
Chest Imaging in Systemic Endemic Mycoses
 , , and
, , and
Abstract
:1. Introduction
2. Imaging Findings
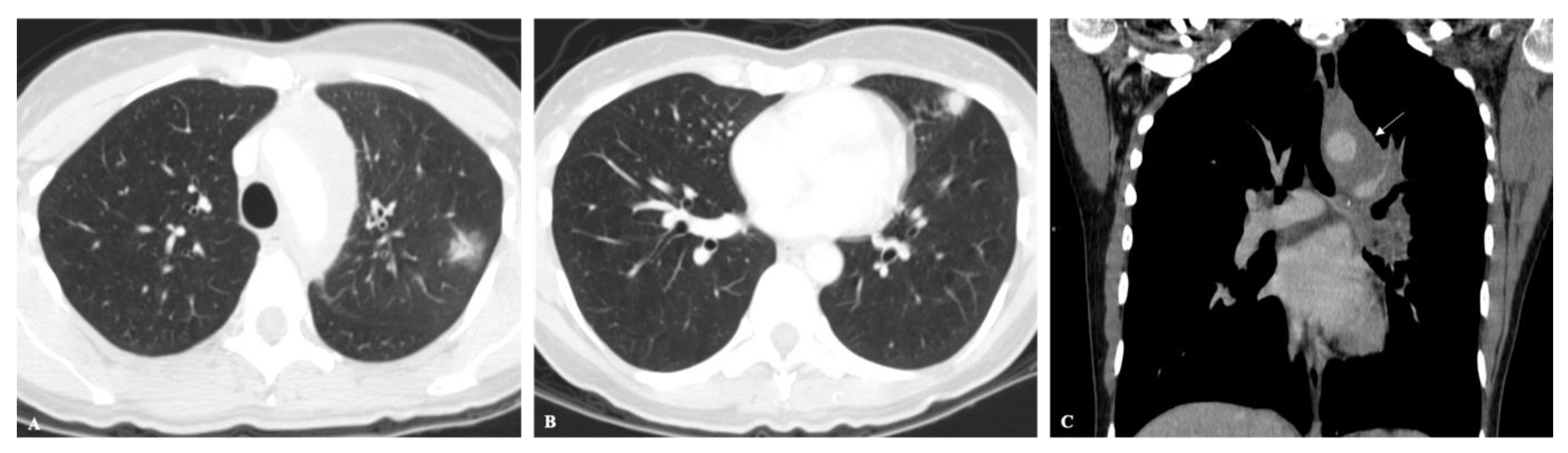
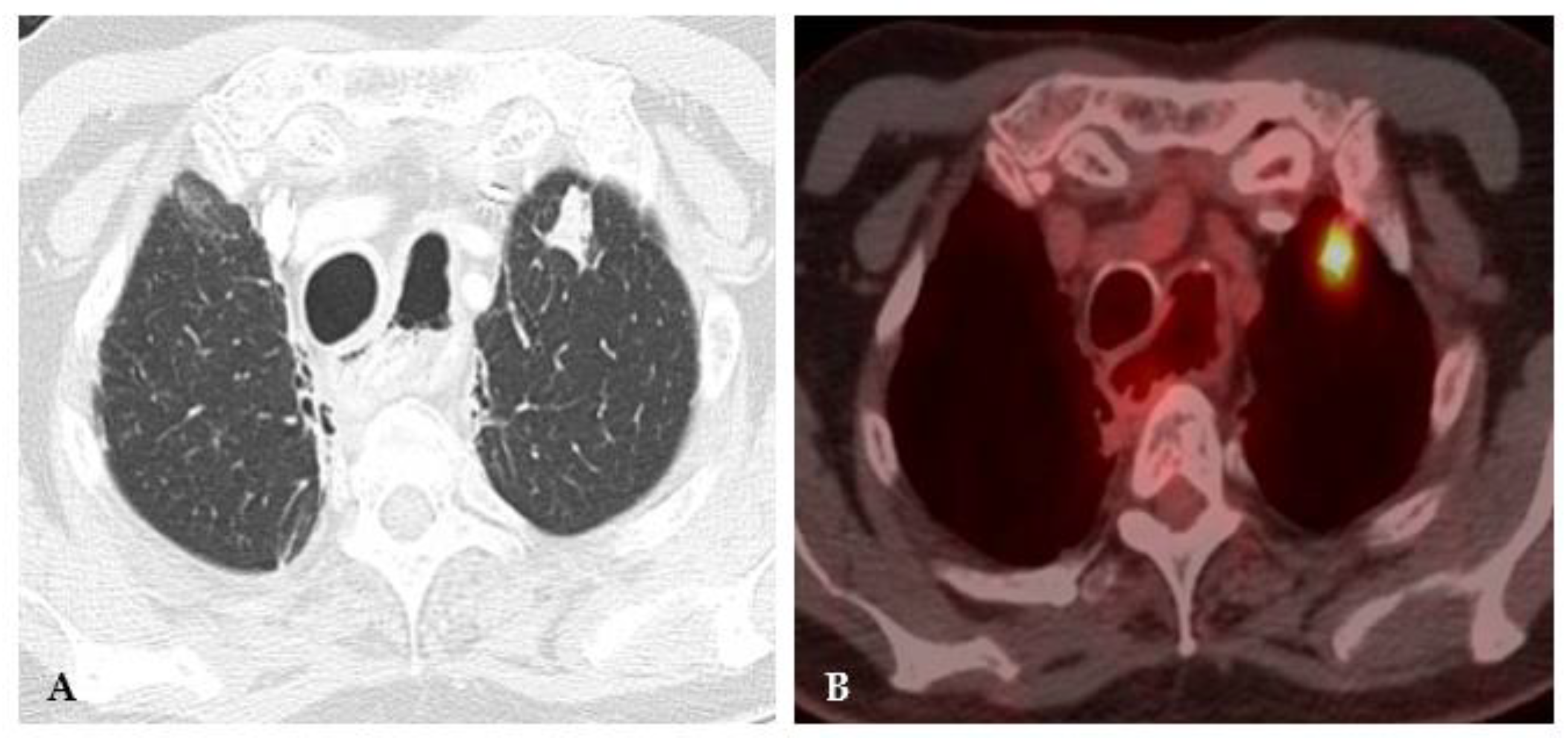
2.1. Lung Nodule or Mass
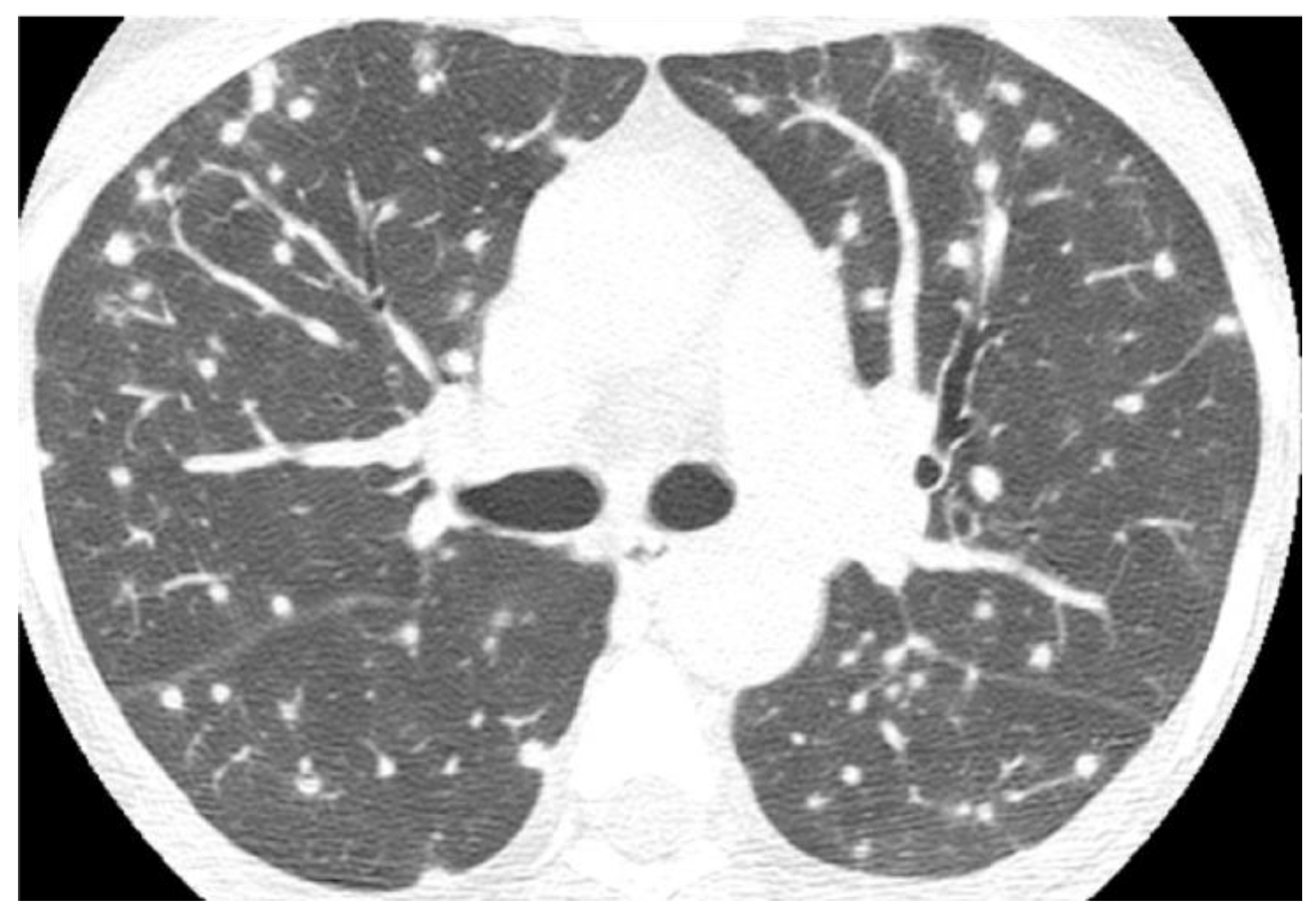
2.2. Non-Resolving Pneumonia
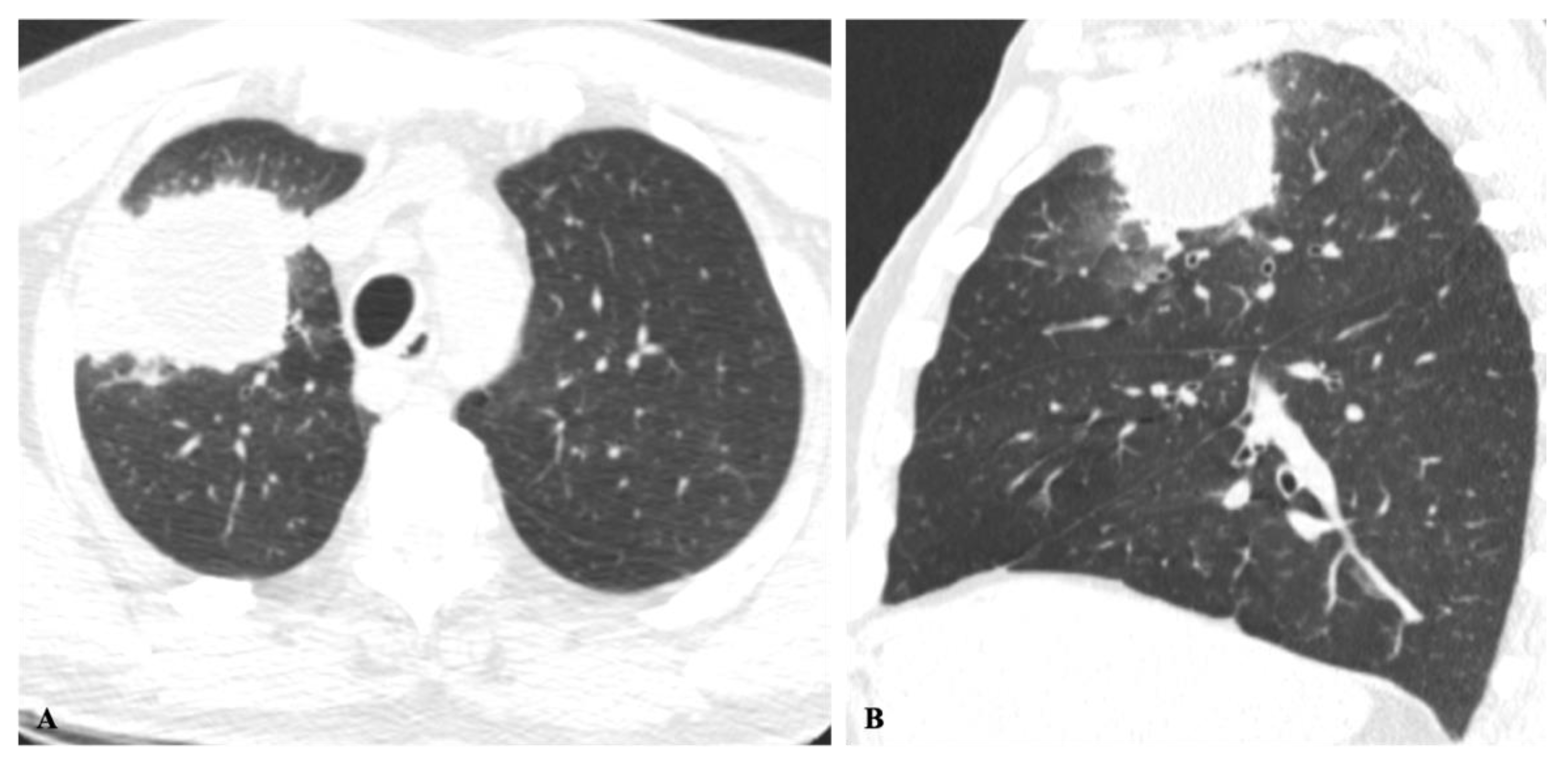
2.3. Chronic Cavitating Disease
2.4. Disseminated Infection
2.5. Mixed Pattern
2.6. Central Bronchiectasis and Asthma
2.7. Additional Intra and Extrathoracic Findings
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Salzer, H.J.; Burchard, G.; Cornely, O.A.; Lange, C.; Rolling, T.; Schmiedel, S.; Libman, M.; Capone, D.; Le, T.; Dalcolmo, M.P.; et al. Diagnosis and Management of Systemic Endemic Mycoses Causing Pulmonary Disease. Respiration 2018, 96, 283–301. [Google Scholar] [CrossRef] [PubMed]
- Denning, D.W.; Chakrabarti, A. Pulmonary and sinus fungal diseases in non-immunocompromised patients. Lancet Infect. Dis. 2017, 17, e357–e366. [Google Scholar] [CrossRef]
- Borchardt, R.A. Endemic Fungal Infections in the United States. Physician Assist. Clin. 2017, 2, 297–312. [Google Scholar] [CrossRef]
- Kunin, J.R.; Flors, L.; Hamid, A.; Fuss, C.; Sauer, D.; Walker, C.M. Thoracic Endemic Fungi in the United States: Importance of Patient Location [published correction appears in Radiographics. Radiographics 2021, 41, 380–398. [Google Scholar] [CrossRef] [PubMed]
- Di Mango, A.L.; Zanetti, G.; Penha, D.; Menna Barreto, M.; Marchiori, E. Endemic pulmonary fungal diseases in immunocompetent patients: An emphasis on thoracic imaging. Expert Rev. Respir. Med. 2019, 13, 263–277. [Google Scholar] [CrossRef]
- Narayanasamy, S.; Dougherty, J.; van Doorn, H.R.; Le, T. Pulmonary talaromycosis: A window into the immunopathogenesis of an endemic mycosis. Mycopathologia 2021, 186, 707–715. [Google Scholar] [CrossRef]
- Reddy, D.L.; Nel, J.; Govender, N.P. Emergomycosis. J. Med. Mycol. 2022, 101313. [Google Scholar] [CrossRef]
- Chong, S.; Lee, K.S.; Yi, C.A.; Chung, M.J.; Kim, T.S.; Han, J. Pulmonary fungal infection: Imaging findings in immunocompetent and immunocompromised patients. Eur. J. Radiol. 2006, 59, 371–383. [Google Scholar] [CrossRef]
- Semionov, A.; Rossi, A.; Perillo, M.; Sayegh, K.; Pressacco, J.; Kosiuk, J. Many Faces of Thoracic Histoplasmosis-Pictorial Essay. Can. Assoc. Radiol. J. 2019, 70, 273–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, P.P.T.E.S.; Rabahi, M.F.; Moreira, M.A.C.; Santana, P.R.P.; Gomes, A.C.P.; Marchiori, E. Tomographic assessment of thoracic fungal diseases: A pattern and signs approach. Radiol. Bras. 2018, 51, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Jude, C.M.; Nayak, N.B.; Patel, M.K.; Deshmukh, M.; Batra, P. Pulmonary coccidioidomycosis: Pictorial review of chest radiographic and CT findings. Radiographics 2014, 34, 912–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, D.L.; Müller, N.L. Pulmonary cryptococcosis in immunocompetent patients: CT findings in 12 patients. AJR Am. J. Roentgenol. 2005, 185, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.-X.; Zhang, Q.; Wen, Q.-T.; Ding, G.-X.; Wang, Y.-G.; Du, F.-X.; Zhang, T.-Y.; Zheng, X.-Y.; Cong, H.-Y.; Du, Y.-L.; et al. Comparison of CT findings and histopathological characteristics of pulmonary cryptococcosis in immunocompetent and immunocompromised patients. Sci. Rep. 2022, 12, 5712. [Google Scholar] [CrossRef] [PubMed]
- Maini, R.; Ranjha, S.; Tandan, N.; Regmi, M.R.; Ullah, S.; Stone, T.; Nayeemuddin, F.; Pervin, N. Pulmonary Blastomycosis: A case series and review of unique radiological findings. Med. Mycol. Case Rep. 2020, 28, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Nagelschneider, A.; Broski, S.M.; Holland, W.P.; E Midthun, D.; Sykes, A.-M.; Lowe, V.J.; Peller, P.J.; Johnson, G.B. The flip-flop fungus sign: An FDG PET/CT sign of benignity. Am. J. Nucl. Med. Mol. Imaging 2017, 7, 212–217. [Google Scholar] [PubMed]
- Kshatriya, R.; Patel, V.; Chaudhari, S.; Patel, P.; Prajapati, D.; Khara, N.; Paliwal, R.; Patel, S. Cannon ball appearance on radiology in a middle-aged diabetic female. Lung India 2016, 33, 562–568. [Google Scholar] [CrossRef]
- Gabe, L.M.; Malo, J.; Knox, K.S. Diagnosis and Management of Coccidioidomycosis. Clin. Chest Med. 2017, 38, 417–433. [Google Scholar] [CrossRef]
- Capone, D.; Marchiori, E.; Wanke, B.; E Dantas, K.; Cavalcanti, M.A.S.; Filho, A.D.; Escuissato, D.L.; Warszawiak, D. Acute pulmonary coccidioidomycosis: CT findings from 15 patients. Br. J. Radiol. 2008, 81, 721–724. [Google Scholar] [CrossRef]
- Fang, W.; Washington, L.; Kumar, N. Imaging manifestations of blastomycosis: A pulmonary infection with potential dissemination. Radiographics 2007, 27, 641–655. [Google Scholar] [CrossRef]
- Ronald, S.; Strzelczyk, J.; Moore, S.; Trepman, E.; Cheang, M.; Limerick, B.; Wiebe, L.; Sarsfield, P.; Macdonald, K.; Meyers, M.; et al. Computed tomographic scan evaluation of pulmonary blastomycosis. Can. J. Infect. Dis. Med. Microbiol. 2009, 20, 112–116. [Google Scholar] [CrossRef]
- Liu, K.; Ding, H.; Xu, B.; You, R.; Xing, Z.; Chen, J.; Lin, Q.; Qu, J. Clinical analysis of non-AIDS patients pathologically diagnosed with pulmonary cryptococcosis. J. Thorac. Dis. 2016, 8, 2813–2821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qu, Y.; Liu, G.; Ghimire, P.; Liao, M.; Shi, H.; Yang, G.; Xu, L.; Wang, G. Primary pulmonary cryptococcosis: Evaluation of CT characteristics in 26 immunocompetent Chinese patients. Acta Radiol. 2012, 53, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Melzani, A.; Michel, R.D.R.D.S.; Ntab, B.; Djossou, F.; Epelboin, L.; Nacher, M.; Blanchet, D.; Demar, M.P.; Couppie, P.; Adenis, A. Incidence and trends in immune reconstitution inflammatory syndrome associated with histoplasma capsulatum among people living with human immunodeficiency virus: A 20-year case series and literature review. Clin. Infect. Dis. 2020, 70, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Wright, T.; Coruh, B.; Fredricks, D.; Kim, N. Immune reconstitution inflammatory syndrome associated with disseminated histoplasmosis and TNF-alpha inhibition. Med. Mycol. Case Rep. 2018, 23, 62–64. [Google Scholar] [CrossRef]
- Batra, P. Pulmonary coccidioidomycosis. J. Thorac. Imaging 1992, 7, 29–38. [Google Scholar] [CrossRef]
- Abreu e Silva, M.À.; Salum, F.G.; Figueiredo, M.A.; Cherubini, K. Important aspects of oral paracoccidioidomycosis--a literature review. Mycoses 2013, 56, 189–199. [Google Scholar] [CrossRef]
- Denning, D.W.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C.; Dimopoulos, Christoph Lange on behalf of the European Society for Clinical Microbiology and Infectious Diseases and European Respiratory Society. Chronic pulmonary aspergillosis: Rationale and clinical guidelines for diagnosis and management. Eur. Respir. J. 2016, 47, 45–68. [Google Scholar] [CrossRef] [Green Version]
- Wheat, L.J.; Connolly-Stringfield, P.A.; Baker, R.L.; Curfman, M.F.; Eads, M.E.; Israel, K.S.; Norris, S.A.; Webb, D.H.; Zeckel, M.L. Disseminated histoplasmosis in the acquired immune deficiency syndrome: Clinical findings, diagnosis and treatment, and review of the literature. Medicine (Baltimore) 1990, 69, 361–374. [Google Scholar] [CrossRef]
- Stockamp, N.W.; Thompson GR 3rd. Coccidioidomycosis. Infect. Dis. Clin. N. Am. 2016, 30, 229–246. [Google Scholar] [CrossRef]
- Restrepo, A.; Benard, G.; de Castro, C.C.; Agudelo, C.A.; Tobón, A.M. Pulmonary paracoccidioidomycosis. Semin. Respir. Crit. Care Med. 2008, 29, 182–197. [Google Scholar] [CrossRef]
- Mendes, R.P.; Cavalcante, R.D.S.; Marques, S.A.; Marques, M.E.A.; Venturini, J.; Sylvestre, T.F.; Paniago, A.M.M.; Pereira, A.C.; Silva, J.D.F.D.; Fabro, A.T.; et al. Paracoccidioidomycosis: Current perspectives from Brazil. Open Microbiol. J. 2017, 11, 224–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tobon, A.M.; Agudelo, C.A.; Osorio, M.L.; Alvarez, D.L.; Arango, M.; Cano, L.E.; Restrepo, A. Residual pulmonary abnormalities in adult patients with chronic paracoccidioidomycosis: Prolonged follow-up after itraconazole therapy. Clin. Infect. Dis. 2003, 37, 898–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barreto, M.M.; Marchiori, E.; Amorim, V.B.; Zanetti, G.; Takayassu, T.C.; Escuissato, D.L.; Souza, A.S.; Rodrigues, R.S. Thoracic paracoccidioidomycosis: Radiographic and CT findings [published correction appears in Radiographics. Radiographics 2012, 32, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Marchiori, E.; Valiante, P.M.; Mano, C.M.; Zanetti, G.; Escuissato, D.L.; Souza, A.S.; Capone, D. Paracoccidioidomycosis: High-resolution computed tomography-pathologic correlation. Eur. J. Radiol. 2011, 77, 80–84. [Google Scholar] [CrossRef]
- Shah, A.; Panjabi, C. Allergic aspergillosis of the respiratory tract. Eur. Respir. Rev. 2014, 23, 8–29. [Google Scholar] [CrossRef] [Green Version]
- Garrana, S.H.; Buckley, J.R.; Rosado-de-Christenson, M.L.; Martínez-Jiménez, S.; Muñoz, P.; Borsa, J.J. Multimodality Imaging of Focal and Diffuse Fibrosing Mediastinitis. Radiographics 2019, 39, 651–667. [Google Scholar] [CrossRef]
- Polesky, A.P.; Kirsch, C.M.; Synder, L.S.; LoBue, P.; Kagawa, F.T.; Dykstra, B.J.; Wehner, J.H.; Catanzaro, A.; Ampel, N.M.; Stevens, D.A. Airway coccidioidomycosis-report of cases and review. Clin. Infect. Dis. 1999, 28, 1273–1280. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lung Nodule or Mass | Non-Resolving Pneumonia | Chronic Cavitating Disease | Disseminated Infection | Bronchiectasis & Asthma | |||||
|---|---|---|---|---|---|---|---|---|---|
| Imaging Clue | Dx | Imaging Clue | Dx | Imaging Clue | Dx | Imaging Clue | Dx | Imaging Clue | Dx |
| Adenopathy | Coccidioidomycosis Histoplasmosis | Consolidation + large nodules/masses | Blastomycosis Cryptococcosis Paracoccidioidomycosis | Grape-skin cavities + Lymphadenopathy | Coccidioidomycosis | Miliary ARDS Extrathoracic | ++ Histoplasmosis Coccidioidomycosis | High-attenuation mucus plugging Finger in glove | ABPA |
| Lung Mass | Cryptococcosis Blastomycosis | Adenopathy | Coccidioidomycosis Histoplasmosis | Calcified nodes | Histoplasmosis | ||||
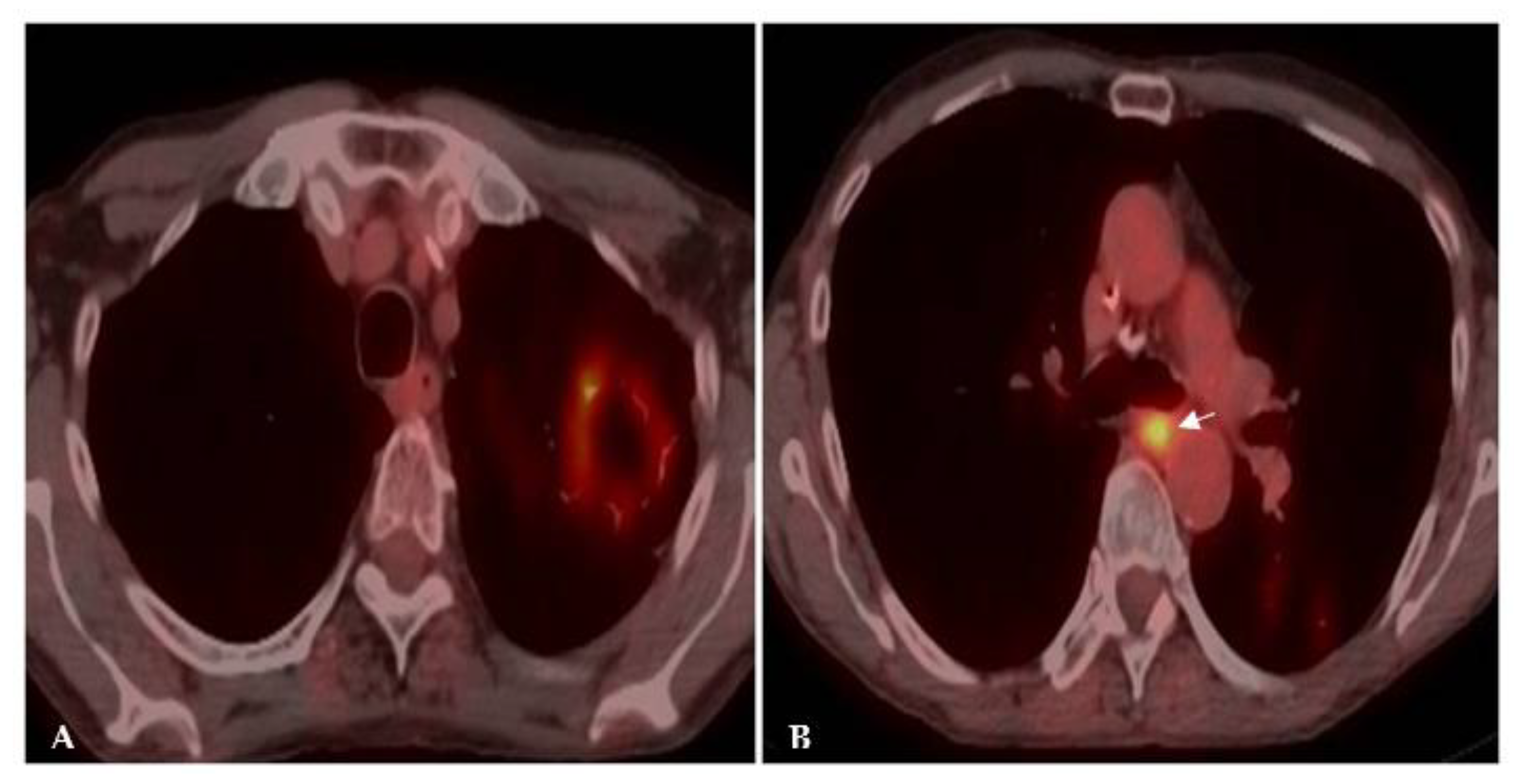
| Flip-flop node SUVmax > lung mass | Granulomatous Infection | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sousa, C.; Marchiori, E.; Youssef, A.; Mohammed, T.-L.; Patel, P.; Irion, K.; Pasini, R.; Mançano, A.; Souza, A.; Pasqualotto, A.C.; et al. Chest Imaging in Systemic Endemic Mycoses. J. Fungi 2022, 8, 1132. https://doi.org/10.3390/jof8111132
Sousa C, Marchiori E, Youssef A, Mohammed T-L, Patel P, Irion K, Pasini R, Mançano A, Souza A, Pasqualotto AC, et al. Chest Imaging in Systemic Endemic Mycoses. Journal of Fungi. 2022; 8(11):1132. https://doi.org/10.3390/jof8111132
Chicago/Turabian StyleSousa, Célia, Edson Marchiori, Ali Youssef, Tan-Lucien Mohammed, Pratik Patel, Klaus Irion, Romulo Pasini, Alexandre Mançano, Arthur Souza, Alessandro C. Pasqualotto, and et al. 2022. "Chest Imaging in Systemic Endemic Mycoses" Journal of Fungi 8, no. 11: 1132. https://doi.org/10.3390/jof8111132