
Dental and Oral Manifestations of COVID-19 Related Mucormycosis: Diagnoses, Management Strategies and Outcomes

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. COVID-19 and Dentistry
3. COVID-19 Related Fungal Infections (Pulmonary and ROCM)
4. Mucormycosis
- ▪
- ▪
- Pulmonary; prevalent in cancer patients or those underwent stem cell or organ transplant.
- ▪
- ▪
- Burn or other skin damage in patients with leukemia, poorly managed diabetes, graft-versus-host disease, human immunodeficiency virus (HIV), or intravenous (IV) drug abuse [38].
- ▪
- Widespread (disseminated), spreads to other body parts through the bloodstream.
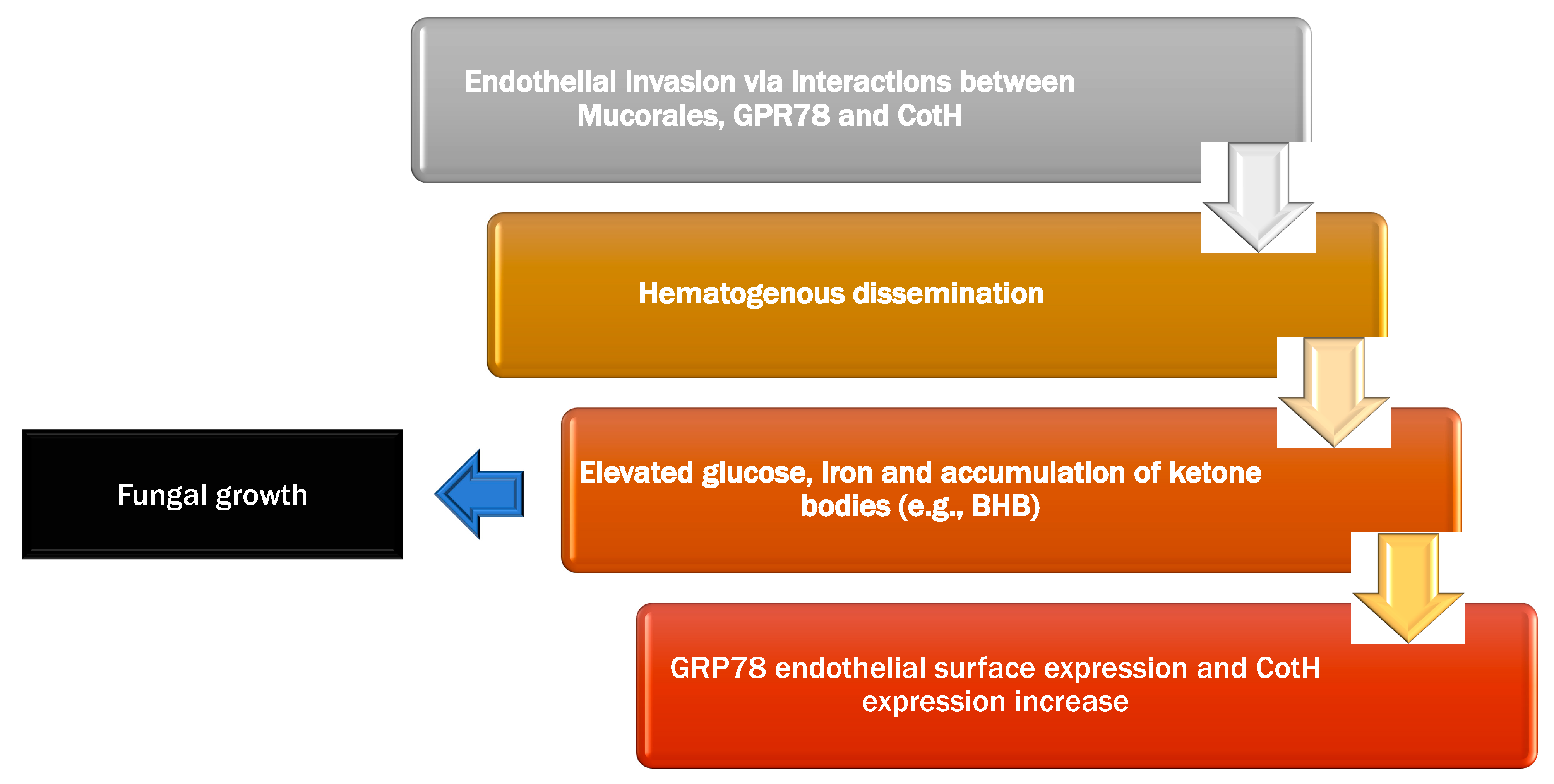
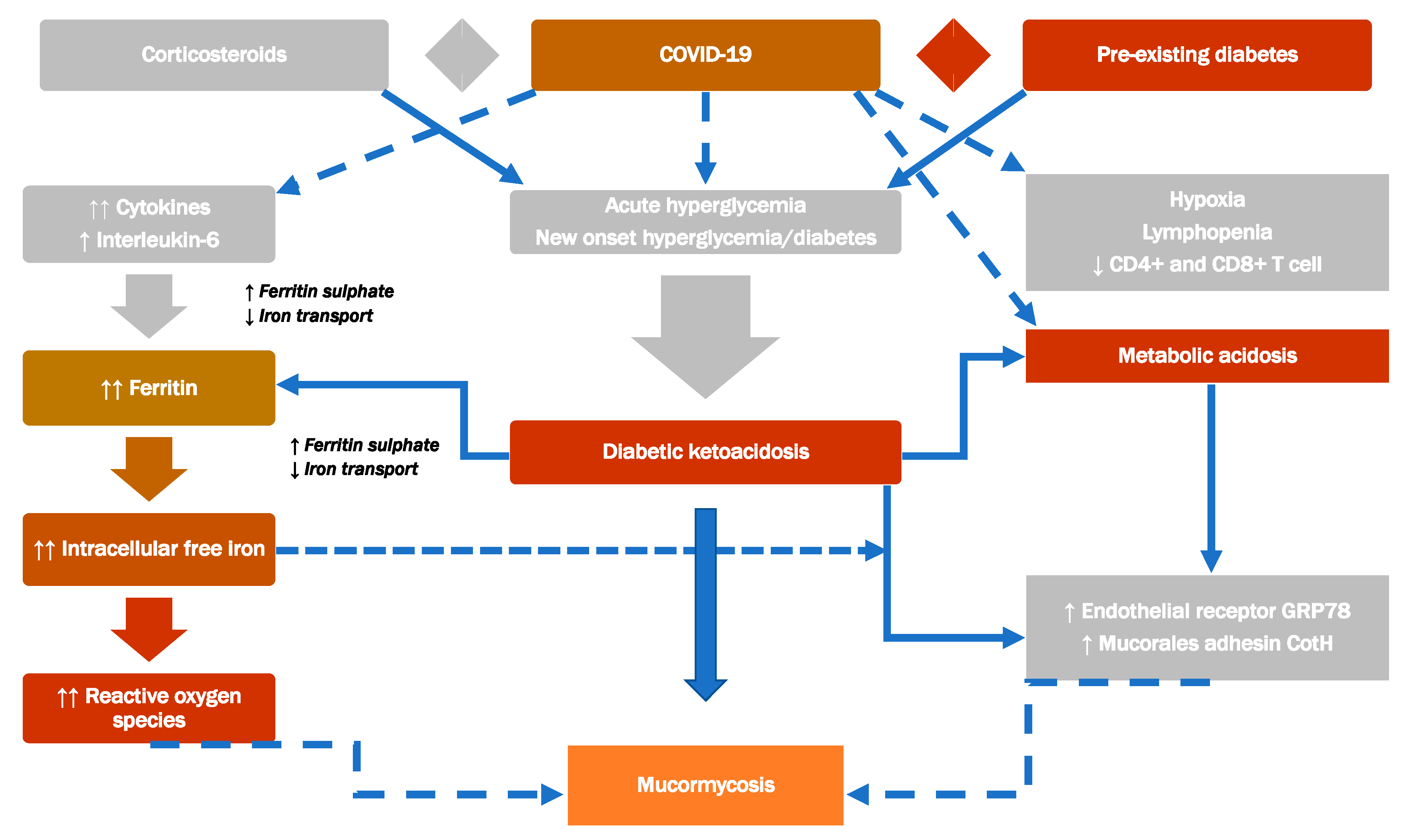
4.1. Etiopathogenesis/Pathogenesis
4.1.1. Endothelial Interaction
4.1.2. Uptake of Iron
4.1.3. Interaction between Mucorales and Immune Defense
Platelets
Natural Killer (NK) Cells
T Cells
4.2. The Most Common Risk Factors for Mucormycosis
4.3. Mucormycosis Clinical Manifestations
4.4. Mucormycosis Diagnosis
4.4.1. Clinical Diagnosis
4.4.2. Microscopic Examination and Culture
4.4.3. Antifungal Susceptibility Testing and Identification of Species
4.4.4. Serology
4.4.5. Molecular Assays
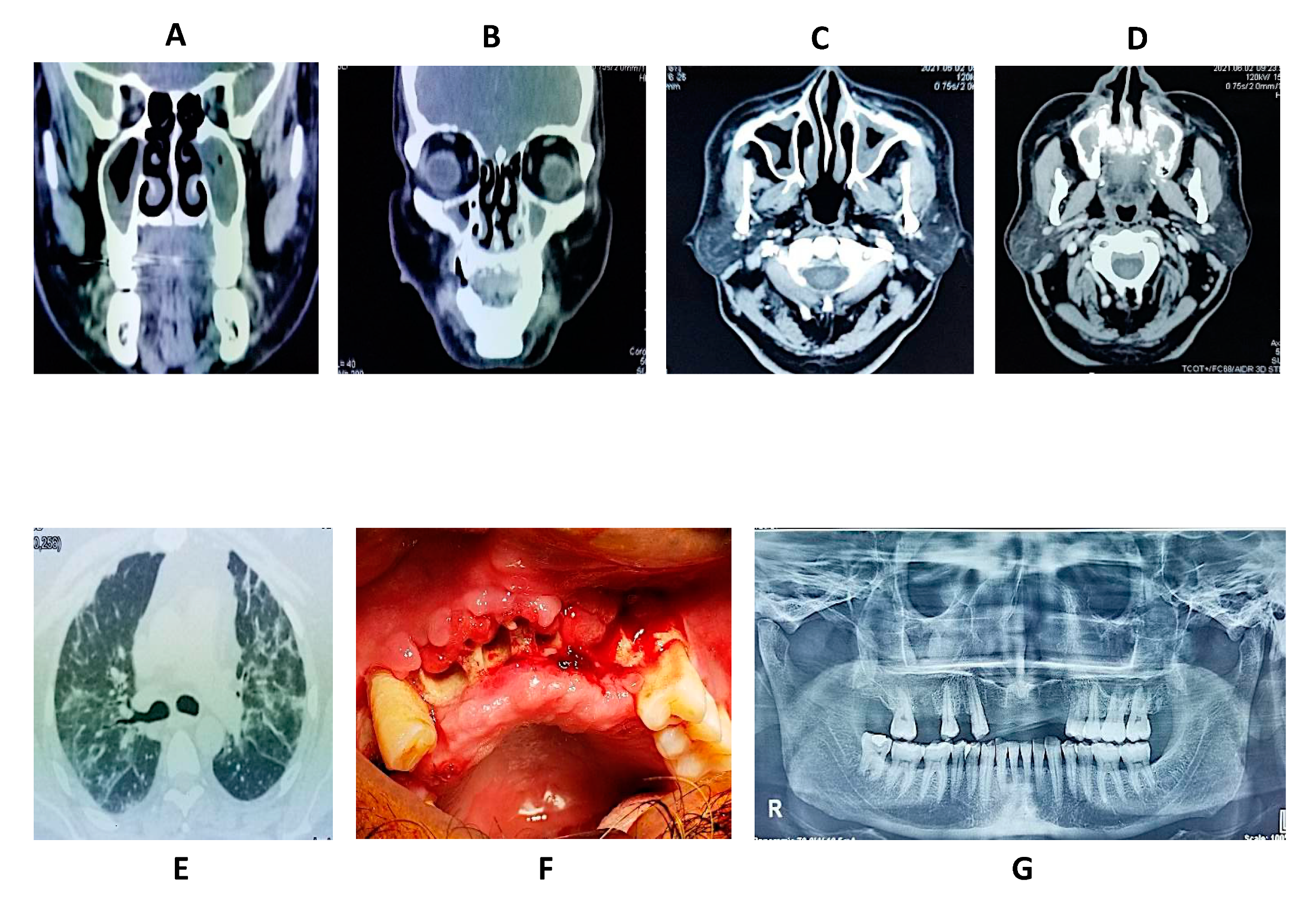
4.4.6. Imaging
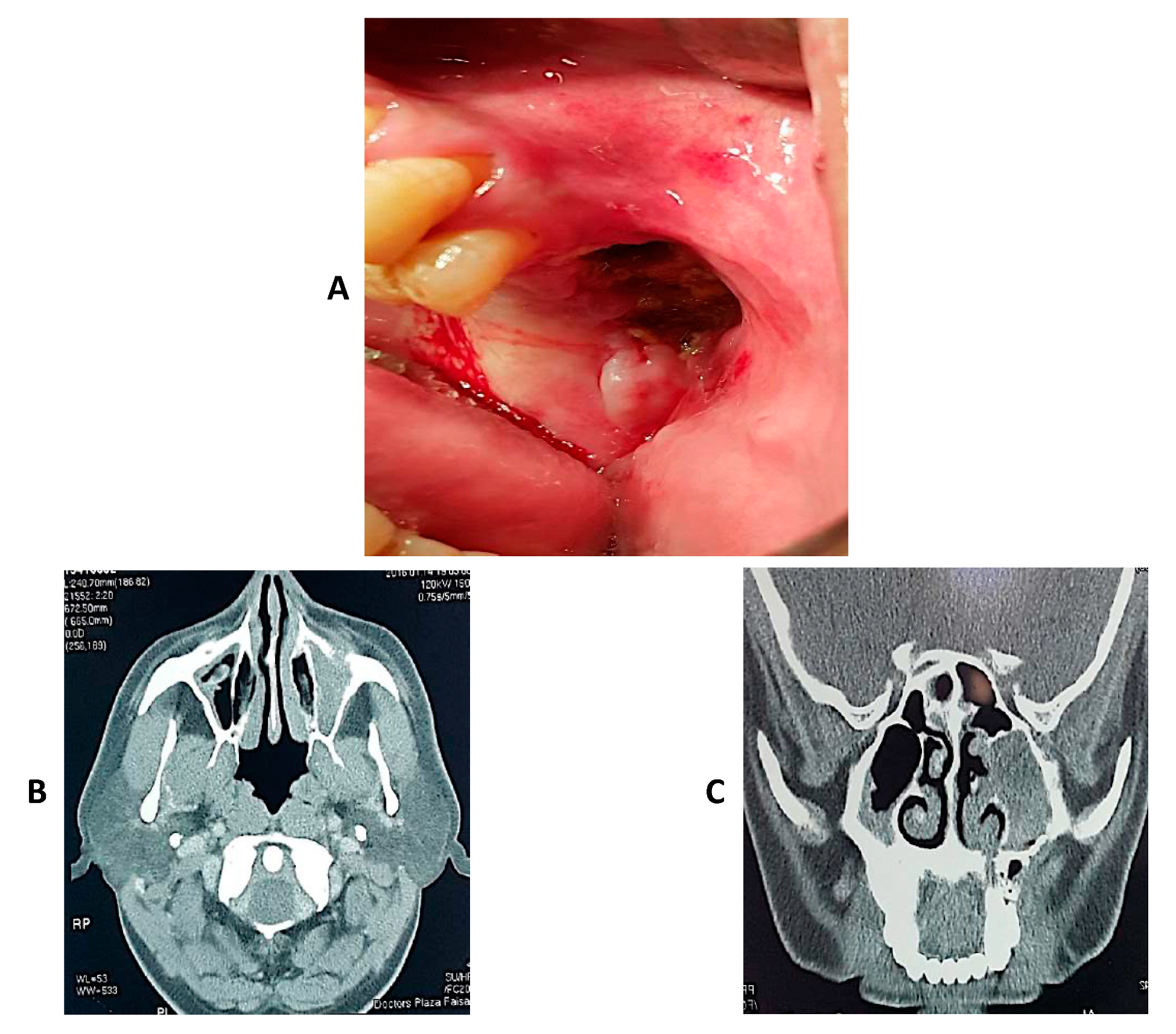
4.5. Clinical Cases of Mucormycosis
4.6. Oral and Dental Manifestations
5. Management of COVID-19 Related Fungal Infections
5.1. Prevention of Mucormycosis
- ▪
- Promoting personal hygiene, including general hygiene like that of hands and face as well as the oral hygiene through proper brushing and antiseptic mouth rinses (chlorhexidine 0.2% or betadine)
- ▪
- Delivery of oxygen should be in a strictly aseptic environment with regular changing of filters and tubes as they can harbor fungus, if contaminated.
- ▪
- Aggressive management and monitoring of immunocompromised state like in case of diabetes, monitoring of blood sugar levels and employing strict control.
- ▪
- Using steroids very carefully, under strict control and according to recommended guidelines.
- ▪
- Caution in using tocilizumab and other related agents.
- ▪
- Consider prophylactic oral delayed release posaconazole (600 mg day 1, 400 mg 2 to 14 days and 300 mg for 3-months) or isavuconazole (200 mg q8H for 1- to 2-days and 200 mg/day for 3-months) [117].
5.2. Treatment of Mucormycosis
5.2.1. Medical Treatment
Systemic Agents
Topical Agents
5.2.2. Surgical Treatment
Turbinectomy
Maxillectomy/Palatal Resection
Orbital Exenteration
5.3. Complications
5.3.1. Complications of the Disease
5.3.2. Complications of Medical Treatment
5.3.3. Complications of Surgical Treatment
5.4. Prognosis
5.5. Future Directions/Recommendations
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Roden, M.M.; Zaoutis, T.E.; Buchanan, W.L.; Knudsen, T.A.; Sarkisova, T.A.; Schaufele, R.L.; Sein, M.; Sein, T.; Chiou, C.C.; Chu, J.H. Epidemiology and outcome of zygomycosis: A review of 929 reported cases. Clin. Infect. Dis. 2005, 41, 634–653. [Google Scholar] [CrossRef] [Green Version]
- Petrikkos, G.; Skiada, A.; Lortholary, O.; Roilides, E.; Walsh, T.J.; Kontoyiannis, D.P. Epidemiology and clinical manifestations of mucormycosis. Clin. Infect. Dis. 2012, 54, S23–S34. [Google Scholar] [CrossRef]
- Walsh, T.J.; Gamaletsou, M.N.; McGinnis, M.R.; Hayden, R.T.; Kontoyiannis, D.P. Early clinical and laboratory diagnosis of invasive pulmonary, extrapulmonary, and disseminated mucormycosis (zygomycosis). Clin. Infect. Dis. 2012, 54, S55–S60. [Google Scholar] [CrossRef]
- Butt, R.T.; Janjua, O.S.; Qureshi, S.M.; Shaikh, M.S.; Guerrero-Gironés, J.; Rodríguez-Lozano, F.J.; Zafar, M.S. Dental Healthcare Amid the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11008. [Google Scholar] [CrossRef]
- Richardson, M. The ecology of the Zygomycetes and its impact on environmental exposure. Clin. Microbiol. Infect. 2009, 15, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Sivagnanam, S.; Sengupta, D.J.; Hoogestraat, D.; Jain, R.; Stednick, Z.; Fredricks, D.N.; Hendrie, P.; Whimbey, E.; Podczervinski, S.T.; Krantz, E.M. Seasonal clustering of sinopulmonary mucormycosis in patients with hematologic malignancies at a large comprehensive cancer center. Antimicrob. Resist. Infect. Control 2017, 6, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, K.; Agolli, A.; Patel, M.H.; Garimella, R.; Devi, M.; Garcia, E.; Amin, H.; Domingue, C.; Del Castillo, R.G.; Sanchez-Gonzalez, M. High mortality co-infections of COVID-19 patients: Mucormycosis and other fungal infections. Discoveries 2021, 9, e126. [Google Scholar] [CrossRef]
- Kumar, M.; Sarma, D.K.; Shubham, S.; Kumawat, M.; Verma, V.; Singh, B.; Nagpal, R.; Tiwari, R. Mucormycosis in COVID-19 pandemic: Risk factors and linkages. Curr. Res. Microb. Sci. 2021, 2, 100057. [Google Scholar] [CrossRef] [PubMed]
- Gupta, G.; Singh, Y.; Thangavelu, L.; Singh, S.K.; Dureja, H.; Chellappan, D.K.; Dua, K. Emerging cases of mucormycosis under COVID-19 pandemic in India: Misuse of antibiotics. Drug Dev. Res. 2021, 82, 880–882. [Google Scholar] [CrossRef] [PubMed]
- Fattah, S.-Y.-A.-S.-A.; Hariri, F.; Ngui, R.; Husman, S.-I.-S. Tongue necrosis secondary to mucormycosis in a diabetic patient: A first case report in Malaysia. J. Mycol. Med. 2018, 28, 519–522. [Google Scholar] [CrossRef] [PubMed]
- Pandilwar, P.; Khan, K.; Shah, K.; Sanap, M.; KS, A.U.; Nerurkar, S. Mucormycosis: A rare entity with rising clinical presentation in immunocompromised hosts. Int. J. Surg. Case Rep. 2020, 77, 57–61. [Google Scholar] [CrossRef]
- Salisbury III, P.L.; Caloss Jr, R.; Cruz, J.M.; Powell, B.L.; Cole, R.; Kohut, R.I. Mucormycosis of the mandible after dental extractions in a patient with acute myelogenous leukemia. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1997, 83, 340–344. [Google Scholar] [CrossRef]
- Cohen, A.; Shoukair, F.L.; Korem, M.; Shaulov, A.; Casap, N. Successful mandibular mucormycosis treatment in the severely neutropenic patient. J. Oral Maxillofac. Surg. 2019, 77, 1209.e1–1209.e12. [Google Scholar] [CrossRef] [PubMed]
- Nilesh, K.; Vande, A.V. Mucormycosis of maxilla following tooth extraction in immunocompetent patients: Reports and review. J. Clin. Exp. Dent. 2018, 10, e300. [Google Scholar] [CrossRef] [PubMed]
- Rapidis, A. Orbitomaxillary mucormycosis (zygomycosis) and the surgical approach to treatment: Perspectives from a maxillofacial surgeon. Clin. Microbiol. Infect. 2009, 15, 98–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dadhich, A.; Nilesh, K.; Patil, R.; Saluja, H. Unusual presentation of mucormycosis mimicking a localised sino-orbital pathology. BMJ Case Rep. CP 2021, 14, e239199. [Google Scholar] [CrossRef]
- Nilesh, K.; Malik, N.A.; Belgaumi, U. Mucormycosis in a healthy elderly patient presenting as oro-antral fistula: Report of a rare incidence. J. Clin. Exp. Dent. 2015, 7, e333. [Google Scholar] [CrossRef] [PubMed]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA—A scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonkaboni, A.; Amirzade-Iranaq, M.H.; Ziaei, H.; Ather, A. Impact of COVID-19 on Dentistry. Adv. Exp. Med. Biol. 2021, 1318, 623–636. [Google Scholar] [CrossRef]
- Barabari, P.; Moharamzadeh, K. Novel Coronavirus (COVID-19) and Dentistry–A Comprehensive Review of Literature. Dent. J. 2020, 8, 53. [Google Scholar] [CrossRef]
- Humagain, M.; Humagain, R.; Rokaya, D. Dental Practice during COVID-19 in Nepal: A Descriptive Cross-sectional Study. JNMA J. Nepal. Med. Assoc. 2020, 58, 764–769. [Google Scholar] [CrossRef]
- Walter, E.; von Bronk, L.; Hickel, R.; Huth, K.C. Impact of COVID-19 on Dental Care during a National Lockdown: A Retrospective Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 7963. [Google Scholar] [CrossRef]
- Expósito-Delgado, A.J.; Ausina-Márquez, V.; Mateos-Moreno, M.V.; Martínez-Sanz, E.; del Carmen Trullols-Casas, M.; Llamas-Ortuño, M.E.; Blanco-González, J.M.; Almerich-Torres, T.; Bravo, M.; Martínez-Beneyto, Y. Delivery of Health Care by Spanish Dental Hygienists in Private and Public Dental Services during the COVID-19 De-Escalation Phase (June 2020): A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 8298. [Google Scholar] [CrossRef]
- Dyer, O. COVID-19: India sees record deaths as “black fungus” spreads fear. Br. Med. J. 2021, 373, n1238. [Google Scholar] [CrossRef] [PubMed]
- Semwal, N.; Rautela, A.; Joshi, D.; Singh, B. Black Fungus (Mucormycosis) A Rare Fungal Infection caused by COVID-19. Int. J. Pharm. Bio Med. Sci. 2021, 1, 31–37. [Google Scholar]
- Sen, M.; Honavar, S.G.; Sharma, N.; Sachdev, M.S. COVID-19 and eye: A review of ophthalmic manifestations of COVID-19. Indian J. Ophthalmol. 2021, 69, 488. [Google Scholar] [PubMed]
- Garg, D.; Muthu, V.; Sehgal, I.S.; Ramachandran, R.; Kaur, H.; Bhalla, A.; Puri, G.D.; Chakrabarti, A.; Agarwal, R. Coronavirus disease (Covid-19) associated mucormycosis (CAM): Case report and systematic review of literature. Mycopathologia 2021, 186, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S. Mucormycosis: The “black fungus” maiming Covid patients in India. 2021. Available online: https://www.bbc.com/news/world-asia-india-57027829 (accessed on 21 December 2021).
- Baker, R.D. Mucormycosis—A new disease? J. Am. Med. Assoc. 1957, 163, 805–808. [Google Scholar] [CrossRef]
- Eucker, J.; Sezer, O.; Graf, B.; Possinger, K. Mucormycoses. Mycoses 2001, 44, 253–260. [Google Scholar] [CrossRef]
- Thomas, D.; Lemon, S.; Mandell, G.; Bennett, J.; Dolin, R. Principles and Practice of Infectious Diseases; Churchil Livingstone: New York, NY, USA, 2000. [Google Scholar]
- Riley, T.T.; Muzny, C.A.; Swiatlo, E.; Legendre, D.P. Breaking the mold: A review of mucormycosis and current pharmacological treatment options. Ann. Pharmacother. 2016, 50, 747–757. [Google Scholar] [CrossRef]
- Chander, J. Textbook of Medical Mycology; JP Medical Ltd.: New Delhi, India, 2017. [Google Scholar]
- Song, Y.; Qiao, J.; Giovanni, G.; Liu, G.; Yang, H.; Wu, J.; Chen, J. Mucormycosis in renal transplant recipients: Review of 174 reported cases. BMC Infect. Dis. 2017, 17, 283. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Adelmann, D.; Fahal, A.; Verbrugh, H.; van Belkum, A.; de Hoog, S. Environmental occurrence of Madurella mycetomatis, the major agent of human eumycetoma in Sudan. J. Clin. Microbiol. 2002, 40, 1031–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallabhaneni, S.; Mody, R.K. Gastrointestinal mucormycosis in neonates: A review. Curr. Fungal Infect. Rep. 2015, 9, 269–274. [Google Scholar] [CrossRef]
- Francis, J.R.; Villanueva, P.; Bryant, P.; Blyth, C.C. Mucormycosis in children: Review and recommendations for management. J. Pediatric Infect. Dis. Soc. 2018, 7, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Grossman, M.; Fox, L.; Kovarik, C.; Rosenbach, M. Subcutaneous and Deep Mycoses: Zygomucosis/Mucormycosis. In Cutaneous Manifestations of Infection in the Immunocompromised Host; Springer: New York, NY, USA, 2012. [Google Scholar]
- Lewis, R.E.; Kontoyiannis, D.P. Epidemiology and treatment of mucormycosis. Future Microbiol. 2013, 8, 1163–1175. [Google Scholar] [CrossRef] [PubMed]
- Binder, U.; Maurer, E.; Lass-Flörl, C. Mucormycosis–from the pathogens to the disease. Clin. Microbiol. Infect. 2014, 20, 60–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, S.; Tramsen, L.; Perkhofer, S.; Lass-Flörl, C.; Hanisch, M.; Röger, F.; Klingebiel, T.; Koehl, U.; Lehrnbecher, T. Rhizopus oryzae hyphae are damaged by human natural killer (NK) cells, but suppress NK cell mediated immunity. Immunobiology 2013, 218, 939–944. [Google Scholar] [CrossRef]
- Ma, L.-J.; Ibrahim, A.S.; Skory, C.; Grabherr, M.G.; Burger, G.; Butler, M.; Elias, M.; Idnurm, A.; Lang, B.F.; Sone, T. Genomic analysis of the basal lineage fungus Rhizopus oryzae reveals a whole-genome duplication. PLoS Genet. 2009, 5, e1000549. [Google Scholar] [CrossRef]
- Brunke, S.; Mogavero, S.; Kasper, L.; Hube, B. Virulence factors in fungal pathogens of man. Curr. Opin. Microbiol. 2016, 32, 89–95. [Google Scholar] [CrossRef]
- Baldin, C.; Ibrahim, A.S. Molecular mechanisms of mucormycosis—The bitter and the sweet. PLoS Pathog. 2017, 13, e1006408. [Google Scholar] [CrossRef] [Green Version]
- Spellberg, B. Mucormycosis pathogenesis: Beyond rhizopus. Virulence 2017, 8, 1481–1482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pana, Z.D.; Seidel, D.; Skiada, A.; Groll, A.H.; Petrikkos, G.; Cornely, O.A.; Roilides, E. Invasive mucormycosis in children: An epidemiologic study in European and non-European countries based on two registries. BMC Infect. Dis. 2016, 16, 667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xhaard, A.; Lanternier, F.; Porcher, R.; Dannaoui, E.; Bergeron, A.; Clement, L.; Lacroix, C.; Herbrecht, R.; Legrand, F.; Mohty, M. Mucormycosis after allogeneic haematopoietic stem cell transplantation: A French Multicentre Cohort Study (2003–2008). Clin. Microbiol. Infect. 2012, 18, E396–E400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebremariam, T.; Liu, M.; Luo, G.; Bruno, V.; Phan, Q.T.; Waring, A.J.; Edwards, J.E.; Filler, S.G.; Yeaman, M.R.; Ibrahim, A.S. CotH3 mediates fungal invasion of host cells during mucormycosis. J. Clin. Investig. 2014, 124, 237–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aird, W.C. Endothelial cell heterogeneity. Cold Spring Harb. Perspect. Med. 2012, 2, a006429. [Google Scholar] [CrossRef]
- Liu, M.; Spellberg, B.; Phan, Q.T.; Fu, Y.; Fu, Y.; Lee, A.S.; Edwards, J.E.; Filler, S.G.; Ibrahim, A.S. The endothelial cell receptor GRP78 is required for mucormycosis pathogenesis in diabetic mice. J. Clin. Investig. 2010, 120, 1914–1924. [Google Scholar] [CrossRef] [Green Version]
- Roilides, E.; Antachopoulos, C.; Simitsopoulou, M. Pathogenesis and host defence against Mucorales: The role of cytokines and interaction with antifungal drugs. Mycoses 2014, 57, 40–47. [Google Scholar] [CrossRef]
- Gebremariam, T.; Lin, L.; Liu, M.; Kontoyiannis, D.P.; French, S.; Edwards, J.E.; Filler, S.G.; Ibrahim, A.S. Bicarbonate correction of ketoacidosis alters host-pathogen interactions and alleviates mucormycosis. J. Clin. Investig. 2016, 126, 2280–2294. [Google Scholar] [CrossRef] [Green Version]
- Chibucos, M.C.; Soliman, S.; Gebremariam, T.; Lee, H.; Daugherty, S.; Orvis, J.; Shetty, A.C.; Crabtree, J.; Hazen, T.H.; Etienne, K.A. An integrated genomic and transcriptomic survey of mucormycosis-causing fungi. Nat. Commun. 2016, 7, 12218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirazi, F.; Kontoyiannis, D.P.; Ibrahim, A.S. Iron starvation induces apoptosis in Rhizopus oryzae in vitro. Virulence 2015, 6, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Cantinieaux, B.; Janssens, A.; Boelaert, J.R.; Lejeune, M.; Vermylen, C.; Kerrels, V.; Cornu, G.; Winand, J.; Fondu, P. Ferritin-associated iron induces neutrophil dysfunction in hemosiderosis. J. Lab. Clin. Med. 1999, 133, 353–361. [Google Scholar] [CrossRef]
- Farmakiotis, D.; Kontoyiannis, D.P. Mucormycoses. Infect. Dis. Clin. 2016, 30, 143–163. [Google Scholar] [CrossRef]
- Ibrahim, A.S.; Gebermariam, T.; Fu, Y.; Lin, L.; Husseiny, M.I.; French, S.W.; Schwartz, J.; Skory, C.D.; Edwards, J.E.; Spellberg, B.J. The iron chelator deferasirox protects mice from mucormycosis through iron starvation. J. Clin. Investig. 2007, 117, 2649–2657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spellberg, B.; Ibrahim, A.S.; Chin-Hong, P.V.; Kontoyiannis, D.P.; Morris, M.I.; Perfect, J.R.; Fredricks, D.; Brass, E.P. The Deferasirox–AmBisome Therapy for Mucormycosis (DEFEAT Mucor) study: A randomized, double-blinded, placebo-controlled trial. J. Antimicrob. Chemother. 2012, 67, 715–722. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.S.; Voelz, K. The mucormycete–host interface. Curr. Opin. Microbiol. 2017, 40, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Speth, C.; Rambach, G.; Lass-Flörl, C. Platelet immunology in fungal infections. Thromb. Haemost. 2014, 112, 632–639. [Google Scholar] [CrossRef]
- Bruserud, Ø. Bidirectional crosstalk between platelets and monocytes initiated by Toll-like receptor: An important step in the early defense against fungal infections? Platelets 2013, 24, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Schulze, B.; Rambach, G.; Schwartze, V.U.; Voigt, K.; Schubert, K.; Speth, C.; Jacobsen, I.D. Ketoacidosis alone does not predispose to mucormycosis by Lichtheimia in a murine pulmonary infection model. Virulence 2017, 8, 1657–1667. [Google Scholar] [CrossRef] [Green Version]
- Vivier, E.; Tomasello, E.; Baratin, M.; Walzer, T.; Ugolini, S. Functions of natural killer cells. Nat. Immunol. 2008, 9, 503–510. [Google Scholar] [CrossRef]
- Gill, S.; Olson, J.A.; Negrin, R.S. Natural killer cells in allogeneic transplantation: Effect on engraftment, graft-versus-tumor, and graft-versus-host responses. Biol. Blood Marrow Transplant. 2009, 15, 765–776. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, S.; Schneider, A.; Demir, A.; Lass-Flörl, C.; Lehrnbecher, T. Natural killer cell-mediated damage of clinical isolates of mucormycetes. Mycoses 2016, 59, 34–38. [Google Scholar] [CrossRef]
- Potenza, L.; Vallerini, D.; Barozzi, P.; Riva, G.; Forghieri, F.; Zanetti, E.; Quadrelli, C.; Candoni, A.; Maertens, J.; Rossi, G. Mucorales-specific T cells emerge in the course of invasive mucormycosis and may be used as a surrogate diagnostic marker in high-risk patients. Blood J. Am. Soc. Hematol. 2011, 118, 5416–5419. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.K.; Singh, R.; Joshi, S.R.; Misra, A. Mucormycosis in COVID-19: A systematic review of cases reported worldwide and in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102146. [Google Scholar] [CrossRef] [PubMed]
- Spellberg, B.; Edwards, J., Jr.; Ibrahim, A. Novel perspectives on mucormycosis: Pathophysiology, presentation, and management. Clin. Microbiol. Rev. 2005, 18, 556–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S. BrainChip for Microbiology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Johnston, R. Weedon’s Skin Pathology Essentials E-Book; Elsevier Health Sciences, UK: London/Oxford, UK, 2016. [Google Scholar]
- Craig, J.R.; Tataryn, R.W.; Aghaloo, T.L.; Pokorny, A.T.; Gray, S.T.; Mattos, J.L.; Poetker, D.M. Management of odontogenic sinusitis: Multidisciplinary consensus statement. Int. Forum Allergy Rhinol. 2020, 10, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Singh, V. Fungal rhinosinusitis: Unravelling the disease spectrum. J. Maxillofac. Oral Surg. 2019, 18, 164–179. [Google Scholar] [CrossRef]
- Hussain, S.; Baxi, H.; Riad, A.; Klugarová, J.; Pokorná, A.; Slezáková, S.; Líčeník, R.; Najmi, A.K.; Klugar, M. COVID-19-Associated Mucormycosis (CAM): An updated evidence mapping. Int. J. Environ. Res. Public Health 2021, 18, 10340. [Google Scholar] [CrossRef]
- Danion, F.; Aguilar, C.; Catherinot, E.; Alanio, A.; DeWolf, S.; Lortholary, O.; Lanternier, F. Mucormycosis: New developments into a persistently devastating infection. Semin. Respir. Crit. Care Med. 2015, 36, 692–705. [Google Scholar] [CrossRef] [PubMed]
- Dannaoui, E.; Lackner, M. Mucorales and Mucormycosis. J. Fungi 2020, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H. Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, D.; Chander, J.; Janmeja, A.K.; Katyal, R. Pulmonary tuberculosis and mucormycosis co-infection in a diabetic patient. Lung India Off. Organ Indian Chest Soc. 2015, 32, 53. [Google Scholar] [CrossRef]
- Chamilos, G.; Marom, E.M.; Lewis, R.E.; Lionakis, M.S.; Kontoyiannis, D.P. Predictors of pulmonary zygomycosis versus invasive pulmonary aspergillosis in patients with cancer. Clin. Infect. Dis. 2005, 41, 60–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corzo-León, D.E.; Chora-Hernández, L.D.; Rodríguez-Zulueta, A.P.; Walsh, T.J. Diabetes mellitus as the major risk factor for mucormycosis in Mexico: Epidemiology, diagnosis, and outcomes of reported cases. Med. Mycol. 2018, 56, 29–43. [Google Scholar] [CrossRef] [PubMed]
- Van Thiel, D.H.; George, M.; Moore, C.M. Fungal infections: Their diagnosis and treatment in transplant recipients. Int. J. Hepatol. 2012, 2012, 106923. [Google Scholar] [CrossRef] [PubMed]
- Grixti, A.; Sadri, M.; Datta, A.V. Uncommon ophthalmologic disorders in intensive care unit patients. J. Crit. Care 2012, 27, 746.e9–746.e22. [Google Scholar] [CrossRef]
- Frater, J.L.; Hall, G.S.; Procop, G.W. Histologic features of zygomycosis: Emphasis on perineural invasion and fungal morphology. Arch. Pathol. Lab. Med. 2001, 125, 375–378. [Google Scholar] [CrossRef]
- Lass-Flörl, C. Zygomycosis: Conventional laboratory diagnosis. Clin. Microbiol. Infect. 2009, 15, 60–65. [Google Scholar] [CrossRef] [Green Version]
- Lass-Flörl, C.; Resch, G.; Nachbaur, D.; Mayr, A.; Gastl, G.; Auberger, J.; Bialek, R.; Freund, M.C. The value of computed tomography-guided percutaneous lung biopsy for diagnosis of invasive fungal infection in immunocompromised patients. Clin. Infect. Dis. 2007, 45, e101–e104. [Google Scholar] [CrossRef] [PubMed]
- Ribes, J.A.; Vanover-Sams, C.L.; Baker, D.J. Zygomycetes in human disease. Clin. Microbiol. Rev. 2000, 13, 236–301. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Das, A.; Mandal, J.; Shivaprakash, M.; George, V.K.; Tarai, B.; Rao, P.; Panda, N.; Verma, S.C.; Sakhuja, V. The rising trend of invasive zygomycosis in patients with uncontrolled diabetes mellitus. Sabouraudia 2006, 44, 335–342. [Google Scholar] [CrossRef] [Green Version]
- Lass-Flörl, C.; Mayr, A. Diagnosing invasive fungal diseases–limitations of microbiological diagnostic methods. Expert Opin. Med. Diagn. 2009, 3, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Lackner, M.; Caramalho, R.; Lass-Flörl, C. Laboratory diagnosis of mucormycosis: Current status and future perspectives. Future Microbiol. 2014, 9, 683–695. [Google Scholar] [CrossRef]
- Hayden, R.; Qian, X.; Procop, G.; Roberts, G.; Lloyd, R. In situ hybridization for the identification of filamentous fungi in tissue section. Diagn. Mol. Pathol. Am. J. Surg. Pathol. Part B 2002, 11, 119–126. [Google Scholar] [CrossRef]
- Alvarez, E.; Sutton, D.; Cano, J.; Fothergill, A.; Stchigel, A.; Rinaldi, M.; Guarro, J. Spectrum of zygomycete species identified in clinically significant specimens in the United States. J. Clin. Microbiol. 2009, 47, 1650–1656. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Lee, J.H.; Kim, Y.-K.; Ki, C.-S.; Huh, H.J.; Lee, N.Y. Identification of mucorales from clinical specimens: A 4-year experience in a single institution. Ann. Lab. Med. 2016, 36, 60–63. [Google Scholar] [CrossRef]
- Ramani, R.; Gromadzki, S.; Pincus, D.H.; Salkin, I.F.; Chaturvedi, V. Efficacy of API 20C and ID 32C systems for identification of common and rare clinical yeast isolates. J. Clin. Microbiol. 1998, 36, 3396–3398. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, P.; Lortholary, O.; Dromer, F.; Dannaoui, E. Carbon assimilation profiles as a tool for identification of zygomycetes. J. Clin. Microbiol. 2007, 45, 1433–1439. [Google Scholar] [CrossRef] [Green Version]
- Schrödl, W.; Heydel, T.; Schwartze, V.U.; Hoffmann, K.; Große-Herrenthey, A.; Walther, G.; Alastruey-Izquierdo, A.; Rodriguez-Tudela, J.L.; Olias, P.; Jacobsen, I.D. Direct analysis and identification of pathogenic Lichtheimia species by matrix-assisted laser desorption ionization–time of flight analyzer-mediated mass spectrometry. J. Clin. Microbiol. 2012, 50, 419–427. [Google Scholar] [CrossRef] [Green Version]
- Vitale, R.G.; de Hoog, G.S.; Schwarz, P.; Dannaoui, E.; Deng, S.; Machouart, M.; Voigt, K.; van de Sande, W.W.; Dolatabadi, S.; Meis, J.F. Antifungal susceptibility and phylogeny of opportunistic members of the order mucorales. J. Clin. Microbiol. 2012, 50, 66–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandven, P.; Eduard, W. Detection and quantitation of antibodies against Rhizopus by enzyme-linked immunosorbent assay. APMIS 1992, 100, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Wysong, D.R.; Waldorf, A.R. Electrophoretic and immunoblot analyses of Rhizopus arrhizus antigens. J. Clin. Microbiol. 1987, 25, 358–363. [Google Scholar] [CrossRef] [Green Version]
- Jones, K.W.; Kaufman, L. Development and evaluation of an immunodiffusion test for diagnosis of systemic zygomycosis (mucormycosis): Preliminary report. J. Clin. Microbiol. 1978, 7, 97–101. [Google Scholar] [CrossRef]
- Hsiao, C.R.; Huang, L.; Bouchara, J.-P.; Barton, R.; Li, H.C.; Chang, T.C. Identification of medically important molds by an oligonucleotide array. J. Clin. Microbiol. 2005, 43, 3760–3768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagao, K.; Ota, T.; Tanikawa, A.; Takae, Y.; Mori, T.; Udagawa, S.-i.; Nishikawa, T. Genetic identification and detection of human pathogenic Rhizopus species, a major mucormycosis agent, by multiplex PCR based on internal transcribed spacer region of rRNA gene. J. Dermatol. Sci. 2005, 39, 23–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larché, J.; Machouart, M.; Burton, K.; Collomb, J.; Biava, M.; Gérard, A.; Fortier, B. Diagnosis of cutaneous mucormycosis due to Rhizopus microsporus by an innovative PCR-restriction fragment-length polymorphism method. Clin. Infect. Dis. 2005, 41, 1362–1365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machouart, M.; Larché, J.; Burton, K.; Collomb, J.; Maurer, P.; Cintrat, A.; Biava, M.; Greciano, S.; Kuijpers, A.; Contet-Audonneau, N. Genetic identification of the main opportunistic Mucorales by PCR-restriction fragment length polymorphism. J. Clin. Microbiol. 2006, 44, 805–810. [Google Scholar] [CrossRef] [Green Version]
- Nyilasi, I.; Papp, T.; Csernetics, Á.; Krizsán, K.; Nagy, E.; Vágvölgyi, C. High-affinity iron permease (FTR1) gene sequence-based molecular identification of clinically important Zygomycetes. Clin. Microbiol. Infect. 2008, 14, 393–397. [Google Scholar] [CrossRef] [Green Version]
- Springer, J.; Lackner, M.; Ensinger, C.; Risslegger, B.; Morton, C.O.; Nachbaur, D.; Lass-Flörl, C.; Einsele, H.; Heinz, W.J.; Loeffler, J. Clinical evaluation of a Mucorales-specific real-time PCR assay in tissue and serum samples. J. Med. Microbiol. 2016, 65, 1414–1421. [Google Scholar] [CrossRef]
- Kasai, M.; Harrington, S.M.; Francesconi, A.; Petraitis, V.; Petraitiene, R.; Beveridge, M.G.; Knudsen, T.; Milanovich, J.; Cotton, M.P.; Hughes, J. Detection of a molecular biomarker for zygomycetes by quantitative PCR assays of plasma, bronchoalveolar lavage, and lung tissue in a rabbit model of experimental pulmonary zygomycosis. J. Clin. Microbiol. 2008, 46, 3690–3702. [Google Scholar] [CrossRef] [Green Version]
- CDC. Diagnosis and Testing for Mucormycosis. Available online: https://www.cdc.gov/fungal/diseases/mucormycosis/diagnosis.html (accessed on 8 October 2021).
- Thornton, C.R. Detection of the ‘Big Five’ mold killers of humans: Aspergillus, fusarium, lomentospora, scedosporium and mucormycetes. Adv. Appl. Microbiol. 2020, 110, 1–61. [Google Scholar]
- Legouge, C.; Caillot, D.; Chrétien, M.-L.; Lafon, I.; Ferrant, E.; Audia, S.; Pagès, P.-B.; Roques, M.; Estivalet, L.; Martin, L. The reversed halo sign: Pathognomonic pattern of pulmonary mucormycosis in leukemic patients with neutropenia? Clin. Infect. Dis. 2014, 58, 672–678. [Google Scholar] [CrossRef]
- Jung, J.; Kim, M.; Lee, H.; Park, Y.; Lee, S.-O.; Choi, S.-H.; Kim, Y.; Woo, J.; Kim, S.-H. Comparison of computed tomographic findings in pulmonary mucormycosis and invasive pulmonary aspergillosis. Clin. Microbiol. Infect. 2015, 21, 684.e11–684.e18. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Wu, H.; Huang, F.; Fan, Z.; Xu, B. Utility of 18F-FDG PET/CT in diagnosis and management of mucormycosis. Clin. Nucl. Med. 2013, 38, e370–e371. [Google Scholar] [CrossRef]
- Nair, V.; Sharma, R.K.; Khanna, A.; Talwar, D. Pulmonary mucormycosis diagnosed by convex probe endobronchial ultrasound-guided fine needle aspiration of cavity wall. Lung India Off. Organ Indian Chest Soc. 2017, 34, 179. [Google Scholar]
- Sanghvi, D.; Kale, H. Imaging of COVID-19-associated craniofacial mucormycosis: A black and white review of the “black fungus”. Clin. Radiol. 2021, 76, 812–819. [Google Scholar] [CrossRef]
- Rao, R.; Shetty, A.P.; Nagesh, C.P. Orbital infarction syndrome secondary to rhino-orbital mucormycosis in a case of COVID-19: Clinico-radiological features. Indian J. Ophthalmol. 2021, 69, 1627–1630. [Google Scholar] [CrossRef] [PubMed]
- Doni, B.R.; Peerapur, B.V.; Thotappa, L.H.; Hippargi, S.B. Sequence of oral manifestations in rhino-maxillary mucormycosis. Indian J. Dent. Res. 2011, 22, 331. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, E.; Abou-Bakr, A.; Hussein, R.R.; El-Gawish, A.A.; Ras, A.b.E.; Ghalwash, D.M. Oral mucormycosis in post-COVID-19 patients: A case series. Oral Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Honavar, S.G. Code Mucor: Guidelines for the Diagnosis, Staging and Management of Rhino-Orbito-Cerebral Mucormycosis in the Setting of COVID-19. Indian J. Ophthalmol. 2021, 69, 1361–1365. [Google Scholar] [CrossRef]
- Gebremariam, T.; Alkhazraji, S.; Baldin, C.; Kovanda, L.; Wiederhold, N.P.; Ibrahim, A.S. Prophylaxis with isavuconazole or posaconazole protects immunosuppressed mice from pulmonary mucormycosis. Antimicrob. Agents Chemother. 2017, 61, e02589-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kontoyiannis, D.P.; Lewis, R.E. How I treat mucormycosis. Blood J. Am. Soc. Hematol. 2011, 118, 1216–1224. [Google Scholar] [CrossRef]
- Rapp, R.P.; Gubbins, P.O.; Evans, M.E. Amphotericin B lipid complex. Ann. Pharmacother. 1997, 31, 1174–1186. [Google Scholar] [CrossRef]
- Hamill, R.J. Amphotericin B formulations: A comparative review of efficacy and toxicity. Drugs 2013, 73, 919–934. [Google Scholar] [CrossRef]
- Dupont, B. Overview of the lipid formulations of amphotericin B. J. Antimicrob. Chemother. 2002, 49, 31–36. [Google Scholar] [CrossRef]
- Adler-Moore, J.P.; Gangneux, J.-P.; Pappas, P.G. Comparison between liposomal formulations of amphotericin B. Sabouraudia 2016, 54, 223–231. [Google Scholar] [CrossRef]
- Handzel, O.; Landau, Z.; Halperin, D. Liposomal amphotericin B treatment for rhinocerbral mucormycosis: How much is enough? Rhinology 2003, 41, 184–186. [Google Scholar]
- Kintzel, P.; Smith, G.H. Practical guidelines for preparing and administering amphotericin B. Am. J. Hosp. Pharm. 1992, 49, 1156–1164. [Google Scholar] [CrossRef] [PubMed]
- Ellis, D. Amphotericin B: Spectrum and resistance. J. Antimicrob. Chemother. 2002, 49, 7–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moen, M.D.; Lyseng-Williamson, K.A.; Scott, L.J. Liposomal amphotericin B. Drugs 2009, 69, 361–392. [Google Scholar] [CrossRef] [PubMed]
- Laniado-Laborín, R.; Cabrales-Vargas, M.N. Amphotericin B: Side effects and toxicity. Rev. Iberoam. Micol. 2009, 26, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Lanternier, F.; Poiree, S.; Elie, C.; Garcia-Hermoso, D.; Bakouboula, P.; Sitbon, K.; Herbrecht, R.; Wolff, M.; Ribaud, P.; Lortholary, O. Prospective pilot study of high-dose (10 mg/kg/day) liposomal amphotericin B (L-AMB) for the initial treatment of mucormycosis. J. Antimicrob. Chemother. 2015, 70, 3116–3123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Morales, A.J.; Sah, R.; Millan-Oñate, J.; Gonzalez, A.; Montenegro-Idrogo, J.J.; Scherger, S.; Franco-Paredes, C.; Henao-Martínez, A.F. COVID-19 Associated Mucormycosis: The Urgent Need to Reconsider the Indiscriminate Use of Immunosuppressive Drugs; SAGE Publications Sage UK: London, UK, 2021. [Google Scholar]
- Alekseyev, K.; Didenko, L.; Chaudhry, B. Rhinocerebral mucormycosis and COVID-19 pneumonia. J. Med. Cases 2021, 12, 85. [Google Scholar] [CrossRef] [PubMed]
- De Beule, K.; Van Gestel, J. Pharmacology of itraconazole. Drugs 2001, 61, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Pierard, G.; Arrese, J.; Pierard-Franchimont, C. Itraconazole. Expert Opin. Pharmacother. 2000, 1, 287–304. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Chwetzoff, E.; Del Rosso, J.; Baran, R. Hepatic safety of itraconazole. J. Cutan. Med. Surg. Inc. Med. Surg. Dermatol. 2002, 6, 210–213. [Google Scholar] [CrossRef]
- Slain, D.; Rogers, P.D.; Cleary, J.D.; Chapman, S.W. Intravenous itraconazole. Ann. Pharmacother. 2001, 35, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Poirier, J.-M.; Cheymol, G. Optimisation of itraconazole therapy using target drug concentrations. Clin. Pharmacokinet. 1998, 35, 461–473. [Google Scholar] [CrossRef]
- Boutet, K.; Garcia, G.; Degano, B.; Gonzalves-Tavares, M.; Tcherakian, C.; Jais, X.; Humbert, M.; Escourrou, P.; Simonneau, G.; Sitbon, O. Results of a 12-week outpatient cardiovascular rehabilitation in patients with idiopathic pulmonary arterial hypertension (iPAH). Eur. Respir. J. 2008, 32, 240s–241s. [Google Scholar]
- Haria, M.; Bryson, H.M.; Goa, K.L. Itraconazole. Drugs 1996, 51, 585–620. [Google Scholar] [CrossRef]
- Goldstein, E.J.; Spellberg, B.; Walsh, T.J.; Kontoyiannis, D.P.; Edwards, J., Jr.; Ibrahim, A.S. Recent advances in the management of mucormycosis: From bench to bedside. Clin. Infect. Dis. 2009, 48, 1743–1751. [Google Scholar]
- Jeong, W.; Keighley, C.; Wolfe, R.; Lee, W.L.; Slavin, M.A.; Chen, S.C.; Kong, D.C. Contemporary management and clinical outcomes of mucormycosis: A systematic review and meta-analysis of case reports. Int. J. Antimicrob. Agents 2019, 53, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Dannaoui, E.; Meletiadis, J.; Mouton, J.W.; Meis, J.F.; Verweij, P.E. In vitro susceptibilities of zygomycetes to conventional and new antifungals. J. Antimicrob. Chemother. 2003, 51, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Almyroudis, N.G.; Sutton, D.A.; Fothergill, A.W.; Rinaldi, M.G.; Kusne, S. In vitro susceptibilities of 217 clinical isolates of zygomycetes to conventional and new antifungal agents. Antimicrob. Agents Chemother. 2007, 51, 2587–2590. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, R.; Mullane, K.; Van Burik, J.-A.; Raad, I.; Abzug, M.; Anstead, G.; Herbrecht, R.; Langston, A.; Marr, K.; Schiller, G. Posaconazole as salvage therapy for zygomycosis. Antimicrob. Agents Chemother. 2006, 50, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Kersemaekers, W.M.; van Iersel, T.; Nassander, U.; O’Mara, E.; Waskin, H.; Caceres, M.; van Iersel, M.L. Pharmacokinetics and safety study of posaconazole intravenous solution administered peripherally to healthy subjects. Antimicrob. Agents Chemother. 2015, 59, 1246–1251. [Google Scholar] [CrossRef] [Green Version]
- Hof, H. A new, broad-spectrum azole antifungal: Posaconazole–mechanisms of action and resistance, spectrum of activity. Mycoses 2006, 49, 2–6. [Google Scholar] [CrossRef]
- Nagappan, V.; Deresinski, S. Posaconazole: A broad-spectrum triazole antifungal agent. Clin. Infect. Dis. 2007, 45, 1610–1617. [Google Scholar] [CrossRef] [Green Version]
- Krishna, G.; Moton, A.; Ma, L.; Medlock, M.M.; McLeod, J. Pharmacokinetics and absorption of posaconazole oral suspension under various gastric conditions in healthy volunteers. Antimicrob. Agents Chemother. 2009, 53, 958–966. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Theuretzbacher, U.; Clancy, C.J.; Nguyen, M.H.; Derendorf, H. Pharmacokinetic/pharmacodynamic profile of posaconazole. Clin. Pharmacokinet. 2010, 49, 379–396. [Google Scholar] [CrossRef] [PubMed]
- Courtney, R.; Wexler, D.; Radwanski, E.; Lim, J.; Laughlin, M. Effect of food on the relative bioavailability of two oral formulations of posaconazole in healthy adults. Br. J. Clin. Pharmacol. 2004, 57, 218–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walravens, J.; Brouwers, J.; Spriet, I.; Tack, J.; Annaert, P.; Augustijns, P. Effect of pH and comedication on gastrointestinal absorption of posaconazole: Monitoring of intraluminal and plasma drug concentrations. Clin Pharm. 2011, 50, 725–734. [Google Scholar] [CrossRef]
- Torres, H.A.; Hachem, R.Y.; Chemaly, R.F.; Kontoyiannis, D.P.; Raad, I.I. Posaconazole: A broad-spectrum triazole antifungal. Lancet Infect. Dis. 2005, 5, 775–785. [Google Scholar] [CrossRef]
- Rachwalski, E.J.; Wieczorkiewicz, J.T.; Scheetz, M.H. Posaconazole: An oral triazole with an extended spectrum of activity. Ann. Pharmacother. 2008, 42, 1429–1438. [Google Scholar] [CrossRef]
- Guarascio, A.J.; Slain, D. Review of the new delayed-release oral tablet and intravenous dosage forms of posaconazole. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2015, 35, 208–219. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.I. Posaconazole: A new oral antifungal agent with an expanded spectrum of activity. Am. J. Health-Syst. Pharm. 2009, 66, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Panos, G.; Velissaris, D.; Karamouzos, V.; Matzaroglou, C.; Tyllianakis, M. Long QT syndrome leading to multiple cardiac arrests after posaconazole administration in an immune-compromised patient with sepsis: An unusual case report. Am. J. Case Rep. 2016, 17, 295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, G.; Gebremariam, T.; Lee, H.; French, S.W.; Wiederhold, N.P.; Patterson, T.F.; Filler, S.G.; Ibrahim, A.S. Efficacy of liposomal amphotericin B and posaconazole in intratracheal models of murine mucormycosis. Antimicrob. Agents Chemother. 2013, 57, 3340–3347. [Google Scholar] [CrossRef] [Green Version]
- Manesh, A.; John, A.O.; Mathew, B.; Varghese, L.; Rupa, V.; Zachariah, A.; Varghese, G.M. Posaconazole: An emerging therapeutic option for invasive rhino-orbito-cerebral mucormycosis. Mycoses 2016, 59, 765–772. [Google Scholar] [CrossRef]
- Spanakis, E.K.; Aperis, G.; Mylonakis, E. New agents for the treatment of fungal infections: Clinical efficacy and gaps in coverage. Clin. Infect. Dis. 2006, 43, 1060–1068. [Google Scholar] [CrossRef] [Green Version]
- Lewis, R.E.; Ben-Ami, R.; Best, L.; Albert, N.; Walsh, T.J.; Kontoyiannis, D.P. Tacrolimus enhances the potency of posaconazole against Rhizopus oryzae in vitro and in an experimental model of mucormycosis. J. Infect. Dis. 2013, 207, 834–841. [Google Scholar] [CrossRef] [Green Version]
- Sipsas, N.V.; Gamaletsou, M.N.; Anastasopoulou, A.; Kontoyiannis, D.P. Therapy of mucormycosis. J. Fungi 2018, 4, 90. [Google Scholar] [CrossRef] [Green Version]
- Kulendra, K.; Habibi, M.; Butler, C.; Clarke, P.; Howard, D. Use of posaconazole in the treatment of infective rhinocerebral mucormycosis. J. Laryngol. Otol. 2010, 124, 1314–1317. [Google Scholar] [CrossRef] [Green Version]
- Arndt, S.; Aschendorff, A.; Echternach, M.; Daemmrich, T.D.; Maier, W. Rhino-orbital-cerebral mucormycosis and aspergillosis: Differential diagnosis and treatment. Eur. Arch. Oto-Rhino-Laryngol. 2009, 266, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Miceli, M.H.; Kauffman, C.A. Isavuconazole: A new broad-spectrum triazole antifungal agent. Clin. Infect. Dis. 2015, 61, 1558–1565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, G.R.; Wiederhold, N.P. Isavuconazole: A comprehensive review of spectrum of activity of a new triazole. Mycopathologia 2010, 170, 291–313. [Google Scholar] [CrossRef] [PubMed]
- Ellsworth, M.; Ostrosky-Zeichner, L. Isavuconazole: Mechanism of action, clinical efficacy, and resistance. J. Fungi 2020, 6, 324. [Google Scholar] [CrossRef]
- Donnelley, M.A.; Zhu, E.S.; Thompson, G.R., 3rd. Isavuconazole in the treatment of invasive aspergillosis and mucormycosis infections. Infect. Drug Resist. 2016, 9, 79. [Google Scholar]
- Graves, B.; Morrissey, C.O.; Wei, A.; Coutsouvelis, J.; Ellis, S.; Pham, A.; Gooi, J.; Ananda-Rajah, M. Isavuconazole as salvage therapy for mucormycosis. Med. Mycol. Case Rep. 2016, 11, 36–39. [Google Scholar] [CrossRef]
- Ashkenazi-Hoffnung, L.; Bilavsky, E.; Levy, I.; Grisaru, G.; Sadot, E.; Ben-Ami, R.; Novikov, A.; Fischer, S.; Nahum, E.; Scheuerman, O. Isavuconazole as successful salvage therapy for mucormycosis in pediatric patients. Pediatric Infect. Dis. J. 2020, 39, 718–724. [Google Scholar] [CrossRef]
- Marty, F.M.; Ostrosky-Zeichner, L.; Cornely, O.A.; Mullane, K.M.; Perfect, J.R.; Thompson III, G.R.; Alangaden, G.J.; Brown, J.M.; Fredricks, D.N.; Heinz, W.J. Isavuconazole treatment for mucormycosis: A single-arm open-label trial and case-control analysis. Lancet Infect. Dis. 2016, 16, 828–837. [Google Scholar] [CrossRef]
- Chandrasekar, P. Management of invasive fungal infections: A role for polyenes. J. Antimicrob. Chemother. 2011, 66, 457–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perlin, D.S. Mechanisms of echinocandin antifungal drug resistance. Ann. N. Y. Acad. Sci. 2015, 1354, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Fera, M.T.; La Camera, E.; De Sarro, A. New triazoles and echinocandins: Mode of action, in vitro activity and mechanisms of resistance. Expert Rev. Anti-Infect. Ther. 2009, 7, 981–998. [Google Scholar] [CrossRef] [PubMed]
- Perea JR, A. Echinocandins: Applied pharmacology. Rev. Iberoam. Micol. 2016, 33, 140–144. [Google Scholar]
- Wagner, C.; Graninger, W.; Presterl, E.; Joukhadar, C. The echinocandins: Comparison of their pharmacokinetics, pharmacodynamics and clinical applications. Pharmacology 2006, 78, 161–177. [Google Scholar] [CrossRef]
- Estes, K.E.; Penzak, S.R.; Calis, K.A.; Walsh, T.J. Pharmacology and antifungal properties of anidulafungin, a new echinocandin. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2009, 29, 17–30. [Google Scholar] [CrossRef]
- Kofla, G.; Ruhnke, M. Pharmacology and metabolism of anidulafungin, caspofungin and micafungin in the treatment of invasive candidosis-review of the literature. Eur. J. Med. Res. 2011, 16, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.I.; Villmann, M. Echinocandins in the management of invasive fungal infections, part 1. Am. J. Health-Syst. Pharm. 2006, 63, 1693–1703. [Google Scholar] [CrossRef]
- Morris, M.I.; Villmann, M. Echinocandins in the management of invasive fungal infections, Part 2. Am. J. Health-Syst. Pharm. 2006, 63, 1813–1820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eschenauer, G.; DePestel, D.D.; Carver, P.L. Comparison of echinocandin antifungals. Ther. Clin. Risk Manag. 2007, 3, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kauffman, C.A.; Carver, P.L. Update on echinocandin antifungals. Semin. Respir. Crit. Care Med. 2008, 29, 211–219. [Google Scholar] [CrossRef]
- Ibrahim, A.S.; Bowman, J.C.; Avanessian, V.; Brown, K.; Spellberg, B.; Edwards, J.E., Jr.; Douglas, C.M. Caspofungin inhibits Rhizopus oryzae 1, 3-β-d-glucan synthase, lowers burden in brain measured by quantitative PCR, and improves survival at a low but not a high dose during murine disseminated zygomycosis. Antimicrob. Agents Chemother. 2005, 49, 721–727. [Google Scholar] [CrossRef] [Green Version]
- Huang, A.M.; Nagel, J.L.; Crass, R.L.; Nguyen, C. Combination Therapy for the Treatment of Mucormycosis: Examining the Evidence. Curr. Fungal Infect. Rep. 2015, 9, 94–110. [Google Scholar] [CrossRef]
- Walsh, T.J.; Kontoyiannis, D.P. What is the role of combination therapy in management of zygomycosis? Clin Infect Dis. 2008, 47, 372–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaux, G.E. Combination antifungal therapy for invasive mold infections involving polyenes: A case report and brief review of the literature. Infect. Dis. Clin. Pract. 2010, 18, 7–15. [Google Scholar] [CrossRef]
- Lal, A.; Porter, J.; Sweeters, N.; Ng, V.; Evans, P.; Neumayr, L.; Kurio, G.; Harmatz, P.; Vichinsky, E. Combined chelation therapy with deferasirox and deferoxamine in thalassemia. Blood Cells Mol. Dis. 2013, 50, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Vichinsky, E.; Onyekwere, O.; Porter, J.; Swerdlow, P.; Eckman, J.; Lane, P.; Files, B.; Hassell, K.; Kelly, P.; Wilson, F. A randomised comparison of deferasirox versus deferoxamine for the treatment of transfusional iron overload in sickle cell disease. Br. J. Haematol. 2007, 136, 501–508. [Google Scholar] [CrossRef]
- Kontoghiorghe, C.N.; Kontoghiorghes, G.J. Efficacy and safety of iron-chelation therapy with deferoxamine, deferiprone, and deferasirox for the treatment of iron-loaded patients with non-transfusion-dependent thalassemia syndromes. Drug Des. Dev. Ther. 2016, 10, 465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grady, R.W.; Galanello, R.; Randolph, R.E.; Kleinert, D.A.; Dessi, C.; Giardina, P.J. Toward optimizing the use of deferasirox: Potential benefits of combined use with deferoxamine. Haematologica 2013, 98, 129. [Google Scholar] [CrossRef] [PubMed]
- Cappellini, M.D. Long-term efficacy and safety of deferasirox. Blood Rev. 2008, 22, S35–S41. [Google Scholar] [CrossRef]
- Ibrahim, A.; Spellberg, B.; Edwards Jr, J. Iron Acquisition: A novel prospective on mucormycosis pathogenesis and treatment. Curr. Opin. Infect. Dis. 2008, 21, 620. [Google Scholar] [CrossRef] [Green Version]
- Emodi, O.; Ohayon, C.; Bilder, A.; Capucha, T.; Wolff, A.; Racmiel, A. Post extraction mucormycosis in immunocompromised patient Management and review of literature. J. Oral Maxillofac. Surg. 2021, 79, 1482–1491. [Google Scholar] [CrossRef]
- Ravani, S.A.; Agrawal, G.A.; Leuva, P.A.; Modi, P.H.; Amin, K.D. Rise of the phoenix: Mucormycosis in COVID-19 times. Indian J. Ophthalmol. 2021, 69, 1563–1568. [Google Scholar]
- Hosseini, S.M.S.; Borghei, P. Rhinocerebral mucormycosis: Pathways of spread. Eur. Arch. Oto-Rhino-Laryngol. Head Neck 2005, 262, 932–938. [Google Scholar] [CrossRef] [PubMed]
- Safder, S.; Carpenter, J.; Roberts, T.; Bailey, N. The “black turbinate” sign: An early MR imaging finding of nasal mucormycosis. Am. J. Neuroradiol. 2010, 31, 771–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roithmann, R. Inferior turbinectomy: What is the best technique? Braz. J. Otorhinolaryngol. 2018, 84, 133–134. [Google Scholar] [CrossRef]
- Mignogna, M.D.; Fortuna, G.; Leuci, S.; Adamo, D.; Ruoppo, E.; Siano, M.; Mariani, U. Mucormycosis in immunocompetent patients: A case-series of patients with maxillary sinus involvement and a critical review of the literature. Int. J. Infect. Dis. 2011, 15, e533–e540. [Google Scholar] [CrossRef] [Green Version]
- Ochi, J.W.; Harris, J.P.; Feldman, J.I.; Press, G.A. Rhinocerebral mucormycosis: Results of aggressive surgical debridement and amphotericin B. Laryngoscope 1988, 98, 1339–1342. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Han, D.; Cui, S.; Huang, Q.; Wei, Y.; Liu, H.; Liu, M. Endoscopic nasal lateral wall dissection approach to maxillary sinus. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi= Chin. J. Otorhinolaryngol. Head Neck Surg. 2007, 42, 743–748. [Google Scholar]
- Rubin, J.S.; Lund, V.J.; Salmon, B. Frontoethmoidectomy in the treatment of mucoceles: A neglected operation. Arch. Otolaryngol. –Head Neck Surg. 1986, 112, 434–436. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, F.A.; Javer, A.R. Primary endoscopic management of the frontal sinus. Otolaryngol. Clin. N. Am. 2001, 34, 59–75. [Google Scholar] [CrossRef]
- Dessi, P.; Castro, F.; Triglia, J.; Zanaret, M.; Cannoni, M. Major complications of sinus surgery: A review of 1192 procedures. J. Laryngol. Otol. 1994, 108, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Buus, D.R.; David, T.T.; Farris, B.K. Ophthalmic complications of sinus surgery. Ophthalmology 1990, 97, 612–619. [Google Scholar] [CrossRef]
- Balai, E.; Mummadi, S.; Jolly, K.; Darr, A.; Aldeerawi, H. Rhinocerebral mucormycosis: A ten-year single centre case series. Cureus 2020, 12, e11776. [Google Scholar] [CrossRef]
- Augustine, H.F.; White, C.; Bain, J. Aggressive combined medical and surgical management of mucormycosis results in disease eradication in 2 pediatric patients. Plast. Surg. 2017, 25, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Oh, W.-s.; Roumanas, E. Dental implant–assisted prosthetic rehabilitation of a patient with a bilateral maxillectomy defect secondary to mucormycosis. J. Prosthet. Dent. 2006, 96, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Mani, U.M.; Mohamed, K.; Krishna Kumar, A.; Inbarajan, A. A modified technique to fabricate a complete hollow obturator for bilateral maxillectomy in a patient with mucormycosis—A technical case report. Spec. Care Dent. 2019, 39, 610–616. [Google Scholar] [CrossRef]
- Schmidt, B.L.; Pogrel, M.; Young, C.W.; Sharma, A. Reconstruction of extensive maxillary defects using zygomaticus implants. J. Oral Maxillofac. Surg. 2004, 62, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Palacios, J.J.; Hanson, E.V.; Rendon, M.A.M.; Infante, R.-S.L. Reconstruction of head and neck mucormycosis: A literature review and own experience in immediate reconstruction. J. Reconstr. Microsurg. Open 2019, 4, e65–e72. [Google Scholar] [CrossRef] [Green Version]
- AK, A.K.; Gupta, V. Rhino-orbital Cerebral Mucormycosis. StatPearls 2021. [Google Scholar] [PubMed]
- Kohn, R.; Hepler, R. Management of limited rhino-orbital mucormycosis without exenteration. Ophthalmology 1985, 92, 1440–1444. [Google Scholar] [CrossRef]
- Godinho, G.; Abreu, I.; Alves, G.; Vaz, R.; Leal, V.; Carvalho, A.C.; Sarmento, A.; Falcão-Reis, F. Orbital Apex Syndrome due to Orbital Mucormycosis after Teeth Infection: A Successful Case Report. Case Rep. Ophthalmol. 2021, 12, 110–115. [Google Scholar] [CrossRef]
- Croce, A.; Moretti, A.; D’agostino, L.; Zingariello, P. Orbital exenteration in elderly patients: Personal experience. Acta Otorhinolaryngol. Ital. 2008, 28, 193. [Google Scholar]
- Rahman, I.; Cook, A.; Leatherbarrow, B. Orbital exenteration: A 13 year Manchester experience. Br. J. Ophthalmol. 2005, 89, 1335–1340. [Google Scholar] [CrossRef] [Green Version]
- Menon, N.G.; Girotto, J.A.; Goldberg, N.H.; Silverman, R.P. Orbital reconstruction after exenteration: Use of a transorbital temporal muscle flap. Ann. Plast. Surg. 2003, 50, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Rabey, N.; Abood, A.; Gillespie, P.; Athanassoglou, V.; Rene, C.; Malata, C.M. Reconstruction of complex orbital exenteration defects: A single center’s experience with a five-year follow-up. Ann. Plast. Surg. 2014, 73, 158–163. [Google Scholar] [CrossRef]
- Kolekar, J.S. Rhinocerebral mucormycosis: A retrospective study. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 93–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Naaj, I.A.; Leiser, Y.; Wolff, A.; Peled, M. The surgical management of rhinocerebral mucormycosis. J. Cranio-Maxillofac. Surg. 2013, 41, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Sorrell, T.C. Antifungal agents. Med. J. Aust. 2007, 187, 404. [Google Scholar] [CrossRef] [PubMed]
- Peterson, K.L.; Wang, M.; Canalis, R.F.; Abemayor, E. Rhinocerebral mucormycosis: Evolution of the disease and treatment options. Laryngoscope 1997, 107, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Rawlani, S.S.; Siddiqui, A.; Reza, M.; Chelkar, S.; Rani, T.; Roy, H.K.B. Black Fungus Mucormycosis, Epidemiology, Etiopathogenesis, Clinical Diagnosis, Histopathology and its Management—A Review. Int. J. Med. Dent. Res. 2021, 1, 1–8. [Google Scholar]
- El-Kholy, N.A.; Abd El-Fattah, A.M.; Khafagy, Y.W. Invasive fungal sinusitis in post COVID-19 patients: A new clinical entity. Laryngoscope 2021, 131, 2652–2658. [Google Scholar] [CrossRef] [PubMed]
- Pagano, L.; Offidani, M.; Fianchi, L.; Nosari, A.; Candoni, A.; Picardi, M.; Corvatta, L.; D’Antonio, D.; Girmenia, C.; Martino, P. Mucormycosis in hematologic patients. Haematologica 2004, 89, 207–214. [Google Scholar] [PubMed]
- Agrawal, R.; Yeldandi, A.; Savas, H.; Parekh, N.D.; Lombardi, P.J.; Hart, E.M. Pulmonary mucormycosis: Risk factors, radiologic findings, and pathologic correlation. Radiographics 2020, 40, 656–666. [Google Scholar] [CrossRef] [PubMed]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef]
- Gutiérrez-Delgado, E.M.; Treviño-González, J.L.; Montemayor-Alatorre, A.; Ceceñas-Falcón, L.A.; Ruiz-Holguín, E.; Andrade-Vázquez, C.J.; Lara-Medrano, R.; Ramos-Jiménez, J. Chronic rhino-orbito-cerebral mucormycosis: A case report and review of the literature. Ann. Med. Surg. 2016, 6, 87–91. [Google Scholar] [CrossRef]
- Do, N.Y.; Lee, J.H.; Dong, G.W. Clinical study of rhinocerebral mucormycosis. Korean J. Otolaryngol.-Head Neck Surg. 2005, 48, 1228–1234. [Google Scholar]
- Yasmin, F.; Najeeb, H.; Naeem, A.; Dapke, K.; Phadke, R.; Asghar, M.S.; Shah, S.M.I.; De Berardis, D.; Ullah, I. COVID-19 associated mucormycosis: A systematic review from diagnostic challenges to management. Diseases 2021, 9, 65. [Google Scholar] [CrossRef]
- Aranjani, J.M.; Manuel, A.; Abdul Razack, H.I.; Mathew, S.T. COVID-19–associated mucormycosis: Evidence-based critical review of an emerging infection burden during the pandemic’s second wave in India. PLoS Negl. Trop. Dis. 2021, 15, e0009921. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Blood Associated Malignancies (Lymphoma, Leukemia and Myeloproliferative Disorders) |
|---|
| Uncontrolled diabetes mellitus concurrent with ketoacidosis |
| High dose corticosteroids/immuno-suppressive drugs for 2–3 weeks |
| Solid organ malignancies |
| Solid organ transplantation |
| Therapy with Deferoxamine |
| Metabolic acidosis |
| Hematopoietic stem cell transplantation |
| Rheumatologic disorders |
| Multiple transfusions |
| Neonatal prematurity |
| Malnutrition |
| Prophylaxis with voriconazole (breakthrough invasive fungal infections) |
| Skin injuries, burns, trauma |
| Contaminated bandages, tongue depressors. |
| Combat-related injuries |
| Intravenous drug abuse |
| Prolonged hospital stays |
| Dental pain |
| Mobile teeth |
| Halitosis (bad breath) |
| Nasal stuffiness |
| Nasal discharge with epistaxis, black purulent discharge |
| Necrotic bone/Sequestrum formation in the palate and maxillary alveolus Formation of Oro-antral/Oro-nasal communications/fistulae Non-healing extraction sockets with signs similar to alveolar osteitis or chronic osteomyelitis. Trismus due to involvement of muscles of mastication Para-sinusal pain |
| Intraoral/Extra oral draining sinuses |
| Erythema of nasal mucosa |
| Palatal ulceration |
| Facial erythema |
| Black discoloration of skin |
| Periorbital erythema and edema, cellulitis |
| Orbital Pain, Ptosis, Diplopia, Vision loss, Ophthalmoplegia Headache |
| Drug Name | Class of Drug | Mechanism of Action | Administration | Dosage | Side Effects/Contraindications/Warnings | Role in Mucormycosis |
|---|---|---|---|---|---|---|
| Amphotericin B | Polyene | Damage to fungal cell by binding to ergosterol | IV | Dose of Amphotericin B deoxycholate is 1–1.5 mg/kg/day while dose of Liposomal Amphotericin B is 5–15 mg/kg/day [68]. | Electrolyte disturbances Nephrotoxicity, hepatotoxicity, neurotoxicity | 1st line agent in all cases unless contraindicated or not tolerated by the patient. |
| Itraconazole | Azole | Inhibition conversion of lansosterol to ergosterol by blocking 14-α-demethylase | Capsules, oral solution and IV | 100–200 mg/day | GI disturbances Hypertension Cardiotoxicity | Minimal activity. 2nd or 3rd line agent where better azoles are not available and amphotericin B cannot be used. |
| posaconazole | Azole | Inhibition conversion of lansosterol to ergosterol by blocking 14-α-demethylase | Oral suspension, delayed release tablet and IV | 200–300 mg/day | GI disturbances Hepatotoxicity Nephrotoxicity Infusion related reactions | Used as prophylactic agent in mucormycosis prone individuals 2nd line agent after amphotericin B.Useful as salvage therapy. |
| Isavuconazole | Azole | Inhibition conversion of lansosterol to ergosterol by blocking 14-α-demethylase | Oral and IV | 200 mg/day | GI disturbances Hepatotoxicity Prolongs QT interval Skin rashes | So far, the best azole with efficacy comparable to amphotericin B and can be used as first line agent. Useful as salvage therapy. |
| Echinocandins | Cell wall inhibitor | Inhibits enzyme 1,3-β-D-glucan causing damage to fungal cell wall | IV | 50–70 mg/day | Infusion related reactions Hepatotoxicity | Used as combination therapy with amphotericin B. |
| Deferasirox | Chelators | Chelates and removes excess iron | IV | 40–60 mg/day | Sensorineural deafness Blindness Skin eruptions Anaphylactic reactions | Used in combination with amphotericin B for reducing iron overload. Considered adjunctive treatment in mucormycosis. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janjua, O.S.; Shaikh, M.S.; Fareed, M.A.; Qureshi, S.M.; Khan, M.I.; Hashem, D.; Zafar, M.S. Dental and Oral Manifestations of COVID-19 Related Mucormycosis: Diagnoses, Management Strategies and Outcomes. J. Fungi 2022, 8, 44. https://doi.org/10.3390/jof8010044
Janjua OS, Shaikh MS, Fareed MA, Qureshi SM, Khan MI, Hashem D, Zafar MS. Dental and Oral Manifestations of COVID-19 Related Mucormycosis: Diagnoses, Management Strategies and Outcomes. Journal of Fungi. 2022; 8(1):44. https://doi.org/10.3390/jof8010044
Chicago/Turabian StyleJanjua, Omer Sefvan, Muhammad Saad Shaikh, Muhammad Amber Fareed, Sana Mehmood Qureshi, Muhammad Ikram Khan, Danya Hashem, and Muhammad Sohail Zafar. 2022. "Dental and Oral Manifestations of COVID-19 Related Mucormycosis: Diagnoses, Management Strategies and Outcomes" Journal of Fungi 8, no. 1: 44. https://doi.org/10.3390/jof8010044