
Cunninghamella arunalokei a New Species of Cunninghamella from India Causing Disease in an Immunocompetent Individual

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Details and Laboratory Diagnosis
2.2. Phenotypic Characterization
2.3. Antifungal Susceptibility Testing
2.4. Molecular Characterization
2.5. Phylogenetic Tree Construction
2.6. Whole-Genome Phylogenetic Analysis
2.7. Ethical Statement
3. Results
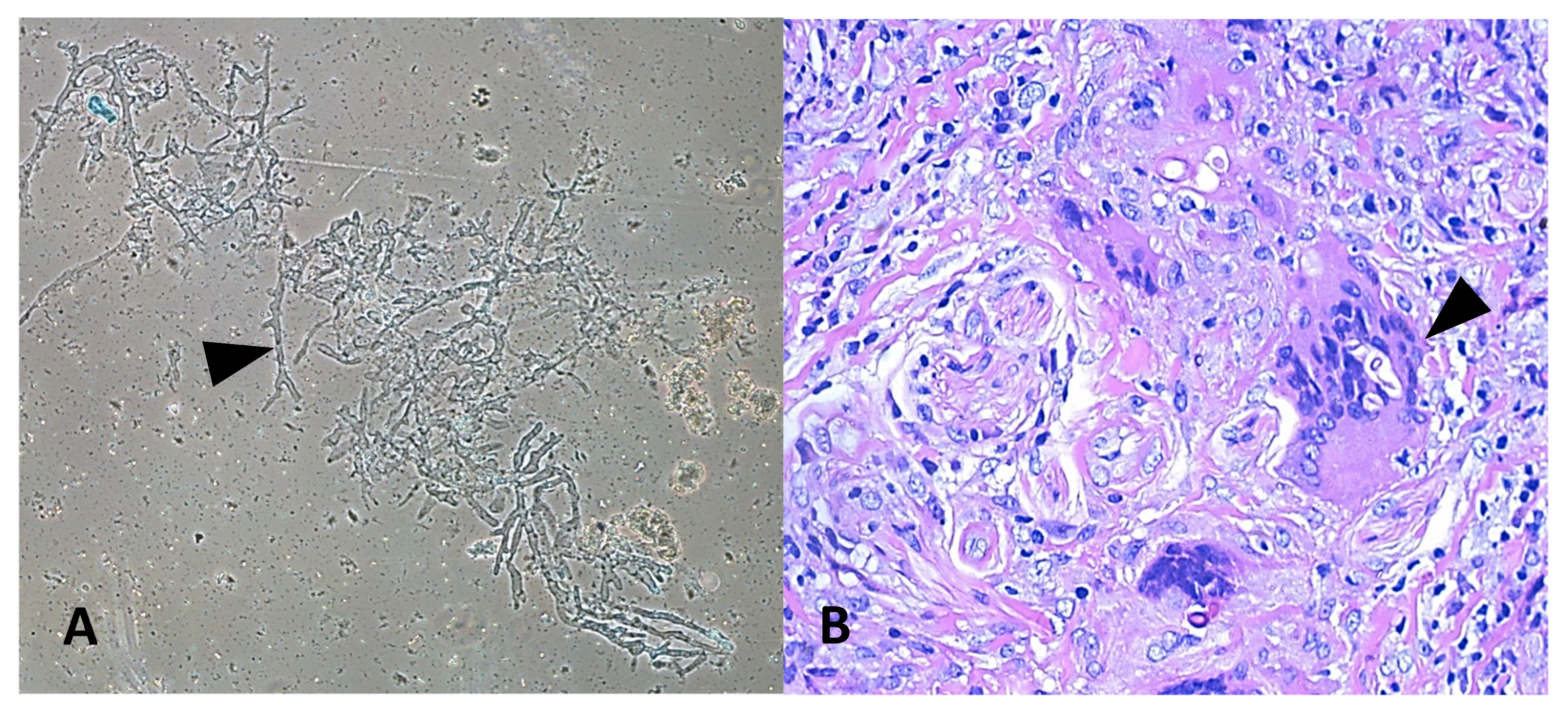
3.1. Clinical Details and Laboratory Diagnosis
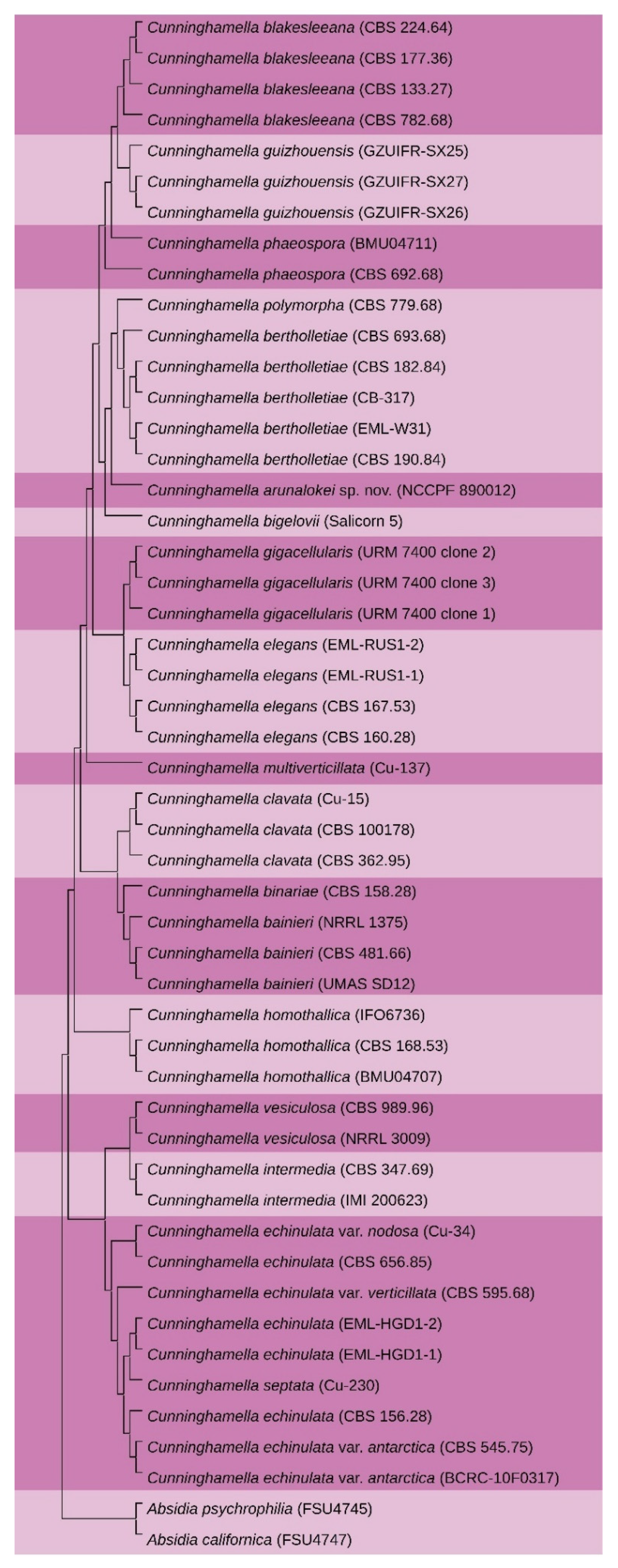
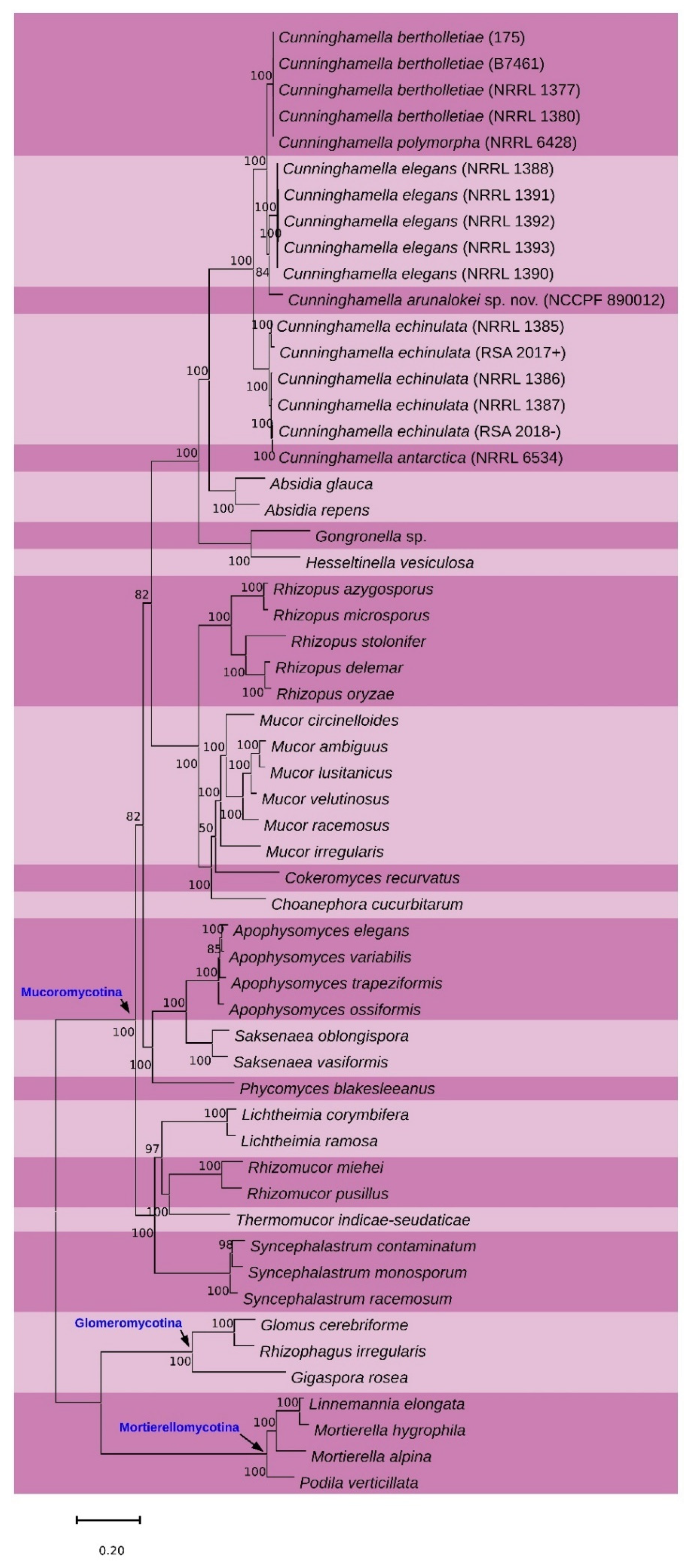
3.2. Phylogenetic Analysis
3.3. Antifungal Susceptibilit
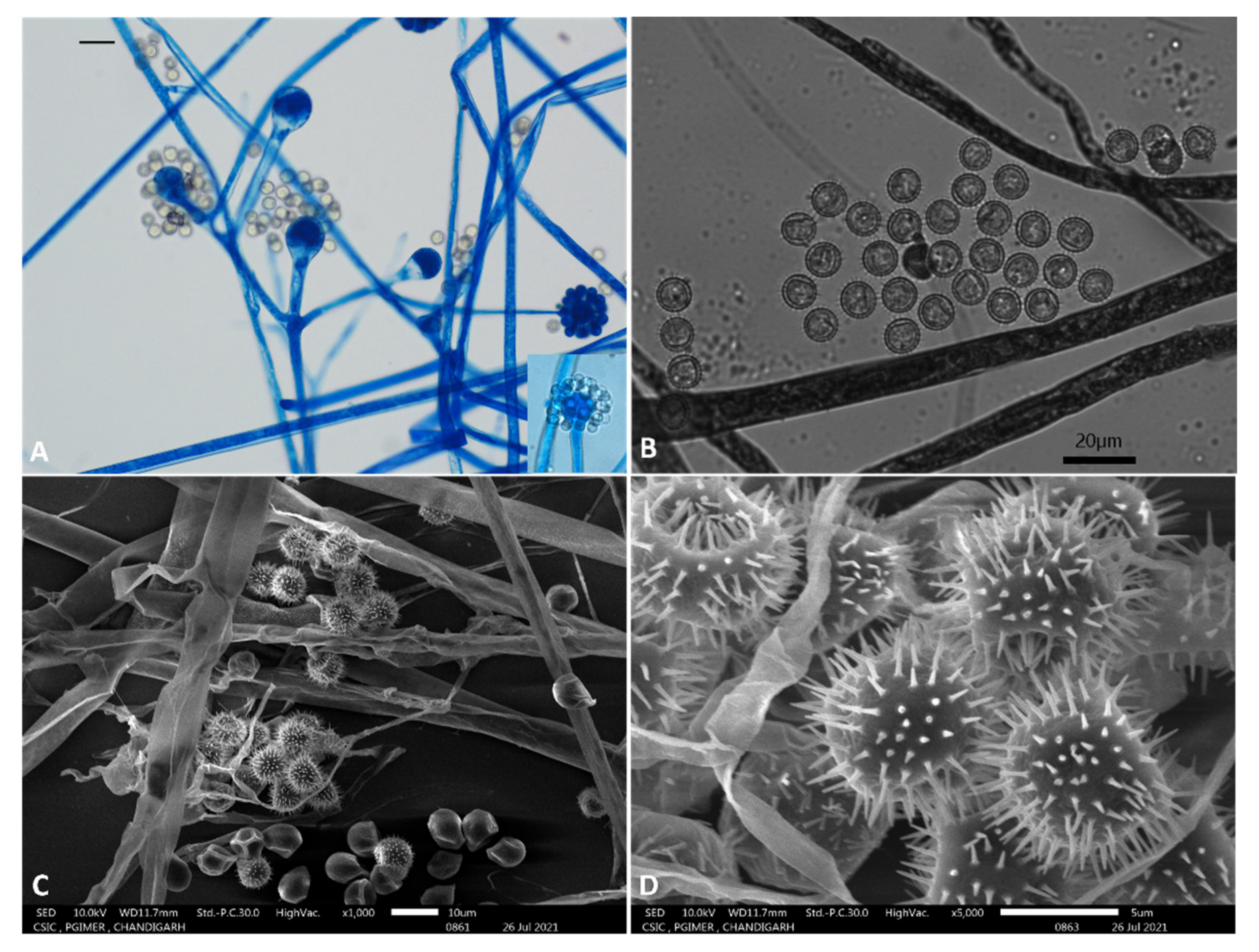
3.4. Taxonomy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prakash, H.; Chakrabarti, A. Epidemiology of Mucormycosis in India. Microorganisms 2021, 9, 523. [Google Scholar] [CrossRef] [PubMed]
- Prakash, H.; Chakrabarti, A. Global Epidemiology of Mucormycosis. J. Fungi 2019, 5, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, W.; Keighley, C.; Wolfe, R.; Lee, W.L.; Slavin, M.A.; Kong, D.C.M.; Chen, S.C. The epidemiology and clinical manifestations of mucormycosis: A systematic review and meta-analysis of case reports. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2019, 25, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Roden, M.M.; Zaoutis, T.E.; Buchanan, W.L.; Knudsen, T.A.; Sarkisova, T.A.; Schaufele, R.L.; Sein, M.; Sein, T.; Chiou, C.C.; Chu, J.H.; et al. Epidemiology and outcome of zygomycosis: A review of 929 reported cases. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2005, 41, 634–653. [Google Scholar] [CrossRef] [Green Version]
- Petraitis, V.; Petraitiene, R.; Antachopoulos, C.; Hughes, J.E.; Cotton, M.P.; Kasai, M.; Harrington, S.; Gamaletsou, M.N.; Bacher, J.D.; Kontoyiannis, D.P.; et al. Increased virulence of Cunninghamella bertholletiae in experimental pulmonary mucormycosis: Correlation with circulating molecular biomarkers, sporangiospore germination and hyphal metabolism. Med. Mycol. 2013, 51, 72–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walther, G.; Wagner, L.; Kurzai, O. Updates on the Taxonomy of Mucorales with an Emphasis on Clinically Important Taxa. J. Fungi 2019, 5, 106. [Google Scholar] [CrossRef] [Green Version]
- Walther, G.; Pawłowska, J.; Alastruey-Izquierdo, A.; Wrzosek, M.; Rodriguez-Tudela, J.L.; Dolatabadi, S.; Chakrabarti, A.; de Hoog, G.S. DNA barcoding in Mucorales: An inventory of biodiversity. Persoonia 2013, 30, 11–47. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Walther, G.; van Diepeningen, A.D.; Gerrits van den Ende, A.H.; Li, R.Y.; Moussa, T.A.; Almaghrabi, O.A.; de Hoog, G.S. DNA barcoding of clinically relevant Cunninghamella species. Med. Mycol. 2015, 53, 99–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.-Y.; Zhao, Y.-X.; Shen, X.; Chen, W.-H.; Han, Y.-F.; Huang, J.-Z.; Liang, Z.-Q. Molecular phylogeny and morphology of Cunninghamella guizhouensis sp. nov. (Cunninghamellaceae, Mucorales), from soil in Guizhou, China. Phytotaxa 2020, 455, 31–39. [Google Scholar] [CrossRef]
- Jillwin, J.; Rudramurthy, S.M.; Singh, S.; Bal, A.; Das, A.; Radotra, B.; Prakash, H.; Dhaliwal, M.; Kaur, H.; Ghosh, A.K.; et al. Molecular identification of pathogenic fungi in formalin-fixed and paraffin-embedded tissues. J. Med. Microbiol. 2021, 70. [Google Scholar] [CrossRef]
- Bialek, R.; Konrad, F.; Kern, J.; Aepinus, C.; Cecenas, L.; Gonzalez, G.M.; Just-Nubling, G.; Willinger, B.; Presterl, E.; Lass-Florl, C.; et al. PCR based identification and discrimination of agents of mucormycosis and aspergillosis in paraffin wax embedded tissue. J. Clin. Pathol. 2005, 58, 1180–1184. [Google Scholar] [CrossRef]
- Alves, E.; Lucas, G.C.; Pozza, E.A.; de Carvalho Alves, M. Scanning Electron Microscopy for Fungal Sample Examination. In Laboratory Protocols in Fungal Biology: Current Methods in Fungal Biology; Gupta, V.K., Tuohy, M.G., Ayyachamy, M., Turner, K.M., O’Donovan, A., Eds.; Springer: New York, NY, USA, 2013; pp. 133–150. [Google Scholar] [CrossRef]
- Prakash, H.; Ghosh, A.K.; Rudramurthy, S.M.; Paul, R.A.; Gupta, S.; Negi, V.; Chakrabarti, A. The environmental source of emerging Apophysomyces variabilis infection in India. Med. Mycol. 2016, 54, 567–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larkin, M.A.; Blackshields, G.; Brown, N.P.; Chenna, R.; McGettigan, P.A.; McWilliam, H.; Valentin, F.; Wallace, I.M.; Wilm, A.; Lopez, R.; et al. Clustal W and Clustal X version 2.0. Bioinformatics 2007, 23, 2947–2948. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Stecher, G.; Tamura, K. MEGA7: Molecular Evolutionary Genetics Analysis Version 7.0 for Bigger Datasets. Mol. Biol. Evol. 2016, 33, 1870–1874. [Google Scholar] [CrossRef] [Green Version]
- Creevey, C.J.; McInerney, J.O. Trees from trees: Construction of phylogenetic supertrees using clann. Methods Mol. Biol. 2009, 537, 139–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bankevich, A.; Nurk, S.; Antipov, D.; Gurevich, A.A.; Dvorkin, M.; Kulikov, A.S.; Lesin, V.M.; Nikolenko, S.I.; Pham, S.; Prjibelski, A.D.; et al. SPAdes: A new genome assembly algorithm and its applications to single-cell sequencing. J. Comput. Biol. A J. Comput. Mol. Cell Biol. 2012, 19, 455–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katoh, K.; Kuma, K.; Miyata, T.; Toh, H. Improvement in the accuracy of multiple sequence alignment program MAFFT. Genome Inform. Int. Conf. Genome Inform. 2005, 16, 22–33. [Google Scholar]
- Capella-Gutierrez, S.; Silla-Martinez, J.M.; Gabaldon, T. trimAl: A tool for automated alignment trimming in large-scale phylogenetic analyses. Bioinformatics 2009, 25, 1972–1973. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.T.; Schmidt, H.A.; von Haeseler, A.; Minh, B.Q. IQ-TREE: A fast and effective stochastic algorithm for estimating maximum-likelihood phylogenies. Mol. Biol. Evol. 2015, 32, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Zeilender, S.; Drenning, D.; Glauser, F.L.; Bechard, D. Fatal Cunninghamella bertholletiae infection in an immunocompetent patient. Chest 1990, 97, 1482–1483. [Google Scholar] [CrossRef] [Green Version]
- Jayasuriya, N.S.; Tilakaratne, W.M.; Amaratunga, E.A.; Ekanayake, M.K. An unusual presentation of rhinofacial zygomycosis due to Cunninghamella sp. in an immunocompetent patient: A case report and literature review. Oral Dis. 2006, 12, 67–69. [Google Scholar] [CrossRef]
- Hirano, T.; Yamada, M.; Sato, K.; Murakami, K.; Tamai, T.; Mitsuhashi, Y.; Tamada, T.; Sugiura, H.; Sato, N.; Saito, R.; et al. Invasive pulmonary mucormycosis: Rare presentation with pulmonary eosinophilia. BMC Pulm. Med. 2017, 17, 76. [Google Scholar] [CrossRef] [Green Version]
- Henriet, S.; Verweij, P.E.; Holland, S.M.; Warris, A. Invasive fungal infections in patients with chronic granulomatous disease. Adv. Exp. Med. Biol. 2013, 764, 27–55. [Google Scholar] [CrossRef]
- Dekkers, R.; Verweij, P.E.; Weemaes, C.M.R.; Severijnen, R.S.V.M.; van Krieken, J.H.J.M.; Warris, A. Gastrointestinal zygomycosis due to Rhizopus microsporus var. rhizopodiformis as a manifestation of chronic granulomatous disease. Med. Mycol. 2008, 46, 491–494. [Google Scholar] [CrossRef] [Green Version]
- Goel, A.; Kini, U.; Shetty, S. Role of histopathology as an aid to prognosis in rhino-orbito-cerebral zygomycosis. Indian J. Pathol. Microbiol. 2010, 53, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Baijal, U.; Mehrotra, B. The genus Cunninghamella: A reassessment. Sydowia 1980, 33, 1–13. [Google Scholar]
- Liu, C.; Liou, G.; Chien, C.Y. New records of the genus Cunninghamella (Mucorales) in Taiwan. Fungal Sci. 2005, 20, 1–9. [Google Scholar]
- Weitzman, I.; Crist, M.Y. Studies with clinical isolates of Cunninghamella II. Physiological and morphological studies. Mycologia 1980, 72, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Wang, H.; Liu, D.; Zhang, J.-N.; Zhao, Y.-H.; Liu, T.-X.; Xin, Z.-H. Isolation of Cunninghamella bigelovii sp.nov. CGMCC 8094 as a new endophytic oleaginous fungus from Salicornia bigelovii. Mycol. Prog. 2015, 14, 11. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Age | Sex | System Involved | Treatment | Clinical Presentation | Species | Outcome |
|---|---|---|---|---|---|---|---|
| USA [21] | 61 | Male | Lungs | Amphotericin B | Invasive pulmonary mucormycosis | C. bertholletiae | Death |
| Sri Lanka [22] | 42 | Male | Sinus and face | Intermittent Amphotericin B | Rhinofacial invasive mucormycosis | Cunninghamella sp. | Cured |
| Japan [23] | 74 | Male | Lungs | Voriconazole + Amphotericin B | Invasive pulmonary mucormycosis | C. bertholletiae | Death |
| Present case | 26 | Male | Face, sinus, and brain | Amphotericin B, Posaconazole, Caspofungin, Terbinafine and Potassium Iodide | Rhinofacial chronic granulamatous invasive mucormycosis | C. arunalokei | Death |
| Name | Colony Color At Maturity | Growth at 40 °C | Terminal Vesicles | Sporangiola | Differentiating Feature |
|---|---|---|---|---|---|
| C. arunalokei | Grey | Restricted | Globose | Translucent to brown, globose, and echinulate | Restricted growth at 40 °C with grey colonies at maturity and presence of brown sporangiola on vesicles ≤ 30 µm [8] |
| C. bertholletiae | Grey | Good | Subglobose to obovate | Translucent to brown, spherical to ellipsoid, rarely tear drop shaped, smooth to punctate | Sporangiophores branching pattern is diverse and sporangiola are tear shaped [8,27] |
| C. blakesleeana | White to light buff | None | Spherical to obovate | Translucent, spherical to ellipsoidal, smooth to echinulate with spines up to 1.6 µm | Opposing suspensors of the zygospores are unequal in size [28]. Finely echinulate to smooth sporangiola borne on solitary or verticillate branches of sporangiophores are reliable character [27]. |
| C. echinulata | White to pale buff | Good | Spherical to subglobose | Translucent, mainly spherical occasionally subglobose to broadly ellipsoidal, studded with spines up to 4 µm | Growth has powdery appearance at 40 °C and sporangiophores branch in pseudo verticillate manner [28] |
| C. elegans | Grey | None | Subglobose to broadly clavate | Translucent to pale brown, spherical to ellipsoidal, smooth to echinulate with spines up to 0.8 µm | Very similar to C. bertholletiae but can be differentiated by absence of growth at 40 °C [29] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hallur, V.; Prakash, H.; Sable, M.; Preetam, C.; Purushotham, P.; Senapati, R.; Shankarnarayan, S.A.; Bag, N.D.; Rudramurthy, S.M. Cunninghamella arunalokei a New Species of Cunninghamella from India Causing Disease in an Immunocompetent Individual. J. Fungi 2021, 7, 670. https://doi.org/10.3390/jof7080670
Hallur V, Prakash H, Sable M, Preetam C, Purushotham P, Senapati R, Shankarnarayan SA, Bag ND, Rudramurthy SM. Cunninghamella arunalokei a New Species of Cunninghamella from India Causing Disease in an Immunocompetent Individual. Journal of Fungi. 2021; 7(8):670. https://doi.org/10.3390/jof7080670
Chicago/Turabian StyleHallur, Vinaykumar, Hariprasath Prakash, Mukund Sable, Chappity Preetam, Prashanth Purushotham, Rabindra Senapati, Shamanth Adekhandi Shankarnarayan, Nerbadyswari Deep Bag, and Shivaprakash Mandya Rudramurthy. 2021. "Cunninghamella arunalokei a New Species of Cunninghamella from India Causing Disease in an Immunocompetent Individual" Journal of Fungi 7, no. 8: 670. https://doi.org/10.3390/jof7080670