
Prognostic Implications of Left Atrial Spontaneous Echo Contrast with Catheter Ablation of Nonvalvular Atrial Fibrillation Patients with Left Atrial Dilation
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Clinical Characteristics
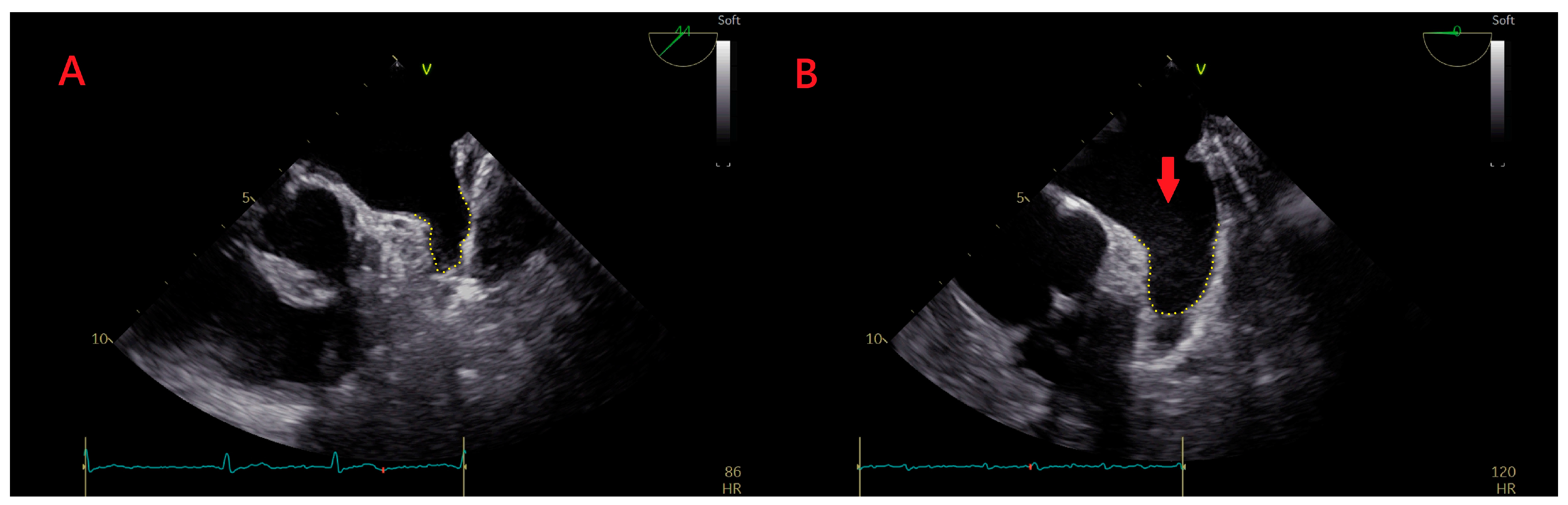
2.3. TEE
2.4. Preparation for the Procedure
2.5. Ablation Procedure
2.6. Follow-Up
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Procedural Details and Medication Use after the Procedure
3.3. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Njoku, A.; Kannabhiran, M.; Arora, R.; Reddy, P.; Gopinathannair, R.; Lakkireddy, D.; Dominic, P. Left atrial volume predicts atrial fibrillation recurrence after radiofrequency ablation: A meta-analysis. Europace 2018, 20, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Cunha, P.S.; Laranjo, S.; Heijman, J.; Oliveira, M.M. The Atrium in Atrial Fibrillation—A Clinical Review on How to Manage Atrial Fibrotic Substrates. Front. Cardiovasc. Med. 2022, 9, 1654. [Google Scholar] [CrossRef] [PubMed]
- Masuda, M.; Iwakura, K.; Inoue, K.; Okamura, A.; Koyama, Y.; Toyoshima, Y.; Tanaka, N.; Nakanishi, H.; Sotomi, Y.; Komuro, I.; et al. Estimation of left atrial blood stasis using diastolic late mitral annular velocity. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 752–757. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Shinoda, Y.; Ikeoka, K.; Inui, H.; Fukuoka, H.; Sunaga, A.; Kanda, T.; Uematsu, M.; Hoshida, S. Dabigatran exhibits low intensity of left atrial spontaneous echo contrast in patients with nonvalvular atrial fibrillation as compared with war-farin. Heart Vessel. 2017, 32, 326–332. [Google Scholar] [CrossRef]
- Unami, N.; Ise, Y.; Suzuki, H. Anticoagulant activity of apixaban can be estimated by multiple regression analysis. J. Arrhythmia 2020, 36, 1032–1038. [Google Scholar] [CrossRef]
- Lin, C.; Bao, Y.; Hua, W.; Zhang, N.; Jin, Q.; Xie, Y.; Wei, Y.; Luo, Q.; Liu, Z.; Ling, T.; et al. Differences in D-dimer blood concentration in atrial fibrillation patients with left atrial thrombus or severe left atrial spontaneous echo contrast. J. Interv. Card. Electrophysiol. 2021, 64, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [PubMed]
- Hahn, R.T.; Abraham, T.; Adams, M.S.; Bruce, C.J.; Glas, K.E.; Lang, R.M.; Reeves, S.T.; Shanewise, J.S.; Siu, S.C.; Stewart, W.; et al. Guidelines for Performing a Comprehensive Transesophageal Echocardiographic Examination: Recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J. Am. Soc. Echocardiogr. 2013, 26, 921–964. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Bao, Y.; Jia, K.; Zhang, N.; Lin, C.; Wei, Y.; Xie, Y.; Luo, Q.; Ling, T.; Chen, K.; et al. Comparison of the Mid-Term Outcomes of Robotic Magnetic Navigation-Guided Radiofrequency Ablation versus Cryoballoon Ablation for Persistent Atrial Fi-brillation. J. Cardiovasc. Dev. Dis. 2022, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Koike, T.; Ejima, K.; Kataoka, S.; Yazaki, K.; Higuchi, S.; Kanai, M.; Yagishita, D.; Shoda, M.; Hagiwara, N. Prognostic signif-icance of diastolic dysfunction in patients with systolic dysfunction undergoing atrial fibrillation ablation. Int. J. Cardiol. Heart Vasc. 2022, 41, 101079. [Google Scholar] [PubMed]
- Jia, F.; Tian, Y.; Lei, S.; Yang, Y.; Luo, S.; He, Q. Incidence and predictors of left atrial thrombus in patients with atrial fibrillation prior to ablation in the real world of China. Indian Pacing Electrophysiol. J. 2019, 19, 134–139. [Google Scholar] [CrossRef]
- Minamisaka, T.; Watanabe, T.; Shinoda, Y.; Ikeoka, K.; Fukuoka, H.; Inui, H.; Ueno, K.; Inoue, S.; Mine, K.; Hoshida, S. Transient manifestation of left ventricular diastolic dysfunction following ablation in patients with paroxysmal atrial fibrillation. Clin. Cardiol. 2018, 41, 978–984. [Google Scholar] [CrossRef]
- Akoum, N.; Fernandez, G.; Wilson, B.; McGann, C.; Kholmovski, E.; Marrouche, N. Association of Atrial Fibrosis Quantified Using LGE-MRI with Atrial Appendage Thrombus and Spontaneous Contrast on Transesophageal Echocardiography in Patients with Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2013, 24, 1104–1109. [Google Scholar] [CrossRef]
- Marrouche, N.F.; Wazni, O.; McGann, C.; Greene, T.; Dean, J.M.; Dagher, L.; Kholmovski, E.; Mansour, M.; Marchlinski, F.; Wilber, D.; et al. Effect of MRI-Guided Fibrosis Ablation vs Conventional Catheter Ablation on Atrial Arrhythmia Recurrence in Patients with Persistent Atrial Fibrillation: The DECAAF II Randomized Clinical Trial. JAMA 2022, 327, 2296–2305. [Google Scholar] [CrossRef] [PubMed]
- Marrouche, N.F.; Wilber, D.; Hindricks, G.; Jais, P.; Akoum, N.; Marchlinski, F.; Kholmovski, E.; Burgon, N.; Hu, N.; Mont, L.; et al. Association of atrial tissue fibrosis identified by delayed enhancement MRI and atrial fibrillation catheter ablation: The DECAAF study. JAMA 2014, 311, 498–506. [Google Scholar] [CrossRef]
- Watson, T.; Shantsila, E.; Lip, G.Y. Mechanisms of thrombogenesis in atrial fibrillation: Virchow’s triad revisited. Lancet 2009, 373, 155–166. [Google Scholar] [CrossRef]
- Choudhury, A.; Lip, G.Y. Atrial fibrillation and the hypercoagulable state: From basic science to clinical practice. Pathophysiol Haemost Thromb. 2005, 33, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Suwa, M. Left atrial spontaneous echo contrast: Relationship with clinical and echocardiographic parameters. Echo Res. Pr. 2019, 6, R65–R73. [Google Scholar] [CrossRef] [PubMed]
- Fatkin, D.; Kelly, R.P.; Feneley, M.P. Relations between left atrial appendage blood flow velocity, spontaneous echocardio-graphic contrast and thromboembolic risk in vivo. J. Am. Coll Cardiol. 1994, 23, 961–969. [Google Scholar] [CrossRef]
- Bernhardt, P.; Schmidt, H.; Hammerstingl, C.; Lüderitz, B.; Omran, H. Patients with Atrial Fibrillation and Dense Spontaneous Echo Contrast at High Risk: A Prospective and Serial Follow-Up Over 12 Months with Transesophageal Echocardiography and Cerebral Magnetic Resonance Imaging. J. Am. Coll. Cardiol. 2005, 45, 1807–1812. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | LASEC Group (n = 73) | No LASEC Group (n = 50) | p Value |
|---|---|---|---|
| Age (years) | 62.6 ± 9.6 | 61.3 ± 8.9 | 0.319 |
| Male sex (n, %) | 47 (64.4%) | 40 (80.0%) | 0.062 |
| PsAF (n, %) | 72 (98.6%) | 46 (92.0%) | 0.173 |
| History of AF (years) | 3.2 ± 2.7 | 3.2 ± 2.9 | 0.779 |
| Duration of AF (years) for PsAF | 0.68 ± 0.45 | 0.73 ± 0.55 | 0.971 |
| BMI (kg/m2) | 25.4 ± 3.3 | 25.9 ± 2.9 | 0.359 |
| DM (n, %) | 14 (19.2%) | 10 (20.0%) | 0.910 |
| Hypertension (n, %) | 45 (61.6%) | 37 (74.0%) | 0.153 |
| Stroke/TIA | 8 (11.0%) | 4 (8.0%) | 0.815 |
| Coronary artery disease (n, %) | 7 (9.6%) | 7 (14.0%) | 0.449 |
| Heart failure (n, %) | 18 (24.7%) | 12 (24.0%) | 0.934 |
| CHA2DS2-VASc score | 2.3 ± 1.3 | 2.2 ± 1.5 | 0.308 |
| Serum creatinine (μmol/L) | 77.3 ± 13.9 | 80.3 ± 15.6 | 0.510 |
| GFR (mL/min/1.73 m²) | 84.9 ± 13.8 | 85.9 ± 16.8 | 0.707 |
| D-dimers (mg/L) | 0.27 ± 0.16 | 0.24 ± 0.18 | 0.059 |
| Homocysteine (μmol/L) | 12.7 ± 3.2 | 12.1 ± 2.7 | 0.554 |
| Pro-BNP (pg/mL) | 1088.6 ± 996.1 | 832.8 ± 887.9 | 0.068 |
| Troponin I | 0.02 ± 0.04 | 0.02 ± 0.01 | 0.233 |
| LAD (mm) | 47.1 ± 2.1 | 46.9 ± 2.0 | 0.598 |
| LAV (cm3) | 182.5 ± 43.9 | 172.8 ± 33.2 | 0.224 |
| LVEDD (mm) | 50.2 ± 4.6 | 50.4 ± 4.3 | 0.512 |
| LVEF (%) | 60.5 ± 8.3 | 61.7 ± 7.8 | 0.360 |
| LASEC Group (n = 73) | No LASEC Group (n = 50) | p Value | |
|---|---|---|---|
| Ablation energy (RFA/CBA) | 53/20 | 33/17 | 0.433 |
| Ablation strategy (PVI/PVI + LA roof line) | 39/34 | 31/19 | 0.346 |
| Total procedure duration (min) | 125.1 ± 36.7 | 123.6 ± 33.0 | 0.903 |
| Left atrial dwell time (min) | 95.6 ± 36.1 | 96.2 ± 31.4 | 0.962 |
| Total fluoroscopy time (min) | 9.6 ± 4.2 | 8.8 ± 6.0 | 0.416 |
| Radiation dose (μGym2) | 2266.7 ± 1532.2 | 2348.4 ± 1822.6 | 0.655 |
| Radiation dose (mGy) | 210.2 ± 135.2 | 220.8 ± 170.3 | 0.518 |
| Medication use after procedure | |||
| Antiarrhythmic drug (n, %) | 70 (95.9%) | 47 (94.0%) | 0.959 |
| Beta-blocker (n, %) | 21 (28.8%) | 17 (34%) | 0.537 |
| NOAC (n, %) | 62 (84.9%) | 48 (96%) | 0.239 |
| ACEI/ARB (n, %) | 43 (58.9%) | 26 (52.0%) | 0.449 |
| No AF/AT Recurrence | With AF/AT Recurrence | |
|---|---|---|
| LASEC group | 33 (45.2%) | 40 (54.8%) |
| No LASEC group | 34 (68.0%) | 16 (32.0%) |
| Total Population (n = 123) | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| p | HR | 95% CI | p | HR | 95% CI | |
| Age (≥65 vs. <65 years) | 0.611 | 0.872 | 0.516–1.475 | |||
| Sex (male vs. female) | 0.621 | 1.161 | 0.642–2.097 | |||
| BMI (abnormal vs. normal) | 0.217 | 0.719 | 0.425–1.215 | |||
| CHA2DS2-VASc score (>2 vs. ≤2) | 0.932 | 1.023 | 0.603–1.737 | |||
| LAD (≥47 vs. <47 mm) | 0.122 | 0.658 | 0.387–1.118 | |||
| HF (HF vs. normal) | 0.011 | 0.379 | 0.179–0.802 | 0.008 | 0.359 | 0.168–0.768 |
| LAV (≥170 vs. <170 cm3) | 0.025 | 1.859 | 1.082–3.196 | 0.040 | 1.787 | 1.028–3.108 |
| History of AF (≥2 vs. <2 years) | 0.003 | 3.005 | 1.471–6.137 | 0.018 | 2.415 | 1.166–5.001 |
| LASEC (LASEC vs. no LASEC) | 0.015 | 2.058 | 1.151–3.679 | 0.009 | 0.455 | 0.253–0.819 |
| Ablation energy (CBA vs. RFA) | 0.411 | 1.261 | 0.725–2.193 | |||
| Ablation strategy (PVI vs. PVI + LA roof line) | 0.905 | 1.035 | 0.590–1.813 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.; Bao, Y.; Xie, Y.; Wei, Y.; Luo, Q.; Ling, T.; Jin, Q.; Pan, W.; Xie, Y.; Wu, L.; et al. Prognostic Implications of Left Atrial Spontaneous Echo Contrast with Catheter Ablation of Nonvalvular Atrial Fibrillation Patients with Left Atrial Dilation. J. Cardiovasc. Dev. Dis. 2022, 9, 306. https://doi.org/10.3390/jcdd9090306
Lin C, Bao Y, Xie Y, Wei Y, Luo Q, Ling T, Jin Q, Pan W, Xie Y, Wu L, et al. Prognostic Implications of Left Atrial Spontaneous Echo Contrast with Catheter Ablation of Nonvalvular Atrial Fibrillation Patients with Left Atrial Dilation. Journal of Cardiovascular Development and Disease. 2022; 9(9):306. https://doi.org/10.3390/jcdd9090306
Chicago/Turabian StyleLin, Changjian, Yangyang Bao, Yun Xie, Yue Wei, Qingzhi Luo, Tianyou Ling, Qi Jin, Wenqi Pan, Yucai Xie, Liqun Wu, and et al. 2022. "Prognostic Implications of Left Atrial Spontaneous Echo Contrast with Catheter Ablation of Nonvalvular Atrial Fibrillation Patients with Left Atrial Dilation" Journal of Cardiovascular Development and Disease 9, no. 9: 306. https://doi.org/10.3390/jcdd9090306