Urine Sediment Findings and the Immune Response to Pathologies in Fungal Urinary Tract Infections Caused by Candida spp.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Fungal Urinary Tract Infection
3. Definition and Diagnosis of Candiduria and UTI Caused by Candida spp.
3.1. Urinalysis
3.1.1. Urinary Particles
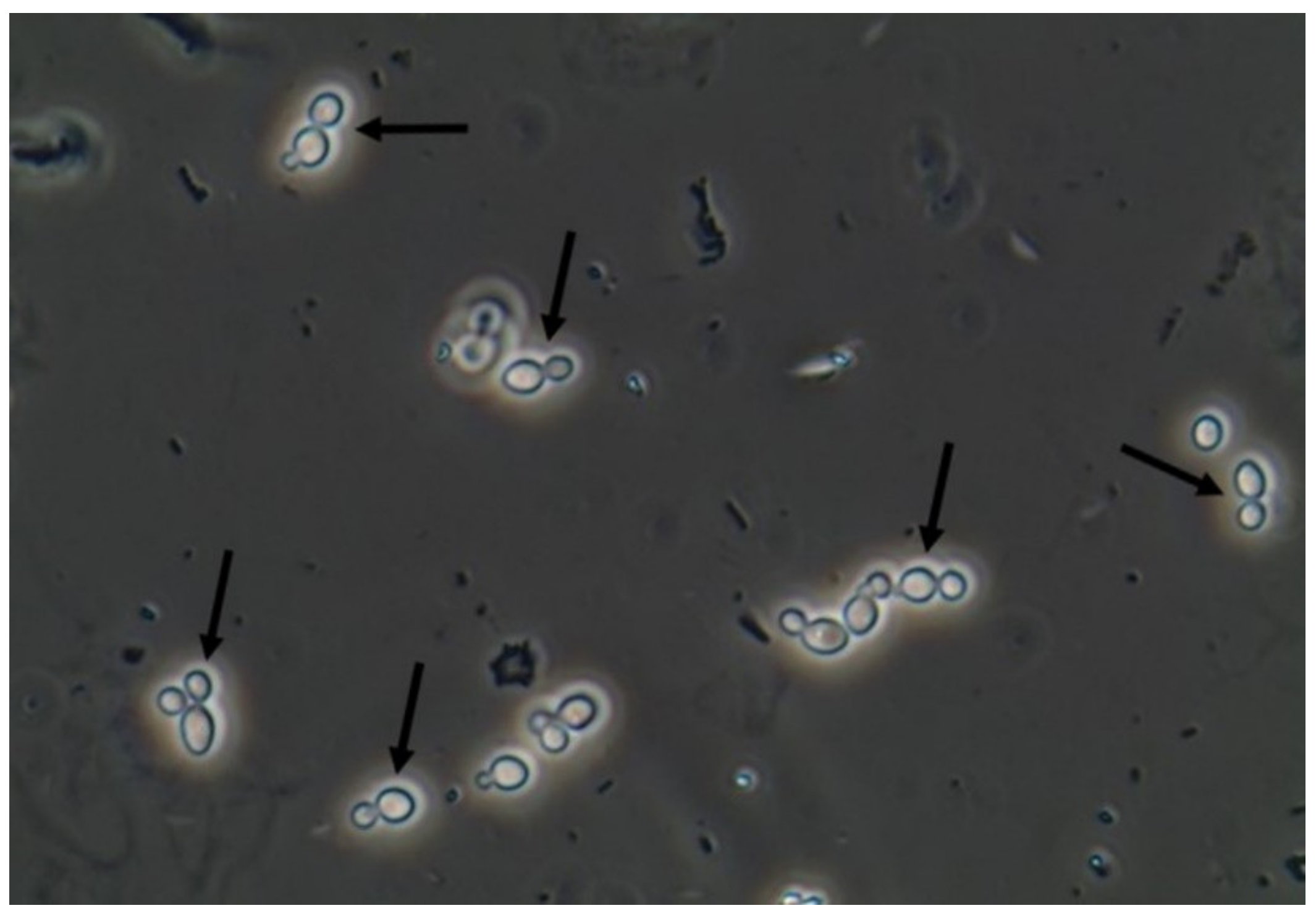
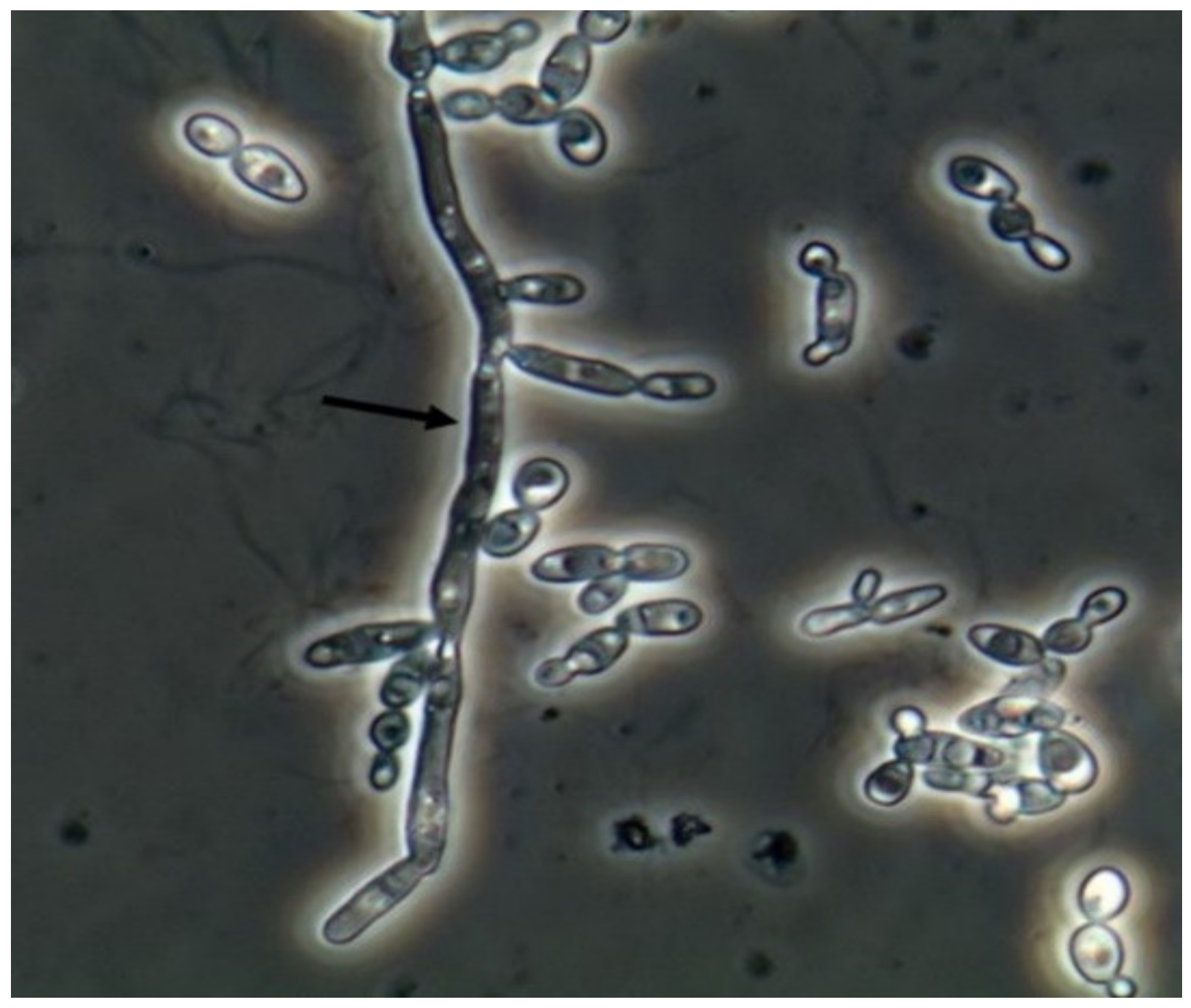
3.1.2. Urine Sediment Profile on Fungal UTI
4. Clinical Presentation of Candiduria
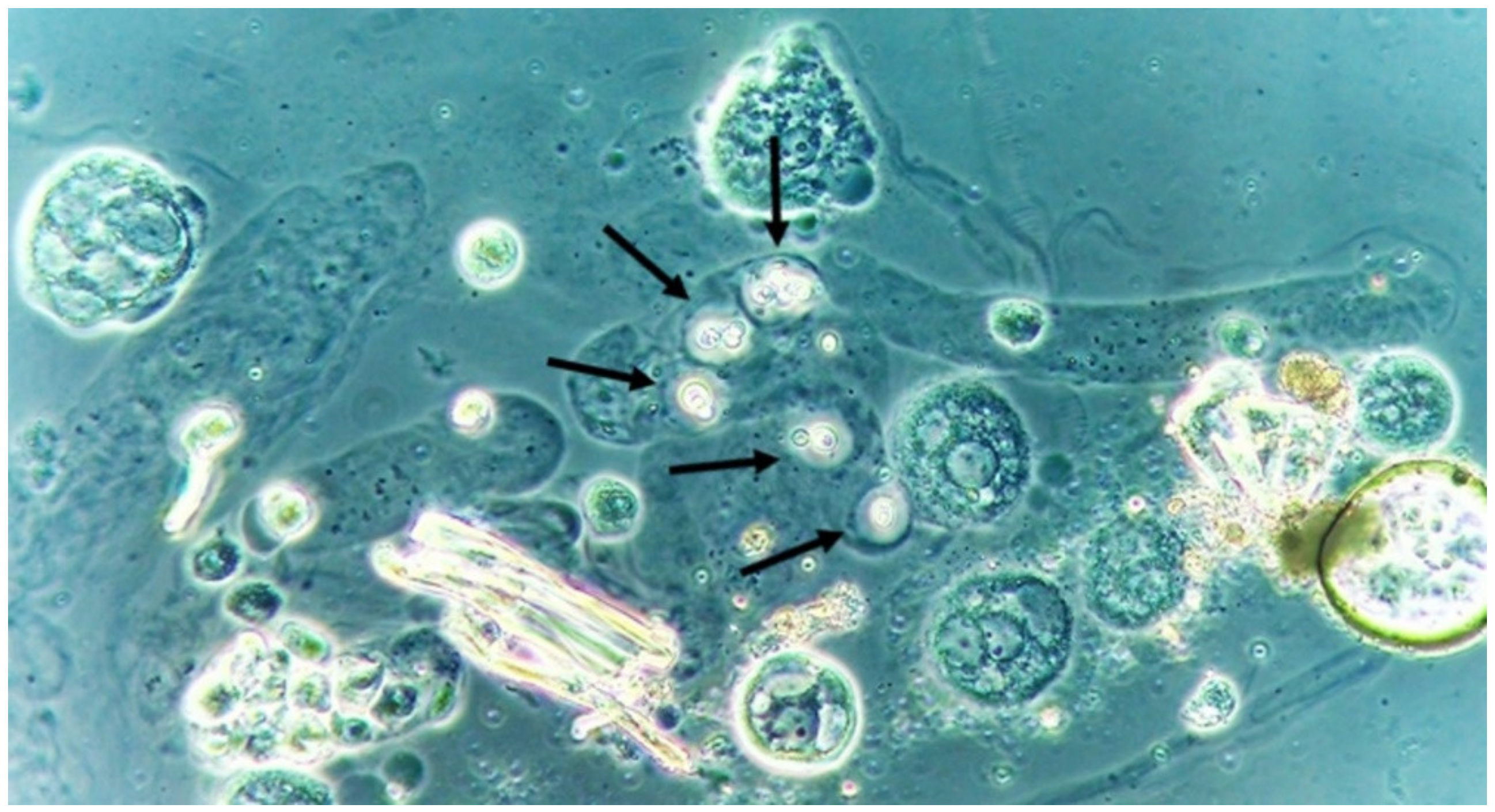
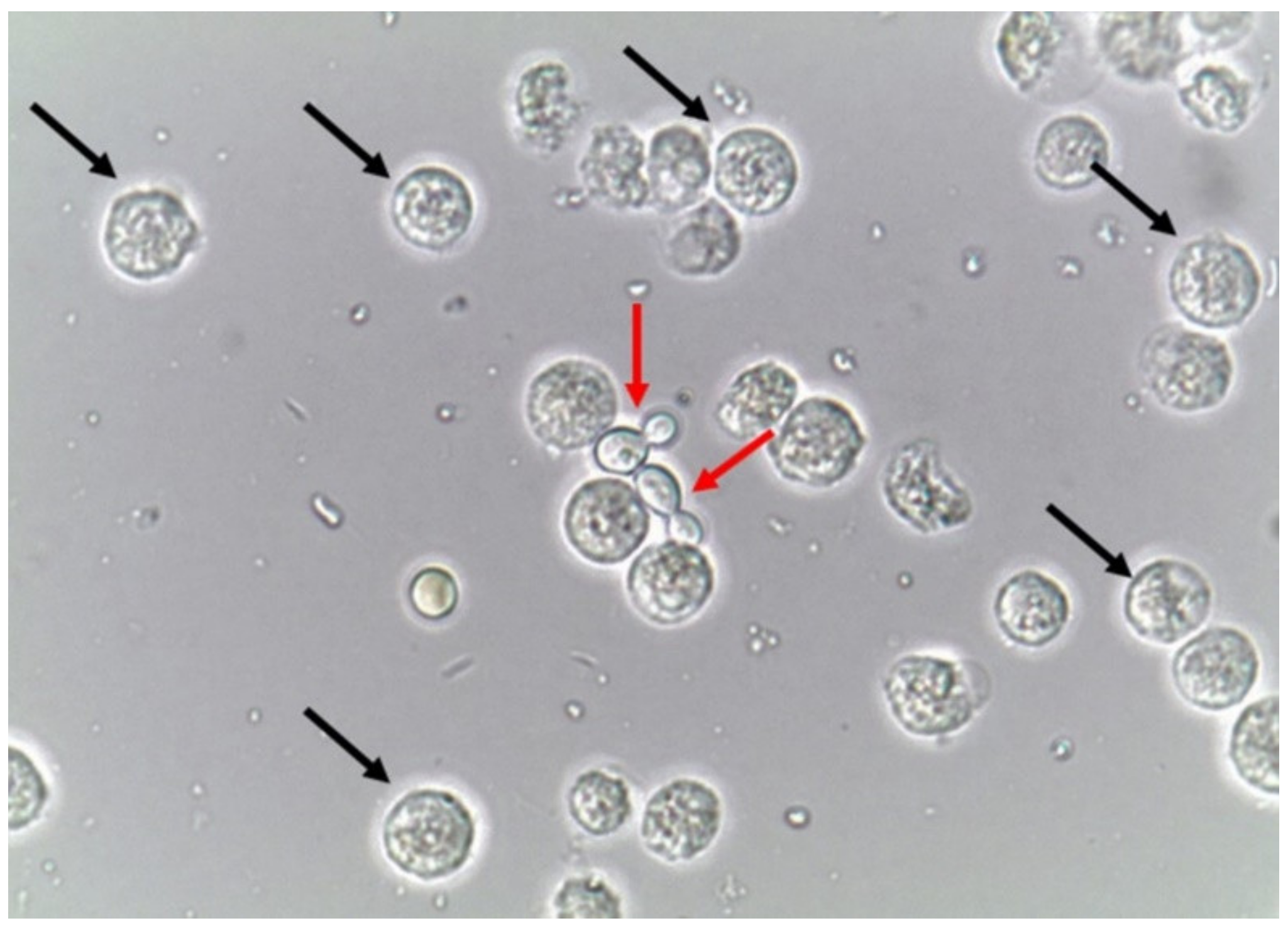
5. Immune Responses to Candiduria
6. Future Perspectives of Urinalysis on Fungal Urinary Tract Infections
7. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Gharanfoli, A.; Mahmoudi, E.; Torabizadeh, R.; Katiraee, F.; Faraji, S. Isolation, characterization, and molecular identification of Candida species from urinary tract infections. Curr. Med. Mycol. 2019, 5, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Kauffman, C.A. Diagnosis and management of fungal urinary tract infection. Infect. Dis. Clin. N. Am. 2014, 28, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Reilly, R.; Perazella, M.A. Nephrology in 30 Days, 2nd ed.; Lange: New York, NY, USA, 2013. [Google Scholar]
- Fogazzi, G.B. The Urinary Sediment—An Integrated View, 3rd ed.; Elsevier: San Francisco, CA, USA, 2010. [Google Scholar]
- Fisher, F.J.; Kavanagh, K.; Sobel, J.D.; Kauffman, C.A.; Newman, C.A. Candida Urinary Tract Infection: Pathogenesis. Clin. Infect. Dis. 2011, 52 (Suppl. S6), S437–S451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odabasi, Z.; Mert, A. Candida urinary tract infections in adults. World J. Urol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Achkar, J.M.; Fries, B.C. Candida infections of the genitourinary tract. Clin. Microbiol. Rev. 2010, 23, 253–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kauffman, C.A.; Vazquez, J.A.; Sobel, J.D.; Gallis, H.A.; McKinsey, D.S.; Karchmer, A.W.; Sugar, A.M.; Sharkey, P.K.; Wise, G.J.; Mangi, R.; et al. Prospective multicenter surveillance study of funguria in hospitalized patients. The National Institute for Allergy and Infectious Diseases (NIAID) Mycoses Study Group. Clin. Infect. Dis. 2000, 30, 14–18. [Google Scholar] [CrossRef] [Green Version]
- Fisher, J.F.; Sobel, J.D.; Kauffman, C.A.; Newman, C.A. Candida urinary tract infections: Treatment. Clin. Infect. Dis. 2011, 52 (Suppl. S6), S457–S466. [Google Scholar] [CrossRef] [Green Version]
- Dias, V. Candida species in the urinary tract: Is it a fungal infection or not? Future Microbiol. 2020, 15, 81–83. [Google Scholar] [CrossRef] [Green Version]
- Gajdács, M.; Dóczi, I.; Ábrók, M.; Lázár, A.; Burián, K. Epidemiology of candiduria and Candida urinary tract infections in inpatients and outpatients: Results from a 10-year retrospective survey. Cent. Eur. J. Urol. 2019, 72, 209–214. [Google Scholar] [CrossRef]
- Colodner, R.Y.; Nuri, Y.; Chazan, B.; Raz, R. Community-acquired and hospital-acquired candiduria: Comparison of prevalence and clinical characteristics. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 27, 301–305. [Google Scholar] [CrossRef]
- Perry, J.D.; Butterworth, A.; Nicholson, M.R.A.; Orr, K.E. Evaluation of a new chromogenic medium, Uriselect 4, for the isolation and identification of urinary tract pathogens. J. Clin. Pathol. 2003, 56, 528–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, N.; Kohli, R.; Cook, E.; Gialanella, P.; Chang, T.; Fries, B.C. Biofilm formation by and antifungal susceptibility of Candida isolates from urine. Appl. Environ. Microbiol. 2007, 73, 1697–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okulicz, J.F.; Rivard, R.G.; Conger, N.G.; Nguyen, M.X.; Hospenthal, D.R. Primary isolation of Candida species from urine specimens using chromogenic medium. Mycoses 2008, 51, 141–146. [Google Scholar] [CrossRef]
- Chabasse, D. Yeast count in urine. Review of the literature and preliminary results of a multicenter prospective study carried out in 15 hospital centers. Ann. Françaises d Anesthésie et de Réanimation 2001, 20, 400–406. [Google Scholar] [CrossRef]
- Fazeli, A.; Kordbacheh, P.; Nazari, A.; Daie Ghazvini, R.; Mirhendi, H.; Safara, M.; Bakhshi, H.; Yaghoubi, R. Candiduria in Hospitalized Patients and Identification of Isolated Candida Species by Morphological and Molecular Methods in Ilam, Iran. Iran. J. Public Health 2019, 48, 156–161. [Google Scholar] [PubMed] [Green Version]
- Navarro, E.E.; Almario, J.S.; King, C.; Bacher, J.; Pizzo, P.A.; Walsh, T.J. Detection of Candida casts in experimental renal candidiasis: Implications for the diagnosis and pathogenesis of upper urinary tract infection. J. Med. Vet. Mycol. 1994, 32, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Poloni, J.A.; Rotta, L.N.; Voegeli, C.F.; Pasqualotto, A.C. Cryptococcus within a urinary cast. Kidney Int. 2013, 84, 218. [Google Scholar] [CrossRef]
- Tesser Poloni, J.A.; Perazella, M.A.; Neild, G.H. Macrophages at work: Phagocytosis of urinary fungi. Clin. Kidney J. 2013, 6, 233–234. [Google Scholar] [CrossRef] [Green Version]
- Itoh, K.; Asai, H.M.S.; Nozaki, T. Atlas of Urinary Sediment, 1st ed.; Sysmex Corporation Scientific Affairs: Kobe, Japan, 2014. [Google Scholar]
- Poloni, J.A.; Meinerz, G.; Monteiro Ade, A.; Keitel, E.; Rotta, L.N. Klebsiella pneumoniae ESBL forming spheroplasts in the fresh and unstained urine sediment. J. Bras. Nefrol. 2016, 38, 269–270. [Google Scholar] [CrossRef]
- Nikler, A.; Radišić Biljak, V.; Čičak, H.; Marić, N.; Bejuk, D.; Poloni, J.A.T.; Simundic, A.M. Escherichia coli spheroplasts in a Croatian patient misclassified by two urine sediment analysers as erythrocytes: Case report. Biochem. Med. (Zagreb) 2019, 29, 030801. [Google Scholar] [CrossRef]
- Richards, M.J.; Edwards, J.R.; Culver, D.H.; Gaynes, R.P. Nosocomial infections in combined medical-surgical intensive care units in the United States. Infect. Control Hosp. Epidemiol. 2000, 21, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Richards, M.J.; Edwards, J.R.; Culver, D.H.; Gaynes, R.P. Nosocomial infections in pediatric intensive care units in the United States. National Nosocomial Infections Surveillance System. Pediatrics 1999, 103, e39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarez-Lerma, F.; Nolla-Salas, J.; Leon, C.; Palomar, M.; Jorda, R.; Carrasco, N.; Bobillo, F. Candiduria in critically ill patients admitted to intensive care medical units. Intensive Care Med. 2003, 29, 1069–1076. [Google Scholar] [CrossRef]
- Bougnoux, M.E.; Kac, G.; Aegerter, P.; D’Enfert, C.; Fagon, J.-Y. Candidemia and candiduria in critically ill patients admitted to intensive care units in France: Incidence, molecular diversity, management and outcome. Intensive Care Med. 2008, 34, 292–299. [Google Scholar] [CrossRef]
- Safdar, N.; Slattery, W.R.; Knasinski, V.; Gangnon, R.E.; Li, Z.; Pirsch, J.D.; Andes, D. Predictors and outcomes of candiduria in renal transplant recipients. Clin. Infect. Dis. 2005, 40, 1413–1421. [Google Scholar] [CrossRef] [Green Version]
- Bouza, E.; Juan, R.S.; Muñoz, P.; Voss, A.; Kluytmans, J. A European perspective on nosocomial urinary tract infections II. Report on incidence, clinical characteristics and outcome (ESGNI-004 study). European Study Group on Nosocomial Infection. Clin. Microbiol. Infect. 2001, 7, 532–542. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez-Cuadra, M.; Horcajada, J.; Martinez, I. 111-Indium labelled leukocyte renal scintigraphy in patients with candiduria: Preliminary results of a prospective study. Int. J. Antimicrob. Agents 2007, 29 (Suppl. S2), 261. [Google Scholar] [CrossRef]
- Argyle, C.; Schumann, G.B.; Genack, L.; Gregory, M. Identification of fungal casts in a patient with renal candidiasis. Hum. Pathol. 1984, 15, 480–481. [Google Scholar] [CrossRef]
- Gregory, M.C.; GSchumann, G.B.; Schumann, J.L.; Argyle, J.C. The clinical significance of candidal casts. Am. J. Kidney Dis. 1984, 4, 179–184. [Google Scholar] [CrossRef]
- Tokunaga, S.; Ohkawa, M.; Takashima, M.; Hisazumi, H. Clinical significance of measurement of serum D-arabinitol levels in candiduria patients. Urol. Int. 1992, 48, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Wise, G.J.; Shteynshlyuger, A. How to diagnose and treat fungal infections in chronic prostatitis. Curr. Urol. Rep. 2006, 7, 320–328. [Google Scholar] [CrossRef]
- Sultana, S.R.; McNeill, S.A.; Phillips, G.; Byrne, D.J. Candidal urinary tract infection as a cause of pneumaturia. J. R. Coll. Surg. Edinb. 1998, 43, 198–199. [Google Scholar] [PubMed]
- Donders, G.G. Lower genital tract infections in diabetic women. Curr. Infect. Dis. Rep. 2002, 4, 536–539. [Google Scholar] [CrossRef] [PubMed]
- High, K.P.; Quagliarello, V.J. Yeast perinephric abscess: Report of a case and review. Clin. Infect. Dis. 1992, 15, 128–133. [Google Scholar] [CrossRef]
- Ronald, A.; Ludwig, E. Urinary tract infections in adults with diabetes. Int. J. Antimicrob. Agents 2001, 17, 287–292. [Google Scholar] [CrossRef]
- Stapleton, A. Urinary tract infections in patients with diabetes. Am. J. Med. 2002, 113 (Suppl. S1A), 80S–84S. [Google Scholar] [CrossRef]
- Svanborg-Eden, C.; Svennerholm, A.M. Secretory immunoglobulin A and G antibodies prevent adhesion of Escherichia coli to human urinary tract epithelial cells. Infect. Immun. 1978, 22, 790–797. [Google Scholar] [CrossRef] [Green Version]
- Svanborg Eden, C.; Andersson, B.; Hagberg, L.; Hanson, L.A.; Leffler, H.; Magnusson, G.; Noori, G.; Dahmen, J.; Soderstrom, T. Receptor analogues and anti-pili antibodies as inhibitors of bacterial attachment in vivo and in vitro. Ann. N. Y. Acad. Sci. 1983, 409, 580–592. [Google Scholar] [CrossRef]
- Uehling, D.T.; James, L.J.; Hopkins, W.J.; Balish, E. Immunization against urinary tract infection with a multi-valent vaginal vaccine. J. Urol. 1991, 146, 223–226. [Google Scholar] [CrossRef]
- Uehling, D.T.; Hopkins, W.J.; Balish, E.; Xing, Y.; Heisey, D.M. Vaginal mucosal immunization for recurrent urinary tract infection: Phase II clinical trial. J. Urol. 1997, 157, 2049–2052. [Google Scholar] [CrossRef]
- Domergue, R.; Castaño, I.; Peñas, A.D.L.; Zupancic, M.; Lockatell, V.; Hebel, J.R.; Johnson, D.; Cormack, B.P. Nicotinic acid limitation regulates silencing of Candida adhesins during UTI. Science 2005, 308, 866–870. [Google Scholar] [CrossRef] [PubMed]
- Zasloff, M. Antimicrobial peptides, innate immunity, and the normally sterile urinary tract. J. Am. Soc. Nephrol. 2007, 18, 2810–2816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abiko, Y.; Saitoh, M.; Nishimura, M.; Yamazaki, M.; Sawamura, D.; Kaku, T. Role of beta-defensins in oral epithelial health and disease. Med. Mol. Morphol. 2007, 40, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Coady, A.; Ramos, A.R.; Olson, J.; Nizet, V.; Patrasa, K.A. Tamm-Horsfall Protein Protects the Urinary Tract against Candida albicans. Infect. Immun. 2018, 86, e00451-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantele, A.; Palkola, N.; Arvilommi, H.; Honkinen, O.; Jahnukainen, T.; Mertsola, J.; Kantele, J.M. Local immune response to upper urinary tract infections in children. Clin. Vaccine Immunol. 2008, 15, 412–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantele, A.M.; Palkola, N.V.; Arvilommi, H.S.; Kantele, J.M. Distinctive homing profile of pathogen-specific activated lymphocytes in human urinary tract infection. Clin. Immunol. 2008, 128, 427–434. [Google Scholar] [CrossRef]
- Torres-Rodriguez, J.M.; Madrenys-Brunet, N.; Nolla-Salas, J.; Carceller, A.; Tur, C. Candiduria in non-neutropenic critically-ill surgical patients. Detection of IgA, IgG and IgM antibodies to Candida albicans by germ tube immunofluorescence. Mycoses 1997, 40, 439–444. [Google Scholar] [CrossRef]
- Enko, D.; Stelzer, I.; Böckl, M.; Derler, B.; Schnedl, W.J.; Anderssohn, P.; Meinitzer, A.; Herrmann, M. Comparison of the diagnostic performance of two automated urine sediment analyzers with manual phase-contrast microscopy. Clin. Chem. Lab. Med. 2020, 58, 268–273. [Google Scholar] [CrossRef]
- Cho, J.; Oh, K.J.; Jeon, B.C.; Lee, S.G.; Kim, J.H. Comparison of five automated urine sediment analyzers with manual microscopy for accurate identification of urine sediment. Clin. Chem. Lab. Med. 2019, 57, 1744–1753. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poloni, J.A.T.; Rotta, L.N. Urine Sediment Findings and the Immune Response to Pathologies in Fungal Urinary Tract Infections Caused by Candida spp. J. Fungi 2020, 6, 245. https://doi.org/10.3390/jof6040245
Poloni JAT, Rotta LN. Urine Sediment Findings and the Immune Response to Pathologies in Fungal Urinary Tract Infections Caused by Candida spp. Journal of Fungi. 2020; 6(4):245. https://doi.org/10.3390/jof6040245
Chicago/Turabian StylePoloni, José Antonio Tesser, and Liane Nanci Rotta. 2020. "Urine Sediment Findings and the Immune Response to Pathologies in Fungal Urinary Tract Infections Caused by Candida spp." Journal of Fungi 6, no. 4: 245. https://doi.org/10.3390/jof6040245