
Blastomycosis—Some Progress but Still Much to Learn


Abstract
:1. Introduction
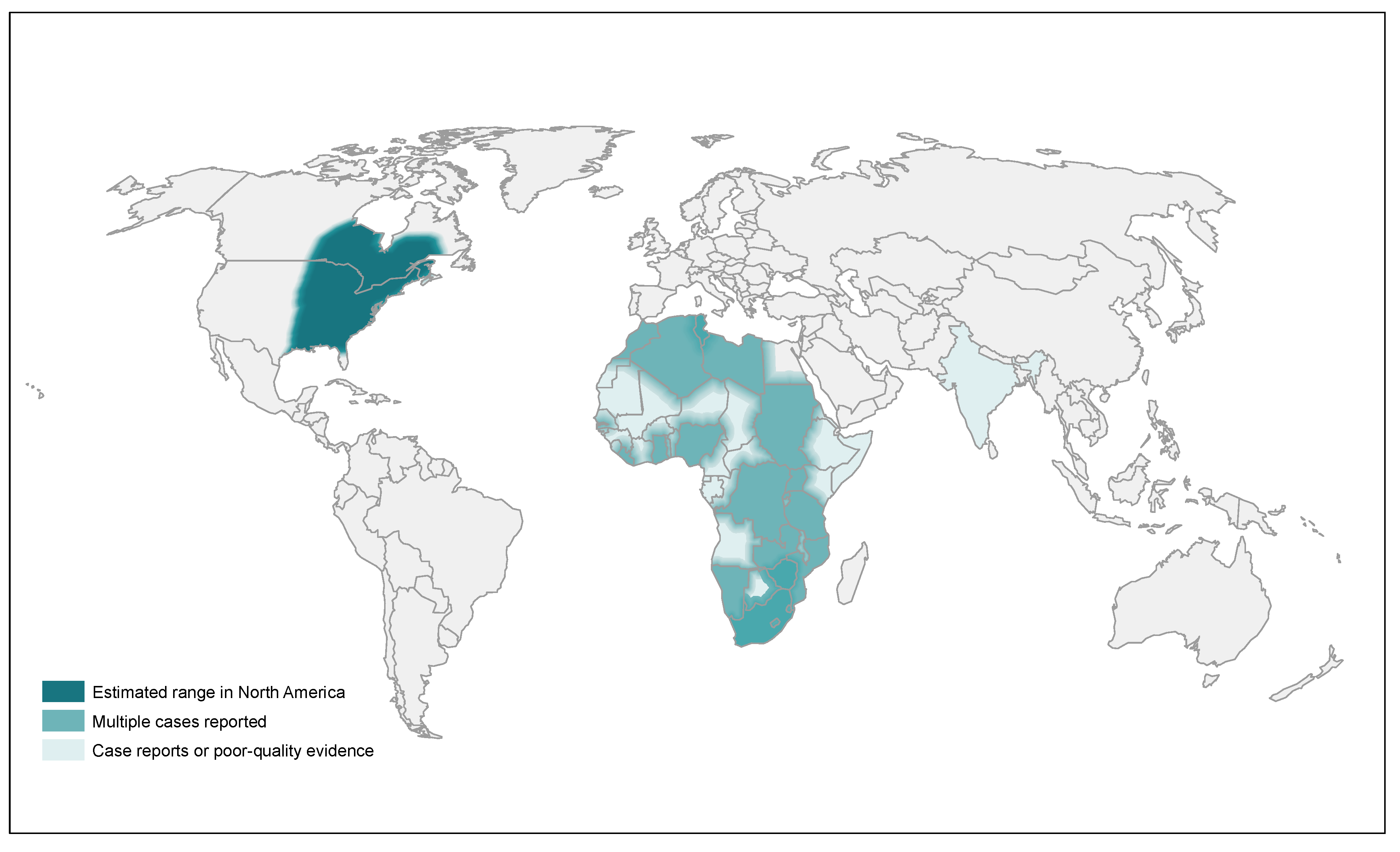
2. Epidemiology
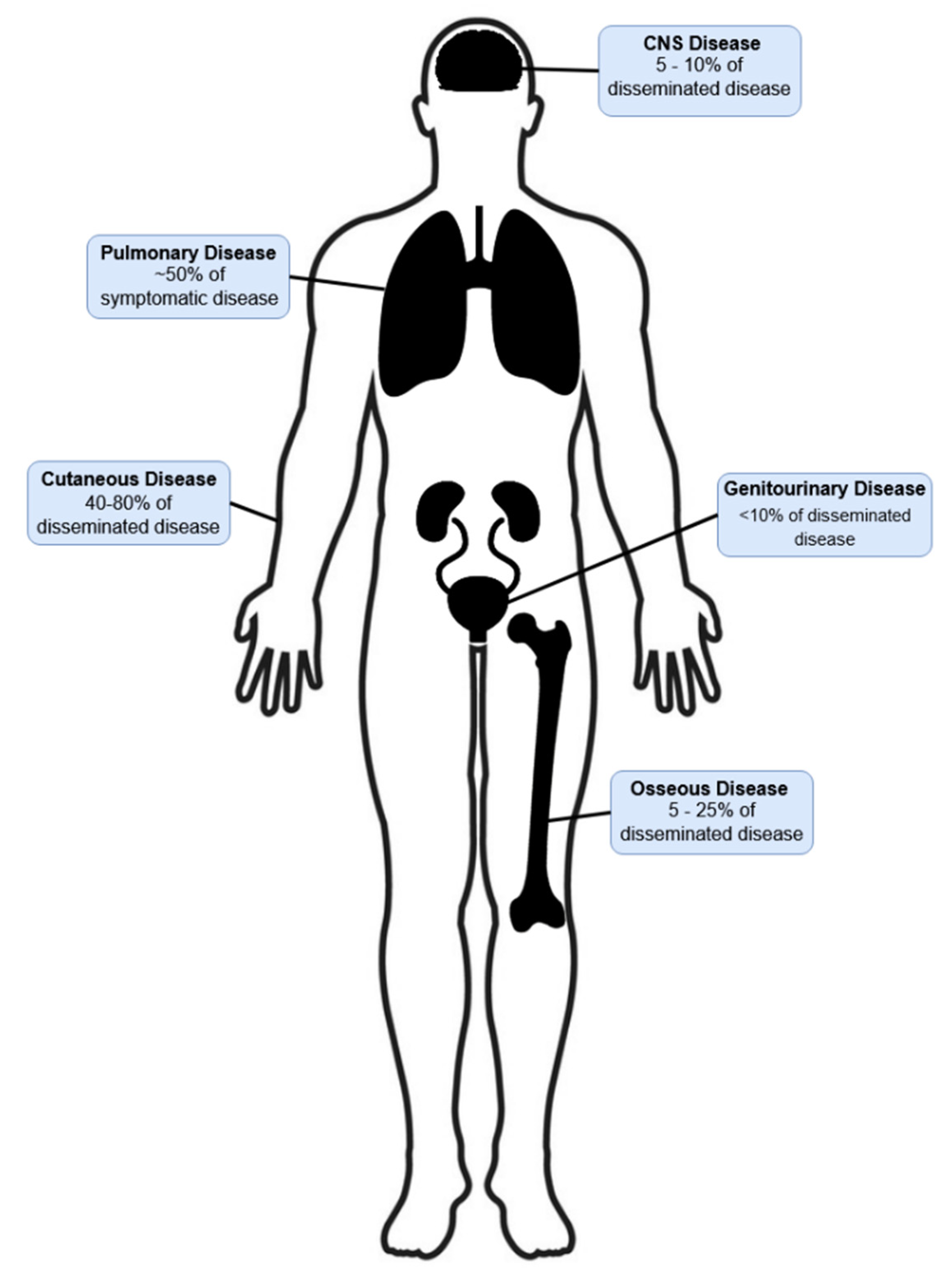
3. Clinical Presentation
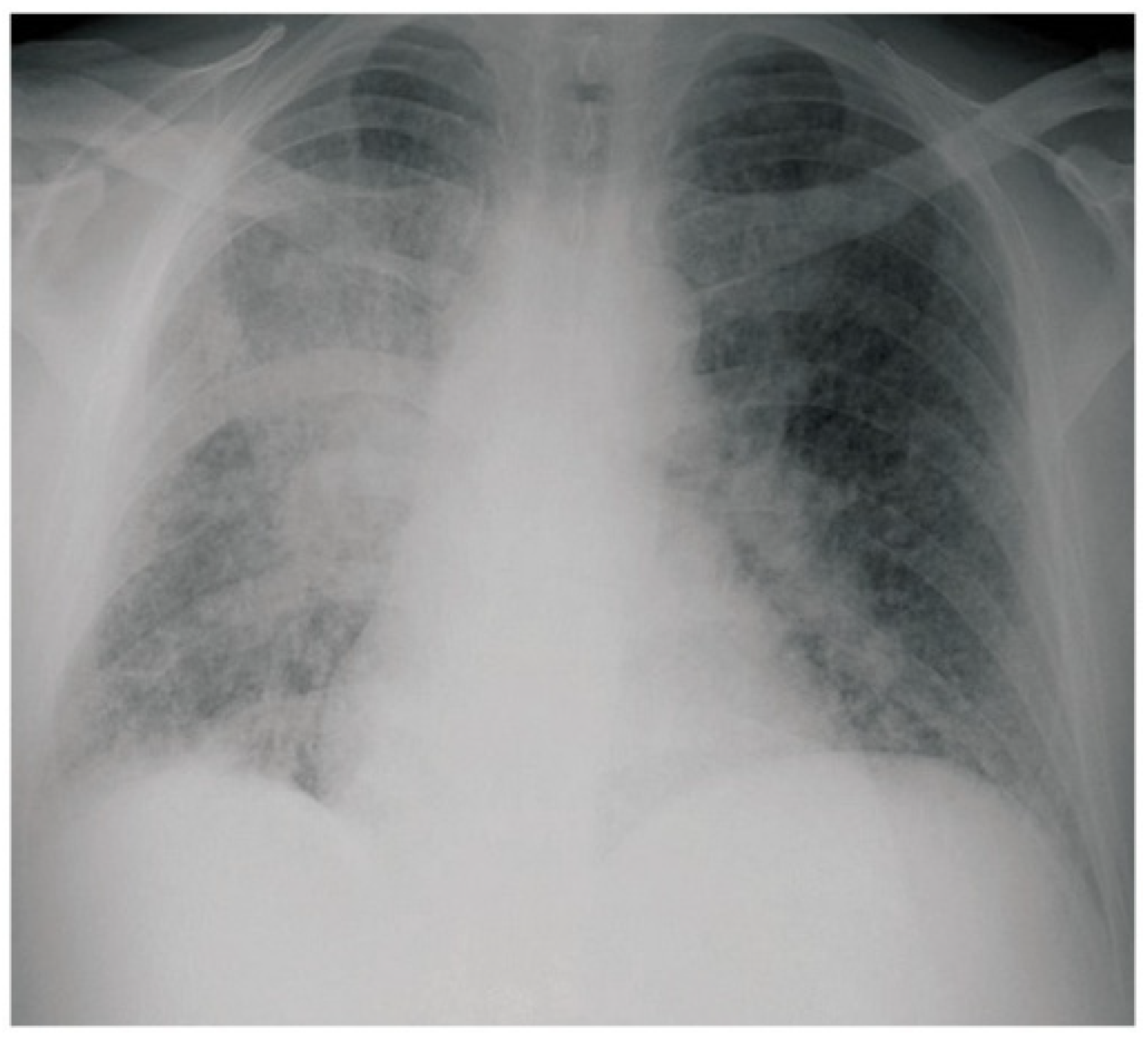
3.1. Pulmonary Blastomycosis
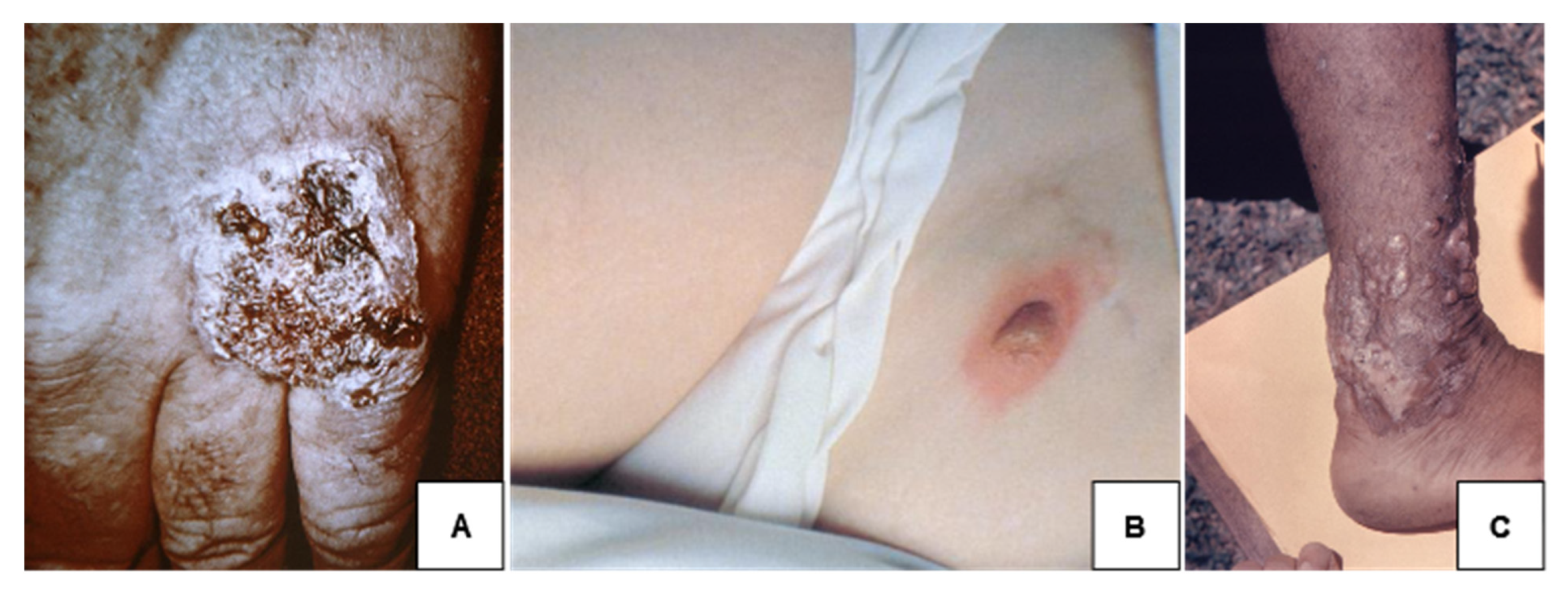
3.2. Cutaneous Blastomycosis
3.3. Osseous Blastomycosis
3.4. Genitourinary Blastomycosis
3.5. Central Nervous System Blastomycosis
4. Diagnosis
5. Treatment
5.1. Pulmonary Blastomycosis
5.1.1. Mild-to-Moderate Pulmonary Blastomycosis
5.1.2. Moderately Severe to Severe Pulmonary Blastomycosis
5.2. Disseminated/Extrapulmonary Blastomycosis
5.3. CNS Blastomycosis
6. Immunosuppressed Patients with Blastomycosis
7. Blastomycosis in Pregnancy and Newborns
8. Alternative Azoles
9. Future Research
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pfaller, M.A.; Diekema, D. Epidemiology of Invasive Mycoses in North America. Crit. Rev. Microbiol. 2010, 36, 1–53. [Google Scholar] [CrossRef]
- Vallabhaneni, S.; Mody, R.K.; Walker, T.; Chiller, T. The Global Burden of Fungal Diseases. Infect. Dis. Clin. N. Am. 2016, 30, 1–11. [Google Scholar] [CrossRef]
- Wheat, J. Endemic mycoses in AIDS: A clinical review. Clin. Microbiol. Rev. 1995, 8, 146–159. [Google Scholar] [CrossRef] [PubMed]
- Khuu, D.; Shafir, S.; Bristow, B.; Sorvillo, F. Blastomycosis Mortality Rates, United States, 1990–2010. Emerg. Infect. Dis. 2014, 20, 1789–1794. [Google Scholar] [CrossRef]
- Ashraf, N.; Kubat, R.C.; Poplin, V.; Adenis, A.A.; Denning, D.W.; Wright, L.; McCotter, O.; Schwartz, I.S.; Jackson, B.R.; Chiller, T.; et al. Re-drawing the Maps for Endemic Mycoses. Mycopathologia 2020, 185, 843–865. [Google Scholar] [CrossRef]
- Linder, K.A.; Kauffman, C.A. Current and New Perspectives in the Diagnosis of Blastomycosis and Histoplasmosis. J. Fungi 2020, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Maphanga, T.G.; Birkhead, M.; Muñoz, J.F.; Allam, M.; Zulu, T.G.; Cuomo, C.A.; Schwartz, I.S.; Ismail, A.; Naicker, S.D.; Mpembe, R.S.; et al. Human Blastomycosis in South Africa Caused by Blastomyces percursus and Blastomyces emzantsi sp. nov., 1967 to 2014. J. Clin. Microbiol. 2020, 58, e01661-19. [Google Scholar] [CrossRef]
- Schwartz, I.S.; Muñoz, J.F.; Kenyon, C.R.; Govender, N.P.; McTaggart, L.; Maphanga, T.G.; Richardson, S.; Becker, P.; Cuomo, C.A.; McEwen, J.G.; et al. Blastomycosis in Africa and the Middle East: A Comprehensive Review of Reported Cases and Reanalysis of Historical Isolates Based on Molecular Data. Clin. Infect. Dis. 2020, 73, e1560–e1569. [Google Scholar] [CrossRef]
- Kuzo, R.S.; Goodman, L.R. Blastomycosis. Semin. Roentgenol. 1996, 31, 45–51. [Google Scholar] [CrossRef]
- Fang, W.; Washington, L.; Kumar, N. Imaging Manifestations of Blastomycosis: A Pulmonary Infection with Potential Dissemination. RadioGraphics 2007, 27, 641–655. [Google Scholar] [CrossRef]
- Caceres, D.H.; Echeverri Tirado, L.C.; Bonifaz, A.; Adenis, A.; Gomez, B.L.; Lizette Banda Flores, C.; Canteros, C.E.; Santos, D.W.; Arathoon, E.; Soto, E.R.; et al. Current Situation of Endemic Mycosis in the Americas and the Caribbean: Proceedings of the First International Meeting on Endemic Mycoses of the Americas (IMEMA). Myocses 2022, in press. [Google Scholar] [CrossRef]
- Pfister, J.R.; Archer, J.R.; Hersil, S.; Boers, T.; Reed, K.D.; Meece, J.K.; Anderson, J.L.; Burgess, J.W.; Sullivan, T.D.; Klein, B.S.; et al. Non-Rural Point Source Blastomycosis Outbreak Near a Yard Waste Collection Site. Clin. Med. Res. 2010, 9, 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, J.W.; Schwan, W.R.; Volk, T.J. PCR-based detection of DNA from the human pathogen Blastomyces dermatitidis from natural soil samples. Med. Mycol. 2006, 44, 741–748. [Google Scholar] [CrossRef] [Green Version]
- Denton, J.F.; McDonough, E.S.; Ajello, L.; Ausherman, R.J. Isolation of Blastomyces dermatitidis from Soil. Science 1961, 133, 1126–1127. [Google Scholar] [CrossRef] [PubMed]
- Tenenbaum, M.J.; Greenspan, J.; Kerkering, T.M.; Utz, J.P. Blastomycosis. CRC Crit. Rev. Microbiol. 1982, 9, 139–163. [Google Scholar] [CrossRef]
- Sarosi, G.A.; Serstock, D.S. Isolation of Blastomyces dermatitidis from pigeon manure. Am. Rev. Respir. Dis. 1976, 114, 1179–1183. [Google Scholar] [CrossRef]
- Bialek, R.; Cirera, A.C.; Herrmann, T.; Aepinus, C.; Shearn-Bochsler, V.I.; Legendre, A.M. Nested PCR Assays for Detection of Blastomyces dermatitidis DNA in Paraffin-Embedded Canine Tissue. J. Clin. Microbiol. 2003, 41, 205–208. [Google Scholar] [CrossRef] [Green Version]
- Jackson, K.M.; Pelletier, K.C.; Scheftel, J.; Kerkaert, J.D.; Robinson, S.L.; McDonald, T.; Bender, J.B.; Knight, J.F.; Ireland, M.; Nielsen, K. Blastomyces dermatitidis Environmental Prevalence in Minnesota: Analysis and Modeling Using Soil Collected at Basal and Outbreak Sites. Appl. Environ. Microbiol. 2021, 87, e01922-20. [Google Scholar] [CrossRef]
- Baumgardner, D.J.; Burdick, J.S. An Outbreak of Human and Canine Blastomycosis. Clin. Infect. Dis. 1991, 13, 898–905. [Google Scholar] [CrossRef]
- Chen, T.; Legendre, A.M.; Bass, C.; Mays, S.E.; Odoi, A. A case-control study of sporadic canine blastomycosis in Tennessee, USA. Med. Mycol. 2008, 46, 843–852. [Google Scholar] [CrossRef] [Green Version]
- Furcolow, M.L.; Busey, J.F.; Menges, R.W.; Chick, E.W. Prevalence and incidence studies of human and canine blastomycosis. II. Yearly incidence studies in three selected states, 1960–1967. Am. J. Epidemiol. 1970, 92, 121–131. [Google Scholar] [CrossRef] [PubMed]
- McBride, J.A.; Gauthier, G.M.; Klein, B.S. Turning on virulence: Mechanisms that underpin the morphologic transition and pathogenicity of Blastomyces. Virulence 2018, 10, 801–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manetti, A.C. Hyperendemic urban blastomycosis. Am. J. Public Health 1991, 81, 633–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seitz, A.E.; Adjemian, J.; Steiner, C.A.; Prevots, D.R. Spatial epidemiology of blastomycosis hospitalizations: Detecting clusters and identifying environmental risk factors. Med. Mycol. 2015, 53, 447–454. [Google Scholar] [CrossRef] [Green Version]
- Brown, E.; McTaggart, L.R.; Dunn, D.; Pszczolko, E.; Tsui, K.G.; Morris, S.K.; Stephens, D.; Kus, J.V.; Richardson, S.E. Epidemiology and Geographic Distribution of Blastomycosis, Histoplasmosis, and Coccidioidomycosis, Ontario, Canada, 1990–2015. Emerg. Infect. Dis. 2018, 24, 1257–1266. [Google Scholar] [CrossRef] [Green Version]
- Baddley, J.W. Geographic Distribution of Endemic Fungal Infections among Older Persons, United States. Emerg. Infect. Dis. 2011, 17, 1664–1669. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Reportable Fungal Diseases by State. 2021. Available online: https://www.cdc.gov/fungal/fungal-disease-reporting-table.html (accessed on 17 June 2022).
- Benedict, K.; Thompson, G.R.; Deresinski, S.; Chiller, T. Mycotic Infections Acquired outside Areas of Known Endemicity, United States. Emerg. Infect. Dis. 2015, 21, 1935–1941. [Google Scholar] [CrossRef]
- Zampogna, J.C.; Hoy, M.J.; Ramos-Caro, F.A. Primary Cutaneous North American Blastomycosis in an Immunosuppressed Child. Pediatr. Dermatol. 2003, 20, 128–130. [Google Scholar] [CrossRef]
- Lehman, W.L.; Ray, L.F. Blastomycosis in Oregon. Northwest Med. 1951, 50, 39–40. [Google Scholar]
- McTaggart, L.R.; Brown, E.; Richardson, S.E. Phylogeographic Analysis of Blastomyces dermatitidis and Blastomyces gilchristii Reveals an Association with North American Freshwater Drainage Basins. PLoS ONE 2016, 11, e0159396. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, I.S.; Wiederhold, N.P.; E Hanson, K.; Patterson, T.F.; Sigler, L. Blastomyces helicus, a New Dimorphic Fungus Causing Fatal Pulmonary and Systemic Disease in Humans and Animals in Western Canada and the United States. Clin. Infect. Dis. 2018, 68, 188–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Frean, J.; Carman, W.F.; Crewe-Brown, H.H.; A Culligan, G.; Young, C.N. Blastomyces dermatitidis infections in the RSA. S. Afr. Med. J. 1989, 76, 13–16. [Google Scholar] [PubMed]
- Fragoyannis, S.; Van Wyk, G.; De Beer, M. North American blastomycosis in South Africa: A case report. S. Afr. Med. J. 1977, 51, 169–171. [Google Scholar] [PubMed]
- Emmons, C.; Murray, I.; Lurie, H.; King, M.; Tulloch, J.; Connor, D. North American blastomycosis: Two autochthonous cases from Africa. Med. Mycol. 1964, 3, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Emerson, P.A.; Higgins, E.; Branfoot, A. North American blastomycosis in Africans. Br. J. Dis. Chest 1984, 78, 286–291. [Google Scholar] [CrossRef]
- Carman, W.F.; Frean, J.A.; Crewe-Brown, H.H.; Culligan, G.A.; Young, C.N. Blastomycosis in Africa. Mycopathologia 1989, 107, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Baily, G.G.; Robertson, V.J.; Neill, P.; Garrido, P.; Levy, L.F. Blastomycosis in Africa: Clinical Features, Diagnosis, and Treatment. Clin. Infect. Dis. 1991, 13, 1005–1008. [Google Scholar] [CrossRef] [Green Version]
- Jordaan, H.F. Blastomycosis in Namibia-report of a case successfully treated with itraconazole. Clin. Exp. Dermatol. 1989, 14, 347–351. [Google Scholar] [CrossRef]
- Ibrahim, T.M.; Edinol, S.T. Pleural effusion from blastomycetes in an adult Nigerian: A case report. Niger. Postgrad. Med. J. 2001, 8, 148–149. [Google Scholar]
- Malak, J.A.; Farah, F.S. Blastomycosis in the Middle East. Report of a suspected case of North American blastomycosis. Br. J. Dermatol. 1971, 84, 161–166. [Google Scholar] [CrossRef]
- Randhawa, H.S.; Chowdhary, A.; Kathuria, S.; Roy, P.; Misra, D.S.; Jain, S.; Chugh, T.D. Blastomycosis in India: Report of an imported case and current status. Med. Mycol. 2013, 51, 185–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silversides, A.; Greer, A.; Ng, V.; Fisman, D. CMA opposes gender discrimination against doctors. Can. Med. Assoc. J. 2008, 178, 715–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, B.S.; Vergeront, J.M.; Weeks, R.J.; Kumar, U.N.; Mathai, G.; Varkey, B.; Kaufman, L.; Bradsher, R.W.; Stoebig, J.F.; Davis, J.P.; et al. Isolation of Blastomyces dermatitidis in Soil Associated with a Large Outbreak of Blastomycosis in Wisconsin. N. Engl. J. Med. 1986, 314, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Tosh, F.E.; Hammerman, K.J.; Weeks, R.J.; Sarosi, G.A. A common source epidemic of North American blastomycosis. Am. Rev. Respir. Dis. 1974, 109, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.W.; Dismukes, W.E.; Proia, L.A.; Bradsher, R.W.; Pappas, P.G.; Threlkeld, M.G.; Kauffman, C.A. Clinical Practice Guidelines for the Management of Blastomycosis: 2008 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2008, 46, 1801–1812. [Google Scholar] [CrossRef]
- McBride, J.A.; Gauthier, G.M.; Klein, B.S. Clinical Manifestations and Treatment of Blastomycosis. Clin. Chest Med. 2017, 38, 435–449. [Google Scholar] [CrossRef]
- Crampton, T.L.; Light, R.B.; Berg, G.M.; Meyers, M.P.; Schroeder, G.C.; Hershfield, E.S.; Embil, J.M. Epidemiology and Clinical Spectrum of Blastomycosis Diagnosed at Manitoba Hospitals. Clin. Infect. Dis. 2002, 34, 1310–1316. [Google Scholar] [CrossRef] [Green Version]
- Fanella, S.; Skinner, S.; Trepman, E.; Embil, J.M. Blastomycosis in children and adolescents: A 30-year experience from Manitoba. Med. Mycol. 2011, 49, 627–632. [Google Scholar] [CrossRef] [Green Version]
- Maini, R.; Ranjha, S.; Tandan, N.; Regmi, M.R.; Ullah, S.; Stone, T.; Nayeemuddin, F.; Pervin, N. Pulmonary Blastomycosis: A case series and review of unique radiological findings. Med. Mycol. Case Rep. 2020, 28, 49–54. [Google Scholar] [CrossRef]
- Brown, L.R.; Swensen, S.J.; Van Scoy, R.E.; Prakash, U.B.; Coles, D.T.; Colby, T.V. Roentgenologic Features of Pulmonary Blastomycosis. Mayo Clin. Proc. 1991, 66, 29–38. [Google Scholar] [CrossRef]
- Tobar, P.; Sanchez-Nadales, A.; Caldeira, E.; Saad, P. Unusual presentation of pulmonary blastomycosis complicated by amphotericin-induced refractory electrolyte abnormalities. Oxf. Med. Case Rep. 2020, 2020, omaa093. [Google Scholar] [CrossRef]
- Hussaini, S.M.Q.; Madut, D.; Tong, B.C.; Pavlisko, E.N.; Schell, W.A.; Perfect, J.R.; Thielman, N.M. Pulmonary blastomycosis presenting as primary lung cancer. BMC Infect. Dis. 2018, 18, 336. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Kunoor, A.; Eapen, M.; Singh, P.K.; Chowdhary, A. Blastomycosis Misdiagnosed as Tuberculosis, India. Emerg. Infect. Dis. 2019, 25, 1776–1777. [Google Scholar] [CrossRef] [PubMed]
- Koroscil, U.M.T.; Skabelund, U.A. Chronic Pulmonary Blastomycosis Mimicking Pulmonary Tuberculosis. Mil. Med. 2018, 183, e332–e333. [Google Scholar] [CrossRef] [Green Version]
- Sarkar, P.K.; Malhotra, P.; Sriram, P.S. Rapid Progression of Pulmonary Blastomycosis in an Untreated Patient of Chronic Lymphocytic Leukemia. Case Rep. Med. 2014, 2014, 514382. [Google Scholar] [CrossRef] [PubMed]
- Bariola, J.R.; Perry, P.; Pappas, P.G.; Proia, L.; Shealey, W.; Wright, P.W.; Sizemore, J.M.; Robinson, M.; Bradsher, J.R.W. Blastomycosis of the Central Nervous System: A Multicenter Review of Diagnosis and Treatment in the Modern Era. Clin. Infect. Dis. 2010, 50, 797–804. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.A.; Riddell, J.; Kauffman, C.A. Cutaneous Manifestations of Endemic Mycoses. Curr. Infect. Dis. Rep. 2013, 15, 440–449. [Google Scholar] [CrossRef]
- Caldito, E.G.; Ajiboye, O.; Flores, E.; Antia, C.; Demarais, P. The importance of skin exam in chronic pulmonary blastomycosis. IDCases 2020, 20, e00812. [Google Scholar] [CrossRef]
- Reder, P.A.; Neel, H.B. Blastornycosis in Otolaryngology. Laryngoscope 1993, 103 Pt 1, 53–58. [Google Scholar] [CrossRef]
- Saccente, M.; Woods, G.L. Clinical and Laboratory Update on Blastomycosis. Clin. Microbiol. Rev. 2010, 23, 367–381. [Google Scholar] [CrossRef] [Green Version]
- Clinton, T.S.; Timko, A.L. Cutaneous Blastomycosis without Evidence of Pulmonary Involvement. Mil. Med. 2003, 168, 651–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, R.; Singh, K.; Lamzabi, I.; Harbhajanka, A.; Gattuso, P.; Reddy, V.B. Blastomycosis of Bone. Am. J. Clin. Pathol. 2014, 142, 609–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oppenheimer, M.; Embil, J.M.; Black, B.; Wiebe, L.; Limerick, B.; MacDonald, K.; Trepman, E. Blastomycosis of Bones and Joints. South. Med. J. 2007, 100, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Nokes, S.R.; Adametz, J.; Gardner, G.; Beaton, J.N. Radiological case of the month. Blastomycosis osteomyelitis with epidural and retropharyngeal abscess. J. Ark. Med. Soc. 1995, 92, 253–254. [Google Scholar]
- Saccente, M.; Abernathy, R.S.; Pappas, P.G.; Shah, H.R.; Bradsher, R.W. Vertebral blastomycosis with paravertebral abscess: Report of eight cases and review of the literature. Clin. Infect. Dis. 1998, 26, 413–418. [Google Scholar] [CrossRef] [Green Version]
- Saiz, P.; Gitelis, S.; Virkus, W.; Piasecki, P.; Bengana, C.; Templeton, A. Blastomycosis of Long Bones. Clin. Orthop. Relat. Res. 2004, 421, 255–259. [Google Scholar] [CrossRef]
- Codifava, M.; Guerra, A.; Rossi, G.; Paolucci, P.; Iughetti, L. Unusual osseous presentation of blastomycosis in an immigrant child: A challenge for European pediatricians. Ital. J. Pediatrics 2012, 38, 69. [Google Scholar] [CrossRef] [Green Version]
- Bergner, D.M.; Kraus, S.D.; Duck, G.B.; Lewis, R. Systemic Blastomycosis Presenting with Acute Prostatic Abscess. J. Urol. 1981, 126, 132–133. [Google Scholar] [CrossRef]
- Sloan, M.J.; Manjee, K.G.; Kaplan, L.J.; Glaser, A.P. Prostatic abscess due to blastomycosis. Urol. Case Rep. 2022, 42, 102007. [Google Scholar] [CrossRef]
- Eickenberg, H.-U.; Amin, M.; Lich, R. Blastomycosis of the Genitourinary Tract. J. Urol. 1975, 113, 650–652. [Google Scholar] [CrossRef]
- Seo, R.; Oyasu, R.; Schaeffer, A. Blastomycosis of the epididymis and prostate. Urology 1997, 50, 980–982. [Google Scholar] [CrossRef]
- Labastida, L.G.; Quintana, O.B.; Sánchez, I.P.R.; Delgado-Enciso, I.; Guzmán-Esquivel, J.; Macías, G.S.G.; Ancer-Rodríguez, J.; Garza-Guajardo, R. Prostatic Blastomycosis: An Infrequent Cause of Granulomatous Prostatitis. Fungal Genom. Biol. 2016, 6. [Google Scholar] [CrossRef] [Green Version]
- Mouzin, E.L.; Seilke, M.A. Female Genital Blastomycosis: Case Report and Review. Clin. Infect. Dis. 1996, 22, 718–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, J.J.; Clark, C.A.; Lands, R.H.; Heim, C.R.; Burnett, L.S. Reactivation blastomycosis presenting as a tuboovarian abscess. Obstet. Gynecol. 1984, 64, 828. [Google Scholar] [PubMed]
- Farber, E.R.; Leahy, M.S.; Meadows, T.R. Endometrial blastomycosis acquired by sexual contact. Obstet. Gynecol. 1968, 32, 195–199. [Google Scholar]
- Bakleh, M.; Aksamit, A.J.; Tleyjeh, I.; Marshall, W.F. Successful Treatment of Cerebral Blastomycosis with Voriconazole. Clin. Infect. Dis. 2005, 40, e69–e71. [Google Scholar] [CrossRef] [Green Version]
- Kravitz, G.R.; Davies, S.F.; Eckman, M.R.; Sarosi, G.A. Chronic blastomycotic meningitis. Am. J. Med. 1981, 71, 501–505. [Google Scholar] [CrossRef]
- Friedman, J.A.; Wijdicks, E.F.; Fulgham, J.R.; Wright, A.J. Meningoencephalitis Due to Blastomyces dermatitidis: Case Report and Literature Review. Mayo Clin. Proc. 2000, 75, 403–408. [Google Scholar] [CrossRef] [Green Version]
- Majdick, K.; Kaye, K.; Shorman, M.A. Central nervous system blastomycosis clinical characteristics and outcomes. Med. Mycol. 2020, 59, 87–92. [Google Scholar] [CrossRef]
- Ryan, D.; Lippert, W.C.; Fenwick, A.J.; Bhatt, M.; Jones, C.R. Central Nervous System Blastomycosis With Multiple Brain Abscesses Presenting as Right Upper Extremity Weakness. Neurohospitalist 2019, 9, 230–234. [Google Scholar] [CrossRef]
- Gonyea, E.F. The spectrum of primary blastomycotic meningitis: A review of central nervous system blastomycosis. Ann. Neurol. 1978, 3, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Benzel, E.C.; King, J.W.; Mirfakhraee, M.; West, B.C.; Misra, R.P.; Hadden, T.A. Blastomycotic meningitis. Surg. Neurol. 1986, 26, 192–196. [Google Scholar] [CrossRef]
- Rippon, J.W.; Zvetina, J.R.; Reyes, C. Case report: Miliary blastomycosis with cerebral involvement. Mycopathologia 1977, 60, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Sarosi, G.A.; Eckman, M.R.; Davies, S.F.; Laskey, W.K. Canine Blastomycosis as a Harbinger of Human Disease. Ann. Intern. Med. 1979, 91, 733. [Google Scholar] [CrossRef] [PubMed]
- Tekin, A.; Pinevich, Y.; Herasevich, V.; Pickering, B.W.; Vergidis, P.; Gajic, O.; O’Horo, J.C. Diagnostic delay in pulmonary blastomycosis: A case series reflecting a referral center experience. Infection 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Poplin, V.; Smith, C.; Milsap, D.; Zabel, L.; Bahr, N. Diagnosis of Pulmonary Infections Due to Endemic Fungi. Diagnostics 2021, 11, 856. [Google Scholar] [CrossRef]
- Wu, S.J.; Valyi-Nagy, T.; Engelhard, H.H.; Do, M.A.; Janda, W.M. Secondary Intracerebral Blastomycosis with Giant Yeast Forms. Mycopathologia 2005, 160, 253–257. [Google Scholar] [CrossRef]
- Alpern, J.D.; Bahr, N.C.; Vazquez-Benitez, G.; Boulware, D.R.; Sellman, J.S.; Sarosi, G.A. Diagnostic Delay and Antibiotic Overuse in Acute Pulmonary Blastomycosis. Open Forum Infect. Dis. 2016, 3, ofw078. [Google Scholar] [CrossRef] [Green Version]
- Carlos, W.G.; Rose, A.S.; Wheat, L.J.; Norris, S.; Sarosi, G.A.; Knox, K.S.; Hage, C.A. Blastomycosis in Indiana. Chest 2010, 138, 1377–1382. [Google Scholar] [CrossRef]
- Martynowicz, M.A.; Prakash, U.B.S. Pulmonary Blastomycosis. Chest 2002, 121, 768–773. [Google Scholar] [CrossRef] [Green Version]
- Kochar, P.S.; O Lath, C.; Klein, A.P.; Ulmer, J.L. Multimodality imaging in cranial blastomycosis, a great mimicker: Case-based illustration with review of clinical and imaging findings. Indian J. Radiol. Imaging 2016, 26, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, I.S.; Kauffman, C.A. Blastomycosis. Semin. Respir. Crit. Care Med. 2020, 41, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Connolly, P.; Hage, C.A.; Bariola, J.R.; Bensadoun, E.; Rodgers, M.; Bradsher, R.W.; Wheat, L.J. Blastomyces dermatitidis Antigen Detection by Quantitative Enzyme Immunoassay. Clin. Vaccine Immunol. 2012, 19, 53–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frost, H.M.; Novicki, T.J. Blastomyces Antigen Detection for Diagnosis and Management of Blastomycosis. J. Clin. Microbiol. 2015, 53, 3660–3662. [Google Scholar] [CrossRef] [Green Version]
- Bariola, J.R.; Hage, C.A.; Durkin, M.; Bensadoun, E.; Gubbins, P.O.; Wheat, L.J.; Bradsher, R.W. Detection of Blastomyces dermatitidis antigen in patients with newly diagnosed blastomycosis. Diagn. Microbiol. Infect. Dis. 2011, 69, 187–191. [Google Scholar] [CrossRef]
- Theel, E.S.; Rodino, K.G.; Granger, D. Detection of Blastomyces dermatitidis Antigen in Urine Using a Commercially Available Quantitative Enzyme Immunoassay. J. Clin. Microbiol. 2021, 59, e0144421. [Google Scholar] [CrossRef]
- O’Dowd, T.R.; Mc Hugh, J.W.; Theel, E.S.; Wengenack, N.L.; O’Horo, J.C.; Enzler, M.J.; Vergidis, P. Diagnostic Methods and Risk Factors for Severe Disease and Mortality in Blastomycosis: A Retrospective Cohort Study. J. Fungi 2021, 7, 888. [Google Scholar] [CrossRef]
- Hage, C.A.; Davis, T.E.; Fuller, D.; Egan, L.; Witt, J.R.; Wheat, L.J.; Knox, K.S. Diagnosis of Histoplasmosis by Antigen Detection in BAL Fluid. Chest 2010, 137, 623–628. [Google Scholar] [CrossRef]
- Cari, E.V.; Leedy, N.; Ribes, J.A.; Soria, J.; Myint, T. Risk factors of severe blastomycosis and comparison of diagnosis and outcomes between immunocompetent and immunocompromised patients. Mycoses 2021, 65, 239–246. [Google Scholar] [CrossRef]
- Durkin, M.; Witt, J.; LeMonte, A.; Wheat, B.; Connolly, P. Antigen Assay with the Potential To Aid in Diagnosis of Blastomycosis. J. Clin. Microbiol. 2004, 42, 4873–4875. [Google Scholar] [CrossRef] [Green Version]
- Richer, S.M.; Smedema, M.L.; Durkin, M.M.; Brandhorst, T.T.; Hage, C.A.; Connolly, P.A.; Leland, D.S.; Davis, T.E.; Klein, B.S.; Wheat, L.J. Development of a Highly Sensitive and Specific Blastomycosis Antibody Enzyme Immunoassay Using Blastomyces dermatitidis Surface Protein BAD-1. Clin. Vaccine Immunol. 2013, 21, 143–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sidamonidze, K.; Peck, M.K.; Perez, M.; Baumgardner, D.; Smith, G.; Chaturvedi, V.; Chaturvedi, S. Real-Time PCR Assay for Identification of Blastomyces dermatitidis in Culture and in Tissue. J. Clin. Microbiol. 2012, 50, 1783–1786. [Google Scholar] [CrossRef] [Green Version]
- Wang, N.; Luo, Z.; Deng, S.; Li, Q. A young male with chronic nonproductive cough diagnosed with blastomycosis in China: A case report. BMC Pulm. Med. 2020, 20, 189. [Google Scholar] [CrossRef]
- Recht, L.D.; Philips, J.R.; Eckman, M.R.; A Sarosi, G. Self-limited blastomycosis: A report of thirteen cases. Am. Rev. Respir. Dis. 1979, 120, 1109–1112. [Google Scholar] [CrossRef] [PubMed]
- Sarosi, G.A.; Davies, S.F.; Phillips, J.R. Self-limited blastomycosis: A report of 39 cases. Semin. Respir. Infect. 1986, 1, 40–44. [Google Scholar] [PubMed]
- Smith, J.A.; Kauffman, C.A. Blastomycosis. Proc. Am. Thorac. Soc. 2010, 7, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Rauseo, A.M.; Mazi, P.; Lewis, P.; Burnett, B.; Mudge, S.; Spec, A. Bioavailability of Single-Dose SUBA-Itraconazole Compared to Conventional Itraconazole under Fasted and Fed Conditions. Antimicrob. Agents Chemother. 2021, 65, e0013421. [Google Scholar] [CrossRef]
- Mayne Pharma. Mayne Pharma Received FDA Approval of TolsuraTM (SUBA®-Itraconazole Capsules) for the Treatment of Certain Fungal Infections [ess Release]. Cision PR Newswire. 2018. Available online: https://www.prnewswire.com/news-releases/mayne-pharma-receives-fda-approval-of-tolsura-suba-itraconazole-capsules-for-the-treatment-of-certain-fungal-infections-300763882.html (accessed on 1 August 2022).
- Pappas, P.G.; Bradsher, R.W.; Kauffman, C.A.; Cloud, G.A.; Thomas, C.J.; Campbell, J.G.D.; Chapman, S.W.; Newman, C.; Dismukes, W.E. The National Institute of Allergy and Infectious Diseases Mycoses Study Group Treatment of Blastomycosis with Higher Doses of Fluconazole. Clin. Infect. Dis. 1997, 25, 200–205. [Google Scholar] [CrossRef]
- National Institute of Allergy and Infectious Diseases Mycoses Study Group. Treatment of blastomycosis and histoplasmosis with ketoconazole. Results of a prospective randomized clinical trial. Ann. Intern. Med. 1985, 103 Pt 1, 861–872. [Google Scholar] [CrossRef]
- Freifeld, A.; Proia, L.; Andes, D.; Baddour, L.M.; Blair, J.; Spellberg, B.; Arnold, S.; Lentnek, A.; Wheat, L.J. Voriconazole Use for Endemic Fungal Infections. Antimicrob. Agents Chemother. 2009, 53, 1648–1651. [Google Scholar] [CrossRef] [Green Version]
- Falci, D.R.; Da Rosa, F.B.; Pasqualotto, A.C. Comparison of nephrotoxicity associated to different lipid formulations of amphotericin B: A real-life study. Mycoses 2015, 58, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.C.; McManus, E.J.; Maki, D.G. Overwhelming Pulmonary Blastomycosis Associated with the Adult Respiratory Distress Syndrome. N. Engl. J. Med. 1993, 329, 1231–1236. [Google Scholar] [CrossRef]
- Lahm, T.; Neese, S.; Thornburg, A.T.; Ober, M.D.; Sarosi, G.A.; Hage, C.A. Corticosteroids for Blastomycosis-Induced ARDS. Chest 2008, 133, 1478–1480. [Google Scholar] [CrossRef]
- Limper, A.H.; Knox, K.S.; Sarosi, G.A.; Ampel, N.M.; Bennett, J.E.; Catanzaro, A.; Davies, S.F.; Dismukes, W.E.; Hage, C.A.; Marr, K.A.; et al. An Official American Thoracic Society Statement: Treatment of Fungal Infections in Adult Pulmonary and Critical Care Patients. Am. J. Respir. Crit. Care Med. 2011, 183, 96–128. [Google Scholar] [CrossRef] [Green Version]
- Felton, T.; Troke, P.F.; Hope, W.W.; Simonsen, K.A.; Anderson-Berry, A.L.; Delair, S.F.; Dele Davies, H. Tissue Penetration of Antifungal Agents. Clin. Microbiol. Rev. 2014, 27, 68–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheat, L.J.; Freifeld, A.G.; Kleiman, M.B.; Baddley, J.W.; McKinsey, D.S.; Loyd, J.; Kauffman, C.A. Clinical Practice Guidelines for the Management of Patients with Histoplasmosis: 2007 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2007, 45, 807–825. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M.D.; Perfect, J.R. Fungal Infections of the Bones and Joints. Curr. Infect. Dis. Rep. 2001, 3, 450–460. [Google Scholar] [CrossRef]
- Groll, A.H.; Giri, N.; Petraitis, V.; Petraitiene, R.; Candelario, M.; Bacher, J.S.; Piscitelli, S.C.; Walsh, T.J. Comparative Efficacy and Distribution of Lipid Formulations of Amphotericin B in Experimental Candida albicans Infection of the Central Nervous System. J. Infect. Dis. 2000, 182, 274–282. [Google Scholar] [CrossRef] [Green Version]
- Ward, B.A.; Parent, A.D.; Raila, F. Indications for the surgical management of central nervous system blastomycosis. Surg. Neurol. 1995, 43, 379–388. [Google Scholar] [CrossRef]
- Pappas, P.G.; Pottage, J.C.; Powderly, W.G.; Fraser, V.J.; Stratton, C.W.; McKenzie, S.; Tapper, M.L.; Chmel, H.; Bonebrake, F.C.; Blum, R.; et al. Blastomycosis in Patients with the Acquired Immunodeficiency Syndrome. Ann. Intern. Med. 1992, 116, 847–853. [Google Scholar] [CrossRef]
- Pappas, P.G.; Threlkeld, M.G.; Bedsole, G.D.; Cleveland, K.O.; Gelfand, M.S.; Dismukes, W.E. Blastomycosis in Immunocompromised Patients. Medicine 1993, 72, 311–325. [Google Scholar] [CrossRef] [PubMed]
- McBride, J.A.; Sterkel, A.K.; Matkovic, E.; Broman, A.T.; Gibbons-Burgener, S.N.; Gauthier, G.M. Clinical Manifestations and Outcomes in Immunocompetent and Immunocompromised Patients With Blastomycosis. Clin. Infect. Dis. 2020, 72, 1594–1602. [Google Scholar] [CrossRef] [PubMed]
- Lemos, L.B.; Soofi, M.; Amir, E. Blastomycosis and pregnancy. Ann. Diagn. Pathol. 2002, 6, 211–215. [Google Scholar] [CrossRef]
- Scolarici, M.J.; King, C.; Sterkel, A.; Smith, J.; Gauthier, G.; Saddler, C. The Role of Isavuconazonium Sulphate for the Treatment of Blastomycosis: A Case Series and Antifungal Susceptibility. Open Forum. Infect. Dis. 2022, 9, ofac220. [Google Scholar] [CrossRef]
- Mehta, T.I.; Kurman, J.; Dolan, S.; Gill, H.; Thapa, B. Blastomycosis in Solid Organ Transplant Recipients—A Retrospective Series from Southeastern Wisconsin. Transpl. Infect. Dis. 2021, 123, e13671. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Infection | Drug(s) of Choice | Duration of Therapy |
|---|---|---|
| Pulmonary, mild to moderate | Itraconazole a | 6–12 months |
| Pulmonary, severe | Induction: Liposomal amphotericin (or amphotericin B deoxycholate) b Step-down: Itraconazole a | Induction therapy × 1–2 weeks (or until clinical improvement), then oral therapy × 6–12 months. |
| Disseminated, mild–moderate, no CNS involvement | Itraconazole a | At least 12 months |
| Disseminated, severe or with CNS involvement | Induction: Liposomal amphotericin (or amphotericin B deoxycholate) b Step-down: Itraconazole a | Induction therapy × 1–2 weeks (or until clinical improvement), then oral therapy × 6–12 months. |
| Immunosuppressed, any form of blastomycosis | Induction: Liposomal amphotericin (or amphotericin B deoxycholate) b Step-down: Itraconazole a | Induction therapy × 1–2 weeks (or until clinical improvement), then oral therapy × 6–12 months (can be continued as lifelong suppression if ongoing immunosuppression) c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pullen, M.F.; Alpern, J.D.; Bahr, N.C. Blastomycosis—Some Progress but Still Much to Learn. J. Fungi 2022, 8, 824. https://doi.org/10.3390/jof8080824
Pullen MF, Alpern JD, Bahr NC. Blastomycosis—Some Progress but Still Much to Learn. Journal of Fungi. 2022; 8(8):824. https://doi.org/10.3390/jof8080824
Chicago/Turabian StylePullen, Matthew F., Jonathan D. Alpern, and Nathan C. Bahr. 2022. "Blastomycosis—Some Progress but Still Much to Learn" Journal of Fungi 8, no. 8: 824. https://doi.org/10.3390/jof8080824