
Fungal Endophthalmitis: A Comprehensive Review

Abstract
:1. Introduction
2. Etiologies and Pathogenesis
2.1. Exogenous Endophthalmitis: Overview
2.1.1. Exogenous Endophthalmitis: Traumatic Endophthalmitis
2.1.2. Exogenous Endophthalmitis: Other Surgical and Procedural Causes
2.1.3. Exogenous Endophthalmitis: Keratitis-Associated Endophthalmitis
2.2. Endogenous Endophthalmitis
3. Clinical Presentation
4. Diagnosis
4.1. General Diagnostic Considerations
4.2. Differential Diagnosis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Bacterial Endophthalmitis | Fungal Endophthalmitis |
|---|---|---|
| Frequency and Disease Associations | More common overall [2], and account for the overwhelming majority of post-cataract [2,23,76] and bleb-associated endophthalmitis cases [77] | Less common overall, though accounts for majority of endogenous endophthalmitis cases [2,7,8] |
| Time Course | Rapidly progressive (days) [2] | Indolent (weeks) [2] |
| Characteristic Lesions | Diffuse intraocular inflammation [1,2], subretinal abscess can also occue | Clumped appearance of intraocular inflammation [7], choroidal mass projecting into the vitreous chamber [4,7], chorioretinal creamy-white or “string of pearls” lesions (Candida species) [7,49] |
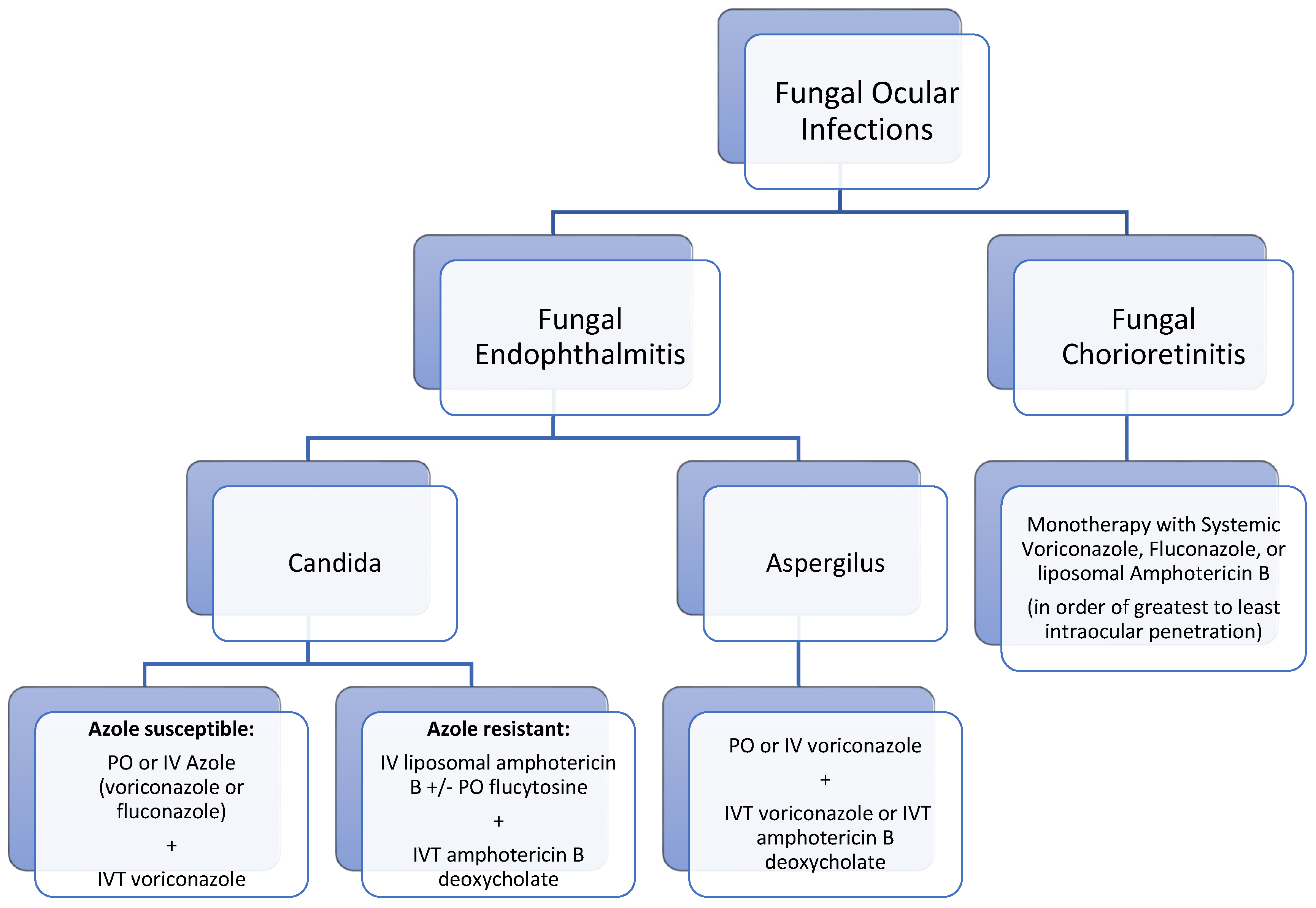
5. Treatment
5.1. Medical Management
5.1.1. Medical Management in Candida Endophthalmitis
5.1.2. Medical Management in Aspergillus Endophthalmitis
5.2. Surgical Management
5.3. Adverse Outcomes in Treatment
6. Visual Prognosis and Complications
6.1. Visual Prognosis
6.2. Complications
7. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Durand, M.L. Endophthalmitis. Clin. Microbiol. Infect. 2013, 19, 227–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durand, M.L. Bacterial and Fungal Endophthalmitis. Clin. Microbiol. Rev. 2017, 30, 597–613. [Google Scholar] [CrossRef] [Green Version]
- Connell, P.P.; O’Neill, E.C.; Fabinyi, D.; Islam, F.M.; Buttery, R.; McCombe, M.; Essex, R.W.; Roufail, E.; Clark, B.; Chiu, D.; et al. Endogenous endophthalmitis: 10-year experience at a tertiary referral centre. Eye 2011, 25, 66–72. [Google Scholar] [CrossRef] [Green Version]
- Kernt, M.; Kampik, A. Endophthalmitis: Pathogenesis, clinical presentation, management, and perspectives. Clin. Ophthalmol. 2010, 4, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Pflugfelder, S.C.; Flynn, H.W., Jr.; Zwickey, T.A.; Forster, R.K.; Tsiligianni, A.; Culbertson, W.W.; Mandelbaum, S. Exogenous fungal endophthalmitis. Ophthalmology 1988, 95, 19–30. [Google Scholar] [CrossRef]
- Sadiq, M.A.; Hassan, M.; Agarwal, A.; Sarwar, S.; Toufeeq, S.; Soliman, M.K.; Hanout, M.; Sepah, Y.J.; Do, D.V.; Nguyen, Q.D. Endogenous endophthalmitis: Diagnosis, management, and prognosis. J. Ophthalmic Inflamm. Infect. 2015, 5, 32. [Google Scholar] [CrossRef] [Green Version]
- Sallam, A.; Lynn, W.; McCluskey, P.; Lightman, S. Endogenous Candida endophthalmitis. Expert Rev. Anti-Infect. Ther. 2006, 4, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Sallam, A.; Taylor, S.R.; Khan, A.; McCluskey, P.; Lynn, W.A.; Manku, K.; Pacheco, P.A.; Lightman, S. Factors determining visual outcome in endogenous Candida endophthalmitis. Retina 2012, 32, 1129–1134. [Google Scholar] [CrossRef] [PubMed]
- Bjerrum, S.S.; la Cour, M. 59 eyes with endogenous endophthalmitis—Causes, outcomes and mortality in a Danish population between 2000 and 2016. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 2023–2027. [Google Scholar] [CrossRef]
- Chee, S.P.; Jap, A. Endogenous endophthalmitis. Curr. Opin. Ophthalmol. 2001, 12, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Shin, Y.U.; Siegel, N.H.; Yu, H.G.; Sobrin, L.; Patel, A.; Durand, M.L.; Miller, J.W.; Husain, D. Endogenous Endophthalmitis in the American and Korean Population: An 8-year Retrospective Study. Ocul. Immunol. Inflamm. 2018, 26, 496–503. [Google Scholar] [CrossRef]
- Lim, H.W.; Shin, J.W.; Cho, H.Y.; Kim, H.K.; Kang, S.W.; Song, S.J.; Yu, H.G.; Oh, J.R.; Kim, J.S.; Moon, S.W.; et al. Endogenous endophthalmitis in the Korean population: A six-year retrospective study. Retina 2014, 34, 592–602. [Google Scholar] [CrossRef]
- Luong, P.M.; Tsui, E.; Batra, N.N.; Zegans, M.E. Endogenous endophthalmitis and other ocular manifestations of injection drug use. Curr. Opin. Ophthalmol. 2019, 30, 506–512. [Google Scholar] [CrossRef]
- Ness, T.; Pelz, K.; Hansen, L.L. Endogenous endophthalmitis: Microorganisms, disposition and prognosis. Acta Ophthalmol. Scand. 2007, 85, 852–856. [Google Scholar] [CrossRef]
- Rychener, R.O. Intra-Ocular Mycosis. Trans. Am. Ophthalmol. Soc. 1933, 31, 477–496. [Google Scholar] [PubMed]
- McCannel, C.A. Meta-analysis of endophthalmitis after intravitreal injection of anti-vascular endothelial growth factor agents: Causative organisms and possible prevention strategies. Retina 2011, 31, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Wykoff, C.C.; Flynn, H.W., Jr.; Miller, D.; Scott, I.U.; Alfonso, E.C. Exogenous fungal endophthalmitis: Microbiology and clinical outcomes. Ophthalmology 2008, 115, 1501–1507. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.A.; Sridhar, J.; Miller, D.; Wykoff, C.C.; Flynn, H.W., Jr. Exogenous fungal endophthalmitis: An analysis of isolates and susceptibilities to antifungal agents over a 20-year period (1990–2010). Am. J. Ophthalmol. 2015, 159, 257–264.e251. [Google Scholar] [CrossRef]
- Bhagat, N.; Nagori, S.; Zarbin, M. Post-traumatic Infectious Endophthalmitis. Surv. Ophthalmol. 2011, 56, 214–251. [Google Scholar] [CrossRef]
- Tan, C.L.; McGuinness, M.B.; Essex, R.; Dawkins, R.C.H.; Allen, P.J. Post-traumatic endophthalmitis: A novel risk scoring system identifying high risk open globe injuries. Clin. Exp. Ophthalmol. 2021, 49, 757–759. [Google Scholar] [CrossRef]
- Essex, R.W.; Yi, Q.; Charles, P.G.; Allen, P.J. Post-traumatic endophthalmitis. Ophthalmology 2004, 111, 2015–2022. [Google Scholar] [CrossRef]
- Long, C.; Liu, B.; Xu, C.; Jing, Y.; Yuan, Z.; Lin, X. Causative organisms of post-traumatic endophthalmitis: A 20-year retrospective study. BMC Ophthalmol. 2014, 14, 34. [Google Scholar] [CrossRef] [Green Version]
- Mollan, S.P.; Gao, A.; Lockwood, A.; Durrani, O.M.; Butler, L. Postcataract endophthalmitis: Incidence and microbial isolates in a United Kingdom region from 1996 through 2004. J. Cataract Refract. Surg. 2007, 33, 265–268. [Google Scholar] [CrossRef]
- Keay, L.; Gower, E.W.; Cassard, S.D.; Tielsch, J.M.; Schein, O.D. Postcataract surgery endophthalmitis in the United States: Analysis of the complete 2003 to 2004 Medicare database of cataract surgeries. Ophthalmology 2012, 119, 914–922. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Gupta, V.; Gupta, A.; Dogra, M.R.; Pandav, S.S.; Ray, P.; Chakraborty, A. Spectrum and clinical profile of post cataract surgery endophthalmitis in north India. Indian J. Ophthalmol. 2003, 51, 139–145. [Google Scholar] [PubMed]
- Narang, S.; Gupta, A.; Gupta, V.; Dogra, M.R.; Ram, J.; Pandav, S.S.; Chakrabarti, A. Fungal endophthalmitis following cataract surgery: Clinical presentation, microbiological spectrum, and outcome. Am. J. Ophthalmol. 2001, 132, 609–617. [Google Scholar] [CrossRef]
- Taban, M.; Behrens, A.; Newcomb, R.L.; Nobe, M.Y.; McDonnell, P.J. Incidence of acute endophthalmitis following penetrating keratoplasty: A systematic review. Arch. Ophthalmol. 2005, 123, 605–609. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.Y.; Jones, M.N.; Srinivasan, S.; Neal, T.J.; Armitage, W.J.; Kaye, S.B.; Group, N.O.T.A.; Contributing, O. Endophthalmitis after penetrating keratoplasty. Ophthalmology 2015, 122, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Keyhani, K.; Seedor, J.A.; Shah, M.K.; Terraciano, A.J.; Ritterband, D.C. The incidence of fungal keratitis and endophthalmitis following penetrating keratoplasty. Cornea 2005, 24, 288–291. [Google Scholar] [CrossRef]
- Wang, S.Y.; Ghodasra, D.H.; Amin, S.R.; Mian, S.I.; Jayasundera, K.T. Fungal Endophthalmitis Associated with DSAEK and Thermal Sclerostomy. Ophthalmic Surg. Lasers Imaging Retina 2016, 47, 691–693. [Google Scholar] [CrossRef]
- Chew, A.C.; Mehta, J.S.; Li, L.; Busmanis, I.; Tan, D.T. Fungal endophthalmitis after descemet stripping automated endothelial keratoplasty—A case report. Cornea 2010, 29, 346–349. [Google Scholar] [CrossRef] [PubMed]
- Kitazawa, K.; Wakimasu, K.; Yoneda, K.; Iliakis, B.; Sotozono, C.; Kinoshita, S. A case of fungal keratitis and endophthalmitis post penetrating keratoplasty resulting from fungal contamination of the donor cornea. Am. J. Ophthalmol. Case Rep. 2017, 5, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Moshfeghi, A.A.; Rosenfeld, P.J.; Flynn, H.W., Jr.; Schwartz, S.G.; Davis, J.L.; Murray, T.G.; Smiddy, W.E.; Berrocal, A.M.; Dubovy, S.R.; Lee, W.H.; et al. Endophthalmitis after intravitreal vascular [corrected] endothelial growth factor antagonists: A six-year experience at a university referral center. Retina 2011, 31, 662–668. [Google Scholar] [CrossRef]
- Tabandeh, H.; Boscia, F.; Sborgia, A.; Ciraci, L.; Dayani, P.; Mariotti, C.; Furino, C.; Flynn, H.W., Jr. Endophthalmitis associated with intravitreal injections: Office-based setting and operating room setting. Retina 2014, 34, 18–23. [Google Scholar] [CrossRef]
- Sheyman, A.T.; Cohen, B.Z.; Friedman, A.H.; Ackert, J.M. An outbreak of fungal endophthalmitis after intravitreal injection of compounded combined bevacizumab and triamcinolone. JAMA Ophthalmol. 2013, 131, 864–869. [Google Scholar] [CrossRef] [Green Version]
- Narita, A.; Seguchi, J.; Shiraga, F. Paecilomyces lilacinus-induced Scleritis Following Bleb-associated Endophthalmitis after Trabeculectomy. Acta Med. Okayama 2015, 69, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Ruesch, R.; Buchi, E.R.; Bischoff, P.; Schneider, P. Pseudallescheria boydii fungal endophthalmitis. 6 years after trabeculectomy. Klin. Monbl. Augenheilkd. 1994, 204, 468–469. [Google Scholar] [CrossRef]
- Green, M.; Apel, A.; Stapleton, F. Risk factors and causative organisms in microbial keratitis. Cornea 2008, 27, 22–27. [Google Scholar] [CrossRef]
- Ritterband, D.C.; Seedor, J.A.; Shah, M.K.; Koplin, R.S.; McCormick, S.A. Fungal keratitis at the new york eye and ear infirmary. Cornea 2006, 25, 264–267. [Google Scholar] [CrossRef]
- Sirikul, T.; Prabriputaloong, T.; Smathivat, A.; Chuck, R.S.; Vongthongsri, A. Predisposing factors and etiologic diagnosis of ulcerative keratitis. Cornea 2008, 27, 283–287. [Google Scholar] [CrossRef]
- Acharya, M.; Farooqui, J.H.; Gaba, T.; Gandhi, A.; Mathur, U. Delhi Infectious Keratitis Study: Update on Clinico-Microbiological Profile and Outcomes of Infectious Keratitis. J. Curr. Ophthalmol. 2020, 32, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Gopinathan, U.; Garg, P.; Fernandes, M.; Sharma, S.; Athmanathan, S.; Rao, G.N. The epidemiological features and laboratory results of fungal keratitis: A 10-year review at a referral eye care center in South India. Cornea 2002, 21, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.; Sridhar, M.S.; Murthy, S.; Sharma, S. Clinical and microbiological profile of microsporidial keratoconjunctivitis in southern India. Ophthalmology 2006, 113, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Wan, L.; Cheng, J.; Zhang, J.; Chen, N.; Gao, Y.; Xie, L.X. Risk Factors, Treatment Strategies, and Outcomes of Endophthalmitis Associated with Severe Fungal Keratitis. Retina 2019, 39, 1076–1082. [Google Scholar] [CrossRef]
- Xie, L.; Zhong, W.; Shi, W.; Sun, S. Spectrum of fungal keratitis in north China. Ophthalmology 2006, 113, 1943–1948. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Sun, S.; Jing, Y.; Han, L.; Zhang, H.; Yue, J. Spectrum of fungal keratitis in central China. Clin. Exp. Ophthalmol. 2009, 37, 763–771. [Google Scholar] [CrossRef] [PubMed]
- An, N.; Liu, X.N.; Wang, Y.N.; Zhu, J.L.; Yang, H.; Wu, J.; Yang, X.Z.; Zhu, X.P. The pathogenic spectrum of fungal keratitis in northwestern China. Int. J. Ophthalmol. 2016, 9, 1846–1848. [Google Scholar] [CrossRef]
- Breazzano, M.P. Choroidal origin of endogenous Candida endophthalmitis. BMC Ophthalmol. 2020, 20, 283. [Google Scholar] [CrossRef]
- Siddiqui, M.Z.; Gebhard, G.M.; Ahmad, K.T.; Sallam, A.B.; Rosenbaum, E.R.; Uwaydat, S.H. Incidence of chorioretinitis and endophthalmitis in hospitalized patients with fungemia. Eye 2021, in press. [Google Scholar] [CrossRef]
- Verduyn Lunel, F.M.; Meis, J.F.; Voss, A. Nosocomial fungal infections: Candidemia. Diagn. Microbiol. Infect. Dis. 1999, 34, 213–220. [Google Scholar] [CrossRef]
- Pulimood, S.; Ganesan, L.; Alangaden, G.; Chandrasekar, P. Polymicrobial candidemia. Diagn. Microbiol. Infect. Dis. 2002, 44, 353–357. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Shivaprakash, M.R.; Singh, R.; Tarai, B.; George, V.K.; Fomda, B.A.; Gupta, A. Fungal endophthalmitis: Fourteen years’ experience from a center in India. Retina 2008, 28, 1400–1407. [Google Scholar] [CrossRef] [PubMed]
- Mir, T.A.; Papudesu, C.; Fang, W.; Hinkle, D.M. Incidence of Drug Use-Related Endogenous Endophthalmitis Hospitalizations in the United States, 2003 to 2016. JAMA Ophthalmol. 2021, 139, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Danielescu, C.; Anton, N.; Stanca, H.T.; Munteanu, M. Endogenous Endophthalmitis: A Review of Case Series Published between 2011 and 2020. J. Ophthalmol. 2020, 2020, 8869590. [Google Scholar] [CrossRef] [PubMed]
- Baley, J.E.; Annable, W.L.; Kliegman, R.M. Candida endophthalmitis in the premature infant. J. Pediatr. 1981, 98, 458–461. [Google Scholar] [CrossRef]
- Shroff, D.; Narula, R.; Atri, N.; Chakravarti, A.; Gandhi, A.; Sapra, N.; Bhatia, G.; Pawar, S.R.; Narain, S. Endogenous fungal endophthalmitis following intensive corticosteroid therapy in severe COVID-19 disease. Indian J. Ophthalmol. 2021, 69, 1909–1914. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.K.; Venkatramani, D.; Majumder, P.D. A case series of presumed fungal endogenous endophthalmitis in post COVID-19 patients. Indian J. Ophthalmol. 2021, 69, 1322–1325. [Google Scholar] [CrossRef] [PubMed]
- Binder, M.I.; Chua, J.; Kaiser, P.K.; Procop, G.W.; Isada, C.M. Endogenous endophthalmitis: An 18-year review of culture-positive cases at a tertiary care center. Medicine 2003, 82, 97–105. [Google Scholar] [CrossRef]
- Tirpack, A.R.; Duker, J.S.; Baumal, C.R. An Outbreak of Endogenous Fungal Endophthalmitis Among Intravenous Drug Abusers in New England. JAMA Ophthalmol. 2017, 135, 534–540. [Google Scholar] [CrossRef] [Green Version]
- Modjtahedi, B.S.; Finn, A.P.; Papakostas, T.D.; Durand, M.; Husain, D.; Eliott, D. Intravenous Drug Use-Associated Endophthalmitis. Ophthalmol. Retina 2017, 1, 192–199. [Google Scholar] [CrossRef]
- Gonzales, C.A.; Scott, I.U.; Chaudhry, N.A.; Luu, K.M.; Miller, D.; Murray, T.G.; Davis, J.L. Endogenous endophthalmitis caused by Histoplasma capsulatum var. capsulatum: A case report and literature review. Ophthalmology 2000, 107, 725–729. [Google Scholar] [CrossRef]
- Jackson, T.L.; Eykyn, S.J.; Graham, E.M.; Stanford, M.R. Endogenous bacterial endophthalmitis: A 17-year prospective series and review of 267 reported cases. Surv. Ophthalmol. 2003, 48, 403–423. [Google Scholar] [CrossRef]
- Au, L.; Guduru, K.; Lipscomb, G.; Kelly, S.P. Candida endophthalmitis: A critical diagnosis in the critically ill. Clin. Ophthalmol. 2007, 1, 551–554. [Google Scholar]
- Baker, A.; Durand, M. The Endophthalmitis Vitrectomy Study. Arch. Ophthalmol. 1996, 114, 1025–1026, author reply 1026–1027. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, D.S.; Flynn, H.W., Jr. Endophthalmitis after penetrating ocular trauma. Curr. Opin. Ophthalmol. 1997, 8, 32–38. [Google Scholar] [CrossRef]
- Rao, N.A.; Hidayat, A. A comparative clinicopathologic study of endogenous mycotic endophthalmitis: Variations in clinical and histopathologic changes in candidiasis compared to aspergillosis. Trans. Am. Ophthalmol. Soc. 2000, 98, 183–193, discussion 193–184. [Google Scholar]
- Spadea, L.; Giannico, M.I. Diagnostic and Management Strategies of Aspergillus Endophthalmitis: Current Insights. Clin. Ophthalmol. 2019, 13, 2573–2582. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, M.; Kobayashi, Y.; Takebayashi, H.; Kiyokawa, M.; Qiu, H. Analysis of predisposing clinical and laboratory findings for the development of endogenous fungal endophthalmitis. A retrospective 12-year study of 79 eyes of 46 patients. Retina 2001, 21, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Anand, A.; Madhavan, H.; Neelam, V.; Lily, T. Use of polymerase chain reaction in the diagnosis of fungal endophthalmitis. Ophthalmology 2001, 108, 326–330. [Google Scholar] [CrossRef]
- Sandhu, H.S.; Hajrasouliha, A.; Kaplan, H.J.; Wang, W. Diagnostic Utility of Quantitative Polymerase Chain Reaction versus Culture in Endophthalmitis and Uveitis. Ocul. Immunol. Inflamm. 2019, 27, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Okada, A.A.; Johnson, R.P.; Liles, W.C.; D’Amico, D.J.; Baker, A.S. Endogenous bacterial endophthalmitis. Report of a ten-year retrospective study. Ophthalmology 1994, 101, 832–838. [Google Scholar] [CrossRef]
- Davis, J.L. Diagnostic dilemmas in retinitis and endophthalmitis. Eye 2012, 26, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.J.; Wu, W.C.; Sun, M.H.; Lai, C.C.; Chao, A.N. Endogenous fungal endophthalmitis: Causative organisms, management strategies, and visual acuity outcomes. Am. J. Ophthalmol. 2012, 154, 213–214, author reply 214. [Google Scholar] [CrossRef]
- Shen, X.; Xu, G. Vitrectomy for endogenous fungal endophthalmitis. Ocul. Immunol. Inflamm. 2009, 17, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Schiedler, V.; Scott, I.U.; Flynn, H.W., Jr.; Davis, J.L.; Benz, M.S.; Miller, D. Culture-proven endogenous endophthalmitis: Clinical features and visual acuity outcomes. Am. J. Ophthalmol. 2004, 137, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Keay, L.J.; Gower, E.W.; Iovieno, A.; Oechsler, R.A.; Alfonso, E.C.; Matoba, A.; Colby, K.; Tuli, S.S.; Hammersmith, K.; Cavanagh, D.; et al. Clinical and microbiological characteristics of fungal keratitis in the United States, 2001–2007: A multicenter study. Ophthalmology 2011, 118, 920–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ba’arah, B.T.; Smiddy, W.E. Bleb-related Endophthalmitis: Clinical Presentation, Isolates, Treatment and Visual Outcome of Culture-proven Cases. Middle East Afr. J. Ophthalmol. 2009, 16, 20–24. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, H.; Miyazaki, Y.; Geber, A.; Parkinson, T.; Hitchcock, C.; Falconer, D.J.; Ward, D.J.; Marsden, K.; Bennett, J.E. Fluconazole resistance associated with drug efflux and increased transcription of a drug transporter gene, PDH1, in Candida glabrata. Antimicrob. Agents Chemother. 1998, 42, 1695–1701. [Google Scholar] [CrossRef] [Green Version]
- Anderson, M.Z.; Saha, A.; Haseeb, A.; Bennett, R.J. A chromosome 4 trisomy contributes to increased fluconazole resistance in a clinical isolate of Candida albicans. Microbiology 2017, 163, 856–865. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.A.; Slain, D.; Khakoo, R.A. Candida endophthalmitis: Focus on current and future antifungal treatment options. Pharmacotherapy 2007, 27, 1711–1721. [Google Scholar] [CrossRef]
- Nguyen, M.H.; Yu, C.Y. Voriconazole against fluconazole-susceptible and resistant candida isolates: In-vitro efficacy compared with that of itraconazole and ketoconazole. J. Antimicrob. Chemother. 1998, 42, 253–256. [Google Scholar] [CrossRef] [Green Version]
- Fukuoka, T.; Johnston, D.A.; Winslow, C.A.; de Groot, M.J.; Burt, C.; Hitchcock, C.A.; Filler, S.G. Genetic basis for differential activities of fluconazole and voriconazole against Candida krusei. Antimicrob. Agents Chemother. 2003, 47, 1213–1219. [Google Scholar] [CrossRef] [Green Version]
- Adam, M.K.; Vahedi, S.; Nichols, M.M.; Fintelmann, R.E.; Keenan, J.D.; Garg, S.J.; Hsu, J.; Maguire, J.I.; Spirn, M.J. Inpatient Ophthalmology Consultation for Fungemia: Prevalence of Ocular Involvement and Necessity of Funduscopic Screening. Am. J. Ophthalmol. 2015, 160, 1078–1083.e1072. [Google Scholar] [CrossRef]
- Brooks, R.G. Prospective study of Candida endophthalmitis in hospitalized patients with candidemia. Arch. Intern. Med. 1989, 149, 2226–2228. [Google Scholar] [CrossRef] [PubMed]
- Breazzano, M.P.; Bond, J.B., 3rd; Bearelly, S.; Kim, D.H.; Donahue, S.P.; Lum, F.; Olsen, T.W.; American Academy of Ophthalmology. American Academy of Ophthalmology Recommendations on Screening for Endogenous Candida endophthalmitis. Ophthalmology 2021, in press. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef] [PubMed]
- Goldblum, D.; Rohrer, K.; Frueh, B.E.; Theurillat, R.; Thormann, W.; Zimmerli, S. Ocular distribution of intravenously administered lipid formulations of amphotericin B in a rabbit model. Antimicrob. Agents Chemother. 2002, 46, 3719–3723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, J.E., Jr.; Foos, R.Y.; Montgomerie, J.Z.; Guze, L.B. Ocular manifestations of Candida septicemia: Review of seventy-six cases of hematogenous Candida endophthalmitis. Medicine 1974, 53, 47–75. [Google Scholar] [CrossRef]
- Akler, M.E.; Vellend, H.; McNeely, D.M.; Walmsley, S.L.; Gold, W.L. Use of fluconazole in the treatment of candidal endophthalmitis. Clin. Infect. Dis. 1995, 20, 657–664. [Google Scholar] [CrossRef]
- Rex, J.H.; Bennett, J.E.; Sugar, A.M.; Pappas, P.G.; van der Horst, C.M.; Edwards, J.E.; Washburn, R.G.; Scheld, W.M.; Karchmer, A.W.; Dine, A.P.; et al. A randomized trial comparing fluconazole with amphotericin B for the treatment of candidemia in patients without neutropenia. Candidemia Study Group and the National Institute. N. Engl. J. Med. 1994, 331, 1325–1330. [Google Scholar] [CrossRef]
- Filler, S.G.; Crislip, M.A.; Mayer, C.L.; Edwards, J.E., Jr. Comparison of fluconazole and amphotericin B for treatment of disseminated candidiasis and endophthalmitis in rabbits. Antimicrob. Agents Chemother. 1991, 35, 288–292. [Google Scholar] [CrossRef] [Green Version]
- Breit, S.M.; Hariprasad, S.M.; Mieler, W.F.; Shah, G.K.; Mills, M.D.; Grand, M.G. Management of endogenous fungal endophthalmitis with voriconazole and caspofungin. Am. J. Ophthalmol. 2005, 139, 135–140. [Google Scholar] [CrossRef]
- Majji, A.B.; Jalali, S.; Das, T.; Gopinathan, U. Role of intravitreal dexamethasone in exogenous fungal endophthalmitis. Eye 1999, 13 Pt 5, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Coats, M.L.; Peyman, G.A. Intravitreal corticosteroids in the treatment of exogenous fungal endophthalmitis. Retina 1992, 12, 46–51. [Google Scholar] [CrossRef]
- Patterson, T.F.; Thompson, G.R., 3rd; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef] [PubMed]
- Dave, V.P.; Pappuru, R.R.; Pathengay, A.; Gupta, R.; Joseph, J.; Sharma, S.; Das, T. Aspergillus Endophthalmitis: Clinical Presentations and Factors Determining Outcomes. Asia-Pac. J. Ophthalmol. 2020, 9, 9–13. [Google Scholar] [CrossRef]
- Danielescu, C.; Cantemir, A.; Chiselita, D. Successful treatment of fungal endophthalmitis using intravitreal caspofungin. Arq. Bras. Oftalmol. 2017, 80, 196–198. [Google Scholar] [CrossRef]
- Yoshida, M.; Kiyota, N.; Maruyama, K.; Kunikata, H.; Toyokawa, M.; Hagiwara, S.; Makimura, K.; Sato, N.; Taniuchi, S.; Nakazawa, T. Endogenous Fusarium Endophthalmitis During Treatment for Acute Myeloid Leukemia, Successfully Treated with 25-Gauge Vitrectomy and Antifungal Medications. Mycopathologia 2018, 183, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Alves da Costa Pertuiset, P.A.; Logrono, J.F. Fusarium Endophthalmitis following cataract Surgery: Successful Treatment with Intravitreal and Systemic Voriconazole. Case Rep. Ophthalmol. Med. 2016, 2016, 4593042. [Google Scholar] [CrossRef] [Green Version]
- Rizzello, I.; Castagnetti, F.; Toschi, P.G.; Bertaccini, P.; Primavera, L.; Paolucci, M.; Faccioli, L.; Spinardi, L.; Lewis, R.E.; Cavo, M.; et al. Successful treatment of bilateral endogenous Fusarium solani endophthalmitis in a patient with acute lymphocytic leukaemia. Mycoses 2018, 61, 53–60. [Google Scholar] [CrossRef]
- Behera, U.C.; Budhwani, M.; Das, T.; Basu, S.; Padhi, T.R.; Barik, M.R.; Sharma, S. Role of Early Vitrectomy in the Treatment of Fungal Endophthalmitis. Retina 2018, 38, 1385–1392. [Google Scholar] [CrossRef]
- Celiker, H.; Kazokoglu, H. The role of pars plana vitrectomy in the management of fungal endogenous endophthalmitis. Eur. J. Ophthalmol. 2020, 30, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Ghoraba, H.H.; Ellakwa, A.F.; Elgemai, E.M.; Mansour, H.O.; Heikal, M.A. Results of Pars Plana Vitrectomy for the Management of Endogenous Fungal Endophthalmitis after Urinary Tract Procedures. Retin. Cases Brief. Rep. 2017, 11, 171–174. [Google Scholar] [CrossRef]
- Thomas, B.J.; Mehta, N.; Yonekawa, Y.; Sridhar, J.; Kuriyan, A.E.; Relhan, N.; Liang, M.C.; Woodward, M.A.; Witkin, A.J.; Shah, C.; et al. Pars plana vitrectomy for late vitreoretinal sequelae of infectious endophthalmitis: Surgical Management and Outcomes. Retina 2017, 37, 651–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamill, R.J. Amphotericin B formulations: A comparative review of efficacy and toxicity. Drugs 2013, 73, 919–934. [Google Scholar] [CrossRef]
- Laniado-Laborin, R.; Cabrales-Vargas, M.N. Amphotericin B: Side effects and toxicity. Rev. Iberoam. Micol. 2009, 26, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Wade, R.L.; Chaudhari, P.; Natoli, J.L.; Taylor, R.J.; Nathanson, B.H.; Horn, D.L. Nephrotoxicity and other adverse events among inpatients receiving liposomal amphotericin B or amphotericin B lipid complex. Diagn. Microbiol. Infect. Dis. 2013, 76, 361–367. [Google Scholar] [CrossRef]
- Slain, D. Lipid-based amphotericin B for the treatment of fungal infections. Pharmacotherapy 1999, 19, 306–323. [Google Scholar] [CrossRef]
- Thompson, G.R., 3rd; Lewis, J.S., 2nd. Pharmacology and clinical use of voriconazole. Expert Opin. Drug Metab. Toxicol. 2010, 6, 83–94. [Google Scholar] [CrossRef]
- Aksoy, F.; Akdogan, E.; Aydin, K.; Yilmaz, M.; Altunayoglu, V.; Sozen, E.E.; Omay, S.B.; Koksal, I. Voriconazole-induced neuropathy. Chemotherapy 2008, 54, 224–227. [Google Scholar] [CrossRef]
- Solis-Munoz, P.; Lopez, J.C.; Bernal, W.; Willars, C.; Verma, A.; Heneghan, M.A.; Wendon, J.; Auzinger, G. Voriconazole hepatotoxicity in severe liver dysfunction. J. Infect. 2013, 66, 80–86. [Google Scholar] [CrossRef]
- Matsumoto, K.; Ikawa, K.; Abematsu, K.; Fukunaga, N.; Nishida, K.; Fukamizu, T.; Shimodozono, Y.; Morikawa, N.; Takeda, Y.; Yamada, K. Correlation between voriconazole trough plasma concentration and hepatotoxicity in patients with different CYP2C19 genotypes. Int. J. Antimicrob. Agents 2009, 34, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.D.; den Hollander, J.G.; van der Holt, B.; Rijnders, B.J.; van Vliet, M.; Sonneveld, P.; van Schaik, R.H. Hepatotoxicity of oral and intravenous voriconazole in relation to cytochrome P450 polymorphisms. J. Antimicrob. Chemother. 2007, 60, 1104–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashbee, H.R.; Barnes, R.A.; Johnson, E.M.; Richardson, M.D.; Gorton, R.; Hope, W.W. Therapeutic drug monitoring (TDM) of antifungal agents: Guidelines from the British Society for Medical Mycology. J. Antimicrob. Chemother. 2014, 69, 1162–1176. [Google Scholar] [CrossRef] [Green Version]
- William, A.; Spitzer, M.S.; Deuter, C.; Blumenstock, G.; Partsch, M.; Voykov, B.; Ziemssen, F.; Bartz-Schmidt, K.U.; Doycheva, D. Outcomes of Primary Transconjunctival 23-Gauge Vitrectomy in the Diagnosis and Treatment of Presumed Endogenous Fungal Endophthalmitis. Ocul. Immunol. Inflamm. 2017, 25, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Weishaar, P.D.; Flynn, H.W., Jr.; Murray, T.G.; Davis, J.L.; Barr, C.C.; Gross, J.G.; Mein, C.E.; McLean, W.C., Jr.; Killian, J.H. Endogenous Aspergillus endophthalmitis. Clinical features and treatment outcomes. Ophthalmology 1998, 105, 57–65. [Google Scholar] [CrossRef]
- Naoi, N.; Sawada, A. Effect of vitrectomy on epiretinal membranes after endogenous fungal endophthalmitis. Jpn. J. Ophthalmol. 1996, 40, 434–438. [Google Scholar]






| Organism | Number (%) |
|---|---|
| Total Fungi | 60 (100%) |
| Aspergillus fumigatus | 11 (18.3%) |
| Aspergillus nidulans | 7 (11.7%) |
| Aspergillus niger | 6 (10%) |
| Aspergillus flavus | 2 (3.3%) |
| Fusarium solani | 5 (8.3%) |
| Fusarium equiseti | 1 (1.7%) |
| Fusarium moniliforme | 1 (1.7%) |
| Bipolaris sorodiana | 4 (6.7%) |
| Curvularia geniculate | 2 (3.3%) |
| Conidia | 2 (3.3%) |
| Penicilium | 1 (1.7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haseeb, A.A.; Elhusseiny, A.M.; Siddiqui, M.Z.; Ahmad, K.T.; Sallam, A.B. Fungal Endophthalmitis: A Comprehensive Review. J. Fungi 2021, 7, 996. https://doi.org/10.3390/jof7110996
Haseeb AA, Elhusseiny AM, Siddiqui MZ, Ahmad KT, Sallam AB. Fungal Endophthalmitis: A Comprehensive Review. Journal of Fungi. 2021; 7(11):996. https://doi.org/10.3390/jof7110996
Chicago/Turabian StyleHaseeb, Abid A., Abdelrahman M. Elhusseiny, Mohammad Z. Siddiqui, Kinza T. Ahmad, and Ahmed B. Sallam. 2021. "Fungal Endophthalmitis: A Comprehensive Review" Journal of Fungi 7, no. 11: 996. https://doi.org/10.3390/jof7110996