
Management of May Thurner Syndrome in Pregnant Patients
 ,
,
Abstract
:1. Introduction
2. Cases
3. Discussion
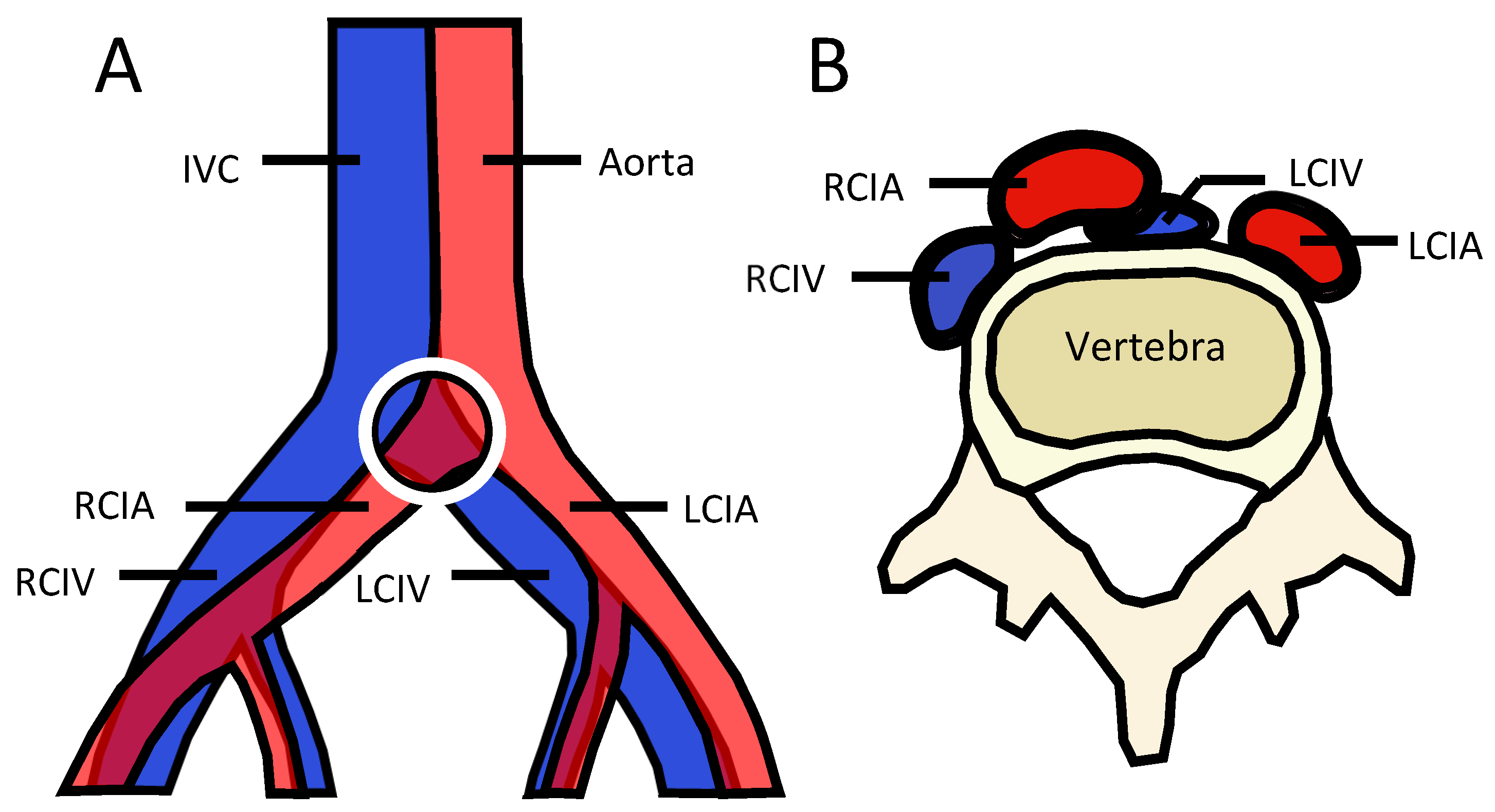
3.1. Diagnosis
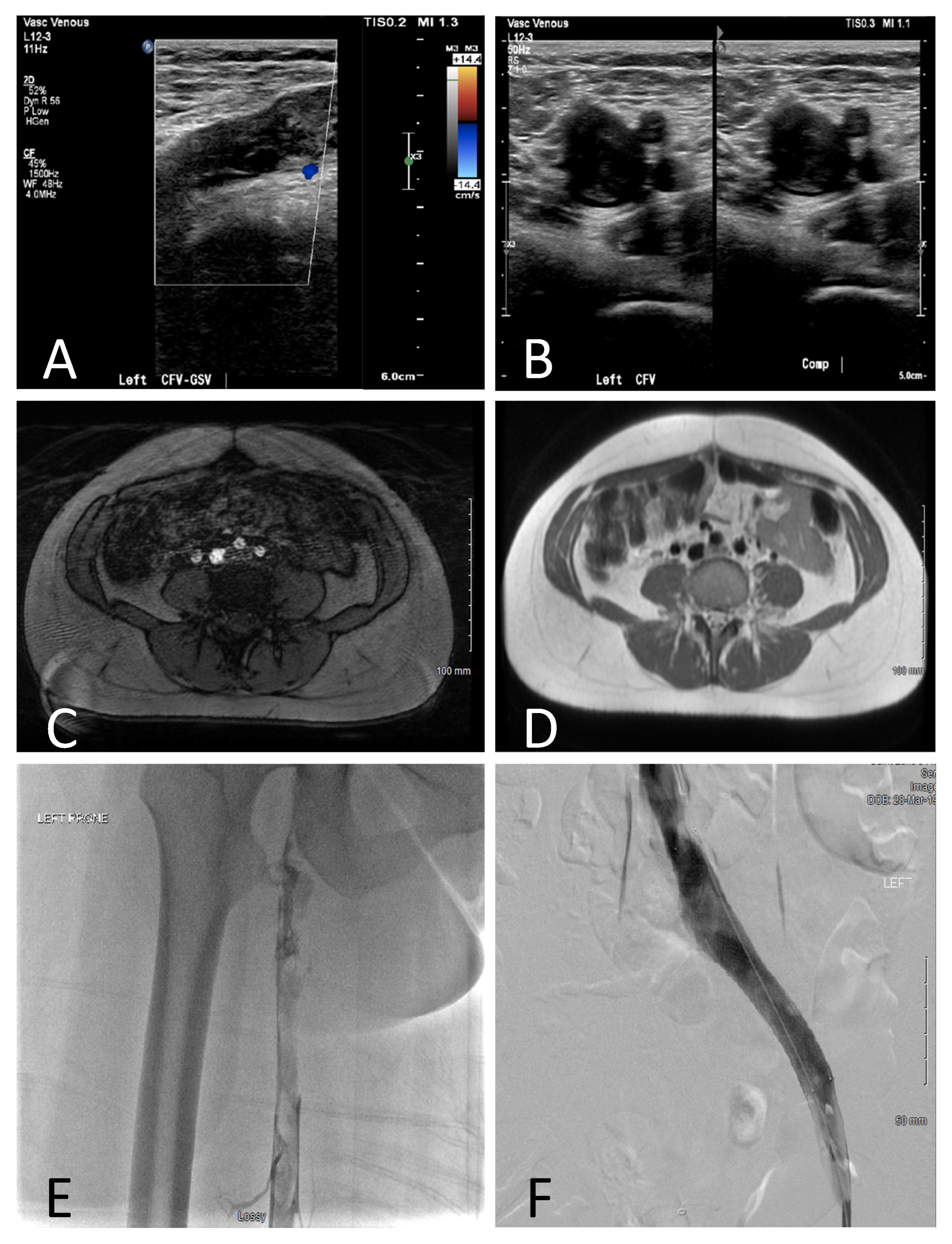
3.1.1. Ultrasound
3.1.2. Magnetic Resonance Imaging
3.1.3. Computed Tomography and Venography
3.1.4. Intravenous Ultrasound
3.2. Radiation Exposure
3.3. Surgical Management
3.3.1. Endovascular Therapy
3.3.2. Vascular Stent Placement
3.4. Pharmacologic Management
Anticoagulation
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- May, R.; Thurner, J. The Cause of the Predominantly Sinistral Occurrence of Thrombosis of the Pelvic Veins. Angiology 1957, 8, 419–427. [Google Scholar] [CrossRef]
- Goto, M.; Miura, S.-I.; Yamamoto, T.; Fukuda, Y.; Kuwano, T.; Kimura, I.; Sanui, A.; Miyamoto, S.; Saku, K. Anticoagulant Therapy in a Pregnant Woman with May-Thurner Syndrome. Intern. Med. 2016, 55, 59–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mousa, A.Y.; AbuRahma, A.F. May–Thurner Syndrome: Update and Review. Ann. Vasc. Surg. 2013, 27, 984–995. [Google Scholar] [CrossRef] [PubMed]
- Cockett, F. The Iliac Compression Syndrome Alias “iliofemoral Thrombosis” of “White Leg”. Proc. R. Soc. Med. 1966, 59, 360–361. [Google Scholar] [PubMed]
- Cockett, F.B.; Thomas, M.L. The Iliac Compression Syndrome. Br. J. Surg. 1965, 52, 816. [Google Scholar] [CrossRef]
- O’Sullivan, G.J.; Semba, C.P.; Bittner, C.A.; Kee, S.T.; Razavi, M.K.; Sze, D.Y.; Dake, M.D. Endovascular Management of Iliac Vein Compression (May-Thurner) Syndrome. J. Vasc. Interv. Radiol. 2000, 11, 823–836. [Google Scholar] [CrossRef]
- Ehrich, W.E.; Krumbhaar, E.B. A Frequent Obstructive Anomaly of the Mouth of the Left Common Iliac Vein. Am. Heart J. 1943, 26, 737–750. [Google Scholar] [CrossRef]
- Mcmurrich, J.P. The Occurrence of Congenital Adhesions in the Commone Iliac Veins, and Their Relation to Thrombosis of the Femoral and Iliac Veins. Am. J. Med. Sci. 1908, 135, 342. [Google Scholar] [CrossRef] [Green Version]
- Mewissen, M.W.; Seabrook, G.R.; Meissner, M.H.; Cynamon, J.; Labropoulos, N.; Haughton, S.H. Catheter-Directed Thrombolysis for Lower Extremity Deep Venous Thrombosis: Report of a National Multicenter Registry. Radiology 1999, 211, 39–49. [Google Scholar] [CrossRef]
- Oguzkurt, L.; Tercan, F.; Ozkan, U.; Gulcan, O. Iliac Vein Compression Syndrome: Outcome of Endovascular Treatment with Long-Term Follow-Up. Eur. J. Radiol. 2008, 68, 487–492. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Committee on Practice Bulletins—Obstetrics ACOG Practice Bulletin No. 196: Thromboembolism in Pregnancy. Obs. Gynecol 2018, 132, e1–e17. [Google Scholar] [CrossRef] [PubMed]
- Labropoulos, N.; Leon, L.R. Duplex Evaluation of Venous Insufficiency. Semin. Vasc. Surg. 2005, 18, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Oguzkurt, L.; Tercan, F.; Pourbagher, M.A.; Kizilkilic, O.; Turkoz, R.; Boyvat, F. Computed Tomography Findings in 10 Cases of Iliac Vein Compression (May–Thurner) Syndrome. Eur. J. Radiol. 2005, 55, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Ou-Yang, L.; Lu, G. Underlying Anatomy and Typing Diagnosis of May-Thurner Syndrome and Clinical Significance. Spine (Phila Pa 1976) 2016, 41, E1284–E1291. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-Y.; Choi, D.; Guk Ko, Y.; Park, S.; Jang, Y.; Lee, D.Y. Percutaneous Treatment of Deep Vein Thrombosis in May-Thurner Syndrome. Cardiovasc. Intervent. Radiol. 2006, 29, 571–575. [Google Scholar] [CrossRef]
- van Vuuren, T.M.A.J.; Kurstjens, R.L.M.; Wittens, C.H.A.; van Laanen, J.H.H.; de Graaf, R. Illusory Angiographic Signs of Significant Iliac Vein Compression in Healthy Volunteers. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 874–879. [Google Scholar] [CrossRef] [Green Version]
- Zamboni, P.; Franceschi, C. How to Assess Illusory May-Thurner Syndrome by Ultrasound. Eur. J. Vasc. Endovasc. Surg. 2019, 58, 305. [Google Scholar] [CrossRef]
- Chan, W.S.; Spencer, F.A.; Ginsbergm, J.S. Anatomic Distribution of Deep Vein Thrombosis in Pregnancy. Can. Med. Assoc. J. 2010, 182, 657–660. [Google Scholar] [CrossRef] [Green Version]
- James, A.H.; Tapson, V.F.; Goldhaber, S.Z. Thrombosis during Pregnancy and the Postpartum Period. Am. J. Obstet. Gynecol. 2005, 193, 216–219. [Google Scholar] [CrossRef]
- Ray, J.G.; Chan, W.S. Deep Vein Thrombosis During Pregnancy and the Puerperium: A Meta-Analysis of the Period of Risk and the Leg of Presentation. Obstet. Gynecol. Surv. 1999, 54, 265–271. [Google Scholar] [CrossRef]
- Brinegar, K.N.; Sheth, R.A.; Khademhosseini, A.; Bautista, J.; Oklu, R. Iliac Vein Compression Syndrome: Clinical, Imaging and Pathologic Findings. World J. Radiol. 2015, 7, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Radaideh, Q.; Patel, N.; Shammas, N.W. Iliac Vein Compression: Epidemiology, Diagnosis and Treatment. Vasc. Health Risk Manag. 2019, 15, 115–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zucker, E.J.; Ganguli, S.; Ghoshhajra, B.B.; Gupta, R.; Prabhakar, A.M. Imaging of Venous Compression Syndromes. Cardiovasc Diagn 2016, 6, 519–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clements, H.; Duncan, K.R.; Fielding, K.; Gowland, P.A.; Johnson, I.R.; Baker, P.N. Infants Exposed to MRI in Utero Have a Normal Paediatric Assessment at 9 Months of Age. Br. J. Radiol. 2000, 73, 190–194. [Google Scholar] [CrossRef]
- Kok, R.D.; de Vries, M.M.; Heerschap, A.; van den Berg, P.P. Absence of Harmful Effects of Magnetic Resonance Exposure at 1.5 T in Utero during the Third Trimester of Pregnancy: A Follow-up Study. Magn Reson Imaging 2004, 22, 851–854. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.N.; Johnson, I.R.; Harvey, P.R.; Gowland, P.A.; Mansfield, P. A Three-Year Follow-up of Children Imaged in Utero with Echo-Planar Magnetic Resonance. Am. J. Obstet. Gynecol. 1994, 170, 32–33. [Google Scholar] [CrossRef]
- Glover, P.; Hykin, J.; Gowland, P.; Wright, J.; Johnson, I.; Mansfield, P. An Assessment of the Intrauterine Sound Intensity Level during Obstetric Echo-Planar Magnetic Resonance Imaging. Br. J. Radiol 1995, 68, 1090–1094. [Google Scholar] [CrossRef] [PubMed]
- Jain, C. ACOG Committee Opinion No. 723: Guidelines for Diagnostic Imaging During Pregnancy and Lactation. Obstet. Gynecol. 2019, 133, 186. [Google Scholar] [CrossRef]
- Dronkers, C.E.A.; Srámek, A.; Huisman, M.V.; Klok, F.A. Accurate Diagnosis of Iliac Vein Thrombosis in Pregnancy with Magnetic Resonance Direct Thrombus Imaging (MRDTI). BMJ Case Rep. 2016, 2016, bcr2016218091. [Google Scholar] [CrossRef]
- Meissner, M.H.; Gloviczki, P.; Comerota, A.J.; Dalsing, M.C.; Eklof, B.G.; Gillespie, D.L.; Lohr, J.M.; McLafferty, R.B.; Murad, M.H.; Padberg, F.; et al. Early Thrombus Removal Strategies for Acute Deep Venous Thrombosis: Clinical Practice Guidelines of the Society for Vascular Surgery and the American Venous Forum. J. Vasc. Surg. 2012, 55, 1449–1462. [Google Scholar] [CrossRef]
- Thomas, S.M.; Goodacre, S.W.; Sampson, F.C.; van Beek, E.J.R. Diagnostic Value of CT for Deep Vein Thrombosis: Results of a Systematic Review and Meta-Analysis. Clin. Radiol. 2008, 63, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.W.; Yoon, C.J.; Jung, S.I.; Kim, H.-C.; Lee, W.; Kim, Y.I.; Jae, H.J.; Park, J.H. Acute Iliofemoral Deep Vein Thrombosis: Evaluation of Underlying Anatomic Abnormalities by Spiral CT Venography. J. Vasc. Interv. Radiol. 2004, 15, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Birn, J.; Vedantham, S. May–Thurner Syndrome and Other Obstructive Iliac Vein Lesions: Meaning, Myth, and Mystery. Vasc. Med. 2015, 20, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Albrechtsson, U.; Einarsson, E.; Eklöf, B. Femoral Vein Pressure Measurements for Evaluation of Venous Function in Patients with Postthrombotic Iliac Veins. Cardiovasc. Intervent. Radiol 1981, 4, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Raju, S.; Neglen, P. High Prevalence of Nonthrombotic Iliac Vein Lesions in Chronic Venous Disease: A Permissive Role in Pathogenicity. J. Vasc. Surg. 2006, 44, 136–143; discussion 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vedantham, S.; Sista, A.K.; Klein, S.J.; Nayak, L.; Razavi, M.K.; Kalva, S.P.; Saad, W.E.; Dariushnia, S.R.; Caplin, D.M.; Chao, C.P.; et al. Quality Improvement Guidelines for the Treatment of Lower-Extremity Deep Vein Thrombosis with Use of Endovascular Thrombus Removal. J. Vasc. Interv. Radiol. 2014, 25, 1317–1325. [Google Scholar] [CrossRef]
- Bloom, A.I.; Farkas, A.; Kalish, Y.; Elchalal, U.; Spectre, G. Pharmacomechanical Catheter-Directed Thrombolysis for Pregnancy-Related Iliofemoral Deep Vein Thrombosis. J. Vasc. Interv. Radiol. 2015, 26, 992–1000. [Google Scholar] [CrossRef]
- Herrera, S.; Comerota, A.J.; Thakur, S.; Sunderji, S.; DiSalle, R.; Kazanjian, S.N.; Assi, Z. Managing Iliofemoral Deep Venous Thrombosis of Pregnancy with a Strategy of Thrombus Removal Is Safe and Avoids Post-Thrombotic Morbidity. J. Vasc. Surg. 2014, 59, 456–464. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.-W.; Liu, P.-Y. Postpartum Deep Vein Thrombosis Resolved by Catheter-Directed Thrombolysis: A Case Report. Medicine 2019, 98, e16052. [Google Scholar] [CrossRef]
- DeStephano, C.C.; Werner, E.F.; Holly, B.P.; Lessne, M.L. Diagnosis and Management of Iliac Vein Thrombosis in Pregnancy Resulting from May–Thurner Syndrome. J. Perinatol. 2014, 34, 566–568. [Google Scholar] [CrossRef]
- Du, X.; Zhuang, H.; Hong, L.; Zhang, Y.; Li, C.; Qian, A.; Sang, H.; Li, X. Long-Term Outcome of Catheter-Directed Thrombolysis in Pregnancy-Related Venous Thrombosis. Med. Sci. Monit. 2019, 25, 3771–3777. [Google Scholar] [CrossRef]
- Krishnamurthy, P.; Martin, C.B.; Kay, H.H.; Diesner, J.; Friday, R.O.; Weber, C.A.; Droste, S. Catheter-Directed Thrombolysis for Thromboembolic Disease During Pregnancy: A Viable Option. J. Matern. Fetal. Neonatal. Med. 1999, 8, 24–27. [Google Scholar] [CrossRef]
- Siah, T.H.; Chapman, A. Should Catheter-Directed Thrombolysis Be the Standard of Care for Pregnancy-Related Iliofemoral Deep Vein Thrombosis? BMJ Case Rep. 2018, 2018, bcr-2017-223105. [Google Scholar] [CrossRef]
- Pillny, M.; Sandmann, W.; Luther, B.; Müller, B.T.; Tutschek, B.; Gerhardt, A.; Zotz, R.B.; Scharf, R.E. Deep Venous Thrombosis during Pregnancy and after Delivery: Indications for and Results of Thrombectomy. J. Vasc. Surg. 2003, 37, 528–532. [Google Scholar] [CrossRef] [Green Version]
- Wong, P.C.; Chan, Y.C.; Law, Y.; Cheng, S.W.K. Percutaneous Mechanical Thrombectomy in the Treatment of Acute Iliofemoral Deep Vein Thrombosis: A Systematic Review. Hong Kong Med. J. 2019, 25, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Mickley, V.; Schwagierek, R.; Rilinger, N.; Görich, J.; Sunder-Plassmann, L. Left Iliac Venous Thrombosis Caused by Venous Spur: Treatment with Thrombectomy and Stent Implantation. J. Vasc. Surg. 1998, 28, 492–497. [Google Scholar] [CrossRef] [Green Version]
- Neglén, P.; Hollis, K.C.; Olivier, J.; Raju, S. Stenting of the Venous Outflow in Chronic Venous Disease: Long-Term Stent-Related Outcome, Clinical, and Hemodynamic Result. J. Vasc. Surg. 2007, 46, 979–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vedantham, S.; Thorpe, P.E.; Cardella, J.F.; Grassi, C.J.; Patel, N.H.; Ferral, H.; Hofmann, L.V.; Janne d’Othée, B.M.; Antonaci, V.P.; Brountzos, E.N.; et al. Quality Improvement Guidelines for the Treatment of Lower Extremity Deep Vein Thrombosis with Use of Endovascular Thrombus Removal. J. Vasc. Interv. Radiol. 2006, 17, 435–447; quiz 448. [Google Scholar] [CrossRef] [Green Version]
- Vedantham, S.; Millward, S.F.; Cardella, J.F.; Hofmann, L.V.; Razavi, M.K.; Grassi, C.J.; Sacks, D.; Kinney, T.B. Society of Interventional Radiology Position Statement: Treatment of Acute Iliofemoral Deep Vein Thrombosis with Use of Adjunctive Catheter-Directed Intrathrombus Thrombolysis. J. Vasc. Interv. Radiol. 2009, 20, S332–S335. [Google Scholar] [CrossRef]
- Mangla, A.; Hamad, H. May-Thurner Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Liu, Q.; Liu, F.; Lü, P.; Wu, H.; Ye, P.; You, Y.; Yao, Z. Current Status and Prospect of Stent Placement for May-Thurner Syndrome. Curr. Med. Sci. 2021, 41, 1178–1186. [Google Scholar] [CrossRef]
- Sigua-Arce, P.; Mando, R.; Spencer, L.; Halalau, A. Treatment of May–Thurner’s Syndrome and Associated Complications: A Multicenter Experience. Int. J. Gen. Med. 2021, 14, 4705–4710. [Google Scholar] [CrossRef] [PubMed]
- Jayaraj, A.; Buck, W.; Knight, A.; Johns, B.; Raju, S. Impact of Degree of Stenosis in May-Thurner Syndrome on Iliac Vein Stenting. J. Vasc. Surg. Venous Lymphat. Disord. 2019, 7, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Saleem, T.; Raju, S. An Overview of In-Stent Restenosis in Iliofemoral Venous Stents. J. Vasc. Surg. Venous Lymphat. Disord. 2022, 10, 492–503.e2. [Google Scholar] [CrossRef] [PubMed]
- Mando, R.; Sigua-Arce, P.; Spencer, L.; Halalau, A. Slippery Stents: A Case Report and Review of the Literature Describing Patients with May-Thurner Syndrome That Experienced Stent Migration. Case Rep. Vasc. Med. 2019, 2019, 7606727. [Google Scholar] [CrossRef] [Green Version]
- Hartung, O.; Benmiloud, F.; Barthelemy, P.; Dubuc, M.; Boufi, M.; Alimi, Y.S. Late Results of Surgical Venous Thrombectomy with Iliocaval Stenting. J. Vasc. Surg. 2008, 47, 381–387. [Google Scholar] [CrossRef] [Green Version]
- Dasari, M.; Avgerinos, E.; Raju, S.; Tahara, R.; Chaer, R.A. Outcomes of Iliac Vein Stents after Pregnancy. J. Vasc. Surg. Venous Lymphat. Disord. 2017, 5, 353–357. [Google Scholar] [CrossRef]
- Bates, S.M.; Greer, I.A.; Middeldorp, S.; Veenstra, D.L.; Prabulos, A.-M.; Vandvik, P.O. VTE, Thrombophilia, Antithrombotic Therapy, and Pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th Ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, e691S–e736S. [Google Scholar] [CrossRef] [Green Version]
- Comerota, A.J.; Grewal, N.; Martinez, J.T.; Chen, J.T.; DiSalle, R.; Andrews, L.; Sepanski, D.; Assi, Z. Postthrombotic Morbidity Correlates with Residual Thrombus Following Catheter-Directed Thrombolysis for Iliofemoral Deep Vein Thrombosis. J. Vasc. Surg. 2012, 55, 768–773. [Google Scholar] [CrossRef] [Green Version]
- Bozkaya, H.; Cinar, C.; Ertugay, S.; Korkmaz, M.; Guneyli, S.; Posacioglu, H.; Parıldar, M. Endovascular Treatment of Iliac Vein Compression (May-Thurner) Syndrome: Angioplasty and Stenting with or without Manual Aspiration Thrombectomy and Catheter-Directed Thrombolysis. Ann. Vasc. Dis. 2015, 8, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Watson, L.; Broderick, C.; Armon, M.P. Thrombolysis for Acute Deep Vein Thrombosis. Cochrane Database Syst. Rev. 2016, 11, CD002783. [Google Scholar] [CrossRef]
- Sitruk-Ware, R.; Nath, A. Metabolic Effects of Contraceptive Steroids. Rev. Endocr. Metab. Disord. 2011, 12, 63–75. [Google Scholar] [CrossRef]
- Aburahma, A.F.; Boland, J.P. Management of Deep Vein Thrombosis of the Lower Extremity in Pregnancy: A Challenging Dilemma. Am. Surg. 1999, 65, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Obstetricians and Gynaecologists. Thrombosis and Embolism during Pregnancy and the Puerperium: Acute Management (Green-Top Guideline No. 37b). 2015. Available online: https://www.rcog.org.uk/media/wj2lpco5/gtg-37b-1.pdf (accessed on 28 September 2022).
- Gould, M.K.; Dembitzer, A.D.; Doyle, R.L.; Hastie, T.J.; Garber, A.M. Low-Molecular-Weight Heparins Compared with Unfractionated Heparin for Treatment of Acute Deep Venous Thrombosis. A Meta-Analysis of Randomized, Controlled Trials. Ann. Intern. Med. 1999, 130, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, B.; Rambiritch, V.; Paek, D.; Sayre, T.; Naidoo, P.; Shan, J.; Leisegang, R. Safety and Efficacy of Enoxaparin in Pregnancy: A Systematic Review and Meta-Analysis. Adv. 2020, 37, 27–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leffert, L.; Butwick, A.; Carvalho, B.; Arendt, K.; Bates, S.M.; Friedman, A.; Horlocker, T.; Houle, T.; Landau, R.; Dubois, H.; et al. The Society for Obstetric Anesthesia and Perinatology Consensus Statement on the Anesthetic Management of Pregnant and Postpartum Women Receiving Thromboprophylaxis or Higher Dose Anticoagulants. Anesth. Analg. 2018, 126, 928–944. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Case/Age | GP | History | GA at MTS Diagnosis | Diagnostic Modality | Management | Obstetric Outcome | Complications (Obstetric/Venous) |
|---|---|---|---|---|---|---|---|
| 1/29 | G2P2 | 9 | Doppler/Duplex US (DVT LCFV to tibial), MRI/A/V (DVT extending from IVC, LCIV, LCFV, c/w MTS), venography (MTS) | UFH, CDT, balloon angioplasty of LCIV and LSFV. Adjusted dose LMWH, continued through 8 wks PP, ASA, compression stockings. LCIV stent PP. | SVD at term | None | |
| 2a */29 | G1P1 | h/o DVT, known MTS with h/o LCIV stent | NA | Initial diagnosis with Duplex US (MTS) | Adjusted dose LMWH, transitioned to UFH, ASA, compression stockings. LMWH continued for 6 wks PP with ASA. | IOL at 39 wks, SVD Female 3690 g (83%) | None |
| 2b ‡/32 | G2P2 | NA | Adjusted dose LMWH, transitioned to UFH, ASA, compression stockings. LMWH continued for 6 wks PP with ASA. | IOL at 40 wks, SVD Male 4470 g (98%) | None | ||
| 3/33 | G2P2 | Known MTS with h/o LCIV stent, followed by complete stent occlusion | NA | Initial diagnosis with Duplex US, venogram/IVUS (MTS) | Adjusted dose LMWH, transitioned to UFH, ASA, compression stockings. LMWH bridged to warfarin postpartum. | IOL at 39, SVD Male 3060 g (27%) | None |
| 4/33 | G4P4 | Pelvic/perineal varicosities | 3 | Duplex US (pelvic congestion, reflux and collaterals), venogram/IVUS (MTS) | LCIV and LEIV stents placed early pregnancy (prior to knowledge of pregnancy). Prophylactic LMWH transitioned to UFH, ASA, compression stockings. Prophylactic LMWH PP. | SVD at 39 Male, 3593 g (69%) | Gonadal v. thrombosis 6 d PP, (single missed dose of LMWH) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schrufer-Poland, T.L.; Florio, K.; Grodzinsky, A.; Borsa, J.J.; Schmidt, L. Management of May Thurner Syndrome in Pregnant Patients. J. Cardiovasc. Dev. Dis. 2022, 9, 410. https://doi.org/10.3390/jcdd9120410
Schrufer-Poland TL, Florio K, Grodzinsky A, Borsa JJ, Schmidt L. Management of May Thurner Syndrome in Pregnant Patients. Journal of Cardiovascular Development and Disease. 2022; 9(12):410. https://doi.org/10.3390/jcdd9120410
Chicago/Turabian StyleSchrufer-Poland, Tabitha L., Karen Florio, Anna Grodzinsky, John J. Borsa, and Laura Schmidt. 2022. "Management of May Thurner Syndrome in Pregnant Patients" Journal of Cardiovascular Development and Disease 9, no. 12: 410. https://doi.org/10.3390/jcdd9120410