
Pulmonary Cryptococcosis
 , , ,
, , ,
Abstract
:1. Introduction
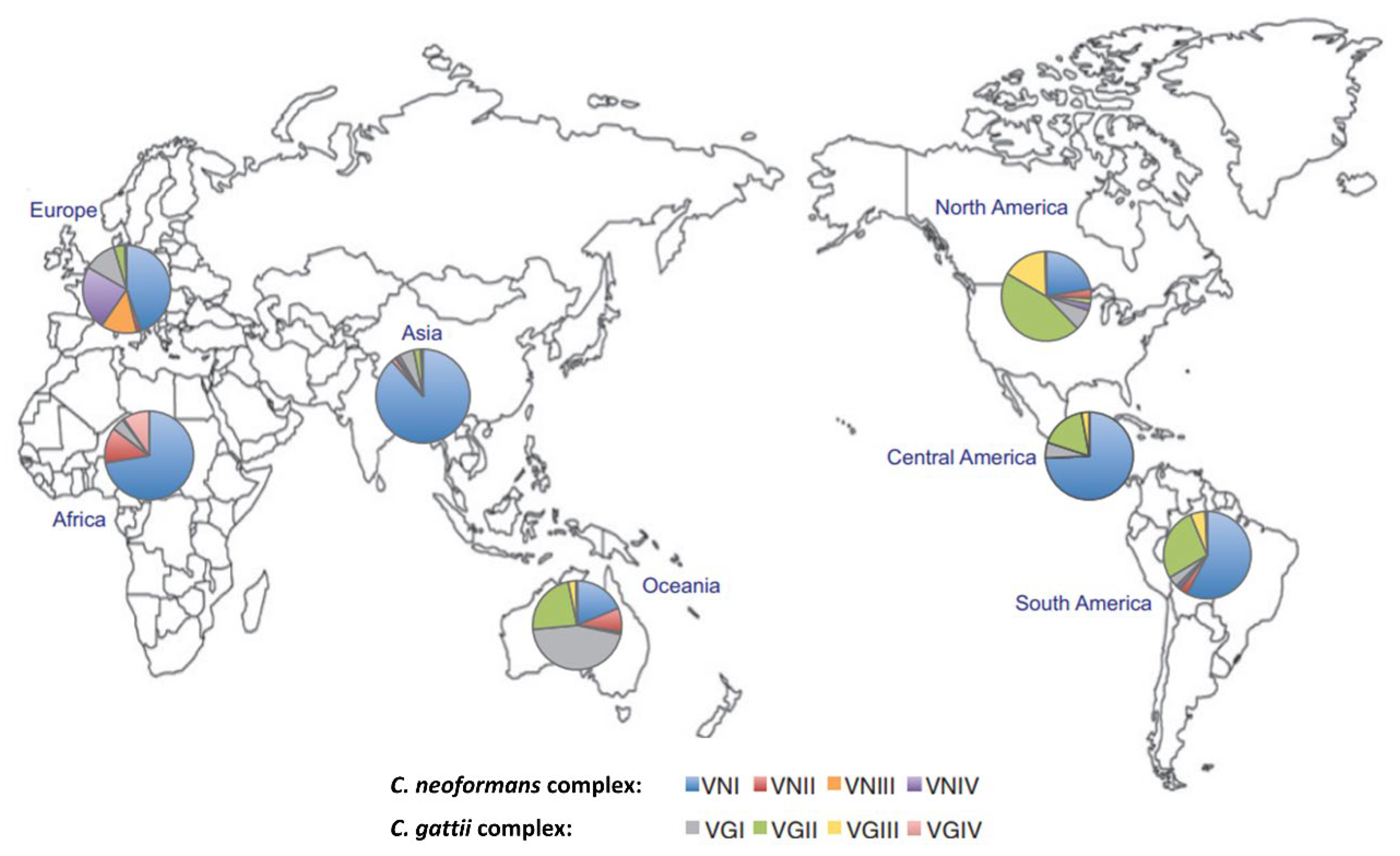
2. Epidemiology and Host Risk Factors


{kind=link}
{kind=link}
| Species Complex and Historical Variants | Genotype (Molecular Subtype) | Historical Serotype | Proposed Species Name [18] |
|---|---|---|---|
| C. neoformans complex | |||
| C. neoformans var. grubii | VNI, VNII, VNBI, VNBII and VNIII | A | C. neoformans |
| C. neoformans var. neoformans | VNIV | D | C. deneoformans |
| C. neoformans hybrid * | VNIII | AD hybrid | C. neoformans × C. deneoformans hybrid |
| C. gattii complex | |||
| C. gattii | VGI VGII, VGIIa, VGIIb, VGIIc VGIII VGIV VGV VGVI | B B C B and C B B | C. gattii C. deuterogattii C. bacillisporus C. tetragattii - † C. decagattii |
3. Clinical Manifestations
Comparison of C. gattii with C. neoformans Infection
4. Diagnosis
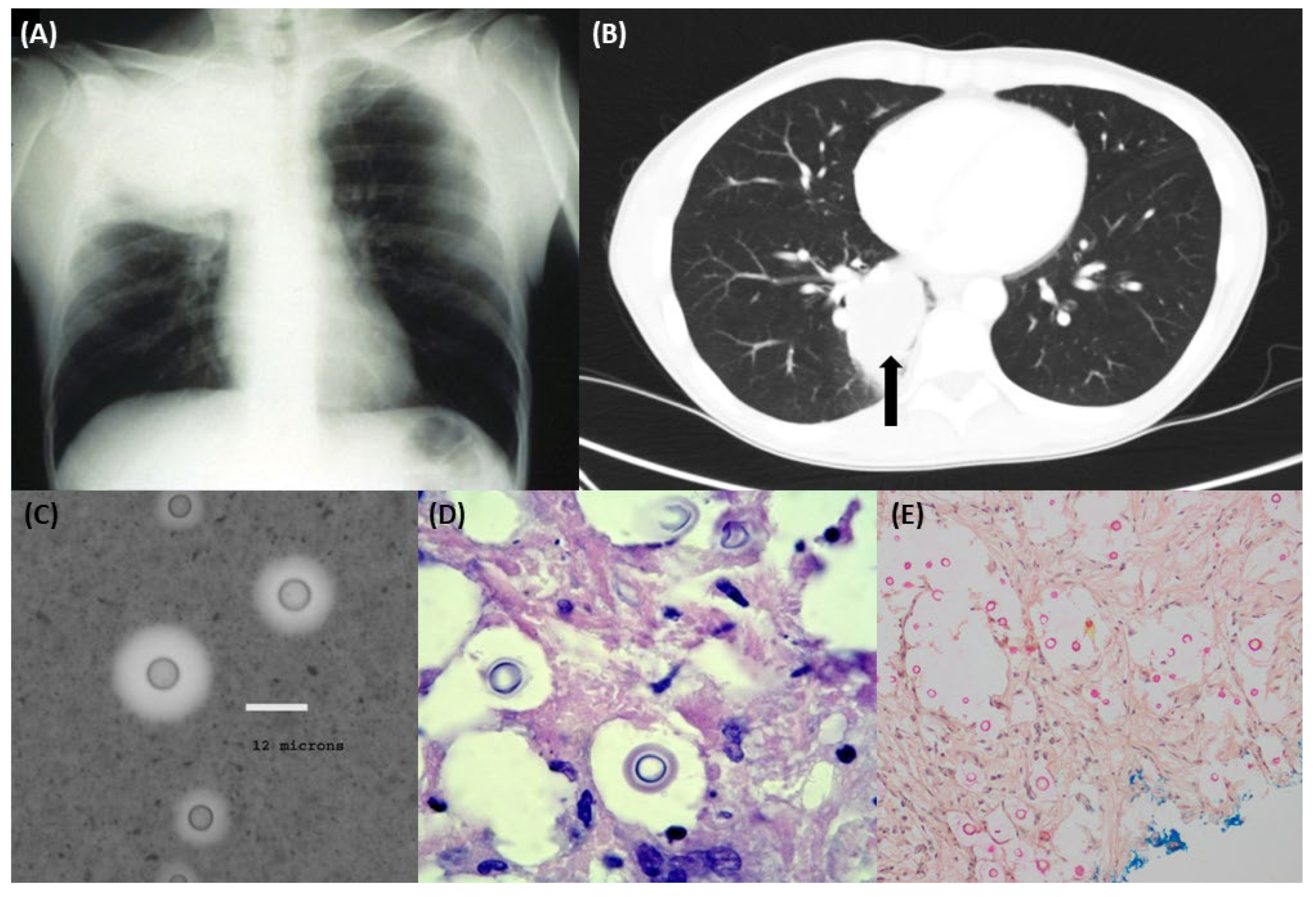
4.1. Radiology
4.2. Cryptococcal Antigen Testing
4.3. Microscopy
4.4. Histopathology
4.5. Culture and Susceptibility Testing
4.6. Nucleic Acid Amplification Testing
5. Treatment of Pulmonary Cryptococcosis
| Host Risk Group/Severity of Disease | First Line Antifungal Therapy | Alternative Antifungal Regimen | Duration of Therapy/Comments |
|---|---|---|---|
Immunocompetent
| Fluconazole 400–800 mg orally, daily | Itraconazole (loading doses of 200 mg orally three times daily for three days, then 200 mg orally twice daily) Voriconazole (loading doses of 6 mg/kg intravenously twice daily or 400 mg orally twice daily on the first day, then 200 mg orally twice daily) Posaconazole delayed-release tablets (loading doses of 300 mg orally twice daily on the first day, then 300 mg orally once daily) | 6 to 12 months |
| Induction: Liposomal amphotericin 3 mg/kg/day intravenously (or conventional amphotericin 0.7–1.0 mg/kg/day) plus flucytosine 100 mg/kg/day orally Consolidation: Fluconazole 400–800 mg orally, daily Maintenance: Fluconazole 200-400 mg orally, daily | Induction: 2–4 weeks Consolidation: 8 weeks Maintenance: 12 months | |
Immunocompromised—HIV and non-HIV
| Fluconazole 400 mg orally, daily | Itraconazole (loading doses of 200 mg orally three times daily for three days, then 200 mg orally twice daily) Voriconazole (loading doses of 6 mg/kg intravenously twice daily or 400 mg orally twice daily on the first day, then 200 mg orally twice daily) Posaconazole delayed-release tablets (loading doses of 300 mg orally twice daily on the first day, then 300 mg orally once daily) | 6 to 12 months In patients with HIV coinfection, suppressive therapy (fluconazole 200 mg orally, daily) should be given after the acute treatment course. This may be ceased after 12 months if CD4 count > 100 cells/μL, HIV viral load is undetectable and cryptococcal antigen titre is stable at <1:512. |
| Treat as for immunocompetent, severe disease | ||
Pregnant women
| “Watch and wait”, close clinical monitoring | Seek expert opinion Consider amphotericin in 1st trimester; fluconazole 400 mg orally, daily in 2nd and 3rd trimester if required | Recommended to defer treatment until after delivery unless severe disease |
| Treat as for immunocompetent, severe disease with expert input | ||
Children
| Fluconazole 6–12 mg/kg orally, daily | Treat as for children, severe disease | 6 to 12 months |
| Induction: Amphotericin B 1 mg/kg per day intravenously plus flucytosine 100 mg/kg per day orally (in 4 divided doses) Consolidation: fluconazole 10–12 mg/kg per day orally Maintenance: fluconazole 6–12 mg/kg per day orally | Liposomal Amphotericin B 5 mg/kg per day intravenously (or Amphotericin B lipid complex 5 mg/kg per day intravenously) | Induction: 2 weeks Consolidation: 8 weeks Maintenance: 6 to 12 months |
5.1. Special Populations
5.1.1. HIV
5.1.2. Immunocompromised Non-HIV
5.1.3. Pregnancy
5.1.4. Children
6. Prognosis
7. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
Abbreviations
| AIDS | acquired immunodeficiency syndrome |
| AST | American Society of Transplantation |
| BALF | bronchoalveolar lavage fluid |
| CLSI | Clinical & Laboratory Standards Institute |
| CNS | central nervous system |
| CSF | cerebrospinal fluid |
| CrAg | Cryptococcal antigen |
| DNA | deoxyribonucleic acid |
| ECV | epidemiological cutoff value |
| EUCAST | European Committee on Antimicrobial Susceptibility Testing |
| GM-CSF | granulocyte-macrophage-colony stimulating factor |
| HIV | human immunodeficiency virus |
| IDSA | Infectious Diseases Society of America |
| IRIS | immune reconstitution inflammatory syndrome |
| MALDI-TOF | matrix-assisted laser desorption ionisation-time of flight |
| MIC | minimum inhibitory concentration |
| NAAT | nucleic acid amplification testing |
| PJP | Pneumocystis jirovecii pneumonia |
| TB | tuberculosis |
References
- Maziarz, E.K.; Perfect, J.R. Cryptococcosis. Infect. Dis. Clin. N. Am. 2016, 30, 179–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suwatanapongched, T.; Sangsatra, W.; Boonsarngsuk, V.; Watcharananan, S.P.; Incharoen, P. Clinical and radiologic manifestations of pulmonary cryptococcosis in immunocompetent patients and their outcomes after treatment. Diagn. Interv. Radiol. 2013, 19, 438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baddley, J.W.; Chen, S.C.; Huisingh, C.; Benedict, K.; DeBess, E.E.; Galanis, E.; Jackson, B.R.; MacDougall, L.; Marsden-Haug, N.; Oltean, H.; et al. MSG07: An International Cohort Study Comparing Epidemiology and Outcomes of Patients with Cryptococcus neoformans or Cryptococcus gattii Infections. Clin. Infect. Dis. 2021, 73, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Sorrell, T.; Nimmo, G.; Speed, B.; Currie, B.; Ellis, D.; Marriott, D.; Pfeiffer, T.; Parret, D.; Byth, K.; et al. Epidemiology and host- and variety-dependent characteristics of infection due to Cryptococcus neoformans in Australia and New Zealand. Australasian Cryptococcal Study Group. Clin. Infect. Dis. 2000, 31, 499–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.C.; Sorrell, T.C.; Chen, S.C. Pulmonary Cryptococcosis. Semin. Respir. Crit. Care Med. 2015, 36, 681–691. [Google Scholar] [CrossRef]
- Danesi, P.; Falcaro, C.; Schmertmann, L.J.; de Miranda, L.H.M.; Krockenberger, M.; Malik, R. Cryptococcus in Wildlife and Free-Living Mammals. J. Fungi 2021, 7, 29. [Google Scholar] [CrossRef]
- Smith, K.D.; Achan, B.; Hullsiek, K.H.; McDonald, T.R.; Okagaki, L.H.; Alhadab, A.A.; Akampurira, A.; Rhein, J.R.; Meya, D.B.; Boulware, D.R.; et al. Increased Antifungal Drug Resistance in Clinical Isolates of Cryptococcus neoformans in Uganda. Antimicrob. Agents Chemother. 2015, 59, 7197–7204. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.C.; Hall, V.; Cooper, C.; Grigoriadis, G.; Beardsley, J.; Sorrell, T.C.; Heath, C.H.; Slavin, M.A.; Thursky, K.A.; Roberts, J.A.; et al. Consensus guidelines for the diagnosis and management of cryptococcosis and rare yeast infections in the haematology/oncology setting, 2021. Intern. Med. J. 2021, 51 (Suppl. S7), 118–142. [Google Scholar] [CrossRef]
- Perfect, J.R.; Dismukes, W.E.; Dromer, F.; Goldman, D.L.; Graybill, J.R.; Hamill, R.J.; Harrison, T.S.; Larsen, R.A.; Lortholary, O.; Nguyen, M.-H.; et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of America. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2010, 50, 291–322. [Google Scholar] [CrossRef] [Green Version]
- Brizendine, K.D.; Baddley, J.W.; Pappas, P.G. Pulmonary Cryptococcosis. Semin. Respir. Crit. Care Med. 2011, 32, 727–734. [Google Scholar] [CrossRef]
- Setianingrum, F.; Rautemaa-Richardson, R.; Denning, D.W. Pulmonary cryptococcosis: A review of pathobiology and clinical aspects. Med. Mycol. 2019, 57, 133–150. [Google Scholar] [CrossRef]
- Baddley, J.W.; Schain, D.C.; Gupte, A.A.; Lodhi, S.A.; Kayler, L.K.; Frade, J.P.; Lockhart, S.R.; Chiller, T.; Bynon, J.S.; Bower, W.A. Transmission of Cryptococcus neoformans by Organ Transplantation. Clin. Infect. Dis. 2011, 52, e94–e98. [Google Scholar] [CrossRef] [Green Version]
- Grimshaw, A.; Palasanthiran, P.; Huynh, J.; Marais, B.; Chen, S.; McMullan, B. Cryptococcal infections in children: Retrospective study and review from Australia. Future Microbiol. 2019, 14, 1531–1544. [Google Scholar] [CrossRef]
- Emmons, C.W. Saprophytic sources of Cryptococcus neoformans associated with the pigeon (Columba livia). Am. J. Hyg. 1955, 62, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Lazéra, M.S.; Pires, F.D.; Camillo-Coura, L.; Nishikawa, M.M.; Bezerra, C.C.; Trilles, L.; Wanke, B. Natural habitat of Cryptococcus neoformans var. neoformans in decaying wood forming hollows in living trees. J. Med. Vet. Mycol. 1996, 34, 127–131. [Google Scholar] [CrossRef] [Green Version]
- Callejas, A.; Ordoñez, N.; Rodriguez, M.C.; Castañeda, E. First isolation of Cryptococcus neoformans var. gattii, serotype C, from the environment in Colombia. Med. Mycol. 1998, 36, 341–344. [Google Scholar] [CrossRef] [Green Version]
- Springer, D.J.; Chaturvedi, V. Projecting global occurrence of Cryptococcus gattii. Emerg. Infect. Dis. 2010, 16, 14–20. [Google Scholar] [CrossRef]
- Hagen, F.; Khayhan, K.; Theelen, B.; Kolecka, A.; Polacheck, I.; Sionov, E.; Falk, R.; Parnmen, S.; Lumbsch, H.T.; Boekhout, T. Recognition of seven species in the Cryptococcus gattii/Cryptococcus neoformans species complex. Fungal Genet. Biol. FGB 2015, 78, 16–48. [Google Scholar] [CrossRef] [Green Version]
- Kwon-Chung, K.J.; Bennett, J.E.; Wickes, B.L.; Meyer, W.; Cuomo, C.A.; Wollenburg, K.R.; Bicanic, T.A.; Castañeda, E.; Chang, Y.C.; Chen, J.; et al. The Case for Adopting the “Species Complex” Nomenclature for the Etiologic Agents of Cryptococcosis. mSphere 2017, 2, e00357-16. [Google Scholar] [CrossRef] [Green Version]
- Farrer, R.A.; Chang, M.; Davis, M.J.; van Dorp, L.; Yang, D.-H.; Shea, T.; Sewell, T.R.; Meyer, W.; Balloux, F.; Edwards, H.M.; et al. A New Lineage of Cryptococcus gattii (VGV) Discovered in the Central Zambezian Miombo Woodlands. mBio 2019, 10, e02306-19. [Google Scholar] [CrossRef] [PubMed]
- Monroy-Nieto, J.; Bowers, J.R.; Montfort, P.; Adame, G.; Taverna, C.G.; Yaglom, H.; Sykes, J.E.; Brady, S.; Mochon, A.B.; Meyer, W.; et al. Phylogenomic Placement of American Southwest-Associated Clinical and Veterinary Isolates Expands Evidence for Distinct Cryptococcus gattii VGVI. Microorganisms 2022, 10, 1681. [Google Scholar] [CrossRef] [PubMed]
- Cogliati, M.; Barchiesi, F.; Spreghini, E.; Tortorano, A.M. Heterozygosis and Pathogenicity of Cryptococcus neoformans AD-Hybrid Isolates. Mycopathologia 2012, 173, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Litvintseva, A.P.; Lin, X.; Templeton, I.; Heitman, J.; Mitchell, T.G. Many Globally Isolated AD Hybrid Strains of Cryptococcus neoformans Originated in Africa. PLoS Pathog. 2007, 3, e114. [Google Scholar] [CrossRef] [Green Version]
- Desnos-Ollivier, M.; Patel, S.; Raoux-Barbot, D.; Heitman, J.; Dromer, F. Cryptococcosis Serotypes Impact Outcome and Provide Evidence of Cryptococcus neoformans Speciation. mBio 2015, 6, e00311. [Google Scholar] [CrossRef] [Green Version]
- Firacative, C.; Trilles, L.; Meyer, W. Advances in the understanding of the Cryptococcus neoformans and C. gattii species complexes and cryptococcosis. Microbiol. Aust. 2017, 38, 106–111. [Google Scholar] [CrossRef] [Green Version]
- Mirza, S.A.; Phelan, M.; Rimland, D.; Graviss, E.; Hamill, R.; Brandt, M.E.; Gardner, T.; Sattah, M.; de Leon, G.P.; Baughman, W.; et al. The changing epidemiology of cryptococcosis: An update from population-based active surveillance in 2 large metropolitan areas, 1992–2000. Clin. Infect. Dis. 2003, 36, 789–794. [Google Scholar] [CrossRef]
- Tardieu, L.; Divard, G.; Lortholary, O.; Scemla, A.; Rondeau, É.; Accoceberry, I.; Agbonon, R.; Alanio, A.; Angoulvant, A.; Albano, L.; et al. Cryptococcal Meningitis in Kidney Transplant Recipients: A Two-Decade Cohort Study in France. Pathogens 2022, 11, 699. [Google Scholar] [CrossRef]
- Lin, Y.Y.; Shiau, S.; Fang, C.T. Risk factors for invasive Cryptococcus neoformans diseases: A case-control study. PLoS ONE 2015, 10, e0119090. [Google Scholar] [CrossRef] [Green Version]
- Yang, D.-H.; England, M.R.; Salvator, H.; Anjum, S.; Park, Y.-D.; Marr, K.A.; Chu, L.A.; Govender, N.P.; Lockhart, S.R.; Desnos-Ollivier, M.; et al. Cryptococcus gattii Species Complex as an Opportunistic Pathogen: Underlying Medical Conditions Associated with the Infection. mBio 2021, 12, e0270821. [Google Scholar] [CrossRef]
- Lin, C.; Yang, T.Y.; Chan, M.C.; Hsu, K.H.; Huang, Y.H.; Tseng, J.S. Comprehensive Analysis and Risk Identification of Pulmonary Cryptococcosis in Non-HIV Patients. J. Fungi 2021, 7, 657. [Google Scholar] [CrossRef]
- Tashiro, H.; Haraguchi, T.; Takahashi, K.; Sadamatsu, H.; Tajiri, R.; Takamori, A.; Kimura, S.; Sueoka-Aragane, N. Clinical impact of advanced chronic kidney disease in patients with non-HIV pulmonary cryptococcosis. BMC Pulm. Med. 2020, 20, 116. [Google Scholar] [CrossRef]
- Speed, B.; Dunt, D. Clinical and host differences between infections with the two varieties of Cryptococcus neoformans. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 1995, 21, 28–34. [Google Scholar] [CrossRef]
- Mitchell, D.H.; Sorrell, T.C. Pancoast’s syndrome due to pulmonary infection with Cryptococcus neoformans variety gattii. Clin. Infect. Dis. 1992, 14, 1142–1144. [Google Scholar] [CrossRef]
- Kohno, S.; Kakeya, H.; Izumikawa, K.; Miyazaki, T.; Yamamoto, Y.; Yanagihara, K.; Mitsutake, K.; Miyazaki, Y.; Maesaki, S.; Yasuoka, A.; et al. Clinical features of pulmonary cryptococcosis in non-HIV patients in Japan. J. Infect. Chemother. Off. J. Jpn. Soc. Chemother. 2015, 21, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Song, K.D.; Lee, K.S.; Chung, M.P.; Kwon, O.J.; Kim, T.S.; A Yi, C.; Chung, M.J. Pulmonary cryptococcosis: Imaging findings in 23 non-AIDS patients. Korean J. Radiol. 2010, 11, 407–416. [Google Scholar] [CrossRef] [Green Version]
- Ye, F.; Xie, J.X.; Zeng, Q.S.; Chen, G.Q.; Zhong, S.Q.; Zhong, N.S. Retrospective analysis of 76 immunocompetent patients with primary pulmonary cryptococcosis. Lung 2012, 190, 339–346. [Google Scholar] [CrossRef]
- Visnegarwala, F.; Graviss, E.A.; Lacke, C.E.; Dural, A.T.; Johnson, P.C.; Atmar, R.L.; Hamill, R.J. Acute respiratory failure associated with cryptococcosis in patients with AIDS: Analysis of predictive factors. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 1998, 27, 1231–1237. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, E.P.; Inácio, C.P.; de Freitas, J.F.; Valeriano, C.A.T.; Neves, R.P.; Sobrinho, P.M.; Lima-Neto, R.G. Tuberculosis and neurocryptococcosis by Cryptococcus neoformans molecular type VNI in A non-HIV patient: A comorbidities case report. J. Mycol. Med. 2022, 32, 101213. [Google Scholar] [CrossRef]
- Limper, A.H.; Knox, K.S.; Sarosi, G.A.; Ampel, N.M.; Bennett, J.E.; Catanzaro, A.; Davies, S.F.; Dismukes, W.E.; Hage, C.A.; Marr, K.A.; et al. An official American Thoracic Society statement: Treatment of fungal infections in adult pulmonary and critical care patients. Am. J. Respir. Crit. Care Med. 2011, 183, 96–128. [Google Scholar] [CrossRef] [Green Version]
- Temfack, E.; Bigna, J.J.; Luma, H.N.; Spijker, R.; Meintjes, G.; Jarvis, J.N.; Dromer, F.; Harrison, T.; Cohen, J.F.; Lortholary, O. Impact of Routine Cryptococcal Antigen Screening and Targeted Preemptive Fluconazole Therapy in Antiretroviral-naive Human Immunodeficiency Virus-infected Adults with CD4 Cell Counts < 100/μL: A Systematic Review and Meta-analysis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2019, 68, 688–698. [Google Scholar] [CrossRef]
- Kuo, C.Y.; Wang, S.Y.; Shih, H.P.; Tu, K.H.; Huang, W.C.; Ding, J.Y.; Lin, C.H.; Yeh, C.F.; Ho, M.W.; Chang, S.C.; et al. Disseminated Cryptococcosis Due to Anti-Granulocyte-Macrophage Colony-Stimulating Factor Autoantibodies in the Absence of Pulmonary Alveolar Proteinosis. J. Clin. Immunol. 2017, 37, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.-A.; Slavin, M.A.; Heath, C.H.; Playford, E.G.; Byth, K.; Marriott, D.; Kidd, S.E.; Bak, N.; Currie, B.; Hajkowicz, K.; et al. Clinical manifestations of Cryptococcus gattii infection: Determinants of neurological sequelae and death. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2012, 55, 789–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurenson, I.F.; Trevett, A.J.; Lalloo, D.G.; Nwokolo, N.; Naraqi, S.; Black, J.; Tefurani, N.; Saweri, A.; Mavo, B.; Igo, J.; et al. Meningitis caused by Cryptococcus neoformans var. gattii and var. neoformans in Papua New Guinea. Trans. R. Soc. Trop. Med. Hyg. 1996, 90, 57–60. [Google Scholar] [CrossRef]
- Mitchell, D.H.; Sorrell, T.; Allworth, A.M.; Heath, C.H.; McGregor, A.R.; Papanaoum, K.; Richards, M.; Gottlieb, T. Cryptococcal disease of the CNS in immunocompetent hosts: Influence of cryptococcal variety on clinical manifestations and outcome. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 1995, 20, 611–616. [Google Scholar] [CrossRef]
- McMullan, B.J.; Sorrell, T.C.; Chen, S.C. Cryptococcus gattii infections: Contemporary aspects of epidemiology, clinical manifestations and management of infection. Future Microbiol. 2013, 8, 1613–1631. [Google Scholar] [CrossRef]
- Chau, T.T.; Mai, N.H.; Phu, N.H.; Nghia, H.D.; Chuong, L.V.; Sinh, D.X.; Duong, V.A.; Diep, P.T.; Campbell, J.I.; Baker, S.; et al. A prospective descriptive study of cryptococcal meningitis in HIV uninfected patients in Vietnam—High prevalence of Cryptococcus neoformans var grubii in the absence of underlying disease. BMC Infect. Dis. 2010, 10, 199. [Google Scholar] [CrossRef] [Green Version]
- Chastain, D.B.; Rao, A.; Yaseyyedi, A.; Henao-Martínez, A.F.; Borges, T.; Franco-Paredes, C. Cerebral Cryptococcomas: A Systematic Scoping Review of Available Evidence to Facilitate Diagnosis and Treatment. Pathogens 2022, 11, 205. [Google Scholar] [CrossRef]
- Chen, S.C.; Korman, T.M.; Slavin, M.A.; Marriott, D.; Byth, K.; Bak, N.; Currie, B.J.; Hajkowicz, K.; Heath, C.H.; Kidd, S.; et al. Antifungal therapy and management of complications of cryptococcosis due to Cryptococcus gattii. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2013, 57, 543–551. [Google Scholar] [CrossRef] [Green Version]
- Saijo, T.; Chen, J.; Chen, S.C.; Rosen, L.B.; Yi, J.; Sorrell, T.C.; Bennett, J.E.; Holland, S.M.; Browne, S.K.; Kwon-Chung, K.J. Anti-granulocyte-macrophage colony-stimulating factor autoantibodies are a risk factor for central nervous system infection by Cryptococcus gattii in otherwise immunocompetent patients. mBio 2014, 5, e00912-14. [Google Scholar] [CrossRef] [Green Version]
- Stevenson, B.; Bundell, C.; Mulrennan, S.; McLean-Tooke, A.; Murray, R.; Brusch, A. The significance of anti-granulocyte-macrophage colony-stimulating factor antibodies in cryptococcal infection: Case series and review of antibody testing. Intern. Med. J. 2019, 49, 1446–1450. [Google Scholar] [CrossRef]
- Jarvis, J.N.; Lawn, S.D.; Vogt, M.; Bangani, N.; Wood, R.; Harrison, T.S. Screening for cryptococcal antigenemia in patients accessing an antiretroviral treatment program in South Africa. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2009, 48, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Kabanda, T.; Siedner, M.J.; Klausner, J.D.; Muzoora, C.; Boulware, D.R. Point-of-care diagnosis and prognostication of cryptococcal meningitis with the cryptococcal antigen lateral flow assay on cerebrospinal fluid. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2014, 58, 113–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vijayan, T.; Chiller, T.; Klausner, J.D. Sensitivity and specificity of a new cryptococcal antigen lateral flow assay in serum and cerebrospinal fluid. MLO Med. Lab. Obs. 2013, 45, 16. [Google Scholar]
- Goldman, D.L.; Khine, H.; Abadi, J.; Lindenberg, D.J.; Pirofski, L.-A.; Niang, R.; Casadevall, A. Serologic evidence for Cryptococcus neoformans infection in early childhood. Pediatrics 2001, 107, e66. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Li, N.; Li, H.; Chen, X.; Wang, S.; Zhang, X.; Zhang, R.; Xu, J.; Shi, J.; Yung, R.C.; et al. Clinical analysis of 76 patients pathologically diagnosed with pulmonary cryptococcosis. Eur. Respir. J. 2012, 40, 1191. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.C.; Sorrell, T.C.; Chang, C.C.; Paige, E.K.; Bryant, P.A.; Slavin, M.A. Consensus guidelines for the treatment of yeast infections in the haematology, oncology and intensive care setting, 2014. Intern. Med. J. 2014, 44, 1315–1332. [Google Scholar] [CrossRef]
- Kishi, K.; Homma, S.; Kurosaki, A.; Kohno, T.; Motoi, N.; Yoshimura, K. Clinical features and high-resolution CT findings of pulmonary cryptococcosis in non-AIDS patients. Respir. Med. 2006, 100, 807–812. [Google Scholar] [CrossRef] [Green Version]
- Lindsley, M.D.; Mekha, N.; Baggett, H.C.; Surinthong, Y.; Autthateinchai, R.; Sawatwong, P.; Harris, J.R.; Park, B.J.; Chiller, T.; Balajee, S.A.; et al. Evaluation of a newly developed lateral flow immunoassay for the diagnosis of cryptococcosis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2011, 53, 321–325. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Wang, M.; Zeng, P.; Chen, Z.; Zhan, Y.; Li, S.; Lin, Y.; Cheng, J.; Ye, F. Examination of a Chinese-made cryptococcal glucuronoxylomannan antigen test in serum and bronchoalveolar lavage fluid for diagnosing pulmonary cryptococcosis in HIV-negative patients. J. Microbiol. Immunol. Infect. 2022, 55, 307–313. [Google Scholar] [CrossRef]
- Lee, G.H.; Arthur, I.; Leung, M. False-Negative Serum Cryptococcal Lateral Flow Assay Result Due to the Prozone Phenomenon. J. Clin. Microbiol. 2018, 56, e01878-17. [Google Scholar] [CrossRef] [Green Version]
- Gassiep, I.; Aye, C.; Armstrong, M.; Emeto, T.I.; Heather, C.S.; Norton, R.E. Correlation between serum cryptococcal antigen titre and meningitis in immunocompetent patients. J. Med. Microbiol. 2018, 67, 1515–1518. [Google Scholar] [CrossRef] [PubMed]
- Gassiep, I.; McDougall, D.; Douglas, J.; Francis, R.; Playford, E.G. Cryptococcal infections in solid organ transplant recipients over a 15-year period at a state transplant center. Transpl. Infect. Dis. 2017, 19, e12639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banshodani, M.; Marubayashi, S.; Shintaku, S.; Moriishi, M.; Tsuchiya, S.; Ohdan, H.; Kawanishi, H. Isolated Pulmonary Cryptococcosis Confused with Lung Tumor 5 Years After Kidney Transplantation: A Case Report. Transplant. Proc. 2019, 51, 561–564. [Google Scholar] [CrossRef]
- Zaragoza, O.; Rodrigues, M.L.; De Jesus, M.; Frases, S.; Dadachova, E.; Casadevall, A. The capsule of the fungal pathogen Cryptococcus neoformans. Adv. Appl. Microbiol. 2009, 68, 133–216. [Google Scholar]
- Coovadia, Y.M.C.; Mahomed, S.; Dorasamy, A.; Chang, C. A comparative evaluation of the Gram stain and India ink stain for the rapid diagnosis of cryptococcal meningitis in HIV infected patients in Durban. S. Afr. J. Infect. Dis. 2015, 30, 61–63. [Google Scholar] [CrossRef]
- Dewar, G.J.; Kelly, J.K. Cryptococcus gattii: An emerging cause of pulmonary nodules. Can. Respir. J. 2008, 15, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Lazcano, O.; Speights, V.O., Jr.; Bilbao, J.; Becker, J.; Diaz, J. Combined Fontana-Masson-mucin staining of Cryptococcus neoformans. Arch. Pathol. Lab. Med. 1991, 115, 1145–1149. [Google Scholar]
- Perfect, J.R. Cryptococcus neoformans: The yeast that likes it hot. FEMS Yeast Res. 2006, 6, 463–468. [Google Scholar] [CrossRef] [Green Version]
- Randhawa, H.S.; Staib, F.; Blisse, A. Observations on the occurrence of Cryptococcus neoformans in an aviary, using niger-seed creatinine agar and membrane-filtration technique. Zent. Bakteriol. Parasitenkd. Infekt. Hyg. Zweite Nat. Allg. Landwirtsch. Tech. Mikrobiol. 1973, 128, 795–799. [Google Scholar] [CrossRef]
- Firacative, C.; Trilles, L.; Meyer, W. MALDI-TOF MS enables the rapid identification of the major molecular types within the Cryptococcus neoformans/C. gattii species complex. PLoS ONE 2012, 7, e37566. [Google Scholar] [CrossRef] [Green Version]
- McTaggart, L.R.; Lei, E.; Richardson, S.E.; Hoang, L.; Fothergill, A.; Zhang, S.X. Rapid identification of Cryptococcus neoformans and Cryptococcus gattii by matrix-assisted laser desorption ionization-time of flight mass spectrometry. J. Clin. Microbiol. 2011, 49, 3050–3053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Posteraro, B.; Vella, A.; Cogliati, M.; De Carolis, E.; Florio, A.R.; Posteraro, P.; Sanguinetti, M.; Tortorano, A.M. Matrix-assisted laser desorption ionization-time of flight mass spectrometry-based method for discrimination between molecular types of Cryptococcus neoformans and Cryptococcus gattii. J. Clin. Microbiol. 2012, 50, 2472–2476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siqueira, L.P.M.; Gimenes, V.M.F.; de Freitas, R.S.; Melhem, M.S.C.; Bonfietti, L.X.; da Silva, A.R., Jr.; Souza Santos, L.B.; Motta, A.L.; Rossi, F.; Benard, G.; et al. Evaluation of Vitek MS for Differentiation of Cryptococcus neoformans and Cryptococcus gattii Genotypes. J. Clin. Microbiol. 2019, 57, e01282-18. [Google Scholar] [CrossRef]
- Sidrim, J.J.C.; Costa, A.K.F.; Cordeiro, R.A.; Brilhante, R.S.N.; Moura, F.E.A.; Castelo-Branco, D.S.C.M.; Neto, M.P.D.A.; Rocha, M.F.G. Molecular methods for the diagnosis and characterization of Cryptococcus: A review. Can. J. Microbiol. 2010, 56, 445–458. [Google Scholar] [CrossRef]
- Firacative, C.; Escandón, P. Antifungal susceptibility of clinical Cryptococcus gattii isolates from Colombia varies among molecular types. Med. Mycol. 2021, 59, 1122–1125. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Iqbal, N.; Bolden, C.B.; DeBess, E.E.; Marsden-Haug, N.; Worhle, R.; Thakur, R.; Harris, J.R. Epidemiologic cutoff values for triazole drugs in Cryptococcus gattii: Correlation of molecular type and in vitro susceptibility. Diagn. Microbiol. Infect. Dis. 2012, 73, 144–148. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. M27-A3: Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts, 3rd ed.; Approved Standard; CLSI: Wayne, PA, USA, 2008. [Google Scholar]
- Arendrup, M.C.; Meletiadis, J.; Mouton, J.W.; Lagrou, K.; Hamal, P.; Guinea, J. EUCAST Definitive Document E.DEF 7.3.2: Method for the Determination of Broth Dilution Minimum Inhibitory Concentrations of Antifungal Agents for Yeasts. 2020. Available online: https://www.eucast.org/astoffungi/methodsinantifungalsusceptibilitytesting/susceptibility_testing_of_yeasts (accessed on 1 October 2022).
- Pfaller, M.A.; Castanheira, M.; Diekema, D.J.; Messer, S.A.; Jones, R.N. Wild-type MIC distributions and epidemiologic cutoff values for fluconazole, posaconazole, and voriconazole when testing Cryptococcus neoformans as determined by the CLSI broth microdilution method. Diagn. Microbiol. Infect. Dis. 2011, 71, 252–259. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs for Antifungal Agents, v 10.0. 2020. Available online: https://www.eucast.org/ (accessed on 1 October 2022).
- Clinical and Laboratory Standards Institute. M57S Epidemiological Cutoff Values for Antifungal Susceptibility Testing; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2022; ISBN 978-1-68440-159-8. [Google Scholar]
- Bongomin, F.; Oladele, R.O.; Gago, S.; Moore, C.B.; Richardson, M.D. A systematic review of fluconazole resistance in clinical isolates of Cryptococcus species. Mycoses 2018, 61, 290–297. [Google Scholar] [CrossRef]
- Kelly, S.L.; Lamb, D.C.; Taylor, M.; Corran, A.J.; Baldwin, B.C.; Powderly, W.G. Resistance to amphotericin B associated with defective sterol delta 8-->7 isomerase in a Cryptococcus neoformans strain from an AIDS patient. FEMS Microbiol. Lett. 1994, 122, 39–42. [Google Scholar] [CrossRef]
- Al-Odaini, N.; Li, X.Y.; Li, B.K.; Chen, X.C.; Huang, C.Y.; Lv, C.Y.; Pan, K.S.; Zheng, D.Y.; Zheng, Y.Q.; Liao, W.Q.; et al. In vitro Antifungal Susceptibility Profiles of Cryptococcus neoformans var. grubii and Cryptococcus gattii Clinical Isolates in Guangxi, Southern China. Front. Microbiol. 2021, 12, 708280. [Google Scholar] [CrossRef]
- Espinel-Ingroff, A.; Aller, A.I.; Canton, E.; Castañón-Olivares, L.R.; Chowdhary, A.; Cordoba, S.; Cuenca-Estrella, M.; Fothergill, A.; Fuller, J.; Govender, N.; et al. Cryptococcus neoformans-Cryptococcus gattii species complex: An international study of wild-type susceptibility endpoint distributions and epidemiological cutoff values for fluconazole, itraconazole, posaconazole, and voriconazole. Antimicrob. Agents Chemother. 2012, 56, 5898–5906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morera-López, Y.; Torres-Rodríguez, J.M.; Jiménez-Cabello, T.; Baró-Tomás, T. Cryptococcus gattii: In vitro susceptibility to the new antifungal albaconazole versus fluconazole and voriconazole. Med. Mycol. 2005, 43, 505–510. [Google Scholar] [CrossRef] [Green Version]
- Torres-Rodríguez, J.M.; Alvarado-Ramírez, E.; Murciano, F.; Sellart, M. MICs and minimum fungicidal concentrations of posaconazole, voriconazole and fluconazole for Cryptococcus neoformans and Cryptococcus gattii. J. Antimicrob. Chemother. 2008, 62, 205–206. [Google Scholar] [CrossRef]
- Trilles, L.; Fernández-Torres, B.; Lazéra Mdos, S.; Wanke, B.; Guarro, J. In vitro antifungal susceptibility of Cryptococcus gattii. J. Clin. Microbiol. 2004, 42, 4815–4817. [Google Scholar] [CrossRef] [Green Version]
- Lau, A.; Sorrell, T.C.; Chen, S.; Stanley, K.; Iredell, J.; Halliday, C. Multiplex tandem PCR: A novel platform for rapid detection and identification of fungal pathogens from blood culture specimens. J. Clin. Microbiol. 2008, 46, 3021–3027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, A.; Sorrell, T.C.; Lee, O.; Stanley, K.; Halliday, C. Colony multiplex-tandem PCR for rapid, accurate identification of fungal cultures. J. Clin. Microbiol. 2008, 46, 4058–4060. [Google Scholar] [CrossRef] [Green Version]
- Van, T.T.; Kim, T.H.; Butler-Wu, S.M. Evaluation of the Biofire FilmArray meningitis/encephalitis assay for the detection of Cryptococcus neoformans/gattii. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2020, 26, 1375–1379. [Google Scholar] [CrossRef]
- Lau, A.; Chen, S.; Sorrell, T.; Carter, D.; Malik, R.; Martin, P.; Halliday, C. Development and clinical application of a panfungal PCR assay to detect and identify fungal DNA in tissue specimens. J. Clin. Microbiol. 2007, 45, 380–385. [Google Scholar] [CrossRef] [Green Version]
- Tay, E.; Chen, S.C.; Green, W.; Lopez, R.; Halliday, C.L. Development of a Real-Time PCR Assay to Identify and Distinguish between Cryptococcus neoformans and Cryptococcus gattii Species Complexes. J. Fungi 2022, 8, 462. [Google Scholar] [CrossRef]
- Singh, N.; Forrest, G. Cryptococcosis in solid organ transplant recipients. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2009, 9 (Suppl. S4), S192–S198. [Google Scholar] [CrossRef]
- Baddley, J.W.; Forrest, G.N. Cryptococcosis in solid organ transplantation—Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13543. [Google Scholar] [CrossRef]
- Smith, F.S.; Gibson, P.; Nicholls, T.T.; Simpson, J.A. Pulmonary resection for localized lesions of cryptococcosis (torulosis): A review of eight cases. Thorax 1976, 31, 121–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spec, A.; Olsen, M.A.; Raval, K.; Powderly, W.G. Impact of Infectious Diseases Consultation on Mortality of Cryptococcal infection in Patients without HIV. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2017, 64, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Nadrous, H.F.; Antonios, V.S.; Terrell, C.L.; Ryu, J.H. Pulmonary cryptococcosis in nonimmunocompromised patients. Chest 2003, 124, 2143–2147. [Google Scholar] [CrossRef]
- Fisher, J.F.; Valencia-Rey, P.A.; Davis, W.B. Pulmonary Cryptococcosis in the Immunocompetent Patient-Many Questions, Some Answers. Open Forum Infect. Dis. 2016, 3, ofw167. [Google Scholar] [CrossRef] [Green Version]
- Pappas, P.G.; Perfect, J.R.; Cloud, G.A.; Larsen, R.A.; Pankey, G.A.; Lancaster, D.J.; Henderson, H.; Kauffman, C.A.; Haas, D.W.; Saccente, M.; et al. Cryptococcosis in human immunodeficiency virus-negative patients in the era of effective azole therapy. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2001, 33, 690–699. [Google Scholar] [CrossRef] [Green Version]
- Garrett, L.; Marr, K.; West, S.; Allada, G. 74-year-old man from the pacific northwest with fever and a lung mass. Chest 2011, 140, 814–817. [Google Scholar] [CrossRef]
- Nakao, M.; Fujita, K.; Arakawa, S.; Hayashi, S.; Tomita, S.; Sato, H.; Muramatsu, H. Treatment of Cryptococcus gattii Infection Using Voriconazole. Intern. Med. 2021, 60, 3635–3638. [Google Scholar] [CrossRef]
- Thornton, C.S.; Larios, O.; Grossman, J.; Griener, T.P.; Vaughan, S. Pulmonary Cryptococcus infections as a manifestation of idiopathic CD4 lymphocytopenia: Case report and literature review. BMC Infect. Dis. 2019, 19, 862. [Google Scholar] [CrossRef]
- Wu, H.H.; Chen, Y.X.; Fang, S.Y. Pleural effusion in an immunocompetent host with cryptococcal pneumonia: A case report. World J. Clin. Cases 2020, 8, 1295–1300. [Google Scholar] [CrossRef]
- Linder, K.A.; Gandhi, T.N.; Miceli, M.H. Treatment Failure of Isavuconazole in a Patient with Cryptococcosis. Mycopathologia 2019, 184, 667–670. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., 3rd; Rendon, A.; Ribeiro Dos Santos, R.; Queiroz-Telles, F.; Ostrosky-Zeichner, L.; Azie, N.; Maher, R.; Lee, M.; Kovanda, L.; Engelhardt, M.; et al. Isavuconazole Treatment of Cryptococcosis and Dimorphic Mycoses. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 63, 356–362. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Guidelines for Diagnosing, Preventing and Managing Cryptococcal Disease among Adults, Adolescents and Children Living with HIV; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Jarvis, J.N.; Lawrence, D.S.; Meya, D.B.; Kagimu, E.; Kasibante, J.; Mpoza, E.; Rutakingirwa, M.K.; Ssebambulidde, K.; Tugume, L.; Rhein, J.; et al. Single-Dose Liposomal Amphotericin B Treatment for Cryptococcal Meningitis. N. Engl. J. Med. 2022, 386, 1109–1120. [Google Scholar] [CrossRef]
- Beardsley, J.; Wolbers, M.; Kibengo, F.M.; Ggayi, A.-B.M.; Kamali, A.; Cuc, N.T.K.; Binh, T.Q.; Chau, N.V.V.; Farrar, J.; Merson, L.; et al. Adjunctive Dexamethasone in HIV-Associated Cryptococcal Meningitis. N. Engl. J. Med. 2016, 374, 542–554. [Google Scholar] [CrossRef]
- Seaton, R.A.; Verma, N.; Naraqi, S.; Wembri, J.P.; Warrell, D.A. The effect of corticosteroids on visual loss in Cryptococcus neoformans var. gattii meningitis. Trans. R. Soc. Trop. Med. Hyg. 1997, 91, 50–52. [Google Scholar] [CrossRef]
- Gerlach, E.S.; Altamirano, S.; Yoder, J.M.; Luggya, T.S.; Akampurira, A.; Meya, D.B.; Boulware, D.R.; Rhein, J.; Nielsen, K. ATI-2307 Exhibits Equivalent Antifungal Activity in Cryptococcus neoformans Clinical Isolates with High and Low Fluconazole IC(50). Front. Cell. Infect. Microbiol. 2021, 11, 695240. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Fothergill, A.W.; Iqbal, N.; Bolden, C.B.; Grossman, N.T.; Garvey, E.P.; Brand, S.R.; Hoekstra, W.J.; Schotzinger, R.J.; Ottinger, E.; et al. The Investigational Fungal Cyp51 Inhibitor VT-1129 Demonstrates Potent In vitro Activity against Cryptococcus neoformans and Cryptococcus gattii. Antimicrob. Agents Chemother. 2016, 60, 2528–2531. [Google Scholar] [CrossRef] [Green Version]
- Mitsuyama, J.; Nomura, N.; Hashimoto, K.; Yamada, E.; Nishikawa, H.; Kaeriyama, M.; Kimura, A.; Todo, Y.; Narita, H. In vitro and in vivo antifungal activities of T-2307, a novel arylamidine. Antimicrob. Agents Chemother. 2008, 52, 1318–1324. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, H.; Fukuda, Y.; Mitsuyama, J.; Tashiro, M.; Tanaka, A.; Takazono, T.; Saijo, T.; Yamamoto, K.; Nakamura, S.; Imamura, Y.; et al. In vitro and in vivo antifungal activities of T-2307, a novel arylamidine, against Cryptococcus gattii: An emerging fungal pathogen. J. Antimicrob. Chemother. 2017, 72, 1709–1713. [Google Scholar] [CrossRef] [Green Version]
- Shaw, K.J.; Schell, W.A.; Covel, J.; Duboc, G.; Giamberardino, C.; Kapoor, M.; Moloney, M.; Soltow, Q.A.; Tenor, J.L.; Toffaletti, D.L.; et al. In vitro and In vivo Evaluation of APX001A/APX001 and Other Gwt1 Inhibitors against Cryptococcus. Antimicrob. Agents Chemother. 2018, 62, e00523-18. [Google Scholar] [CrossRef] [Green Version]
- Wiederhold, N.P.; Xu, X.; Wang, A.; Najvar, L.K.; Garvey, E.P.; Ottinger, E.A.; Alimardanov, A.; Cradock, J.; Behnke, M.; Hoekstra, W.J.; et al. In vivo Efficacy of VT-1129 against Experimental Cryptococcal Meningitis with the Use of a Loading Dose-Maintenance Dose Administration Strategy. Antimicrob. Agents Chemother. 2018, 62, e01315-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treviño-Rangel Rde, J.; Villanueva-Lozano, H.; Hernández-Rodríguez, P.; Martínez-Reséndez, M.F.; García-Juárez, J.; Rodríguez-Rocha, H.; González, G.M. Activity of sertraline against Cryptococcus neoformans: In vitro and in vivo assays. Med. Mycol. 2016, 54, 280–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulware, D.R.; Nalintya, E.; Rajasingham, R.; Kirumira, P.; Naluyima, R.; Turya, F.; Namanda, S.; Rutakingirwa, M.K.; Skipper, C.P.; Nikweri, Y.; et al. Adjunctive sertraline for asymptomatic cryptococcal antigenemia: A randomized clinical trial. Med. Mycol. 2020, 58, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Rhein, J.; Hullsiek, K.H.; Tugume, L.; Nuwagira, E.; Mpoza, E.; E Evans, E.; Kiggundu, R.; A Pastick, K.; Ssebambulidde, K.; Akampurira, A.; et al. Adjunctive sertraline for HIV-associated cryptococcal meningitis: A randomised, placebo-controlled, double-blind phase 3 trial. Lancet Infect. Dis. 2019, 19, 843–851. [Google Scholar] [CrossRef]
- Panel on Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV. National Institutes of Health, Centers for Disease Control and Prevention, the HIV Medicine Association, and the Infectious Disease Society of America. 2022. Available online: https://www.idsociety.org/practice-guideline/prevention-and-treatment-of-opportunistic-infections-among-adults-and-adolescents/ (accessed on 19 September 2022).
- Bozzette, S.A.; Larsen, R.A.; Chiu, J.; Leal, M.A.E.; Jacobsen, J.; Rothman, P.; Robinson, P.; Gilbert, G.; McCutchan, J.A.; Tilles, J.; et al. A placebo-controlled trial of maintenance therapy with fluconazole after treatment of cryptococcal meningitis in the acquired immunodeficiency syndrome. California Collaborative Treatment Group. N. Engl. J. Med. 1991, 324, 580–584. [Google Scholar] [CrossRef]
- Mussini, C.; Pezzotti, P.; Miró, J.M.; Martinez, E.; de Quiros, J.C.; Cinque, P.; Borghi, V.; Bedini, A.; Domingo, P.; Cahn, P.; et al. Discontinuation of maintenance therapy for cryptococcal meningitis in patients with AIDS treated with highly active antiretroviral therapy: An international observational study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2004, 38, 565–571. [Google Scholar] [CrossRef]
- Vibhagool, A.; Sungkanuparph, S.; Mootsikapun, P.; Chetchotisakd, P.; Tansuphaswaswadikul, S.; Bowonwatanuwong, C.; Ingsathit, A. Discontinuation of secondary prophylaxis for cryptococcal meningitis in human immunodeficiency virus-infected patients treated with highly active antiretroviral therapy: A prospective, multicenter, randomized study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2003, 36, 1329–1331. [Google Scholar] [CrossRef]
- Henao-Martínez, A.F.; Chastain, D.B.; Franco-Paredes, C. Treatment of cryptococcosis in non-HIV immunocompromised patients. Curr. Opin. Infect. Dis. 2018, 31, 278–285. [Google Scholar] [CrossRef]
- Saag, M.S.; Cloud, G.A.; Graybill, J.R.; Sobel, J.D.; Tuazon, C.U.; Johnson, P.C.; Fessel, W.J.; Moskovitz, B.L.; Wiesinger, B.; Cosmatos, D.; et al. A comparison of itraconazole versus fluconazole as maintenance therapy for AIDS-associated cryptococcal meningitis. National Institute of Allergy and Infectious Diseases Mycoses Study Group. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 1999, 28, 291–296. [Google Scholar] [CrossRef] [Green Version]
- Thompson, G.R., 3rd; Wiederhold, N.P.; Fothergill, A.W.; Vallor, A.C.; Wickes, B.L.; Patterson, T.F. Antifungal susceptibilities among different serotypes of Cryptococcus gattii and Cryptococcus neoformans. Antimicrob. Agents Chemother. 2009, 53, 309–311. [Google Scholar] [CrossRef] [Green Version]
- Castro, G.; Cervi, M.C.; Martinez, R. Vertical transmission of Cryptococcus neoformans from a mother coinfected with human immunodeficiency virus: Case report. Rev. Soc. Bras. Med. Trop. 2006, 39, 501–503. [Google Scholar] [CrossRef] [Green Version]
- Sirinavin, S.; Intusoma, U.; Tuntirungsee, S. Mother-to-child transmission of Cryptococcus neoformans. Pediatr. Infect. Dis. J. 2004, 23, 278–279. [Google Scholar] [CrossRef]
- Ely, E.W.; Peacock, J.E., Jr.; Haponik, E.F.; Washburn, R.G. Cryptococcal pneumonia complicating pregnancy. Medicine 1998, 77, 153–167. [Google Scholar] [CrossRef]
- LaGatta, M.A.; Jordan, C.; Khan, W.; Toomey, J. Isolated pulmonary cryptococcosis in pregnancy. Obstet. Gynecol. 1998, 92, 682–684. [Google Scholar]
- Nakamura, S.; Izumikawa, K.; Seki, M.; Kakeya, H.; Yamamoto, Y.; Yanagihara, K.; Miyazaki, Y.; Kohno, S. Pulmonary cryptococcosis in late pregnancy and review of published literature. Mycopathologia 2009, 167, 125–131. [Google Scholar] [CrossRef] [Green Version]
- Pastick, K.A.; Nalintya, E.; Tugume, L.; Ssebambulidde, K.; Stephens, N.; E Evans, E.; Ndyetukira, J.F.; Nuwagira, E.; Skipper, C.; Muzoora, C.; et al. Cryptococcosis in pregnancy and the postpartum period: Case series and systematic review with recommendations for management. Med. Mycol. 2020, 58, 282–292. [Google Scholar] [CrossRef]
- Severo, C.B.; Xavier, M.O.; Gazzoni, A.F.; Severo, L.C. Cryptococcosis in children. Paediatr. Respir. Rev. 2009, 10, 166–171. [Google Scholar] [CrossRef]
- Sweeney, D.A.; Caserta, M.T.; Korones, D.N.; Casadevall, A.; Goldman, D.L. A ten-year-old boy with a pulmonary nodule secondary to Cryptococcus neoformans: Case report and review of the literature. Pediatr. Infect. Dis. J. 2003, 22, 1089–1093. [Google Scholar] [CrossRef]
- Liu, L.; Guo, L.; Liu, Y.; Chen, T.; Li, S.; Yang, Y.; Liu, G. Clinical characteristics and prognosis of pediatric cryptococcosis in Beijing Children’s Hospital, 2002–2014. Eur. J. Pediatr. 2017, 176, 1235–1244. [Google Scholar] [CrossRef]
- Hevey, M.A.; George, I.A.; Raval, K.; Powderly, W.G.; Spec, A. Presentation and Mortality of Cryptococcal Infection Varies by Predisposing Illness: A Retrospective Cohort Study. Am. J. Med. 2019, 132, 977–983.e1. [Google Scholar] [CrossRef]
- Vilchez, R.A.; Linden, P.; Lacomis, J.; Costello, P.; Fung, J.; Kusne, S. Acute respiratory failure associated with pulmonary cryptococcosis in non-aids patients. Chest 2001, 119, 1865–1869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyohas, M.-C.; Roux, P.; Bollens, D.; Chouaid, C.; Rozenbaum, W.; Meynard, J.-L.; Poirot, J.-L.; Frottier, J.; Mayaud, C. Pulmonary cryptococcosis: Localized and disseminated infections in 27 patients with AIDS. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 1995, 21, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Sifri, C.; Silveira, F.P.; Miller, R.; Gregg, K.S.; Huprikar, S.; Lease, E.D.; Zimmer, A.; Dummer, J.S.; Spak, C.W.; et al. Cryptococcosis in Patients with Cirrhosis of the Liver and Posttransplant Outcomes. Transplantation 2015, 99, 2132–2141. [Google Scholar] [CrossRef] [PubMed]
- George, I.A.; Santos, C.A.Q.; Olsen, M.A.; Powderly, W.G. Epidemiology of Cryptococcosis and Cryptococcal Meningitis in a Large Retrospective Cohort of Patients After Solid Organ Transplantation. Open Forum Infect. Dis. 2017, 4, ofx004. [Google Scholar] [CrossRef]
- Lan, C.Q.; Weng, H.; Li, H.Y.; Chen, L.; Lin, Q.H.; Liu, J.F. Retrospective analysis of 117 cases of pulmonary cryptococcosis. Zhonghua Jie He He Hu Xi Za Zhi Zhonghua Jiehe He Huxi Zazhi Chin. J. Tuberc. Respir. Dis. 2016, 39, 862–865. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Howard-Jones, A.R.; Sparks, R.; Pham, D.; Halliday, C.; Beardsley, J.; Chen, S.C.-A. Pulmonary Cryptococcosis. J. Fungi 2022, 8, 1156. https://doi.org/10.3390/jof8111156
Howard-Jones AR, Sparks R, Pham D, Halliday C, Beardsley J, Chen SC-A. Pulmonary Cryptococcosis. Journal of Fungi. 2022; 8(11):1156. https://doi.org/10.3390/jof8111156
Chicago/Turabian StyleHoward-Jones, Annaleise R., Rebecca Sparks, David Pham, Catriona Halliday, Justin Beardsley, and Sharon C.-A. Chen. 2022. "Pulmonary Cryptococcosis" Journal of Fungi 8, no. 11: 1156. https://doi.org/10.3390/jof8111156