
Unipolar Electrogram-Guided versus Lesion Size Index-Guided Catheter Ablation in Patients with Paroxysmal Atrial Fibrillation

 ,
, 
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Mapping and RF Catheter Ablation
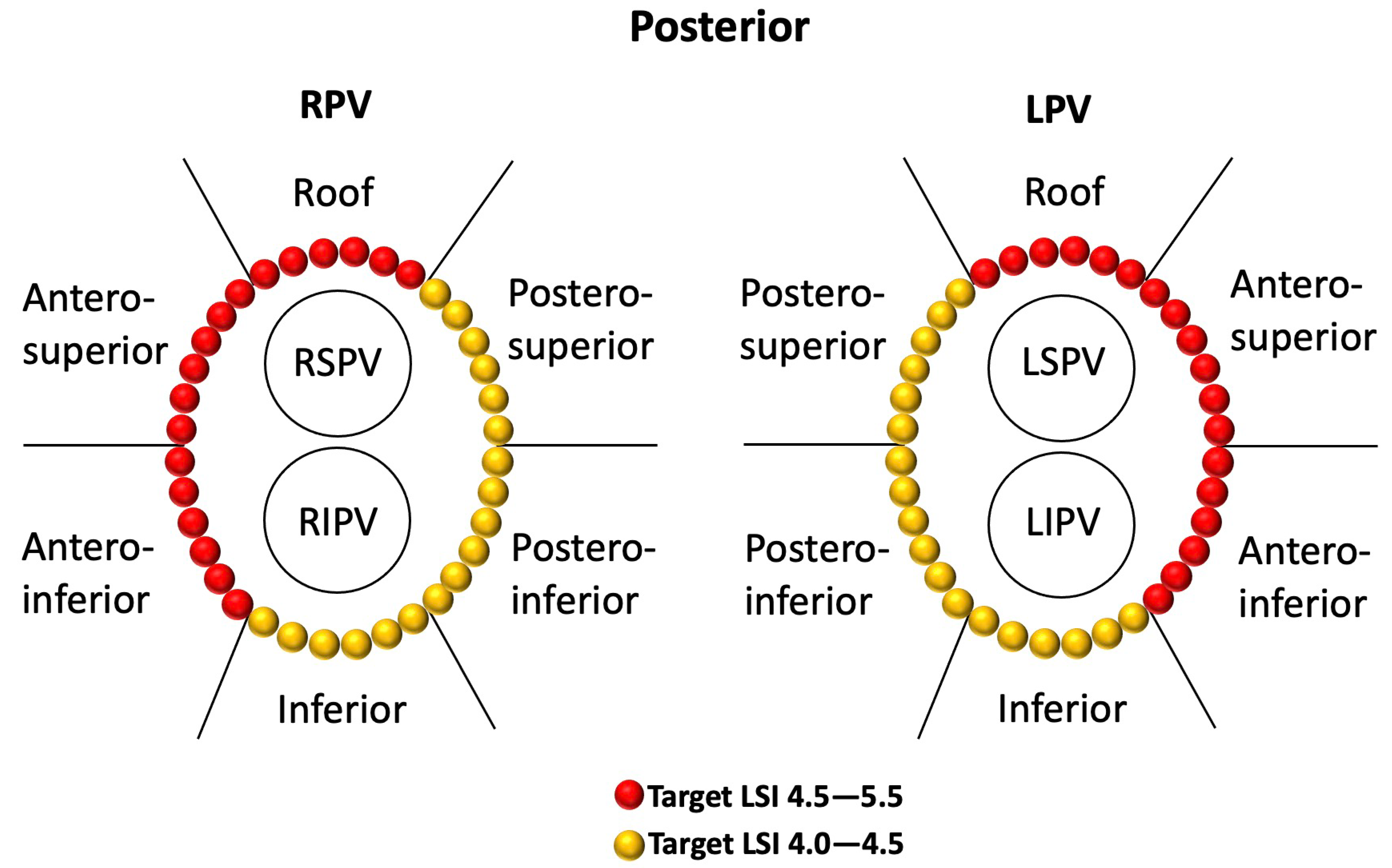
2.2.1. LSI-Guided PVI
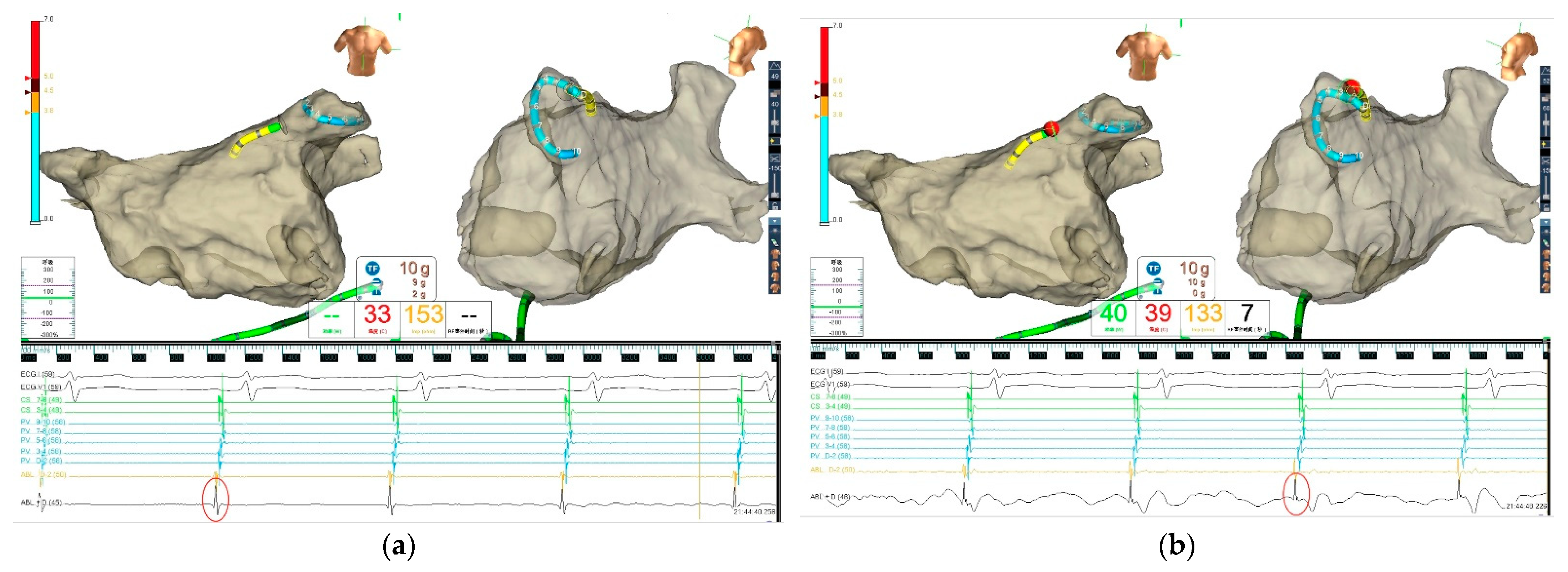
2.2.2. UP-EGM-Guided PVI
2.3. Postablation Management and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Index AF Ablation Procedure
3.3. The First-Pass PVI Rate
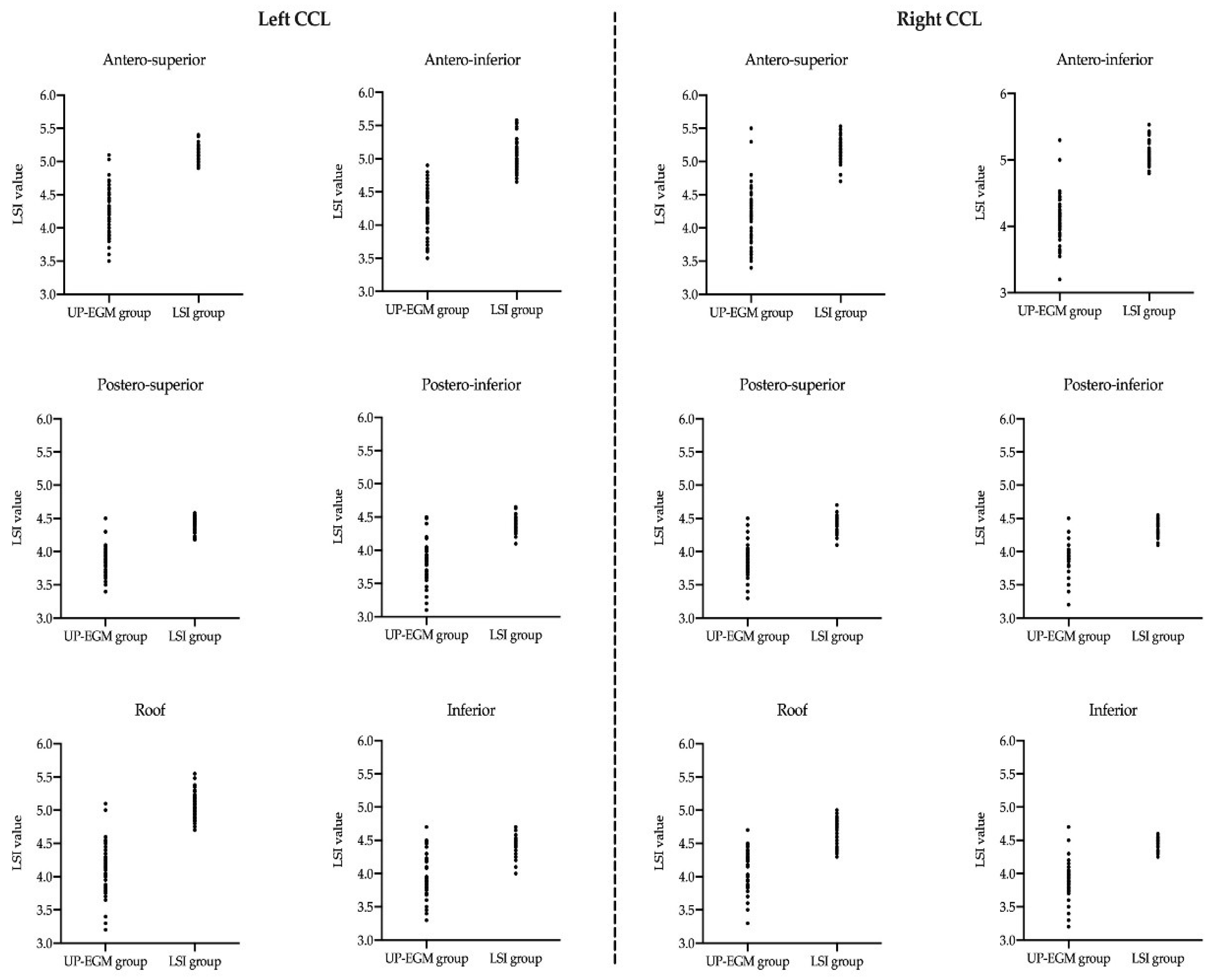
3.4. LSI Values in Different Regions of Continuous Circular Lesions (CCLs)
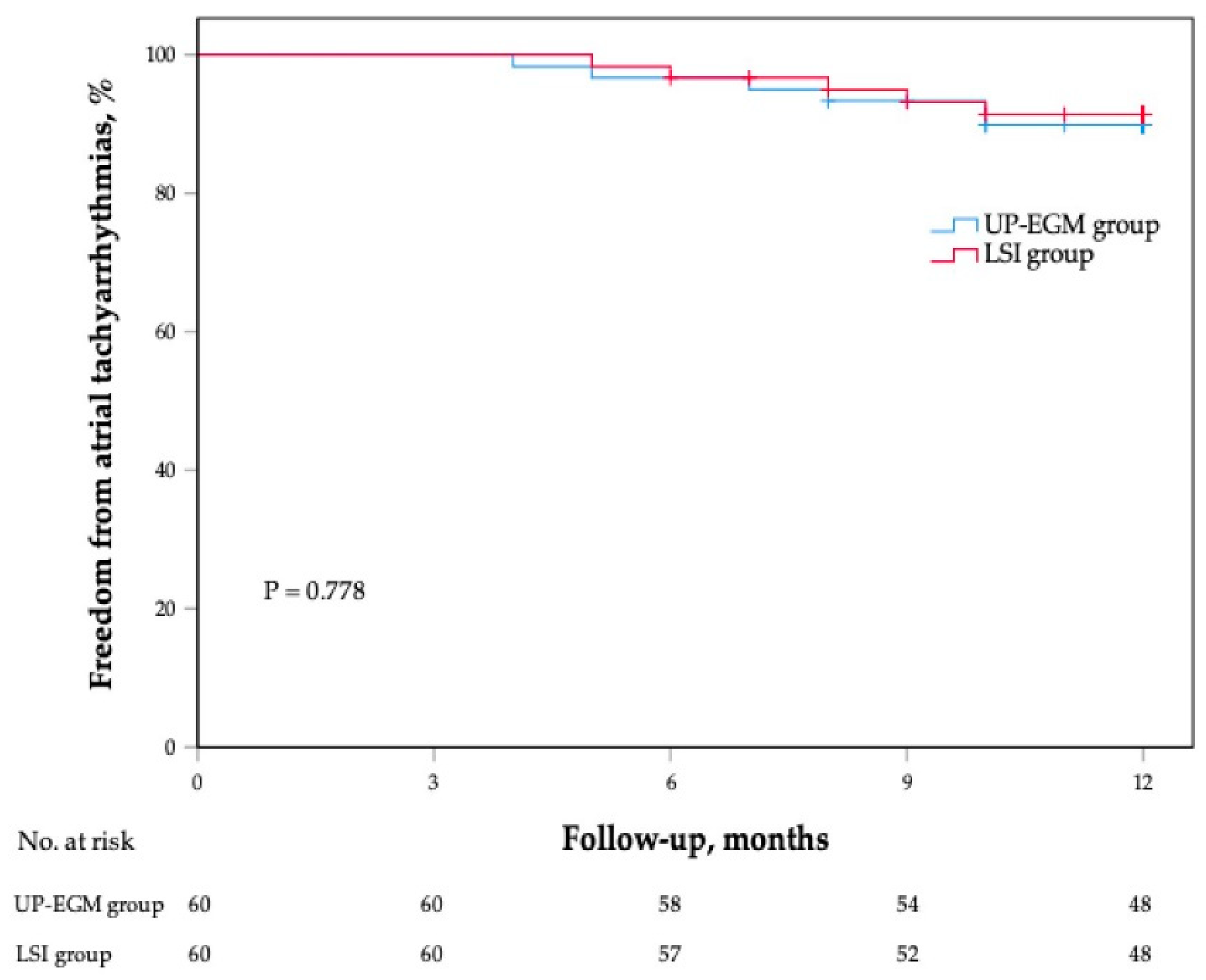
3.5. Follow-Up
4. Discussion
4.1. Main Findings
4.2. The LSI Values
4.3. The Relationship between UP-EGM and LSI
4.4. The Potential Advantages UP-EGM
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [PubMed]
- Calzolari, V.; De Mattia, L.; Indiani, S.; Crosato, M.; Furlanetto, A.; Licciardello, C.; Squasi, P.A.M.; Olivari, Z. In Vitro Validation of the Lesion Size Index to Predict Lesion Width and Depth After Irrigated Radiofrequency Ablation in a Porcine Model. JACC Clin. Electrophysiol. 2017, 3, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- Mattia, L.; Crosato, M.; Indiani, S.; Causin, E.; Licciardello, C.; Maria Squasi, P.A.; De Leo, A.; Calzolari, V. Prospective Evaluation of Lesion Index-Guided Pulmonary Vein Isolation Technique in Patients with Paroxysmal Atrial Fibrillation: 1-year Follow-Up. J. Atr. Fibrillation. 2018, 10, 1858. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, S.; Choe, W.; Jordan, J.R.; Boorman, C.; Mullins, N.; Davies, A.; Stucky, A.; Nath, S. Two Year, Single Center Clinical Outcome After Catheter Ablation for Paroxysmal Atrial Fibrillation Guided by Lesion Index. J. Atr. Fibrillation. 2018, 11, 1760. [Google Scholar] [CrossRef] [PubMed]
- Kanamori, N.; Kato, T.; Sakagami, S.; Saeki, T.; Kato, C.; Kawai, K.; Chikata, A.; Takashima, S.I.; Murai, H.; Usui, S.; et al. Optimal lesion size index to prevent conduction gap during pulmonary vein isolation. J. Cardiovasc. Electrophysiol. 2018, 29, 1616–1623. [Google Scholar] [CrossRef] [PubMed]
- Dello Russo, A.; Fassini, G.M.; Casella, M.; Romanelli, E.; Pala, S.; Riva, S.; Catto, V.; Moltrasio, M.; Tundo, F.; Zucchetti, M.; et al. Lesion index: A novel guide in the path of successful pulmonary vein isolation. J. Interv. Card. Electrophysiol. 2019, 55, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Suenari, K.; Nakano, Y.; Hirai, Y.; Ogi, H.; Oda, N.; Makita, Y.; Ueda, S.; Kajihara, K.; Tokuyama, T.; Motoda, C.; et al. Left atrial thickness under the catheter ablation lines in patients with paroxysmal atrial fibrillation: Insights from 64-slice multidetector computed tomography. Heart Vessel. 2013, 28, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhou, G.; Chen, S.; Wei, Y.; Lu, X.; Xu, J.; Wu, X.; Liu, S. Tailored ablation index for pulmonary vein isolation according to wall thickness within the ablation circle. Pacing. Clin. Electrophysiol. 2021, 44, 575–585. [Google Scholar] [CrossRef] [PubMed]
- Otomo, K.; Uno, K.; Fujiwara, H.; Isobe, M.; Iesaka, Y. Local unipolar and bipolar electrogram criteria for evaluating the transmurality of atrial ablation lesions at different catheter orientations relative to the endocardial surface. Heart Rhythm 2010, 7, 1291–1300. [Google Scholar] [CrossRef] [PubMed]
- Bortone, A.; Appetiti, A.; Bouzeman, A.; Maupas, E.; Ciobotaru, V.; Boulenc, J.M.; Pujadas-Berthault, P.; Rioux, P. Unipolar signal modification as a guide for lesion creation during radiofrequency application in the left atrium: Prospective study in humans in the setting of paroxysmal atrial fibrillation catheter ablation. Circ. Arrhythm. Electrophysiol. 2013, 6, 1095–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bortone, A.; Brault-Noble, G.; Appetiti, A.; Marijon, E. Elimination of the negative component of the unipolar atrial electrogram as an in vivo marker of transmural lesion creation: Acute study in canines. Circ. Arrhythm. Electrophysiol. 2015, 8, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Fu, G.; He, B.; Wang, B.; Liu, J.; Yu, Y.; Du, X.; Feng, M.; Gao, F.; Jin, H.; Fang, R.; et al. Unipolar electrogram-guided radiofrequency catheter ablation in paroxysmal atrial fibrillation: Electrogram patterns and outcomes. J. Interv. Card. Electrophysiol. 2019, 54, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Park, C.I.; Lehrmann, H.; Keyl, C.; Weber, R.; Schiebeling, J.; Allgeier, J.; Schurr, P.; Shah, A.; Neumann, F.J.; Arentz, T.; et al. Mechanisms of pulmonary vein reconnection after radiofrequency ablation of atrial fibrillation: The deterministic role of contact force and interlesion distance. J. Cardiovasc. Electrophysiol. 2014, 25, 701–708. [Google Scholar] [CrossRef] [PubMed]
- El Haddad, M.; Taghji, P.; Phlips, T.; Wolf, M.; Demolder, A.; Choudhury, R.; Knecht, S.; Vandekerckhove, Y.; Tavernier, R.; Nakagawa, H.; et al. Determinants of Acute and Late Pulmonary Vein Reconnection in Contact Force-Guided Pulmonary Vein Isolation: Identifying the Weakest Link in the Ablation Chain. Circ. Arrhythm. Electrophysiol. 2017, 10, e004867. [Google Scholar] [CrossRef] [PubMed]
- Hussein, A.; Das, M.; Riva, S.; Morgan, M.; Ronayne, C.; Sahni, A.; Shaw, M.; Todd, D.; Hall, M.; Modi, S.; et al. Use of Ablation Index-Guided Ablation Results in High Rates of Durable Pulmonary Vein Isolation and Freedom from Arrhythmia in Persistent Atrial Fibrillation Patients: The PRAISE Study Results. Circ. Arrhythm. Electrophysiol. 2018, 11, e006576. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Wang, J.; Niu, H.X.; Chu, J.M.; Hua, W.; Zhang, S.; Yao, Y. Optimal Lesion Size Index for Pulmonary Vein Isolation in High-Power Radiofrequency Catheter Ablation of Atrial Fibrillation. Front. Cardiovasc. Med. 2022, 7, 9:869254. [Google Scholar] [CrossRef] [PubMed]
- Pambrun, T.; Durand, C.; Constantin, M.; Masse, A.; Marra, C.; Meillet, V.; Haïssaguerre, M.; Jaïs, P.; Bortone, A. High-Power (40–50 W) Radiofrequency Ablation Guided by Unipolar Signal Modification for Pulmonary Vein Isolation: Experimental Findings and Clinical Results. Circ. Arrhythm. Electrophysiol. 2019, 12, e007304. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | UP-EGM Group (n = 60) | LSI Group (n = 60) | p-Value |
|---|---|---|---|
| Age, years | 62.9 ± 10.3 | 62.5 ± 9.1 | 0.779 |
| Male, n (%) | 35 (58.3%) | 29 (48.3%) | 0.272 |
| Body mass index, kg/m2 | 24.0 ± 3.0 | 24.0 ± 2.8 | 0.980 |
| History of AF, months | 24 (8.3, 60) | 24 (9.5, 60) | 0.694 |
| CHA2DS2-VASc score | 2 (1, 3) | 2 (1, 3) | 0.388 |
| HAS-BLED score | 1 (0, 2) | 1 (0, 2) | 0.547 |
| Comorbidity | |||
| Hypertension, n (%) | 31 (51.7%) | 38 (63.3%) | 0.196 |
| Diabetes mellitus, n (%) | 7 (11.7%) | 7 (11.7%) | 1.000 |
| Congestive heart failure, n (%) | 4 (6.7%) | 5 (8.3%) | 0.729 |
| Coronary artery disease, n (%) | 4 (6.7%) | 3 (5.0%) | 0.697 |
| Previous TIA/stroke, n (%) | 6 (10.0%) | 7 (11.7%) | 0.769 |
| Echocardiography | |||
| LA diameter, mm | 37.9 ± 5.3 | 36.8 ± 4.9 | 0.207 |
| LVEF, % | 64.2 ± 5.5 | 65.1 ± 5.2 | 0.348 |
| Variables | UP-EGM Group (n = 60) | LSI Group (n = 60) | p-Value |
|---|---|---|---|
| Total ablation points | 86.1 ± 12.5 | 89.7 ± 10.6 | 0.087 |
| Procedural duration, min | 101 (86, 112) | 113 (105, 117) | <0.001 |
| X-ray exposure, min | 4.6 (3.4, 5.5) | 6.0 (4.2, 8.3) | 0.008 |
| Ablation time, min | 21.1 ± 2.4 | 32.6 ± 3.9 | <0.001 |
| Ablation energy delivered, kJ | 49.4 ± 5.7 | 57.8 ± 14.5 | <0.001 |
| Mean CF, g | 11 (10, 12) | 11 (10, 12) | 0.568 |
| Mean impedance decrease, Ω | 12 (11, 13) | 11.5 (10, 14) | 0.736 |
| Required targeting of the carina regions for PVI completion, n (%) | 11 (18.3%) | 12 (20%) | 0.817 |
| The first-pass PVI, n (%) | 54 (90%) | 55 (91.7%) | 0.752 |
| Acutely PVI, n (%) | 100% | 100% | 1.000 |
| Additional ablation after PVI | |||
| Cavotricuspid isthmus ablation, n (%) | 6 (10.0%) | 5 (8.3%) | 0.752 |
| Superior vena cava isolation, n (%) | 1 (1.7%) | 1 (1.7%) | 1.000 |
| Complications | |||
| Reactive pneumonia, n (%) | 0 (0%) | 1 (1.7%) | 1.000 |
| Pseudoaneurysm, n (%) | 1 (1.7%) | 0 (0%) | 1.000 |
| Regions | UP-EGM Group (n = 60) | LSI Group (n = 60) | p-Value |
|---|---|---|---|
| Left CCLs | |||
| Roof | 4.12 ± 0.37 | 5.07 ± 0.18 | <0.001 |
| Antero-superior | 4.23 ± 0.35 | 5.12 ± 0.13 | <0.001 |
| Antero-inferior | 4.20 ± 0.33 | 5.03 ± 0.13 | <0.001 |
| Postero-superior | 3.90 ± 0.29 | 4.43 ± 0.10 | <0.001 |
| Postero-inferior | 3.83 ± 0.29 | 4.39 ± 0.10 | <0.001 |
| Inferior | 3.98 ± 0.30 | 4.45 ± 0.11 | <0.001 |
| Right CCLs | |||
| Roof | 4.13 ± 0.30 | 4.75 ± 0.15 | <0.001 |
| Antero-superior | 4.19 ± 0.40 | 5.16 ± 0.15 | <0.001 |
| Antero-inferior | 4.15 ± 0.32 | 5.06 ± 0.16 | <0.001 |
| Postero-superior | 3.91 ± 0.24 | 4.45 ± 0.11 | <0.001 |
| Postero-inferior | 3.89 ± 0.24 | 4.38 ± 0.10 | <0.001 |
| Inferior | 3.89 ± 0.24 | 4.45 ± 0.08 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, G.; He, B.; Wang, B.; Feng, M.; Du, X.; Liu, J.; Yu, Y.; Gao, F.; Zhuo, W.; Xu, Y.; et al. Unipolar Electrogram-Guided versus Lesion Size Index-Guided Catheter Ablation in Patients with Paroxysmal Atrial Fibrillation. J. Cardiovasc. Dev. Dis. 2022, 9, 229. https://doi.org/10.3390/jcdd9070229
Fu G, He B, Wang B, Feng M, Du X, Liu J, Yu Y, Gao F, Zhuo W, Xu Y, et al. Unipolar Electrogram-Guided versus Lesion Size Index-Guided Catheter Ablation in Patients with Paroxysmal Atrial Fibrillation. Journal of Cardiovascular Development and Disease. 2022; 9(7):229. https://doi.org/10.3390/jcdd9070229
Chicago/Turabian StyleFu, Guohua, Bin He, Binhao Wang, Mingjun Feng, Xianfeng Du, Jing Liu, Yibo Yu, Fang Gao, Weidong Zhuo, Yi Xu, and et al. 2022. "Unipolar Electrogram-Guided versus Lesion Size Index-Guided Catheter Ablation in Patients with Paroxysmal Atrial Fibrillation" Journal of Cardiovascular Development and Disease 9, no. 7: 229. https://doi.org/10.3390/jcdd9070229