
Oral Candidal Colonization in Patients with Different Prosthetic Appliances

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sample Collection
2.3. Determination of Salivary Flow Rate
2.4. Clinical Examination
3. Results
3.1. Participant Demographics
3.2. Oral Candida Colonization
3.3. Identification of Candida Species
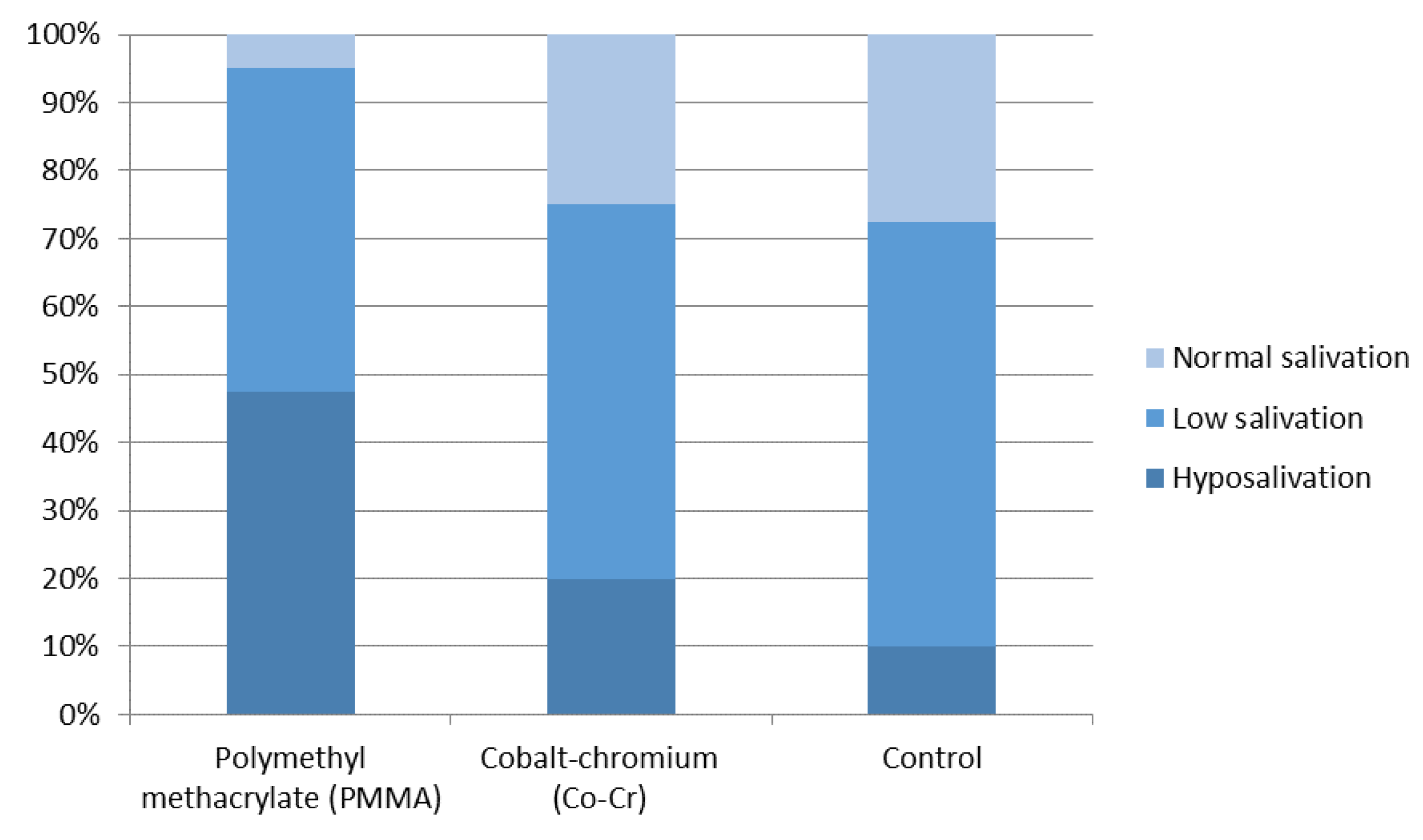
3.4. Salivary Flow Rate
3.5. Clinical Examination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Greendberg, M.; Feagans, M. Burket’s Oral Medicine, 12th ed.; People’s Medical Publishing House: Shelton, CT, USA, 2015; pp. 91–122. [Google Scholar]
- Vila, T.; Sultan, A.S.; Montelongo-Jauregui, D.; Jabra-Rizk, M.A. Oral Candidiasis: A Disease of Opportunity. J. Fungi 2020, 6, 15. [Google Scholar] [CrossRef] [Green Version]
- Hellstein, J.W.; Marek, C.L. Candidiasis: Red and White Manifestations in the Oral Cavity. Head Neck Pathol. 2019, 13, 25–32. [Google Scholar] [CrossRef]
- Gerós-Mesquita, Â.; Carvalho-Pereira, J.; Franco-Duarte, R.; Alves, A. Oral Candida albicans colonization in healthy individuals: Prevalence, genotypic diversity, stability along time and transmissibility. J. Oral. Microbiol. 2020, 12, 1820292. [Google Scholar] [CrossRef] [PubMed]
- Talapko, J.; Juzbašić, M.; Matijević, T.; Pustijanac, E.; Bekić, S.; Kotris, I.; Škrlec, I. Candida albicans-The Virulence Factors and Clinical Manifestations of Infection. J. Fungi 2021, 7, 79. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, C.M.; Bianchi, H.A.; Tadano, T.; Paula, C.R.; Hoffmann-Santos, H.D.; Leite, D.P., Jr.; Hahn, R.C. Factors related to oral candidiasis in elderly users and non-users of removable dental prostheses. Rev. Inst. Med. Trop Sao Paulo 2016, 58, 17. [Google Scholar] [CrossRef] [Green Version]
- Bojang, E.; Ghuman, H.; Kumwenda, P.; Hall, R.A. Immune Sensing of Candida albicans. J. Fungi 2021, 7, 119. [Google Scholar] [CrossRef]
- Nguyen, T.G.; Nguyen, T.T.H.; Tran, Q.W. The incidence of oral candidiasis in patients with diabetes mellitus: A cross-sectional study in Southern Vietnam. J. Crit. Rev. 2020, 7, 82–86. [Google Scholar]
- Khaled, Y.; Pahuja, B.K. Identifying the different kinds of oral candida species in denture wearing patients. EC Dent. Sci. 2019, 18, 1428–1434. [Google Scholar]
- Mardani, M.; Abolghasemi, S.; Darvishnia, D.; Lotfali, E.; Ghasemi, R.; Rabiei, M.M.; Fattahi, A. Oral Candidiasis in Hematological Malignancy Patients: Identification and Antifungal Susceptibility Patterns of Isolates. Jundishapur J. Microbiol. 2020, 13, 103290. [Google Scholar] [CrossRef]
- Aslam, S.; Rotstein, C. Candida infections in solid organ transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, 13623. [Google Scholar] [CrossRef]
- Bansal, R.; Pallagatti, S.; Sheikh, S.; Aggarwal, A.; Gupta, D.; Singh, R. Candidal Species Identification in Malignant and Potentially Malignant Oral Lesions with Antifungal Resistance Patterns. Contemp. Clin. Dent. 2018, 9, 309–313. [Google Scholar] [CrossRef]
- Tooyama, H.; Matsumoto, T.; Hayashi, K.; Kurashina, K.; Kurita, H.; Uchida, M.; Kasuga, E.; Honda, T. Candida concen-trations determined following concentrated oral rinse culture reflect clinical oral signs. BMC Oral Health 2015, 15, 150. [Google Scholar] [CrossRef] [Green Version]
- Sampath, A.; Weerasekera, M.; Dilhari, A.; Gunasekara, C.; Bulugahapitiya, U.; Fernando, N.; Samaranayake, L. Compari-son of duplex PCR and phenotypic analysis in differentiating Candida dubliniensis from Candida albicans from oral samples. AMB Express 2017, 7, 141. [Google Scholar] [CrossRef]
- Ok, S.-M.; Ho, D.; Lynd, T.; Ahn, Y.-W.; Ju, H.-M.; Jeong, S.-H.; Cheon, K. Candida Infection Associated with Salivary Gland—A Narrative Review. J. Clin. Med. 2021, 10, 97. [Google Scholar] [CrossRef] [PubMed]
- Buranarom, N.; Komin, O.; Matangkasombut, O. Hyposalivation, oral health, and Candida colonization in independent dentate elders. PLoS ONE 2020, 15, e0242832. [Google Scholar] [CrossRef] [PubMed]
- Al-Dossary, O.A.E.; Al-Shamahy, H.A. Oral Candida Albicans Colonization in Dental Prosthesis Patients and Individuals with Natural Teeth, Sana’a City, Yemen. J. Sci. Tech. Res. 2018, 11, 8388–8392. [Google Scholar]
- Herbst, D.; Dullabh, H.; Sykes, L.; Vorster, C. Evaluation of surface characteristics of titanium and cobalt chromium implant abutment materials. South Afr. Dent. J. 2013, 68, 350–356. [Google Scholar]
- Alt-Epping, B.; Nejad, R.K.; Jung, K.; Gross, U.; Nauck, F. Symptoms of the oral cavity and their association with local mic-robiological and clinical findings-a prospective survey in palliative care. Support. Care Cancer 2012, 20, 531–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aslani, N.; Janbabaei, G.; Abastabar, M.; Meis, J.F.; Babaeian, M.; Khodavaisy, S.; Boekhout, T.; Badali, H. Identification of uncommon oral yeasts from cancer patients by MALDI-TOF mass spectrometry. BMC Infect. Dis 2018, 18, 24. [Google Scholar] [CrossRef]
- Navazesh, M.; Kumar, S.K. Measuring salivary flow: Challenges and opportunities. J. Am. Dent. Assoc. 2008, 139, 35–40. [Google Scholar] [CrossRef]
- Glazar, I.; Muhvic Urek, M.; Kuis, D.; Prpić, J.; Misković, I.; Kovacevic Pavicic, D.; Pezelj-Ribaric, S. Salivary flow rate, oral yeast colonization and dental status in institutionalized and non-institutionalized elderly. Acta Clin. Croat. 2016, 55, 390–395. [Google Scholar] [CrossRef]
- Mothibe, J.V.; Patel, M. Pathogenic characteristics of Candida albicans isolated from oral cavities of denture wearers and cancer patients wearing oral prostheses. Microb. Pathog. 2017, 110, 128–134. [Google Scholar] [CrossRef]
- Singh, A.; Verma, R.; Murari, A.; Agrawal, A. Oral candidiasis: An overview. J. Oral Maxillofac. Pathol. 2014, 18, 81–85. [Google Scholar]
- Gleiznys, A.; Zdanavičienė, E.; Žilinskas, J. Candida albicans importance to denture wearers. A literature review. Stomatologija 2015, 17, 54–66. [Google Scholar]
- Prakash, B.; Shekar, M.; Maiti, B.; Karunasagar, I.; Padiyath, S. Prevalence of Candida spp. among healthy denture and non denture wearers with respect to hygiene and age. J. Indian Prosthodont Soc. 2015, 15, 29–32. [Google Scholar]
- Nayak, S.; Kavitha, B.; Sriram, G.; Saraswathi, T.R.; Sivapathasundharam, B.; Dorothy, A.L. Comparative study of Candida by conventional and CHROMagar method in non-denture and denture wearers by oral rinse technique. Indian J. Dent. Res. 2012, 23, 490–497. [Google Scholar] [CrossRef]
- Aslanimehr, M.; Rezvani, S.; Mahmoudi, A.; Moosavi, N. Comparison of Candida Albicans Adherence to Conventional Acrylic Denture Base Materials and Injection Molding Acrylic Materials. J. Dent. 2017, 18, 61–64. [Google Scholar]
- Eguia, A.; Arakistain, A.; De-la-Pinta, I.; López-Vicente, J.; Sevillano, E.; Quindós, G.; Eraso, E. Candida albicans biofilms on different materials for manufacturing implant abutments and prostheses. Med. Oral Patol Oral Cir. Bucal 2020, 25, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Taha, E. The Effect of Different Denture Base Materials on Microbial Flora Growth. Curr. Sci. 2017, 6, 314–320. [Google Scholar]
- Gauch, L.; Pedrosa, S.S.; Silveira-Gomes, F.; Esteves, R.A.; Marques-da-Silva, S.H. Isolation of Candida spp. from den-ture-related stomatitis in Pará, Brazil. Braz. J. Microbiol. 2018, 49, 148–151. [Google Scholar]
- Neha, A.; Sumit, B.; Geetika, A.; Tehmeena, Y. Candidiasis-The Most Common Fungal Infection of Oral Cavity. Biomed. J. Sci. Tech. Res. 2018, 8, 6487–6491. [Google Scholar]
- Williams, D.; Lewis, M. Pathogenesis and treatment of oral candidosis. J. Oral Microbiol. 2011, 3, 10–3402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, M.; Jahangiri, L.; Ship, J.A. Hyposalivation, xerostomia and the complete denture: A systematic review. J. Am. Dent. Assoc. 2008, 139, 146–150. [Google Scholar] [CrossRef]
- Brantes, M.F.; Azevedo, R.S.; Rozza-de-Menezes, R.E.; Póvoa, H.C.; Tucci, R.; Gouvêa, A.F.; Takahama Jr, A. Analysis of risk factors for maxillary denture-related oral mucosal lesions: A cross-sectional study. Med. Oral Patol Oral Cir. Buc. 2019, 24, 305–313. [Google Scholar] [CrossRef]
- White, P.L.; Williams, D.W.; Kuriyama, T.; Samad, S.A.; Lewis, M.A.; Barnes, R.A. Detection of Candida in concentrated oral rinse cultures by real-time PCR. J. Clin. Microbiol. 2004, 42, 2101–2107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, M.A.O.; Williams, D.W. Diagnosis and management of oral candidosis. Brit. Dent. J. 2017, 223, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Mohan, S. A study on clinical patterns of mucocutaneous candidiasis in immunosuppressed patients. Int. J. Dermatol. Clin. Res. 2017, 032–034. [Google Scholar]


{kind=link}
| Polymethyl Methacrylate (PMMA) | Cobalt–Chromium (Co–Cr) | Control | p | |
|---|---|---|---|---|
| Subjects (n) | 40 | 40 | 40 | |
| Gender | ||||
| M | 10 | 16 | 14 | 0.78 |
| F | 30 | 24 | 26 | |
| Age | ||||
| Mean ± s.d 1 | 70.22 ± 9.46 | 65.2 ± 7.49 | 60.6 ± 9.61 | 0.09 |
| Number (%) | ||||
|---|---|---|---|---|
| All Denture Wearers | Control | Total | p 1 | |
| Candida spp. | ||||
| Negative | 5 (6.2) | 14 (35) | 19 (15.8) | <0.0001 |
| Positive | 75 (93.8) | 26 (65) | 101 (84.2) | |
| Total | 80 (100) | 40 (100) | 120 (100) |
| Polymethyl Methacrylate (PMMA) | Cobalt–Chromium (Co–Cr) | Control | Total | p 1 | PMMA vs. Control p 2 | Co–Cr vs. Control p 2 | |
|---|---|---|---|---|---|---|---|
| C. albicans | |||||||
| No | 1 (2.5) | 9 (22.5) | 15 (37.5) | 25 (20.8) | 0.001 | <0.001 | 0.22 |
| Yes | 39 (97.5) | 31 (77.5) | 25 (62.5) | 95 (79.2) | |||
| C. krusei | |||||||
| No | 24 (60) | 34 (85) | 37 (92.5) | 95 (79.2) | 0.001 | <0.001 | 0.48 |
| Yes | 16 (40) | 6 (15) | 3 (7.5) | 25 (20.8) | |||
| C. glabrata | |||||||
| No | 37 (92.5) | 35 (87.5) | 37 (92.5) | 109 (90.8) | 0.67 | >0.99 | 0.71 |
| Yes | 3 (7.5) | 5 (12.5) | 3 (7.5) | 11 (9.2) | |||
| C.tropicalis | |||||||
| No | 33 (82.5) | 37 (92.5) | 39 (97.5) | 109 (90.8) | 0.06 | 0.06 | 0.62 |
| Yes | 7 (17,5) | 3 (7,5) | 1 (2,5) | 11 (9,2) | |||
| Candida other spp. | |||||||
| No | 40 (100) | 39 (97.5) | 39 (97.5) | 118 (98.3) | >0.99 | >0.99 | >0.99 |
| Yes | 0 | 1 (2.5) | 1 (2.5) | 2 (1.7) | |||
| Total | 40 (100) | 40 (100) | 40 (100) | 120 (100) |
| Oral Signs and Symptoms | Number (%) Subjects | p 1 | |||
|---|---|---|---|---|---|
| Polymethyl Methacrylate (PMMA) | Cobalt–Chromium (Co–Cr) | Control | Total | ||
| Redness of oral mucosa | |||||
| negative | 24 (60) | 22 (55) | 38 (95) | 84 (70) | <0.001 |
| slight | 13 (32.5) | 13 (32.5) | 2 (5) | 28 (23.3) | |
| moderate | 3 (7.5) | 4 (10) | 0 | 7 (5.8) | |
| severe | 0 | 1 (2.5) | 0 | 1 (0.8) | |
| Redness of the tongue | |||||
| negative | 37 (92.5) | 38 (95) | 40 (100) | 115 (95.8) | 0.37 |
| slight | 3 (7.5) | 2 (5) | 0 | 5 (4.2) | |
| Burning of tongue | |||||
| negative | 25 (62.5) | 34 (85) | 39 (97.5) | 98 (81.7) | <0.001 |
| slight | 4 (10) | 5 (12.5) | 0 | 9 (7.5) | |
| moderate | 7 (17.5) | 1 (2.5) | 1 (2.5) | 9 (7.5) | |
| severe | 4 (10) | 0 | 0 | 4 (3.3) | |
| Taste disorder | |||||
| negative | 38 (95) | 37 (92.5) | 37 (92.5) | 112 (93.3) | >0.99 |
| slight | 1 (2.5) | 2 (5) | 1 (2.5) | 4 (3.3) | |
| moderate | 1 (2.5) | 1 (2.5) | 2 (5) | 4 (3.3) | |
| Coated tongue | |||||
| negative | 26 (65) | 28 (70) | 35 (87.5) | 89 (74.2) | 0.08 |
| slight | 11 (27.5) | 10 (25) | 3 (7.5) | 24 (20) | |
| moderate | 3 (7.5) | 2 (5) | 1 (2.5) | 6 (5) | |
| severe | 0 | 0 | 1 (2.5) | 1 (0.8) | |
| Dry mouth | |||||
| negative | 7 (17.5) | 18 (45) | 32 (80) | 57 (47.5) | <0.001 |
| slight | 20 (50) | 15 (37.5) | 6 (15) | 41 (34.2) | |
| moderate | 10 (25) | 7 (17.5) | 1 (2.5) | 18 (15) | |
| severe | 3 (7.5) | 0 (0) | 1 (2.5) | 4 (3.3) | |
| Total | 40 (100) | 40 (100) | 40 (100) | 120 (100) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinkela Devcic, M.; Simonic-Kocijan, S.; Prpic, J.; Paskovic, I.; Cabov, T.; Kovac, Z.; Glazar, I. Oral Candidal Colonization in Patients with Different Prosthetic Appliances. J. Fungi 2021, 7, 662. https://doi.org/10.3390/jof7080662
Kinkela Devcic M, Simonic-Kocijan S, Prpic J, Paskovic I, Cabov T, Kovac Z, Glazar I. Oral Candidal Colonization in Patients with Different Prosthetic Appliances. Journal of Fungi. 2021; 7(8):662. https://doi.org/10.3390/jof7080662
Chicago/Turabian StyleKinkela Devcic, Maja, Suncana Simonic-Kocijan, Jelena Prpic, Igor Paskovic, Tomislav Cabov, Zoran Kovac, and Irena Glazar. 2021. "Oral Candidal Colonization in Patients with Different Prosthetic Appliances" Journal of Fungi 7, no. 8: 662. https://doi.org/10.3390/jof7080662