

Spinal Arachnoiditis in Patients with Coccidioidomycosis Meningitis—Analysis of Clinical and Imaging Features
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients Selection
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bays, D.J.; Thompson, G.R., 3rd. Coccidioidomycosis. Infect. Dis. Clin. N. Am. 2021, 35, 453–469. [Google Scholar] [CrossRef]
- McCotter, O.Z.; Benedict, K.; Engelthaler, D.M.; Komatsu, K.; Lucas, K.D.; Mohle-Boetani, J.C.; Oltean, H.; Vugia, D.; Chiller, T.M.; Cooksey, G.L.S.; et al. Update on the Epidemiology of coccidioidomycosis in the United States. Med. Mycol. 2019, 57 (Suppl. 1), S30–S40. [Google Scholar] [CrossRef] [PubMed]
- Donovan, F.M.; Shubitz, L.; Powell, D.; Orbach, M.; Frelinger, J.; Galgiani, J.N. Early Events in Coccidioidomycosis. Clin. Microbiol. Rev. 2019, 33, e00112-19. [Google Scholar] [CrossRef] [PubMed]
- Rosenstein, N.E.; Emery, K.W.; Ben Werner, S.; Kao, A.; Johnson, R.; Rogers, D.; Vugia, D.; Reingold, A.; Talbot, R.; Plikaytis, B.D.; et al. Risk factors for severe pulmonary and disseminated coccidioidomycosis: Kern County, California, 1995–1996. Clin. Infect. Dis. 2001, 32, 708–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stockamp, N.W.; Thompson, G.R., 3rd. Coccidioidomycosis. Infect. Dis. Clin. N. Am. 2016, 30, 229–246. [Google Scholar] [CrossRef]
- Kelly, P.C. Coccidioidal Meningitis. In Coccidioidomycosis: A Text; Stevens, D.A., Ed.; Springer: Worcester, MA, USA, 1980; pp. 163–193. [Google Scholar] [CrossRef]
- Johnson, R.; Ho, J.; Fowler, P.; Heidari, A. Coccidioidal Meningitis: A Review on Diagnosis, Treatment, and Management of Complications. Curr. Neurol. Neurosci. Rep. 2018, 18, 19. [Google Scholar] [CrossRef]
- Wrobel, C.J.; Chappell, E.T.; Taylor, W. Clinical presentation, radiological findings, and treatment results of coccidioidomycosis involving the spine: Report on 23 cases. J. Neurosurg. 2001, 95 (Suppl. 1), 33–39. [Google Scholar] [CrossRef]
- Sakya, S.M.; Sakya, J.P.; Hallan, D.R.; Warraich, I. Spinal Coccidioidomycosis: A Complication from Medication Noncompliance. Cureus 2020, 12, e9304. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.A.; Kasliwal, M.K.; Nag, S.; O’Toole, J.E.; Traynelis, V.C. Rapidly progressive quadriparesis heralding disseminated coccidioidomycosis in an immunocompetent patient. J. Clin. Neurosci. 2014, 21, 1049–1051. [Google Scholar] [CrossRef]
- Jackson, N.R.; Blair, J.E.; Ampel, N.M. Central Nervous System Infections Due to Coccidioidomycosis. J. Fungi 2019, 5, 54. [Google Scholar] [CrossRef] [Green Version]
- Lammering, J.C.; Iv, M.; Gupta, N.; Pandit, R.; Patel, M.R. Imaging spectrum of CNS coccidioidomycosis: Prevalence and significance of concurrent brain and spinal disease. AJR Am. J. Roentgenol. 2013, 200, 1334–1346. [Google Scholar] [CrossRef]
- Crete, R.N.; Gallmann, W.; Karis, J.P.; Ross, J. Spinal Coccidioidomycosis: MR Imaging Findings in 41 Patients. AJNR Am. J. Neuroradiol. 2018, 39, 2148–2153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morshed, R.A.; Lee, A.T.; Egladyous, A.; Avalos, L.N.; Aghi, M.K.; Theodosopoulos, P.V.; McDermott, M.W.; Hervey-Jumper, S.L. Shunt Treatment for Coccidioidomycosis-Related Hydrocephalus: A Single-Center Series. World Neurosurg. 2020, 138, e883–e891. [Google Scholar] [CrossRef]
- Wright, M.H.; Denney, L.C. A comprehensive review of spinal arachnoiditis. Orthop. Nurs. 2003, 22, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Nadeem, S.F.; Baig, A.N.; Tariq, Q.U.A.; Shamim, M.S. Spinal arachnoiditis and syringomyelia: Review of literature with emphasis on postinfectious inflammation and treatment. Surg. Neurol. Int. 2022, 13, 299. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Conermann, T. Arachnoiditis. In StatPearls [Internet]; StatPearls Publishing: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Nardone, R.; Alessandrini, F.; Tezzon, F. Syringomyelia following Listeria meningoencephalitis: Report of a case. Neurol. Sci. 2003, 24, 40–43. [Google Scholar] [CrossRef]
- Nash, T.E.; O’Connell, E.M. Subarachnoid neurocysticercosis: Emerging concepts and treatment. Curr. Opin. Infect. Dis. 2020, 33, 339–346. [Google Scholar] [CrossRef]
- Panackal, A.A.; Komori, M.; Kosa, P.; Khan, O.; Hammoud, D.A.; Rosen, L.B.; Browne, S.K.; Lin, Y.-C.; Romm, E.; Ramaprasad, C.; et al. Spinal Arachnoiditis as a Complication of Cryptococcal Meningoencephalitis in Non-HIV Previously Healthy Adults. Clin. Infect. Dis. 2017, 64, 275–283. [Google Scholar] [CrossRef] [Green Version]
- Kannapadi, N.V.; Alomari, S.O.; Caturegli, G.; Bydon, A.; Cho, S.-M. Management of syringomyelia associated with tuberculous meningitis: A case report and systematic review of the literature. J. Clin. Neurosci. 2021, 87, 20–25. [Google Scholar] [CrossRef]
- Gupta, R.; Garg, R.K.; Jain, A.; Malhotra, H.S.; Verma, R.; Sharma, P.K. Spinal cord and spinal nerve root involvement (myeloradiculopathy) in tuberculous meningitis. Medicine 2015, 94, e404. [Google Scholar] [CrossRef]
- Garg, R.K.; Malhotra, H.S.; Gupta, R. Spinal cord involvement in tuberculous meningitis. Spinal Cord. 2015, 53, 649–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, T.L.; Morris, J.M.; Wald, J.T.; Kotsenas, A.L. Imaging Appearance of Advanced Chronic Adhesive Arachnoiditis: A Retrospective Review. AJR Am. J. Roentgenol. 2017, 209, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R.; Ampel, N.M.; Blair, J.E.; Donovan, F.; Fierer, J.; Galgiani, J.N.; Heidari, A.; Johnson, R.; Shatsky, S.A.; Uchiyama, C.M.; et al. Controversies in the Management of Central Nervous System Coccidioidomycosis. Clin. Infect. Dis. 2022, 75, 555–559. [Google Scholar] [CrossRef]
- Galgiani, J.N.; Ampel, N.M.; Blair, J.E.; Catanzaro, A.; Geertsma, F.; Hoover, S.E.; Johnson, R.H.; Kusne, S.; Lisse, J.; MacDonald, J.D.; et al. Executive Summary: 2016 Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for the Treatment of Coccidioidomycosis. Clin. Infect. Dis. 2016, 63, 717–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathisen, G.; Shelub, A.; Truong, J.; Wigen, C. Coccidioidal meningitis: Clinical presentation and management in the fluconazole era. Medicine 2010, 89, 251–284. [Google Scholar] [CrossRef]
- Ho, J.; Fowler, P.; Heidari, A.; Johnson, R.H. Intrathecal Amphotericin B: A 60-Year Experience in Treating Coccidioidal Meningitis. Clin. Infect. Dis. 2017, 64, 519–524. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics |
| Age: 39 [25, 55] (Median IQR **) Sex: Male 29 (78%), Female 8 (22%) Ethnicity: Hispanic 17 (46%), non-Hispanic 20 (54%) Race: Caucasian 24 (64%), African American 5 (13%), Asian 7(18%) |
| Comorbidities and Risk factors |
| Diabetes mellitus: 7 (18%) Human Immunodeficiency Virus: 4 (10%) Cancer: 2 (5%) Smoking: 12 (32%) Alcohol abuse: 7 (18%) Substance abuse: 7 (18%) Outdoor occupational exposure: 18 (48%) |
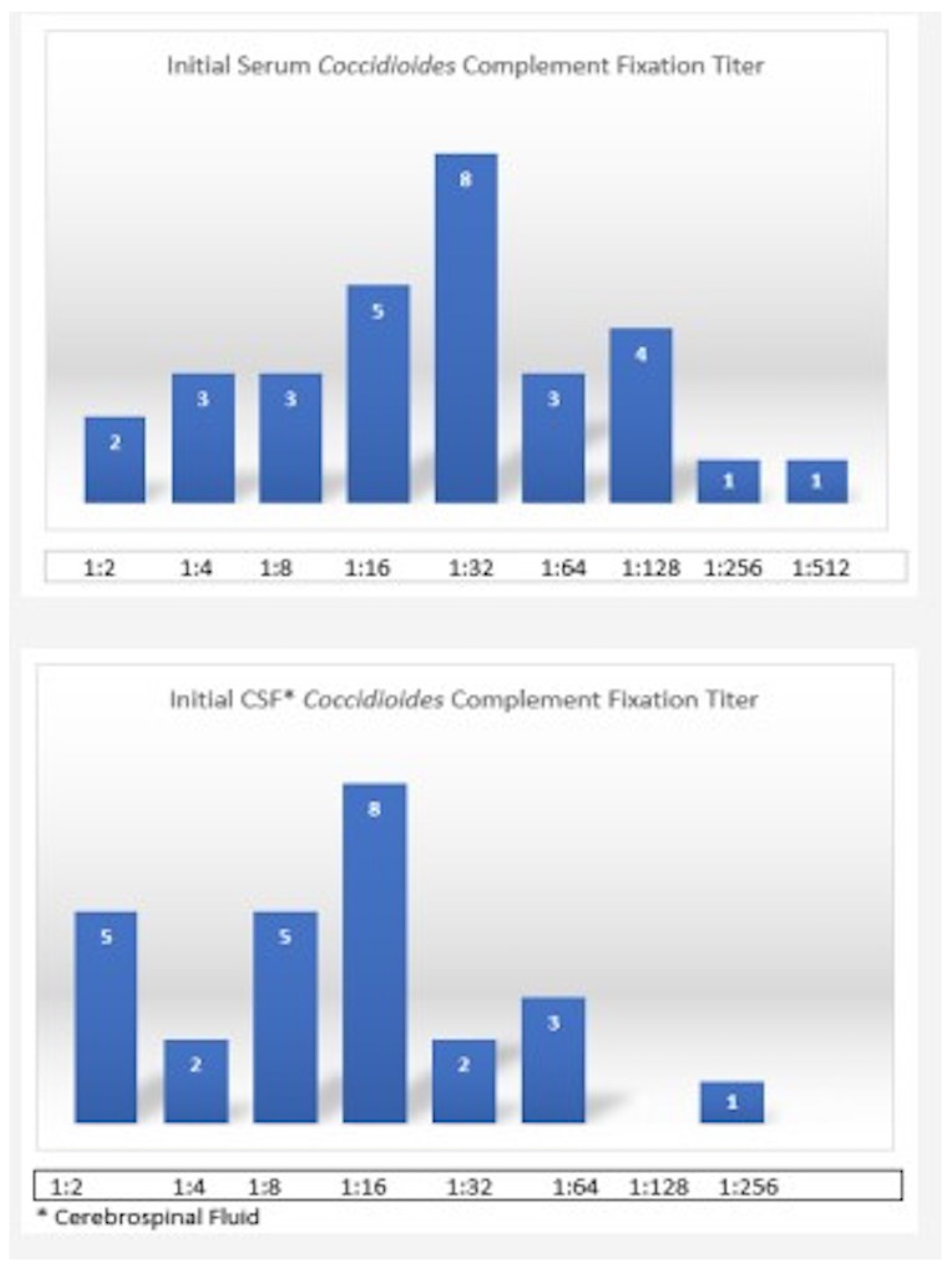
| Serology |
| Initial serum coccidioidomycosis complement fixation titer ≥ 1:32 in 57% Initial CSF *** coccidioidomycosis complement fixation titer ≥ 1:16 in 53% patients |
| Brain Imaging Findings |
| Hydrocephalus: 22 (59%) Diffuse leptomeningeal enhancement: 19 (51%) Stroke: 4 (10%) Normal: 7 (18%) |
| Characteristics | N (%) |
|---|---|
| Antifungal therapy | |
| Agent used for initial management of CM | Fluconazole: 33 (89%) Amphotericin 3 (8%) |
| Fluconazole dose | 400 mg: 2 (6%) 600 mg: 3 (9%) 800 mg: 20 (60%) 1000 mg 6 (18%) 1200 mg 2 (6%) |
| Years on treatment (median with IQR **) | 6 [3, 10] |
| Medication non-adherence to fluconazole | 17/33 (51%) |
| Serologic failure | 19/37 (51%) |
| Intra cranial Pressure Management | |
| VP *** shunt | 27 (72%) |
| Shunt failure and shunt revision | 17/27 (62%) |
| Number of Shunt revisions (range) | 1–6 |
| Follow-up | |
| Duration of follow up in months (median with IQR) | 48 [24, 84] |
| Lost to follow-up | 18 (48%) |
| Death | 6 (16%) |
| CSF Findings | Negative (20) | Positive (17) | p Value | |
|---|---|---|---|---|
| Arachnoiditis/Syringomyelia | N (%) | N (%) | ||
| CSF lymphocytic pleocytosis | 0.489 | |||
| No | 2 (10.0) | 0 (0) | ||
| Yes | 18 (90) | 17 (100.0) | ||
| CSF Eosinophilia | 0.384 | |||
| No | 15 (75.00 | 12 (70.6) | ||
| Yes | 3 (15.0) | 5 (29.4) | ||
| CSF culture Positive | 0.097 | |||
| No | 14 (70.0) | 16 (94.1) | ||
| Yes | 16 (30.0) | 1 (5.9) | ||
| CSF Cocci IgG Positive | 0.999 | |||
| Yes | 19 (95.0) | 16 (94.1) | ||
| CSF Cocci IgM Positive | 0.981 | |||
| No | 9 (45.0) | 8 (47.1) | ||
| Yes | 10 (50.0) | 8 (47.1) | ||
| CSF Cocci PCR Positive | 0.333 | |||
| No | 8 (40.0) | 6 (35.3) | ||
| Yes | 9 (45.0) | 5 (29.4) | ||
| CSF opening pressure, M (SD) ** | 21.3 (9.9) | 34.2 (17.5) | 0.034 | |
| CSF WBC, M (SD) | 1145.1 (3366.7) | 505.3 (388.3) | 0.442 | |
| CSF protein, M (SD) | 255.6 (199.5) | 877.9 (1225.6) | 0.036 | |
| CSF glucose, M (SD) | 40.3 (19.6) | 27.7 (22.9) | 0.084 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sivasubramanian, G.; Kadakia, S.; Kim, J.M.; Pervaiz, S.; Yan, Y.; Libke, R. Spinal Arachnoiditis in Patients with Coccidioidomycosis Meningitis—Analysis of Clinical and Imaging Features. J. Fungi 2022, 8, 1180. https://doi.org/10.3390/jof8111180
Sivasubramanian G, Kadakia S, Kim JM, Pervaiz S, Yan Y, Libke R. Spinal Arachnoiditis in Patients with Coccidioidomycosis Meningitis—Analysis of Clinical and Imaging Features. Journal of Fungi. 2022; 8(11):1180. https://doi.org/10.3390/jof8111180
Chicago/Turabian StyleSivasubramanian, Geetha, Saurin Kadakia, Jani M. Kim, Sarah Pervaiz, Yueqi Yan, and Robert Libke. 2022. "Spinal Arachnoiditis in Patients with Coccidioidomycosis Meningitis—Analysis of Clinical and Imaging Features" Journal of Fungi 8, no. 11: 1180. https://doi.org/10.3390/jof8111180