
Excessive Supraventricular Ectopic Activity and the Risk of Atrial Fibrillation and Stroke: A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Search
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Included Studies
3.2. Association between ESVEA and AF
3.2.1. Association between ESVEA and AF in the General Population
3.2.2. Association between ESVEA and AF in the Ischemic Stroke Patients
3.3. Association between ESVEA and Stroke
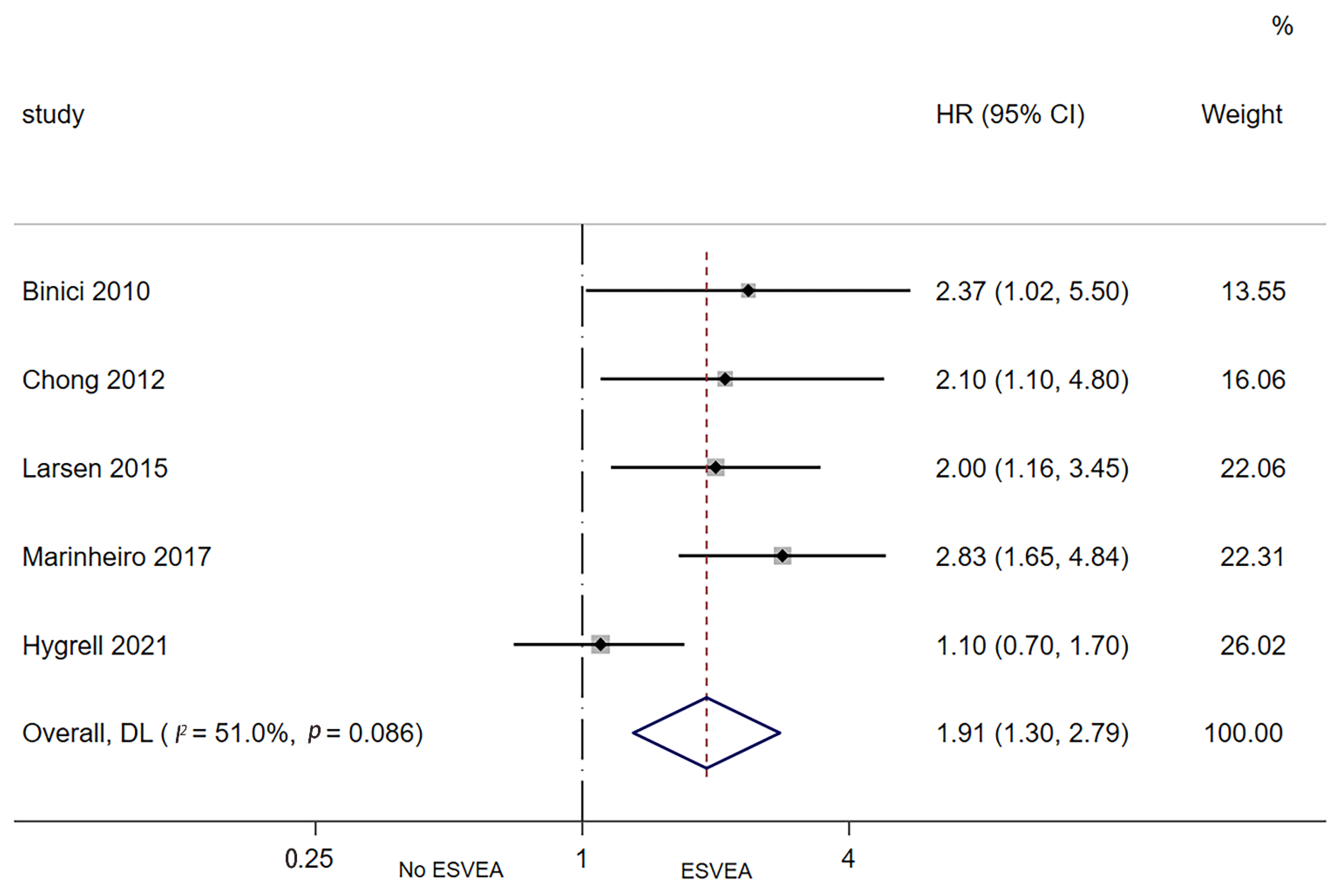
3.3.1. Association between ESVEA and Risk of New-Onset Ischemic Stroke
3.3.2. Association between ESVEA and Risk of Recurrent Ischemic Stroke/Transient Ischemic Attack (TIA)
3.4. Association between ESVEA and All-Cause Mortality
4. Discussion
4.1. Thoughts on Antithrombotic Therapy of ESVEA
4.2. Definition of ESVEA
4.3. Detection Methods of ESVEA
4.4. Limitations
4.5. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.G.; Diener, H.C.; Coutts, S.B.; Easton, J.D.; Granger, C.B.; O’Donnell, M.J.; Sacco, R.L.; Connolly, S.J. Embolic strokes of undetermined source: The case for a new clinical construct. Lancet Neurol. 2014, 13, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial fibrillation as an independent risk factor for stroke: The Framingham Study. Stroke 1991, 22, 983–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heuschmann, P.U.; Kolominsky-Rabas, P.L.; Misselwitz, B.; Hermanek, P.; Leffmann, C.; Janzen, R.W.; Rother, J.; Buecker-Nott, H.J.; Berger, K. Predictors of in-hospital mortality and attributable risks of death after ischemic stroke: The German Stroke Registers Study Group. Arch. Intern. Med. 2004, 164, 1761–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kongbunkiat, K.; Kasemsap, N.; Travanichakul, S.; Thepsuthammarat, K.; Tiamkao, S.; Sawanyawisuth, K. Hospital mortality from atrial fibrillation associated with ischemic stroke: A national data report. Int. J. Neurosci. 2015, 125, 924–928. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.T.; Wong, Y.S.; Wu, C.S.; Su, Y.H. Atrial fibrillation is a predictor of in-hospital mortality in ischemic stroke patients. Ther. Clin. Risk Manag. 2016, 12, 1057–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, K.; Hobohm, L.; Wenzel, P.; Münzel, T.; Espinola-Klein, C.; Ostad, M.A. Impact of atrial fibrillation/flutter on the in-hospital mortality of ischemic stroke patients. Heart Rhythm. 2020, 17, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A.; García-Eroles, L.; Massons, J.B.; Oliveres, M.; Pujades, R.; Targa, C. Atrial fibrillation and stroke: Clinical presentation of cardioembolic versus atherothrombotic infarction. Int. J. Cardiol. 2000, 73, 33–42. [Google Scholar] [CrossRef]
- Flach, C.; Muruet, W.; Wolfe, C.D.A.; Bhalla, A.; Douiri, A. Risk and Secondary Prevention of Stroke Recurrence: A Population-Base Cohort Study. Stroke 2020, 51, 2435–2444. [Google Scholar] [CrossRef]
- Arboix, A.; García-Eroles, L.; Massons, J.; Oliveres, M. Predictive clinical factors of in-hospital mortality in 231 consecutive patients with cardioembolic cerebral infarction. Cerebrovasc. Dis. 1998, 8, 8–13. [Google Scholar] [CrossRef]
- Wallmann, D.; Tuller, D.; Wustmann, K.; Meier, P.; Isenegger, J.; Arnold, M.; Mattle, H.P.; Delacretaz, E. Frequent atrial premature beats predict paroxysmal atrial fibrillation in stroke patients: An opportunity for a new diagnostic strategy. Stroke 2007, 38, 2292–2294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binici, Z.; Intzilakis, T.; Nielsen, O.W.; Køber, L.; Sajadieh, A. Excessive supraventricular ectopic activity and increased risk of atrial fibrillation and stroke. Circulation 2010, 121, 1904–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, B.H.; Pong, V.; Lam, K.F.; Liu, S.; Zuo, M.L.; Lau, Y.F.; Lau, C.P.; Tse, H.F.; Siu, C.W. Frequent premature atrial complexes predict new occurrence of atrial fibrillation and adverse cardiovascular events. Europace 2012, 14, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Dewland, T.A.; Vittinghoff, E.; Mandyam, M.C.; Heckbert, S.R.; Siscovick, D.S.; Stein, P.K.; Psaty, B.M.; Sotoodehnia, N.; Gottdiener, J.S.; Marcus, G.M. Atrial ectopy as a predictor of incident atrial fibrillation: A cohort study. Ann. Intern. Med. 2013, 159, 721–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acharya, T.; Tringali, S.; Bhullar, M.; Nalbandyan, M.; Ilineni, V.K.; Carbajal, E.; Deedwania, P. Frequent Atrial Premature Complexes and Their Association WITH Risk of Atrial Fibrillation. Am. J. Cardiol. 2015, 116, 1852–1857. [Google Scholar] [CrossRef]
- Kochhäuser, S.; Dechering, D.G.; Dittrich, R.; Reinke, F.; Ritter, M.A.; Ramtin, S.; Duning, T.; Frommeyer, G.; Eckardt, L. Supraventricular premature beats and short atrial runs predict atrial fibrillation in continuously monitored patients with cryptogenic stroke. Stroke 2014, 45, 884–886. [Google Scholar] [CrossRef]
- Murakoshi, N.; Xu, D.; Sairenchi, T.; Igarashi, M.; Irie, F.; Tomizawa, T.; Tada, H.; Sekiguchi, Y.; Yamagishi, K.; Iso, H.; et al. Prognostic impact of supraventricular premature complexes in community-based health checkups: The Ibaraki Prefectural Health Study. Eur. Heart J. 2015, 36, 170–178. [Google Scholar] [CrossRef]
- Nguyen, K.T.; Vittinghoff, E.; Dewland, T.A.; Dukes, J.W.; Soliman, E.Z.; Stein, P.K.; Gottdiener, J.S.; Alonso, A.; Chen, L.Y.; Psaty, B.M.; et al. Ectopy on a Single 12-Lead ECG, Incident Cardiac Myopathy, and Death in the Community. J. Am. Heart Assoc. 2017, 6, e006028. [Google Scholar] [CrossRef]
- O’Neal, W.T.; Kamel, H.; Judd, S.E.; Safford, M.M.; Vaccarino, V.; Howard, V.J.; Howard, G.; Soliman, E.Z. Usefulness of Atrial Premature Complexes on Routine Electrocardiogram to Determine the Risk of Atrial Fibrillation (from the REGARDS Study). Am. J. Cardiol. 2017, 120, 782–785. [Google Scholar] [CrossRef]
- Durmaz, E.; Ikitimur, B.; Ebren, C.; Tokdil, H.; Karaca, O.F.; Polat, F.; Ongen, Z. The clinical significance of premature atrial contractions: How frequent should they become predictive of new onset atrial fibrillation. Anatol. J. Cardiol. 2019, 22, 47. [Google Scholar] [CrossRef]
- Conen, D.; Adam, M.; Roche, F.; Barthelemy, J.C.; Felber Dietrich, D.; Imboden, M.; Künzli, N.; von Eckardstein, A.; Regenass, S.; Hornemann, T.; et al. Premature atrial contractions in the general population: Frequency and risk factors. Circulation 2012, 126, 2302–2308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinther, K.H.; Tveskov, C.; Möller, S.; Rosen, T.; Auscher, S.; Osmanagic, A.; Egstrup, K. Prevalence and Prognostic Significance of Runs of Premature Atrial Complexes in Ischemic Stroke Patients. J. Stroke Cerebrovasc. Dis. 2016, 25, 2338–2343. [Google Scholar] [CrossRef] [PubMed]
- Larsen, B.S.; Kumarathurai, P.; Falkenberg, J.; Nielsen, O.W.; Sajadieh, A. Excessive Atrial Ectopy and Short Atrial Runs Increase the Risk of Stroke Beyond Incident Atrial Fibrillation. J. Am. Coll. Cardiol. 2015, 66, 232–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber-Krüger, M.; Gröschel, K.; Mende, M.; Seegers, J.; Lahno, R.; Haase, B.; Niehaus, C.F.; Edelmann, F.; Hasenfuß, G.; Wachter, R.; et al. Excessive supraventricular ectopic activity is indicative of paroxysmal atrial fibrillation in patients with cerebral ischemia. PLoS ONE 2013, 8, e67602. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, N.; Deltour, S.; Vilotijevic, B.; Hornych, A.; Crozier, S.; Leger, A.; Frank, R.; Samson, Y. Detection of paroxysmal atrial fibrillation with transtelephonic EKG in TIA or stroke patients. Neurology 2010, 74, 1666–1670. [Google Scholar] [CrossRef] [PubMed]
- Im, S.I.; Park, D.H.; Kim, B.J.; Cho, K.I.; Kim, H.S.; Heo, J.H. Clinical and electrocardiographic characteristics for prediction of new-onset atrial fibrillation in asymptomatic patients with atrial premature complexes. Int. J. Cardiol. Heart Vasc. 2018, 19, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.J.; Lee, K.Y.; Chung, H.; Kim, I.S.; Choi, E.Y.; Min, P.K.; Yoon, Y.W.; Lee, B.K.; Hong, B.K.; Rim, S.J.; et al. Frequent Premature Atrial Contractions as a Poor Prognostic Factor in Cryptogenic Stroke Patients with Concomitant Non-Sustained Atrial Tachycardia. Yonsei Med. J. 2020, 61, 965–969. [Google Scholar] [CrossRef]
- Durmaz, E.; Ikitimur, B.; Kilickiran Avci, B.; Atıcı, A.; Yurtseven, E.; Tokdil, H.; Ebren, C.; Polat, F.; Karaca, O.; Karadag, B.; et al. The clinical significance of premature atrial contractions: How frequent should they become predictive of new-onset atrial fibrillation. Ann. Noninvasive Electrocardiol. 2020, 25, e12718. [Google Scholar] [CrossRef]
- O’Neal, W.T.; Kamel, H.; Kleindorfer, D.; Judd, S.E.; Howard, G.; Howard, V.J.; Soliman, E.Z. Premature Atrial Contractions on the Screening Electrocardiogram and Risk of Ischemic Stroke: The Reasons for Geographic and Racial Differences in Stroke Study. Neuroepidemiology 2016, 47, 53–58. [Google Scholar] [CrossRef]
- Sajeev, J.K.; Koshy, A.N.; Dewey, H.; Kalman, J.M.; Rajakariar, K.; Tan, M.C.; Street, M.; Roberts, L.; Cooke, J.C.; Wong, M.; et al. Association between excessive premature atrial complexes and cryptogenic stroke: Results of a case-control study. BMJ Open 2019, 9, e029164. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yodogawa, K.; Seino, Y.; Ohara, T.; Hayashi, M.; Miyauchi, Y.; Katoh, T.; Mizuno, K. Prediction of atrial fibrillation after ischemic stroke using P-wave signal averaged electrocardiography. J. Cardiol. 2013, 61, 49–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, L.S.; Juhlin, T.; Juul-Möller, S.; Hedblad, B.; Nilsson, P.M.; Engström, G. A prospective study of supraventricular activity and incidence of atrial fibrillation. Heart Rhythm. 2015, 12, 1898–1904. [Google Scholar] [CrossRef]
- Marinheiro, R.; Parreira, L.; Amador, P.; Sá, C.; Duarte, T.; Caria, R. Excessive atrial ectopic activity as an independent risk factor for ischemic stroke. Int. J. Cardiol. 2017, 249, 226–230. [Google Scholar] [CrossRef]
- Vinther, K.H.; Tveskov, C.; Möller, S.; Auscher, S.; Osmanagic, A.; Egstrup, K. Excessive Premature Atrial Complexes and the Risk of Recurrent Stroke or Death in an Ischemic Stroke Population. J. Stroke Cerebrovasc. Dis. 2017, 26, 1163–1170. [Google Scholar] [CrossRef]
- Raman, D.; Kaffashi, F.; Lui, L.Y.; Sauer, W.H.; Redline, S.; Stone, P.; Cawthon, P.M.; Stone, K.L.; Ensrud, K.E.; Ancoli-Israel, S.; et al. Polysomnographic Heart Rate Variability Indices and Atrial Ectopy Associated with Incident Atrial Fibrillation Risk in Older Community-dwelling Men. JACC Clin. Electrophysiol. 2017, 3, 451–460. [Google Scholar] [CrossRef]
- Persson, A.P.; Fedorowski, A.; Hedblad, B.; Persson, M.; Juul-Moller, S.; Engstrom, G.; Johnson, L.S.B. Heart rate and premature atrial contractions at 24hECG independently predict atrial fibrillation in a population-based study. Heart 2020, 106, 287–291. [Google Scholar] [CrossRef]
- Ntaios, G.; Perlepe, K.; Lambrou, D.; Sirimarco, G.; Strambo, D.; Eskandari, A.; Karagkiozi, E.; Vemmou, A.; Koroboki, E.; Manios, E.; et al. Supraventricular Extrasystoles on Standard 12-lead Electrocardiogram Predict New Incident Atrial Fibrillation after Embolic Stroke of Undetermined Source: The AF-ESUS Study. J. Stroke Cerebrovasc. Dis. 2020, 29, 104626. [Google Scholar] [CrossRef]
- Sejr, M.H.; May, O.; Damgaard, D.; Bruun, N.H.; Nielsen, J.C. Burden of Premature Atrial Complexes and Risk of Recurrent Stroke and Death in Patients with Mild to Moderate Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 104490. [Google Scholar] [CrossRef]
- Vetta, G.; Parlavecchio, A.; Caminiti, R.; Crea, P.; Magnocavallo, M.; Della Rocca, D.G.; Lavalle, C.; Vetta, F.; Marano, G.; Ruggieri, C.; et al. Non-conducted premature atrial complexes: A new independent predictor of atrial fibrillation in cryptogenic stroke. J. Electrocardiol. 2022, 74, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Pinho, J.; Braga, C.G.; Rocha, S.; Santos, A.F.; Gomes, A.; Cabreiro, A.; Magalhães, S.; Ferreira, C. Atrial ectopic activity in cryptogenic ischemic stroke and TIA: A risk factor for recurrence. J. Stroke Cerebrovasc. Dis. 2015, 24, 507–510. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Lin, Y.J.; Chen, Y.Y.; Chang, S.L.; Lo, L.W.; Chao, T.F.; Chung, F.P.; Hu, Y.F.; Chong, E.; Cheng, H.M.; et al. Prognostic Significance of Premature Atrial Complexes Burden in Prediction of Long-Term Outcome. J. Am. Heart Assoc. 2015, 4, e002192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabrera, S.; Vallès, E.; Benito, B.; Alcalde, Ó.; Jiménez, J.; Fan, R.; Martí-Almor, J. Simple predictors for new onset atrial fibrillation. Int. J. Cardiol. 2016, 221, 515–520. [Google Scholar] [CrossRef]
- Hygrell, T.; Stridh, M.; Friberg, L.; Svennberg, E. Prognostic Implications of Supraventricular Arrhythmias. Am. J. Cardiol. 2021, 151, 57–63. [Google Scholar] [CrossRef]
- Sasaki, K.; Nakajima, I.; Higuma, T.; Yamada, M.; Kasagawa, A.; Togashi, D.; Harada, T.; Akashi, Y.J. Revisit to the Prognostic Value of Premature Atrial Contraction Burden in 24-h Holter Electrocardiography for Predicting Undiagnosed Atrial Fibrillation-A Propensity Score-Matched Study. Circ. J. 2021, 85, 1265–1272. [Google Scholar] [CrossRef]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef]
- Yang, M.; Cheng, H.; Wang, X.; Ouyang, M.; Shajahan, S.; Carcel, C.; Anderson, C.; Kristoffersen, E.S.; Lin, Y.; Sandset, E.C.; et al. Antithrombotics prescription and adherence among stroke survivors: A systematic review and meta-analysis. Brain Behav. 2022, 12, e2752. [Google Scholar] [CrossRef]
- Ziegler, P.D.; Glotzer, T.V.; Daoud, E.G.; Singer, D.E.; Ezekowitz, M.D.; Hoyt, R.H.; Koehler, J.L.; Coles, J., Jr.; Wyse, D.G. Detection of previously undiagnosed atrial fibrillation in patients with stroke risk factors and usefulness of continuous monitoring in primary stroke prevention. Am. J. Cardiol. 2012, 110, 1309–1314. [Google Scholar] [CrossRef]
- Lazzaro, M.A.; Krishnan, K.; Prabhakaran, S. Detection of atrial fibrillation with concurrent holter monitoring and continuous cardiac telemetry following ischemic stroke and transient ischemic attack. J. Stroke Cerebrovasc. Dis. 2012, 21, 89–93. [Google Scholar] [CrossRef]
- Ariyarajah, V.; Apiyasawat, S.; Fernandes, J.; Kranis, M.; Spodick, D.H. Association of atrial fibrillation in patients with interatrial block over prospectively followed controls with comparable echocardiographic parameters. Am. J. Cardiol. 2007, 99, 390–392. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A.; Martí, L.; Dorison, S.; Sánchez, M.J. Bayés syndrome and acute cardioembolic ischemic stroke. World J. Clin. Cases. 2017, 5, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Hughes, T.M.; Worrall, B.B. Acute interatrial block is a distinct risk factor for ischemic stroke. Neurology 2016, 87, 344–345. [Google Scholar] [CrossRef] [PubMed]
- Bacharova, L.; Wagner, G.S. The time for naming the Interatrial Block Syndrome: Bayes Syndrome. J. Electrocardiol. 2015, 48, 133–134. [Google Scholar] [CrossRef] [PubMed]
- Ariyarajah, V.; Puri, P.; Apiyasawat, S.; Spodick, D.H. Interatrial block: A novel risk factor for embolic stroke? Ann. Noninvasive Electrocardiol. 2007, 12, 15–20. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Study Design | Population | Number of Subjects | Age (Means ± SD) | Male n (%) | Concomitant Diseases (%) | Follow-up |
|---|---|---|---|---|---|---|---|---|
| Binici 2010 [12] | Denmark | Prospective cohort | Without CVD, stroke, or AF | 678 | 64.5 ± 6.8 | 397 (58.6) | Diabetes (11.1) | 6.3 years |
| Chong 2012 [13] | China | Prospective cohort | Without AF or structural heart disease | 428 | 66.7 ± 10.2 | 187 (43.7) | Hypertension (45.3) Diabetes (17.1) CVD (17.5) | 6.1 years |
| Dewland 2013 [14] | United States | Prospective cohort | Without prevalent AF | 1260 | 71 | 569 (45) | Hypertension (55) Diabetes (15) CVD (20) | 13.0 years |
| Yodogawa 2013 [33] | Japan | Prospective cohort | With AIS, without a history of AF | 68 | 69.9 ± 9.6 | 37 (54.4) | Hypertension (66.2) Diabetes (14.7) | 11 ± 4 months |
| Pinho 2015 [42] | Portugal | Retrospective cohort | With CIS or TIA | 184 | 55.2 ± 15.1 | 96 (52.2) | Hypertension (56.5) Diabetes (14.7) Dyslipidemia (72.8) CVD (3.3) | 27.5 months |
| Acharya 2015 [15] | United States | Retrospective cohort | Free of AF | 1357 | 64 | 1262 (93) | Hypertension (66) Diabetes (22.6) CVD (19.7) | 7.5 years |
| Johnson 2015 [34] | Sweden | Prospective cohort | Free of AF | 383 | 64.6 ± 5.9 | 172 (45) | - | 10.3 years |
| Lin 2015 [43] | China | Retrospective cohort | Without AF and a PPM | 5371 | 61.8 ± 18.6 | 3222 (60) | Hypertension (35.6) Diabetes (20.2) Dyslipidemia (12.8) CVD (29.4) | 10 ± 1 years |
| Larsen 2015 [23] | Denmark | Prospective cohort | Without CVD, stroke, or AF | 678 | 64.5 ± 6.8 | 397 (58.6) | Diabetes (11.1) | 14.4 years |
| Vinther 2016 [22] | Denmark | Retrospective cohort | With IS and without known AF | 565 | - | 313 (55.4) | Hypertension (41.9) Diabetes (10.8) | 4 years |
| Cabrera 2016 [44] | Spain | Retrospective cohort | Free of AF | 299 | 62.5 ± 17.9 | 160 (53.5) | Hypertension (52.3) Diabetes (17.4) | 39.1 months |
| Marinheiro 2017 [35] | Portugal | Prospective cohort | Without stroke or AF | 362 | - | 204 (56.4) | Hypertension (77.6) Diabetes (25.1) | 7.1 years |
| Vinther 2017 [36] | Denmark | Prospective cohort | With AIS and without AF | 256 | 73 ± 12.6 | 141 (55) | Hypertension (57) Diabetes (13) Dyslipidemia (28) CVD (13) | 32 months |
| Raman 2017 [37] | United States | Prospective cohort | Without baseline AF | 2350 | 75.8 ± 5.3 | 2350 (100) | Hypertension (49) Diabetes (13.1) | 8.0 ± 2.6 years |
| Persson 2019 [38] | Sweden | Prospective cohort | Free of AF | 377 | 65 ± 6 | 170 (45) | - | 17 years |
| Ntaios 2020 [39] | United Kingdom | Prospective cohort | Embolic Stroke of Undetermined Source | 853 | 67 | 486 (57) | Hypertension (61.9) Diabetes (18.5) CVD (15) | 3.4 years |
| Sejr 2020 [40] | Denmark | Prospective cohort | with AIS or TIA and without AF | 1453 | 72.8 ± 7.7 | 822 (56.6) | Hypertension (58.6) Diabetes (14.3) | 2.3 ± 1.3 years |
| Hygrell 2021 [45] | Sweden | Retrospective cohort | Free of AF | 6100 | 76 | 2755 (45) | Hypertension (28) Diabetes (10) | 4.2 years |
| Sasaki 2021 [46] | Japan | Retrospective cohort | Free of AF | 138 | 72 ± 10 | 108 (52) | Hypertension (62.3) Diabetes (23.9) Dyslipidemia (39.1) | 5 years |
| Vetta 2022 [41] | Italy | Prospective cohort | With cryptogenic stroke | 112 | 72.2 ± 12.2 | 65 (58) | Hypertension (81) Diabetes (21) CVD (9) | 6 months |
| Study | Definition of ESVEA | Detection of ESVEA | Prevalence of ESVEA n (%) | Definition of Outcome | Numbers of Outcome n (%) |
|---|---|---|---|---|---|
| Binici 2010 [12] | ≥30 SVEC/h or any episode of runs of ≥20 SVEC | 48 h ECG | 99 (14.6) | AF IS All-cause mortality | 22 (5.5) 27 (6.7) 87 (21.4) |
| Chong 2012 [13] | >100 PACs/24 h | 24 h ECG | 107 (25) | AF IS Death | 60 (14) 41 (9.6) 60 (14) |
| Dewland 2013 [14] | The median PAC count was 2.5 beats/h (IQR, 0.8 to 9.5 beats/h) | 24 h ECG | - | AF All-cause mortality | 343 (27.2) 837 (66.4) |
| Yodogawa 2013 [33] | >100 PACs/24 h | 24 h ECG | - | AF | 17 (25) |
| Pinho 2015 [42] | >30 APCs/h | 24 h ECG | 17 (9.2) | Recurrent IS/TIA | 22 (12) |
| Acharya 2015 [15] | ≥100 PACs/24 h | 24 h ECG | 486 (35.8) | AF | 155 (11.4) |
| Johnson 2015 [34] | 30 SVE/h and/or any SVT lasting for ≥20 consecutive beats | 24 h ECG | - | AF | 45 (11.7) |
| Lin 2015 [43] | PAC burden >76 beats per day | 24 h ECG | 2072 (38.6) | All-cause mortality AF | 1209 (22.5) 418 (7.8) |
| Larsen 2015 [23] | ≥30 PACs/h or any episode of runs of ≥20 PACs | 48 h ECG | 99 (14.6) | IS All-cause mortality | 73 (10.8) 259 (38.2) |
| Vinther 2016 [22] | ≥3 PACs lasting less than 30 s during 48 h | 48 h of CICT | 161 (28) | Recurrent IS/TIA All-cause mortality AF | 73 (12.9) 158 (28) 22 (3.9) |
| Cabrera 2016 [44] | Percentage of PAC (during the 24 h period) ≥0.2% | 24 h ECG | - | AF | 31 (10.4) |
| Marinheiro 2017 [35] | >97 PACs/h | 24 h ECG | 124 (34.3) | IS All-cause mortality | 54 (14.9) 129 (35.6) |
| 30–97 PACs/h | 114 (31.5) | ||||
| Vinther 2017 [36] | >14 PACs/h and ≥3 runs of PACs/24 h | 24 h ECG | 31 (12.1) | Recurrent stroke All-cause mortality | 20 (7.8) 34 (13.3) |
| Raman 2017 [37] | PAC/h of sleep ≥ 21.15 | PSG based ECG | - | AF | 269 (11.4) |
| Persson 2019 [38] | Top quartile of PACs (≥5.5 per hour) or SVT (≥0.13 per hour) | 24 h ECG | - | AF | 80 (21.2) |
| Ntaios 2020 [39] | >0–1 SVE per 10 s | 12-lead ECG | 111 (13) | AF Recurrent IS All-cause mortality | 125 (14.7) 103 (12.1) 149 (17.5) |
| >1–2 SVE per 10 s | 57 (6.7) | ||||
| >2 SVE per 10 s | 58 (6.8) | ||||
| Sejr 2020 [40] | 0.5–1.5 PACs/h | 48 h ECG | 359 (24.7) | AF Recurrent IS Recurrent TIA All-cause mortality | 44 (2.9) 78 (5.4) 76 (5.2) 123 (8.5) |
| 1.6–5.9 PACs/h | 365 (25.1) | ||||
| ≥6.0 PACs/h | 362 (24.9) | ||||
| Hygrell 2021 [45] | the top tenth percentile according to SVECs count | 30 s ECG | 709 (11.6) | AF IS Death | 387 (6.3) 161 (2.6) 354 (5.8) |
| Sasaki 2021 [46] | PAC burden ≥ 0.4% | 24 h ECG | - | AF | 61 (29.3) |
| Vetta 2022 [41] | PACs burden ≥ 7 | 24 h ECG | - | AF | 24 (21.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, M.; Lin, Y.; Cheng, H.; Zheng, D.; Tan, S.; Zhu, L.; Li, Z.; Wang, X.; Yang, J. Excessive Supraventricular Ectopic Activity and the Risk of Atrial Fibrillation and Stroke: A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2022, 9, 461. https://doi.org/10.3390/jcdd9120461
Yang M, Lin Y, Cheng H, Zheng D, Tan S, Zhu L, Li Z, Wang X, Yang J. Excessive Supraventricular Ectopic Activity and the Risk of Atrial Fibrillation and Stroke: A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease. 2022; 9(12):461. https://doi.org/10.3390/jcdd9120461
Chicago/Turabian StyleYang, Min, Yapeng Lin, Hang Cheng, Danni Zheng, Song Tan, Liping Zhu, Zimeng Li, Xiaoyun Wang, and Jie Yang. 2022. "Excessive Supraventricular Ectopic Activity and the Risk of Atrial Fibrillation and Stroke: A Systematic Review and Meta-Analysis" Journal of Cardiovascular Development and Disease 9, no. 12: 461. https://doi.org/10.3390/jcdd9120461