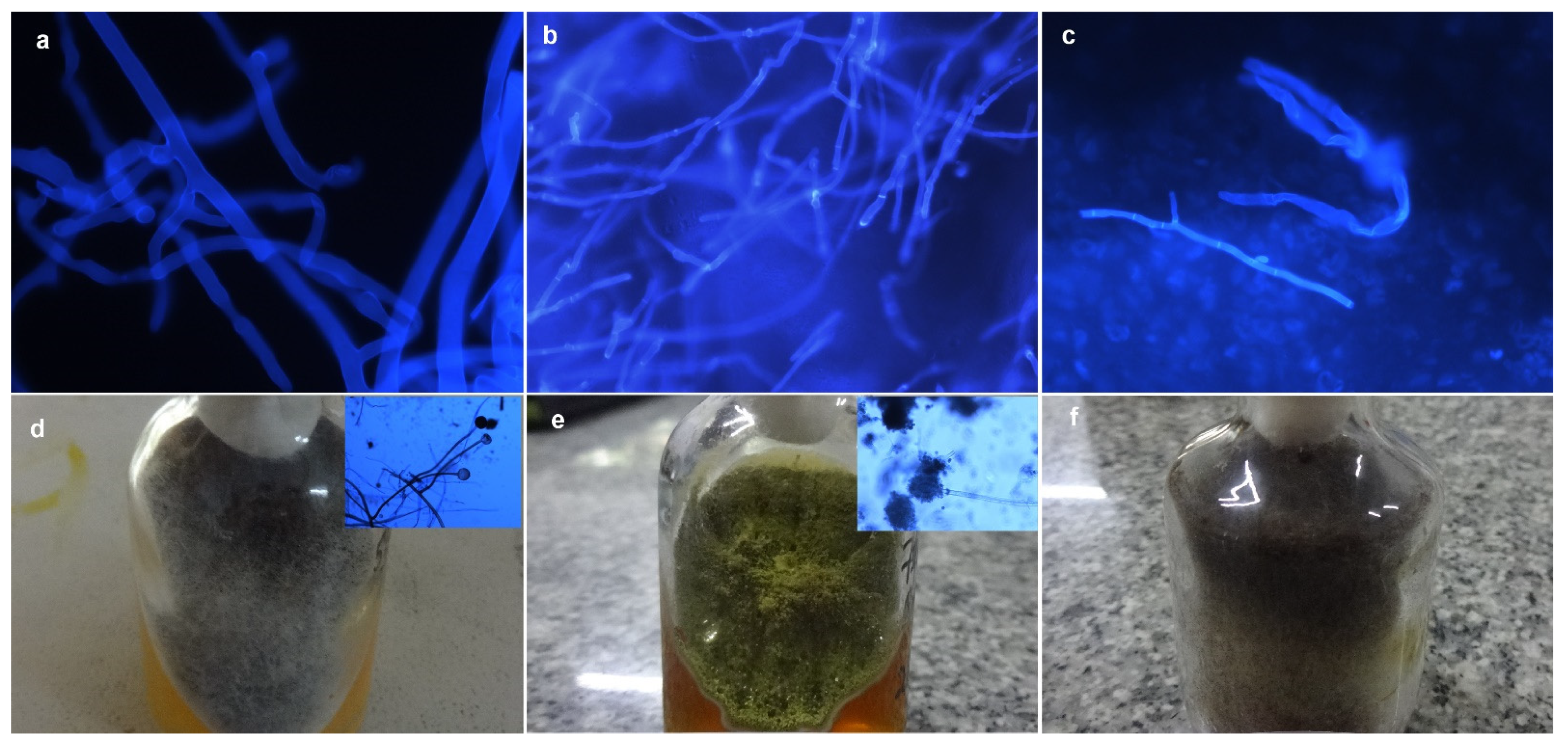
2.4. Conventional Microbiology Examination
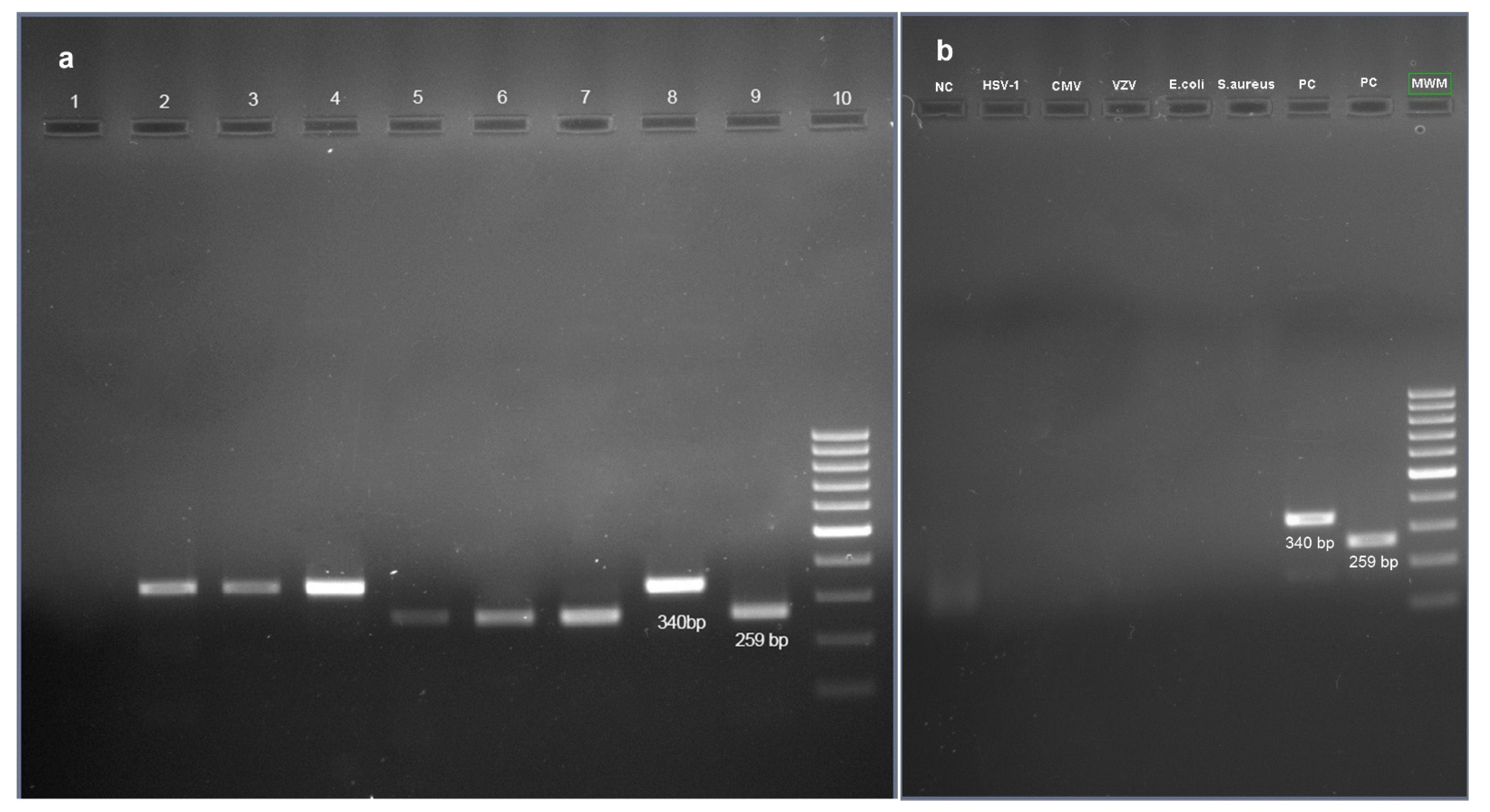
2.5. Standardisation of PCR Assay
2.6. Analytical Sensitivity and Specificity of Primers
2.7. Nucleotide Sequencing and Homology Analysis
2.8. Data Compilation and Statistical Analysis
3. Results
3.1. Demographic and Clinical Details
3.2. Diagnostic Performance of KOH + CFW Smear
3.3. Diagnostic Performance of Culture
3.4. Diagnostic Performance of PCR Assay
3.5. Nucleotide Sequencing
3.6. Efficacy of Nasal Biopsy and Endonasal Swab in Detection of Fungal Pathogens
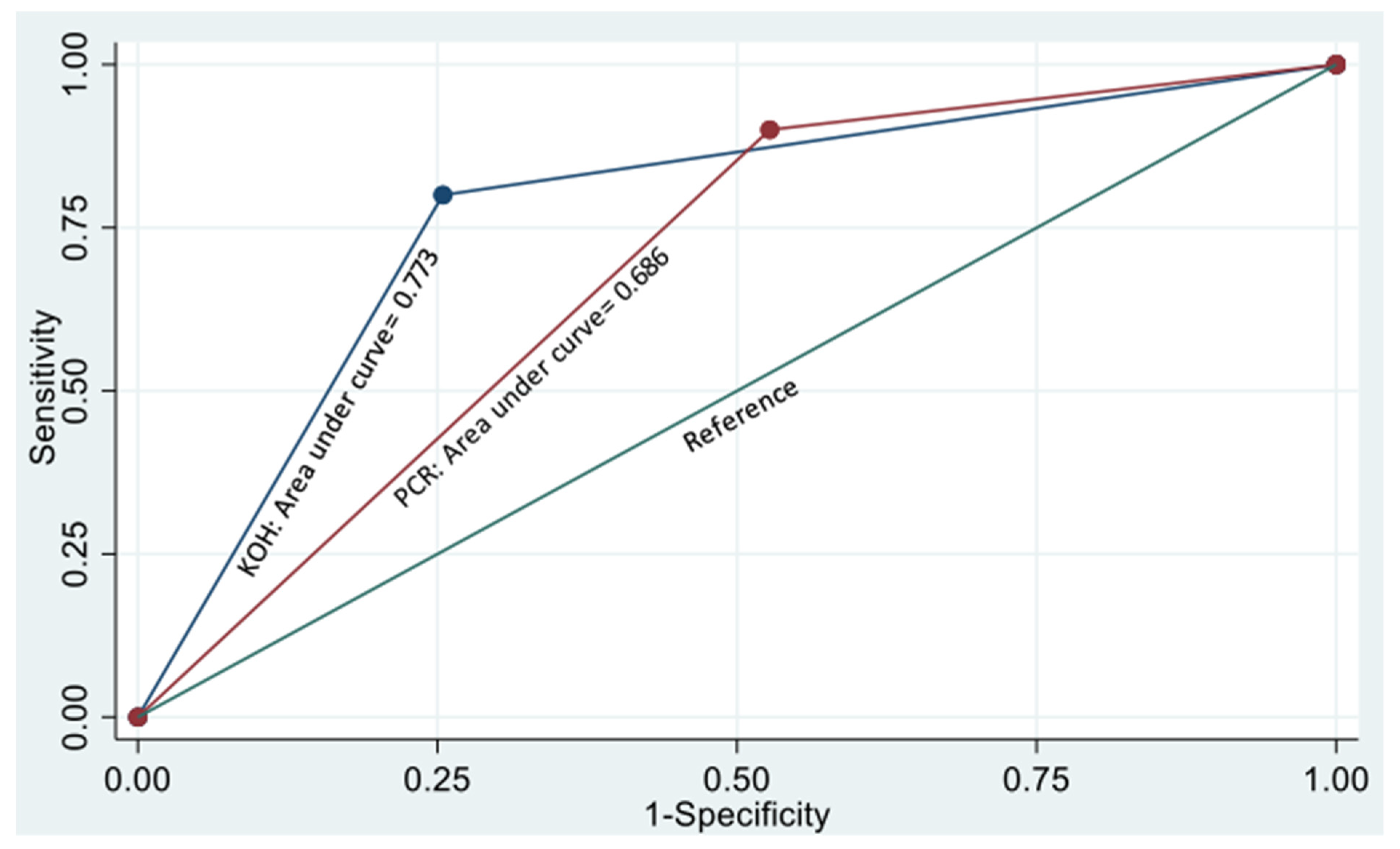
3.7. Comparison of the Diagnostic Performance of Various Tests
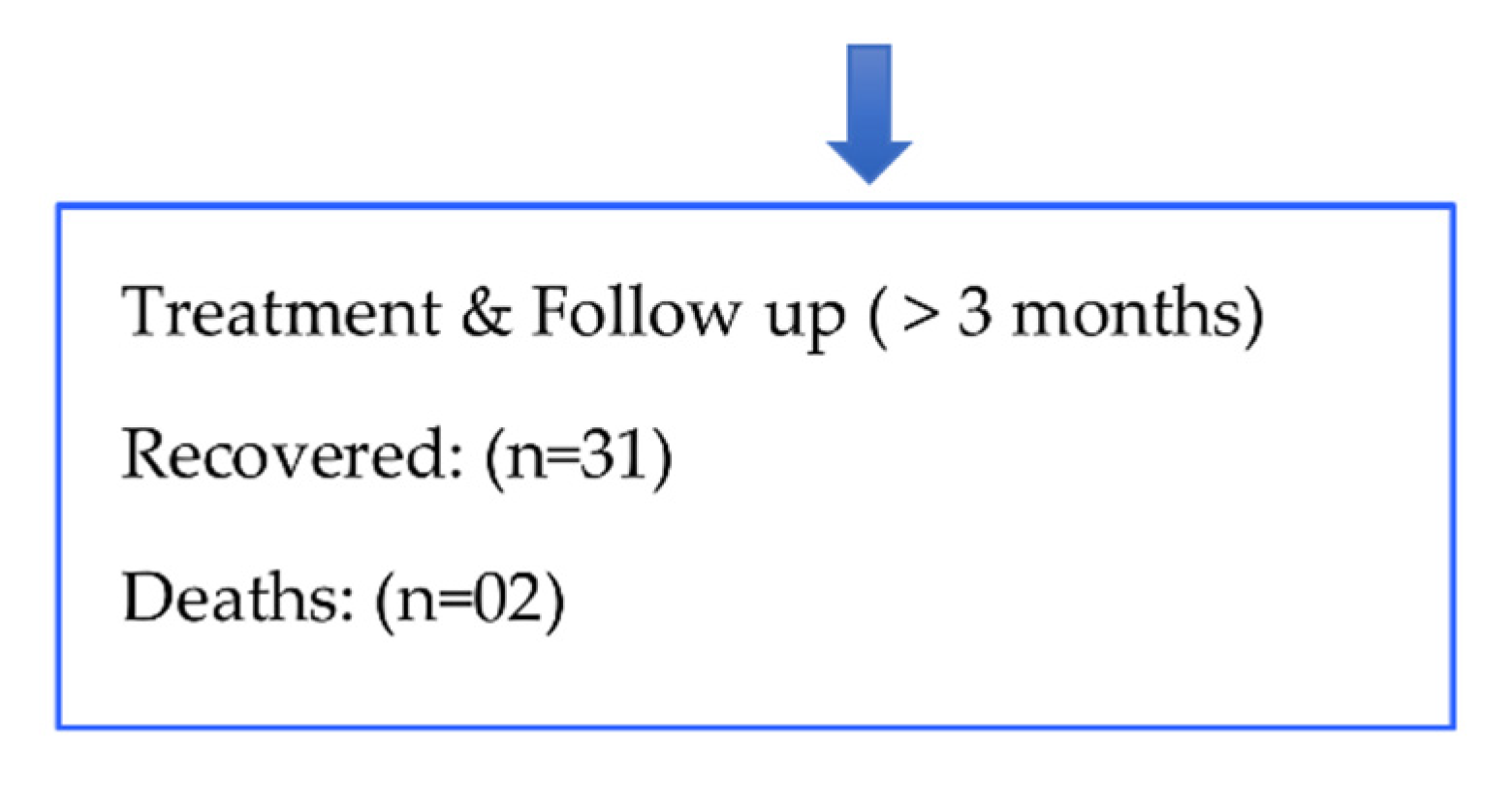
3.8. Treatment Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sarkar, S.; Gokhale, T.; Choudhury, S.S.; Deb, A.K. COVID-19 and orbital mucormycosis. Indian J. Ophthalmol. 2021, 69, 1002–1004. [Google Scholar] [PubMed]
- Honavar, S. Code Mucor: Guidelines for the Diagnosis, Staging and Management of Rhino-Orbito-Cerebral Mucormycosis in the Setting of COVID-19. Indian J. Ophthalmol. 2021, 69, 1361–1365. [Google Scholar] [CrossRef] [PubMed]
- Nagarathna, R.; Bali, P.; Anand, A.; Srivastava, V.; Patil, S.; Sharma, G.; Manasa, K.; Pannu, V.; Singh, A.; Nagendra, H.R. Prevalence of Diabetes and Its Determinants in the Young Adults Indian Population-Call for Yoga Intervention. Front. Endocrinol. 2020, 11, 507064. [Google Scholar] [CrossRef] [PubMed]
- Bari, M.; Hossain, M.; Akhter, S.; Emran, T. Delta variant and black fungal invasion: A bidirectional assault might worsen the massive second/third stream of COVID-19 outbreak in South-Asia. Ethic-Med. Public Health 2021, 19, 100722. [Google Scholar] [CrossRef]
- Asrani, P.; Eapen, M.S.; Hassan, I.; Sohal, S.S. Implications of the second wave of COVID-19 in India. Lancet Respir. Med. 2021, 9, e93–e94. [Google Scholar] [CrossRef]
- Chayakulkeeree, M.; Ghannoum, M.A.; Perfect, J.R. Zygomycosis: The re-emerging fungal infection. Eur. J. Clin. Microbiol. 2006, 25, 215–229. [Google Scholar] [CrossRef]
- Pandey, D.; Agarwal, M.; Chadha, S.; Aggarwal, D. Mixed opportunistic infection with Mucor, Aspergillus and Candida in oculo-rhino-cerebral mycosis: An uncommon case. J. Acad. Clin. Microbiol. 2019, 21, 47–49. [Google Scholar]
- Prakash, H.; Ghosh, A.K.; Rudramurthy, S.M.; Singh, P.; Xess, I.; Savio, J.; Pamidimukkala, U.; Jillwin, J.; Varma, S.; Das, A.; et al. A prospective multicenter study on mucormycosis in India: Epidemiology, diagnosis, and treatment. Med. Mycol. 2019, 57, 395–402. [Google Scholar] [CrossRef]
- Sipsas, N.V.; Gamaletsou, M.N.; Anastasopoulou, A.; Kontoyiannis, D.P. Therapy of Mucormycosis. J. Fungi 2018, 4, 90. [Google Scholar] [CrossRef]
- Zaman, K.; Rudramurthy, S.; Das, A.; Panda, N.; Honnavar, P.; Kaur, H.; Chakrabarti, A. Molecular diagnosis of rhino-orbito-cerebral mucormycosis from fresh tissue samples. J. Med. Microbiol. 2017, 66, 1124–1129. [Google Scholar] [CrossRef]
- Behera, H.S.; Barik, M.R.; Das, S.; Sharma, S. Simple polymerase chain reaction assay to differentiate between fungal and Pythium insidiosum keratitis. Clin. Exp. Ophthalmol. 2021, 49, 630–632. [Google Scholar] [CrossRef]
- Naik, M.N.; Rath, S. The ROC Staging System for COVID-related Rhino-Orbital-Cerebral Mucormycosis. Semin. Ophthalmol. 2021, 37, 279–283. [Google Scholar] [CrossRef]
- Sandhu, G.S.; Kline, B.C.; Stockman, L.; Roberts, G.D. Molecular probes for diagnosis of fungal infections. J. Clin. Microbiol. 1995, 33, 2913–2919. [Google Scholar] [CrossRef]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagro, K.; Lewis, R.E.; et al. Mucormycosis ECMM MSG Global Guideline Writing Group. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar]
- Aranjani, J.M.; Manuel, A.; Razack, H.I.A.; Mathew, S.T. COVID-19–associated mucormycosis: Evidence-based critical review of an emerging infection burden during the pandemic’s second wave in India. PLoS Negl. Trop. Dis. 2021, 15, e0009921. [Google Scholar] [CrossRef]
- Chowdhary, A.; Agarwal, K.; Meis, J.F. Filamentous Fungi in Respiratory Infections. What Lies Beyond Aspergillosis and Mucormycosis? PLOS Pathog. 2016, 12, e1005491. [Google Scholar] [CrossRef]
- Sen, M.; Honavar, S.G.; Bansal, R.; Sengupta, S.; Rao, R.; Kim, U.; Sharma, M.; Sachdev, M.; Grover, A.K.; Surve, A.; et al. Epidemiology, clinical profile, management, and outcome of COVID-19-associated rhino-orbital-cerebral mucormycosis in 2826 patients in India—Collaborative OPAI-IJO Study on Mucormycosis in COVID-19 (COSMIC), Report 1. Indian J. Ophthalmol. 2021, 69, 1670–1692. [Google Scholar]
- Badali, H.; Cañete-Gibas, C.; McCarthy, D.; Patterson, H.; Sanders, C.; David, M.P.; Mele, J.; Fan, H.; Wiederhold, N.P. Epidemiology and Antifungal Susceptibilities of Mucoralean Fungi in Clinical Samples from the United States. J. Clin. Microbiol. 2021, 59, JCM0123021. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Das, A.; Mandal, J.; Shivaprakash, M.R.; George, V.K.; Tarai, B.; Rao, P.; Panda, N.; Verma, S.C.; Sakhuja, V. The rising trend of invasive zygomycosis in patients with uncontrolled diabetes mellitus. Med. Mycol. 2006, 44, 335–342. [Google Scholar] [CrossRef]
- Tandon, A.; Pandey, L. COVID-19, steroids, and mucormycosis: What an ophthalmologist should know. Indian J. Ophthalmol. 2021, 69, 1970. [Google Scholar] [CrossRef]
- Lanternier, F.; Dannaoui, E.; Morizot, G.; Elie, C.; Garcia-Hermoso, D.; Huerre, M.; Bitar, D.; Dromer, F.; Lortholary, O.; The French Mycosis Study Group. A global analysis of mucormycosis in France: The RetroZygo Study (2005–2007). Clin. Infect. Dis. 2012, 54, S35–S43. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Chatterjee, S.S.; Das, A.; Panda, N.; Shivaprakash, M.R.; Kaur, A.; Varma, S.C.; Singhi, S.; Bhansali, A.; Sakhuja, V. Invasive zygomycosis in India: Experience in a tertiary care hospital. Postgrad. Med J. 2009, 85, 573–581. [Google Scholar] [CrossRef]
- Skiada, A.; Lass-Floerl, C.; Klimko, N.; Ibrahim, A.; Roilides, E.; Petrikkos, G. Challenges in the diagnosis and treatment of mucormycosis. Med Mycol. 2018, 56, S93–S101. [Google Scholar] [CrossRef]
- Lass-Flörl, C.; Mutschlechner, W.; Aigner, M.; Grif, K.; Marth, C.; Girschikofsky, M.; Grander, W.; Greil, R.; Russ, G.; Cerkl, P.; et al. Utility of PCR in Diagnosis of Invasive Fungal Infections: Real-Life Data from a Multicenter Study. J. Clin. Microbiol. 2013, 51, 863–868. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease Severity | ROC Gradng | Grade | Clinical + Nasal Endoscopy + Imaging Findings | No of Patients (n = 33) (%) |
|---|---|---|---|---|
| Mild | R (0, 1a, 1b) | 0 | Endoscopy normal, Imaging Normal | 15 (45.45%) |
| 1a | Only Nasal mucosa involved, Sinuses clear | |||
| 1b | Mucosal thickening of One or two sinuses | |||
| O (0, 1) | 0 | No orbital involvement, Vision Normal | ||
| 1 | Mild proptosis/movement restriction, One or Two EOMs enlarged, Vision normal | |||
| C (0) | 0 | No neurological signs, Cavernous sinus normal | ||
| Moderate | R (2a, 2b) | 2a | One or two sinuses hazy | 06 (18.18%) |
| 2b | Unilateral pansinusitis with mucosal thickening | |||
| O (2a, 2b) | 2a | Moderate proptosis/movement restriction medial/focal extra-conal orbital involvement with contrast enhancement | ||
| 2b | Moderate proptosis/movement restriction medial/focal extra-conal orbital involvement with no contrast enhancement | |||
| C (0) | 0 | No neurological signs, Cavernous sinus normal | ||
| Severe | R (3a, 3b) | 3a | Unilateral Sinusitis, completely hazy sinuses | 12 (36.36%) |
| 3b | Bilateral Sinusitis, complete or incompletely hazy | |||
| O (2c, 3a, 3b) | 2c | Localised subperiosteal abscess | ||
| 3a | Severe proptosis/complete ophthalmoplegia, No vision with diffuse orbital involvement | |||
| 3b | Severe proptosis/complete ophthalmoplegia, No vision with diffuse orbital involvement with SOV thrombosis | |||
| C (1, 2, 3) | 1 | Focal Cavernous sinus involvement | ||
| 2 | Focal Cavernous sinus involvement with cavernous sinus thrombosis | |||
| 3 | Unifocal or multifocal CNS disease |
| KOH + CFW | Culture | PCR Assay | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| M (+) | M + F (+) | F (+) | M (+) | M + F (+) | F (+) | M (+) | M + F (+) | F (+) | ||
| Sample Based Diagnosis (N = 83) | Nasal biopsy (n = 30) | 15 (50.0%) | 02 (6.7%) | 03 (10%) | 07 (23.3%) | 01 (3.3%) | 06 (20.0%) | 03 (10.0%) | 16 (53.3%) | 08 (26.7%) |
| Endonasal swabs (n = 27) | 02 (7.4%) | 01 (3.7%) | 01 (3.7%) | 0 (0%) | 0 (0%) | 03 (11.1%) | 03 (11.1%) | 11 (40.7%) | 07 (25.9%) | |
| Orbit Biopsy (n = 7) | 02 (28.6%) | 0 (0%) | 0 (0%) | 02 (28.6%) | 0 (0%) | 03 (42.9%) | 02 (28.5%) | 01 (14.3%) | 04 (57.1%) | |
| Brain Biopsy (n = 1) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 01 (100%) | 0 (0%) | 0 (0%) | |
| Lid Biopsy (n = 1) | 0 (0%) | 01 (100%) | 0 (0%) | 0 (0%) | 01 (100%) | 0 (0%) | 0 (0%) | 01 (100%) | 0 (0%) | |
| Control swabs (n= 17) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Patient Based Diagnosis (N = 33) | 15 (45.5%) | 03 (9.1%) | 04 (12.1%) | 06 (18.2%) | 03 (9.1%) | 07 (21.2%) | 03 (9.1 %) | 17 (51.5%) | 11 (33.3%) | |
| Sample (No of Patients) | KOH + CFW Positive (%) | KOH + CFW Negative | p Value | PCR Positive | PCR Negative | p Value | |
|---|---|---|---|---|---|---|---|
| Overall efficacy | Nasal Biopsy (n = 30) | 20 (66.7%) | 10 (33.3%) | NA | 27 (90%) | 03 (10%) | NA |
| Endonasal Swab (n = 27) | 04 (14.8%) | 23 (85.2%) | NA | 21 (77.8%) | 06 (22.2%) | NA | |
| Comparison of efficacy in select group of patients † | Nasal Biopsy (n = 25) | 17 (68.0%) | 08 (32.0%) | p < 0.001 | 23 (92.0%) | 02 (8.0%) | p = 0.247 |
| Endonasal Swab (n = 25) | 03 (12.0%) | 22 (88.0%) | 19 (76.0%) | 06 (24.0%) |
| Disease Severity | KOH + CFW Smear (95% CI) | PCR Assay (95% CI) | Tests in Series | Tests in Parallel | |
|---|---|---|---|---|---|
| Mild | Sn | 100.0% | 100% | 100% | 100% |
| Sp | 71.4% (55.3–87.6%) | 42.9% (25.2–60.6%) | 83.2% | 29.8% | |
| PPV | 20% (5.7–34.3%) | 11.1% (−0.13–22.4%) | - | - | |
| NPV | 100.0% | 100.0% | - | - | |
| Moderate to severe | Sn | 75% (60.9–89.1%) | 87.5% (76.7–98.3%) | 65.3% | 100% |
| Sp | 78.6% (65.2–92.0%) | 50.0% (33.7–66.3%) | 89% | 39.0% | |
| PPV | 50.0% (33.7–66.3%) | 33.3% (17.9–48.7%) | - | - | |
| NPV | 91.7% (82.6–100%) | 93.3% (85.2–101.5%) | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohapatra, S.; Barik, M.R.; Rath, S.; Sharma, S.; Mohapatra, A.; Behera, S.; Acharya, S.; Pattjoshi, D.R.; Padhi, R.K.; Behera, H.S. Diagnostic Performance and Clinical Utility of Conventional PCR Assay in Early Diagnosis of COVID-19 Associated Rhino-Orbito-Cerebral Mucormycosis. J. Fungi 2022, 8, 844. https://doi.org/10.3390/jof8080844
Mohapatra S, Barik MR, Rath S, Sharma S, Mohapatra A, Behera S, Acharya S, Pattjoshi DR, Padhi RK, Behera HS. Diagnostic Performance and Clinical Utility of Conventional PCR Assay in Early Diagnosis of COVID-19 Associated Rhino-Orbito-Cerebral Mucormycosis. Journal of Fungi. 2022; 8(8):844. https://doi.org/10.3390/jof8080844
Chicago/Turabian StyleMohapatra, Samir, Manas Ranjan Barik, Suryasnata Rath, Savitri Sharma, Archisman Mohapatra, Sharmistha Behera, Souvagini Acharya, Dipti Ranjan Pattjoshi, Rajesh Kumar Padhi, and Himansu Sekhar Behera. 2022. "Diagnostic Performance and Clinical Utility of Conventional PCR Assay in Early Diagnosis of COVID-19 Associated Rhino-Orbito-Cerebral Mucormycosis" Journal of Fungi 8, no. 8: 844. https://doi.org/10.3390/jof8080844