
A Meta-Analysis on the Impact of High BMI in Patients Undergoing Transcatheter Aortic Valve Replacement
 , ,
, ,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
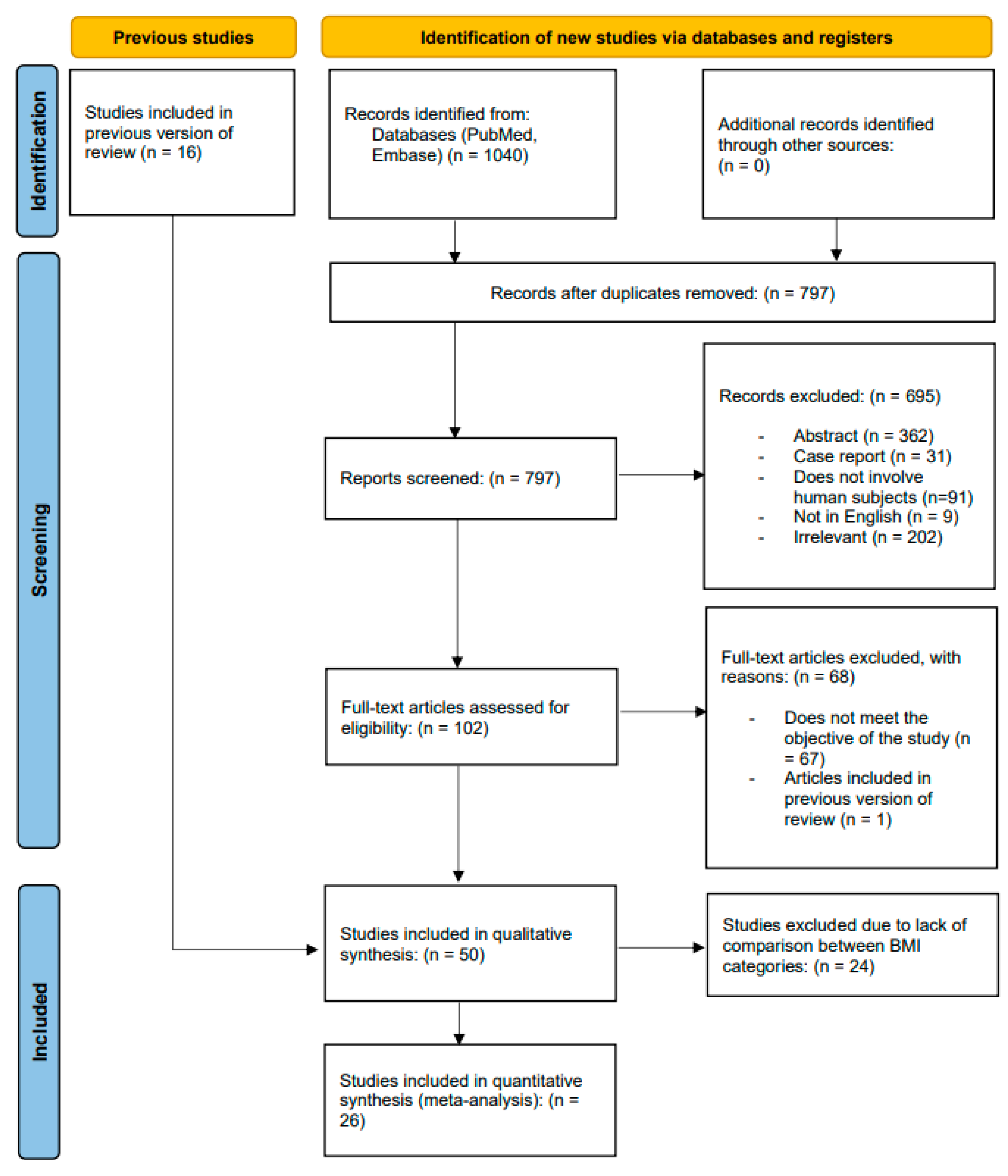
2.1. Database Search and Study Eligibility
2.2. Data Extraction and Outcomes
2.3. Quality of Evidence Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Selection and Characteristics
3.2. Study Quality Assessment
3.3. Primary outcomes
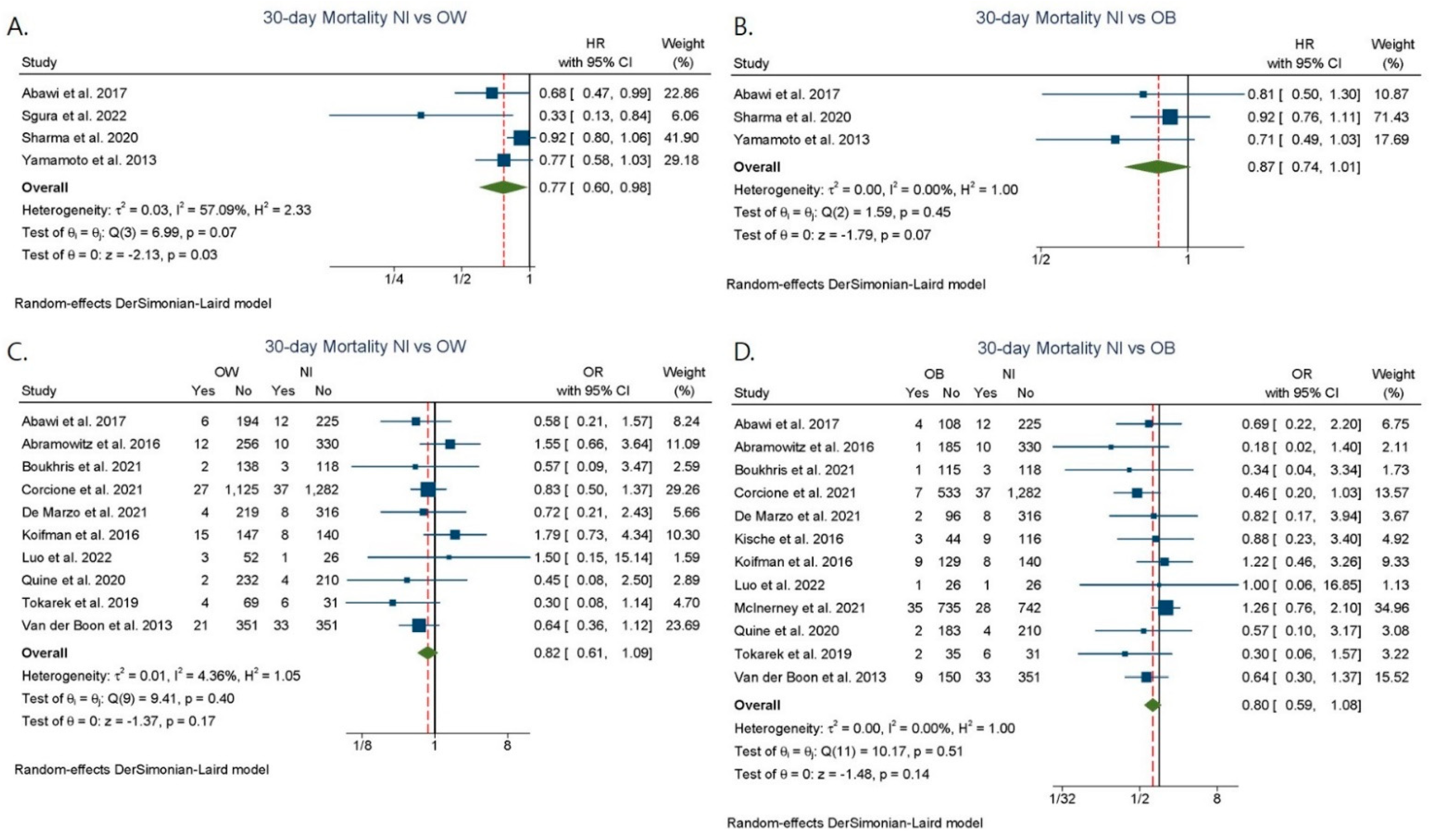
3.3.1. Short-Term Mortality
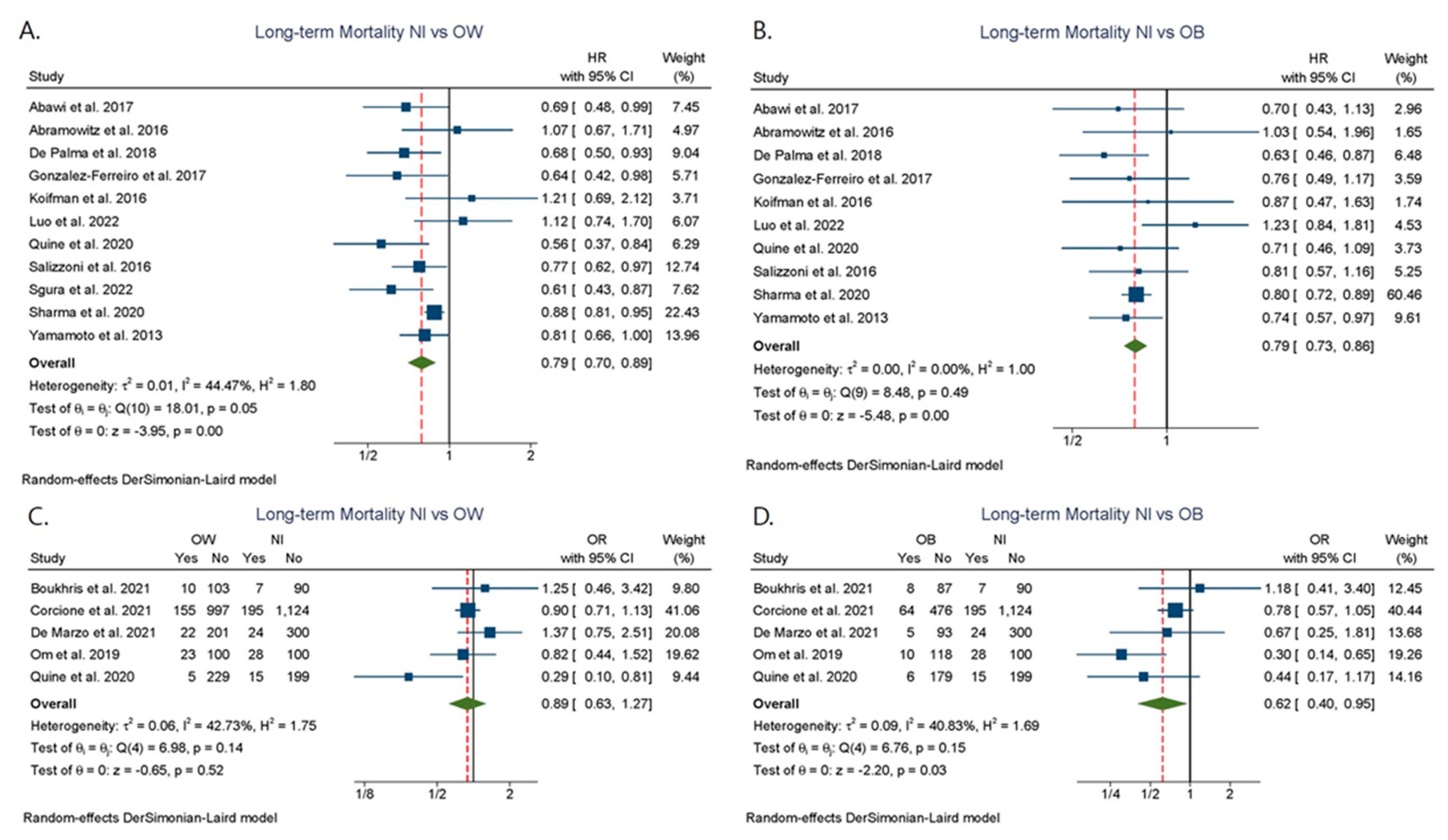
3.3.2. Mid-/Long-Term Mortality
3.4. Secondary Outcomes
3.5. Publication Bias and Meta-Regression
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 23 July 2022).
- Poirier, P.; Giles, T.D.; Bray, G.A.; Hong, Y.; Stern, J.S.; Pi-Sunyer, F.X.; Eckel, R.H. Obesity and cardiovascular disease: Pathophysiology, evaluation, and effect of weight loss: An update of the 1997 American Heart Association Scientific State-ment on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabo-lism. Circulation 2006, 113, 898–918. [Google Scholar] [CrossRef] [Green Version]
- Alperi, A.; McInerney, A.; Modine, T.; Chamandi, C.; Tafur-Soto, J.D.; Barbanti, M.; Lopez, D.; Campelo-Parada, F.; Cheema, A.N.; Toggweiler, S.; et al. Transcatheter aortic valve replacement in obese patients: Procedural vascular complications with the trans-femoral and trans-carotid access routes. Interact. CardioVascular Thorac. Surg. 2021, 34, 982–989. [Google Scholar] [CrossRef]
- Carroll, J.D.; Mack, M.J.; Vemulapalli, S.; Herrmann, H.C.; Gleason, T.G.; Hanzel, G.; Deeb, G.M.; Thourani, V.H.; Cohen, D.J.; Desai, N.; et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2020, 76, 2492–2516. [Google Scholar] [CrossRef]
- Lv, W.; Li, S.; Liao, Y.; Zhao, Z.; Che, G.; Chen, M.; Feng, Y. The ‘obesity paradox’ does exist in patients undergoing transcatheter aortic valve implantation for aortic stenosis: A systematic review and meta-analysis. Interact. Cardiovasc. Thorac. Surg. 2017, 25, 633–642. [Google Scholar] [CrossRef] [Green Version]
- Sannino, A.; Schiattarella, G.G.; Toscano, E.; Gargiulo, G.; Giugliano, G.; Galderisi, M.; Losi, M.A.; Stabile, E.; Cirillo, P.; Imbriaco, M.; et al. Meta-Analysis of Effect of Body Mass Index on Outcomes After Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2017, 119, 308–316. [Google Scholar] [CrossRef]
- Tokarek, T.A.; Dziewierz, A.; Sorysz, D.; Bagienski, M.; Rzeszutko, Ł.; Krawczyk-Ożóg, A.; Dudek, D.; Kleczyński, P. The obesity paradox in patients undergoing transcatheter aortic valve implantation: Is there any effect of body mass index on survival? Kardiol. Pol. 2019, 77, 190–197. [Google Scholar] [CrossRef] [Green Version]
- van Nieuwkerk, A.; Santos, R.B.; Sartori, S.; Regueiro, A.; Tchétché, D.; Mehran, R.; Delewi, R.; the CENTER collaboration. Impact of body mass index on outcomes in patients undergoing transfemoral transcatheter aortic valve implantation. JTCVS Open 2021, 6, 26–36. [Google Scholar] [CrossRef]
- Abramowitz, Y.; Chakravarty, T.; Jilaihawi, H.; Cox, J.; Sharma, R.P.; Mangat, G.; Nakamura, M.; Cheng, W.; Makkar, R.R. Impact of body mass index on the outcomes following transcatheter aortic valve implantation. Catheter. Cardiovasc. Interv. 2016, 88, 127–134. [Google Scholar] [CrossRef]
- McInerney, A.; Tirado-Conte, G.; Rodes-Cabau, J.; Campelo-Parada, F.; Tafur Soto, J.D.; Barbanti, M.; Munoz-Garcia, E.; Arif, M.; Lopez, D.; Toggweiler, S.; et al. Impact of Morbid Obesity and Obesity Phenotype on Outcomes After Transcatheter Aortic Valve Replacement. J. Am. Heart Assoc. 2021, 10, e019051. [Google Scholar] [CrossRef]
- Tzoumas, A.; Kokkinidis, D.G.; Giannopoulos, S.; Giannakoulas, G.; Palaiodimos, L.; Avgerinos, D.V.; Kampaktsis, P.N.; Faillace, R.T. Frailty in patients undergoing transcatheter aortic valve replacement: From risk scores to frailty-based management. J. Geriatr. Cardiol. 2021, 18, 479–486. [Google Scholar] [CrossRef]
- Boukhris, M.; Forcillo, J.; Potvin, J.; Noiseux, N.; Stevens, L.M.; Badreddine, M.; Gobeil, J.F.; Masson, J.B. Does “obesity paradox” apply for patients undergoing transcatheter aortic valve replacement? Arch. Cardiovasc. Dis. Suppl. 2022, 14, 69. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Kappetein, A.P.; Head, S.J.; Genereux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document (VARC-2). Eur. J. Cardiothorac. Surg. 2012, 42, S45–S60. [Google Scholar] [CrossRef]
- Zeng, X.; Zhang, Y.; Kwong, J.S.; Zhang, C.; Li, S.; Sun, F.; Niu, Y.; Du, L. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. J. Evid. Based Med. 2015, 8, 2–10. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2000. [Google Scholar]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Sutton, A.J.; Ioannidis, J.P.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rucker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [Green Version]
- Hunter, J.P.; Saratzis, A.; Sutton, A.J.; Boucher, R.H.; Sayers, R.D.; Bown, M.J. In meta-analyses of proportion studies, funnel plots were found to be an inaccurate method of assessing publication bias. J. Clin. Epidemiol. 2014, 67, 897–903. [Google Scholar] [CrossRef]
- Berti, S.; Bartorelli, A.L.; Koni, E.; Giordano, A.; Petronio, A.S.; Iadanza, A.; Bedogni, F.; Reimers, B.; Spaccarotella, C.; Trani, C.; et al. Impact of High Body Mass Index on Vascular and Bleeding Complications After Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2021, 155, 86–95. [Google Scholar] [CrossRef]
- Corcione, N.; Testa, A.; Ferraro, P.; Morello, A.; Cimmino, M.; Albanese, M.; Giordano, S.; Bedogni, F.; Iadanza, A.; Berti, S.; et al. Baseline, procedural and outcome features of patients undergoing transcatheter aortic valve implantation according to different body mass index categories. Minerva Med. 2021, 112, 474–482. [Google Scholar] [CrossRef]
- Abawi, M.; Rozemeijer, R.; Agostoni, P.; van Jaarsveld, R.C.; van Dongen, C.S.; Voskuil, M.; Kraaijeveld, A.O.; Doevendans, P.; Stella, P.R. Effect of body mass index on clinical outcome and all-cause mortality in patients undergoing transcatheter aortic valve implantation. Neth. Heart J. 2017, 25, 498–509. [Google Scholar] [CrossRef]
- Ahmad, M.; Patel, J.N.; Loc, B.L.; Vipparthy, S.C.; Divecha, C.; Barzallo, P.X.; Kim, M.; Baman, T.; Barzallo, M.; Mungee, S. Association Between Body Mass Index and Permanent Pacemaker Implantation After Transcatheter Aortic Valve Replacement (TAVR) with Edwards SAPIEN 3 TAVR Valves: A Single-Center Experience. Cureus 2019, 11, e5142. [Google Scholar] [CrossRef] [Green Version]
- De Marzo, V.; Crimi, G.; Benenati, S.; Buscaglia, A.; Pescetelli, F.; Vercellino, M.; Della Bona, R.; Sarocchi, M.; Canepa, M.; Ameri, P.; et al. BMI and acute kidney injury post transcatheter aortic valve replacement: Unveiling the obesity paradox. J. Cardiovasc. Med. 2021, 22, 579–585. [Google Scholar] [CrossRef]
- De Palma, R.; Ivarsson, J.; Feldt, K.; Saleh, N.; Ruck, A.; Linder, R.; Settergren, M. The obesity paradox: An analysis of pre-procedure weight trajectory on survival outcomes in patients undergoing transcatheter aortic valve implantation. Obes. Res. Clin. Pract. 2018, 12, 51–60. [Google Scholar] [CrossRef]
- Gonska, B.; Reuter, C.; Morike, J.; Rottbauer, W.; Buckert, D. Vascular Access Site Complications Do Not Correlate With Large Sheath Diameter in TAVI Procedures With New Generation Devices. Front. Cardiovasc. Med. 2021, 8, 738854. [Google Scholar] [CrossRef]
- Gonzalez-Ferreiro, R.; Munoz-Garcia, A.J.; Lopez-Otero, D.; Avanzas, P.; Pascual, I.; Alonso-Briales, J.H.; Trillo-Nouche, R.; Pun, F.; Jimenez-Navarro, M.F.; Hernandez-Garcia, J.M.; et al. Prognostic value of body mass index in transcatheter aortic valve implantation: A “J”-shaped curve. Int. J. Cardiol. 2017, 232, 342–347. [Google Scholar] [CrossRef]
- Kische, S.; D’Ancona, G.; Agma, H.U.; El-Achkar, G.; Dissmann, M.; Ortak, J.; Oner, A.; Ketterer, U.; Barisch, A.; Levenson, B.; et al. Transcatheter aortic valve implantation in obese patients: Overcoming technical challenges and maintaining adequate hemodynamic performance using new generation prostheses. Int. J. Cardiol. 2016, 220, 909–913. [Google Scholar] [CrossRef]
- Koifman, E.; Kiramijyan, S.; Negi, S.I.; Didier, R.; Escarcega, R.O.; Minha, S.; Gai, J.; Torguson, R.; Okubagzi, P.; Ben-Dor, I.; et al. Body mass index association with survival in severe aortic stenosis patients undergoing transcatheter aortic valve replacement. Catheter. Cardiovasc. Interv. 2016, 88, 118–124. [Google Scholar] [CrossRef]
- Konigstein, M.; Havakuk, O.; Arbel, Y.; Finkelstein, A.; Ben-Assa, E.; Leshem Rubinow, E.; Abramowitz, Y.; Keren, G.; Banai, S. The obesity paradox in patients undergoing transcatheter aortic valve implantation. Clin. Cardiol. 2015, 38, 76–81. [Google Scholar] [CrossRef]
- Iung, B.; Laouenan, C.; Himbert, D.; Eltchaninoff, H.; Chevreul, K.; Donzeau-Gouge, P.; Fajadet, J.; Leprince, P.; Leguerrier, A.; Lievre, M.; et al. Predictive factors of early mortality after transcatheter aortic valve implantation: Individual risk assessment using a simple score. Heart 2014, 100, 1016–1023. [Google Scholar] [CrossRef]
- Luo, Z.R.; Chen, L.W.; Qiu, H.F. Does the “obesity paradox” exist after transcatheter aortic valve implantation? J. Cardiothorac. Surg. 2022, 17, 156. [Google Scholar] [CrossRef]
- Om, S.Y.; Ko, E.; Ahn, J.M.; Kang, D.Y.; Lee, K.; Kwon, O.; Lee, P.H.; Lee, S.W.; Kim, H.J.; Kim, J.B.; et al. Relation of Body Mass Index to Risk of Death or Stroke in Patients Who Underwent Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2019, 123, 638–643. [Google Scholar] [CrossRef]
- Owais, T.; El Garhy, M.; Lauten, P.; Haensig, M.; Lapp, H.; Schulze, P.C.; Kuntze, T. Contemporary Results of Transcatheter Aortic Valve Replacement in Obese Patients. Cardiol. Res. Pract. 2020, 2020, 9732943. [Google Scholar] [CrossRef]
- Quine, E.J.; Dagan, M.; William, J.; Nanayakkara, S.; Dawson, L.P.; Duffy, S.J.; Stehli, J.; Dick, R.J.; Htun, N.M.; Stub, D.; et al. Long-Term Outcomes Stratified by Body Mass Index in Patients Undergoing Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2020, 137, 77–82. [Google Scholar] [CrossRef]
- Saji, M.; Kumamaru, H.; Kohsaka, S.; Higuchi, R.; Izumi, Y.; Takamisawa, I.; Tobaru, T.; Shimokawa, T.; Takanashi, S.; Shimizu, H.; et al. Non-cardiovascular readmissions after transcatheter aortic valve replacement: Insights from a Japanese nationwide registry of transcatheter valve therapies. J. Cardiol. 2022, 80, 197–203. [Google Scholar] [CrossRef]
- Salizzoni, S.; D’Onofrio, A.; Agrifoglio, M.; Colombo, A.; Chieffo, A.; Cioni, M.; Besola, L.; Regesta, T.; Rapetto, F.; Tarantini, G.; et al. Early and mid-term outcomes of 1904 patients undergoing transcatheter balloon-expandable valve implantation in Italy: Results from the Italian Transcatheter Balloon-Expandable Valve Implantation Registry (ITER). Eur. J. Cardiothorac. Surg. 2016, 50, 1139–1148. [Google Scholar] [CrossRef] [Green Version]
- Sgura, F.A.; Arrotti, S.; Monopoli, D.; Valenti, A.C.; Vitolo, M.; Magnavacchi, P.; Tondi, S.; Gabbieri, D.; Guiducci, V.; Benatti, G.; et al. Impact of body mass index on the outcome of elderly patients treated with transcatheter aortic valve implantation. Intern. Emerg. Med. 2022, 17, 369–376. [Google Scholar] [CrossRef]
- Sharma, A.; Lavie, C.J.; Elmariah, S.; Borer, J.S.; Sharma, S.K.; Vemulapalli, S.; Yerokun, B.A.; Li, Z.; Matsouaka, R.A.; Marmur, J.D. Relationship of Body Mass Index With Outcomes After Transcatheter Aortic Valve Replacement: Results From the National Cardiovascular Data-STS/ACC TVT Registry. Mayo Clin. Proc. 2020, 95, 57–68. [Google Scholar] [CrossRef] [Green Version]
- van der Boon, R.M.; Chieffo, A.; Dumonteil, N.; Tchetche, D.; Van Mieghem, N.M.; Buchanan, G.L.; Vahdat, O.; Marcheix, B.; Serruys, P.W.; Fajadet, J.; et al. Effect of body mass index on short- and long-term outcomes after transcatheter aortic valve implantation. Am. J. Cardiol. 2013, 111, 231–236. [Google Scholar] [CrossRef]
- Yamamoto, M.; Mouillet, G.; Oguri, A.; Gilard, M.; Laskar, M.; Eltchaninoff, H.; Fajadet, J.; Iung, B.; Donzeau-Gouge, P.; Leprince, P.; et al. Effect of body mass index on 30- and 365-day complication and survival rates of transcatheter aortic valve implantation (from the FRench Aortic National CoreValve and Edwards 2 [FRANCE 2] registry). Am. J. Cardiol. 2013, 112, 1932–1937. [Google Scholar] [CrossRef] [PubMed]
- Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ. Tech. Rep. Ser. 2000, 894, 1–253. [Google Scholar]
- Gilard, M.; Schluter, M.; Snow, T.M.; Dall’Ara, G.; Eltchaninoff, H.; Moat, N.; Goicolea, J.; Ussia, G.P.; Kala, P.; Wenaweser, P.; et al. The 2011–2012 pilot European Society of Cardiology Sentinel Registry of Transcatheter Aortic Valve Implantation: 12-month clinical outcomes. EuroIntervention 2016, 12, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Afilalo, J.; Lauck, S.; Kim, D.H.; Lefevre, T.; Piazza, N.; Lachapelle, K.; Martucci, G.; Lamy, A.; Labinaz, M.; Peterson, M.D.; et al. Frailty in Older Adults Undergoing Aortic Valve Replacement: The FRAILTY-AVR Study. J. Am. Coll. Cardiol. 2017, 70, 689–700. [Google Scholar] [CrossRef]
- Bendayan, M.; Messas, N.; Perrault, L.P.; Asgar, A.W.; Lauck, S.; Kim, D.H.; Arora, R.C.; Langlois, Y.; Piazza, N.; Martucci, G.; et al. Frailty and Bleeding in Older Adults Undergoing TAVR or SAVR: Insights From the FRAILTY-AVR Study. JACC Cardiovasc. Interv. 2020, 13, 1058–1068. [Google Scholar] [CrossRef] [PubMed]
- Kokkinidis, D.G.; Arfaras-Melainis, A.; Giannakoulas, G. Sarcopenia in heart failure: ‘waste’ the appropriate time and resources, not the muscles. Eur. J. Prev. Cardiol. 2021, 28, 1019–1021. [Google Scholar] [CrossRef]
- Rios, S.; Li, W.; Mustehsan, M.H.; Hajra, A.; Takahashi, T.; Chengyue, J.; Wu, L.; Katamreddy, A.; Ghalib, N.; Scotti, A.; et al. Impact of Frailty on Outcomes After Transcatheter Edge-to-Edge Repair With MitraClip (from the National Inpatient Sample Database). Am. J. Cardiol. 2022, 179, 58–63. [Google Scholar] [CrossRef]
- Varc-3 Writing, C.; Genereux, P.; Piazza, N.; Alu, M.C.; Nazif, T.; Hahn, R.T.; Pibarot, P.; Bax, J.J.; Leipsic, J.A.; Blanke, P.; et al. Valve Academic Research Consortium 3: Updated endpoint definitions for aortic valve clinical research. Eur. Heart J. 2021, 42, 1825–1857. [Google Scholar] [CrossRef]
- Head, S.J.; Mokhles, M.M.; Osnabrugge, R.L.; Pibarot, P.; Mack, M.J.; Takkenberg, J.J.; Bogers, A.J.; Kappetein, A.P. The impact of prosthesis-patient mismatch on long-term survival after aortic valve replacement: A systematic review and meta-analysis of 34 observational studies comprising 27 186 patients with 133 141 patient-years. Eur. Heart J. 2012, 33, 1518–1529. [Google Scholar] [CrossRef] [Green Version]
- Fadahunsi, O.O.; Olowoyeye, A.; Ukaigwe, A.; Li, Z.; Vora, A.N.; Vemulapalli, S.; Elgin, E.; Donato, A. Incidence, Predictors, and Outcomes of Permanent Pacemaker Implantation Following Transcatheter Aortic Valve Replacement: Analysis From the U.S. Society of Thoracic Surgeons/American College of Cardiology TVT Registry. JACC Cardiovasc. Interv. 2016, 9, 2189–2199. [Google Scholar] [CrossRef]
- Siontis, G.C.; Juni, P.; Pilgrim, T.; Stortecky, S.; Bullesfeld, L.; Meier, B.; Wenaweser, P.; Windecker, S. Predictors of permanent pacemaker implantation in patients with severe aortic stenosis undergoing TAVR: A meta-analysis. J. Am. Coll. Cardiol. 2014, 64, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Bax, J.J.; Delgado, V.; Bapat, V.; Baumgartner, H.; Collet, J.P.; Erbel, R.; Hamm, C.; Kappetein, A.P.; Leipsic, J.; Leon, M.B.; et al. Open issues in transcatheter aortic valve implantation. Part 2: Procedural issues and outcomes after transcatheter aortic valve implantation. Eur. Heart J. 2014, 35, 2639–2654. [Google Scholar] [CrossRef] [PubMed]
- Ledwoch, J.; Franke, J.; Gerckens, U.; Kuck, K.H.; Linke, A.; Nickenig, G.; Krulls-Munch, J.; Vohringer, M.; Hambrecht, R.; Erbel, R.; et al. Incidence and predictors of permanent pacemaker implantation following transcatheter aortic valve implantation: Analysis from the German transcatheter aortic valve interventions registry. Catheter. Cardiovasc. Interv. 2013, 82, E569–E577. [Google Scholar] [CrossRef] [PubMed]
- Mohamed-Ali, V.; Goodrick, S.; Bulmer, K.; Holly, J.M.; Yudkin, J.S.; Coppack, S.W. Production of soluble tumor necrosis factor receptors by human subcutaneous adipose tissue in vivo. Am. J. Physiol. 1999, 277, E971–E975. [Google Scholar] [CrossRef] [PubMed]
- Chrysant, S.G.; Chrysant, G.S. New insights into the true nature of the obesity paradox and the lower cardiovascular risk. J. Am. Soc. Hypertens. 2013, 7, 85–94. [Google Scholar] [CrossRef]
- Srikanthan, P.; Horwich, T.B.; Tseng, C.H. Relation of Muscle Mass and Fat Mass to Cardiovascular Disease Mortality. Am. J. Cardiol. 2016, 117, 1355–1360. [Google Scholar] [CrossRef]
- Mok, M.; Allende, R.; Leipsic, J.; Altisent, O.A.; Del Trigo, M.; Campelo-Parada, F.; DeLarochelliere, R.; Dumont, E.; Doyle, D.; Cote, M.; et al. Prognostic Value of Fat Mass and Skeletal Muscle Mass Determined by Computed Tomography in Patients Who Underwent Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2016, 117, 828–833. [Google Scholar] [CrossRef]
- Carbone, S.; Billingsley, H.E.; Rodriguez-Miguelez, P.; Kirkman, D.L.; Garten, R.; Franco, R.L.; Lee, D.C.; Lavie, C.J. Lean Mass Abnormalities in Heart Failure: The Role of Sarcopenia, Sarcopenic Obesity, and Cachexia. Curr. Probl. Cardiol. 2020, 45, 100417. [Google Scholar] [CrossRef]
- Ortega, F.B.; Sui, X.; Lavie, C.J.; Blair, S.N. Body Mass Index, the Most Widely Used But Also Widely Criticized Index: Would a Criterion Standard Measure of Total Body Fat Be a Better Predictor of Cardiovascular Disease Mortality? Mayo Clin. Proc. 2016, 91, 443–455. [Google Scholar] [CrossRef] [Green Version]
- Arsalan, M.; Filardo, G.; Kim, W.K.; Squiers, J.J.; Pollock, B.; Liebetrau, C.; Blumenstein, J.; Kempfert, J.; Van Linden, A.; Arsalan-Werner, A.; et al. Prognostic value of body mass index and body surface area on clinical outcomes after transcatheter aortic valve implantation. Clin. Res. Cardiol. 2016, 105, 1042–1048. [Google Scholar] [CrossRef]
- Kandathil, A.; Mills, R.A.; Hanna, M.; Merchant, A.M.; Wehrmann, L.E.; Minhajuddin, A.; Abbara, S.; Fox, A.A. Abdominal adiposity assessed using CT angiography associates with acute kidney injury after trans-catheter aortic valve replacement. Clin. Radiol. 2020, 75, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Kokkinidis, D.G.; Armstrong, E.J.; Giri, J. Balancing Weight Loss and Sarcopenia in Elderly Patients With Peripheral Artery Disease. J. Am. Heart Assoc. 2019, 8, e013200. [Google Scholar] [CrossRef] [PubMed]
- Green, P.; Arnold, S.V.; Cohen, D.J.; Kirtane, A.J.; Kodali, S.K.; Brown, D.L.; Rihal, C.S.; Xu, K.; Lei, Y.; Hawkey, M.C.; et al. Relation of frailty to outcomes after transcatheter aortic valve replacement (from the PARTNER trial). Am. J. Cardiol. 2015, 116, 264–269. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country | Study Characteristic | Study Population (n) | Follow-Up Duration (months) | BMI Classification (kg/m2) | Vascular Access |
|---|---|---|---|---|---|---|---|
| Abawi et al. [24] | 2017 | Netherlands | retrospective single center | 562 | 12 | WHO definition | Tf, Ta, Tao |
| Abramowitz et al. [9] | 2016 | USA | retrospective single center | 805 | 33 | WHO definition | Tf, Ta, Tao, S |
| Ahmad et al. [25] | 2019 | USA | retrospective single center | 269 | N/A | Underweight < 25 Normal 25 –≤ 30 Overweight 30 –≤ 35 Obesity ≥ 35 | N/A |
| Berti et al. [22] | 2021 | Italy | retrospective single center | 3776 | N/A | WHO definition | N/A |
| Boukhris et al. [12] | 2021 | Canada | retrospective single center | 412 | 12 | Underweight < 20 Normal 20 –< 25 Overweight 25 –< 30 Obesity ≥ 30 | Tf |
| Corcione et al. [23] | 2021 | Italy | retrospective single center | 3075 | (mean): 9.8–11.8 | WHO definition | N/A |
| DeMarzo et al. [26] | 2021 | Italy | retrospective single center | 645 | 12 | Low to normal < 25 Overweight 25 –< 30 Obesity ≥ 30 | Tf, Ta, S |
| DePalma et al. [27] | 2018 | Sweden | retrospective single center | 493 | 36 | Underweight < 18 Normal 18—25 Overweight 25.1–30 Obesity > 30 Severe obesity > 35 | Tf, S, Ta, O |
| Gonska et al. [28] | 2021 | Germany | retrospective single center | 611 | N/A | BMI ≥ 25 | Tf |
| Gonzalez-Ferreiro et al. [29] | 2017 | Spain | retrospective multi-center | 770 | 36 | WHO definition | Tf, Tax |
| Kische et al. [30] | 2016 | Germany | retrospective | 172 | 12 | Non-obesity BMI < 30 Obesity BMI ≥ 30 | Tf |
| Koifman et al. [31] | 2016 | USA | retrospective single center | 448 | 12 | Low <20 Normal 20–24.9 Overweight 25–30 Obesity > 30 | Tf |
| Konigstein et al. [32] | 2015 | Israel | retrospective single center | 409 | 2 | WHO definition | Tf |
| Lung et al. [33] | 2014 | France | retrospective multi-center | 2552 | 1 | Low < 18.5 Normal 18.5–29.9 Overweight BMI ≥ 30 | Tf, Ta, S, O |
| Luo et al. [34] | 2022 | China | retrospective single center | 109 | 35 | Low < 21.9 Middle 21.9–27.0 High > 27.0 | Tf, Ta |
| McInerney et al. [10] | 2021 | Europe, USA | retrospective multi-center | 3174 | 24 | Non-obesity 18.5–29.9 Morbidly obesity ≥40 or ≥35 with obesity-related comorbidities | Tf, non-Tf |
| Om et al. [35] | 2019 | Korea | retrospective multi-center | 379 | (median): 18.4 (IQR 7.3 to 37.2) | First tertile ≤ 22.3 Second tertile 22.4–24.8 Third tertile ≥ 24.9 | Tf, Ta, Tao |
| Owais et al. [36] | 2020 | Germany | retrospective single center | 1609 | 12 | WHO definition | Tf |
| Quine et al. [37] | 2020 | Australia | retrospective multi-center | 634 | (median): 24 | WHO definition | Tf, S, Ta, O |
| Saji et al. [38] | 2022 | Japan | retrospective multi-center | 14472 | 12 | Underweight < 20 Normal 20–25 Overweight 25–30 Obesity ≥ 30 | Tf, non-Tf |
| Salizzoni et al. [39] | 2016 | Italy | retrospective multi-center | 1904 | (median): 25.7 (IQR 15.6 to 37.5) | WHO definition | Tf, Ta, Tao, Tax |
| Sgura et al. [40] | 2022 | Italy | retrospective multi-center | 794 | (median): 26.4 | underweight < 20 Normal 20–24.9 Overweight/Obesity ≥ 25 | Tf, Ta |
| Sharma et al. [41] | 2020 | USA | retrospective multi-center | 31929 | 12 | WHO definition | Tf, Ta, Tao, S, O |
| Tokarek et al. [7] | 2019 | Poland | retrospective single center | 148 | (median): 15.3 (IQR 6 to 34.7) | WHO definition | Tf, Ta, Tao, S |
| Van der Boon et al. [42] | 2013 | Europe | retrospective multi-center | 940 | (median): 12 (IQR 6 to 18) | WHO definition | Tf, Ta, S, O |
| Yamamoto et al. [43] | 2013 | France | retrospective multi-center | 3072 | (median): 4.1 (IQR 1 to 8.3) | WHO definition | Tf, Ta, S, O |
| Normal | Overweight | Obesity | |
|---|---|---|---|
| Age (years) | 71.0 ± 24.3 | 65.9 ± 37.8 | 67.6 ± 19.1 |
| Male n (%) | 9198/19,032 (48.3) | 10,187/18,919 (53.8) | 4425/9571 (46.2) |
| BMI (kg/m2) | 22.8 ± 2.6 | 27.6 ± 3.3 | 34.5 ± 5.9 |
| AF n (%) | 1191/3536 (33.7) | 869/2947 (29.5) | 776/2390 (32.5) |
| CAD n (%) | 10,256/17,154 (59.8) | 10,562/17,171 (61.5) | 5433/8627 (63) |
| CKD n (%) | 623/2847 (21.9) | 898/3595 (25) | 93/688 (13.5) |
| COPD n (%) | 1306/6286 (20.8) | 1140/5377 (21.2) | 1021/3601 (28.4) |
| DM n (%) | 2058/8277 (24.9) | 2471/8228 (30) | 1770/3989 (44.4) |
| Dyslipidemia n (%) | 2780/5133 (54.2) | 3283/5523 (59.4) | 1668/2486 (67.1) |
| HTN n (%) | 14,450/17,389 (83.1) | 15,229/17,544 (86.8) | 7994/8933 (89.5) |
| GFR (mL/min/m2) | 57.1 ± 71.8 | 57.1 ± 71.0 | 53.1 ± 58.1 |
| logistic EuroSCORE | 18.0 ± 12.6 | 17.7 ± 11.9 | 14.5 ± 10.7 |
| STS score | 6.1 ± 3.7 | 5.3 ± 3.5 | 4.8 ± 2.6 |
| Outcomes | Studies | Patients | HR/OR | 95% CI, p-Value | I2 (%) | Egger Test | |
|---|---|---|---|---|---|---|---|
| Primary | |||||||
| 30-day Mortality | 4 | 25,050 | 0.77 (HR) | [0.60, 0.98], p = 0.03 | 57.09 | 0.0082 | |
| 10 | 6030 | 0.82 (OR) | [0.61, 1.09], p = 0.17 | 4.36 | 0.6904 | ||
| Mid-/long-term Mortality | 11 | 28,917 | 0.79 (HR) | [0.70, 0.89], p = 0.00 | 44.47 | 0.8864 | |
| 5 | 3978 | 0.89 (OR) | [0.63, 1.27], p = 0.52 | 42.73 | 0.5304 | ||
| Secondary | |||||||
| Major Bleeding | 14 | 11,724 | 1.08 (OR) | [0.92, 1.27], p = 0.33 | 8.92 | 0.5321 | |
| Major Vascular Complications | 14 | 11,875 | 1.09 (OR) | [0.92, 1.29], p = 0.31 | 0 | 0.8544 | |
| Cerebrovascular events | 13 | 9940 | 1.11 (OR) | [0.86, 1.42], p = 0.43 | 0 | 0.3950 | |
| Myocardial Infarction | 8 | 7427 | 0.69 (OR) | [0.36, 1.34], p = 0.27 | 23.37 | 0.8140 | |
| Atrial Fibrillation | 5 | 2362 | 0.78 (OR) | [0.58, 1.04], p = 0.09 | 0 | 0.7519 | |
| Pacemaker Insertion | 15 | 10,071 | 1.16 (OR) | [1.03, 1.30], p = 0.01 | 0 | 0.9191 | |
| Acute Kidney Injury | 12 | 7338 | 1.04 (OR) | [0.82, 1.32], p = 0.73 | 23.73 | 0.9639 | |
| Outcomes | Studies | Patients | HR/OR | 95% CI, p-Value | I2 (%) | Egger Test | |
|---|---|---|---|---|---|---|---|
| Primary | |||||||
| 30-day Mortality | 3 | 18,613 | 0.87 (HR) | [0.74, 1.01], p = 0.07 | 0 | 0.2995 | |
| 12 | 6461 | 0.8 (OR) | [0.59, 1.08], p = 0.14 | 0 | 0.0711 | ||
| Mid-/long-term Mortality | 10 | 21,262 | 0.79 (HR) | [0.73, 0.86], p = 0.00 | 0 | 0.7745 | |
| 5 | 3173 | 0.62 (OR) | [0.40, 0.95], p = 0.03 | 40.83 | 0.8486 | ||
| Secondary | |||||||
| Major Bleeding | 16 | 10,042 | 1.1 (OR) | [0.86, 1.41], p = 0.46 | 54.36 | 0.3594 | |
| Major Vascular Complications | 15 | 10,033 | 1.33 (OR) | [1.05, 1.68], p = 0.02 | 40.85 | 0.4458 | |
| Cerebrovascular events | 14 | 9383 | 1.01 (OR) | [0.76, 1.35], p = 0.94 | 0 | 0.4143 | |
| Myocardial Infarction | 8 | 5804 | 0.72 (OR) | [0.39, 1.34], p = 0.3 | 0 | 0.7074 | |
| Atrial Fibrillation | 5 | 1876 | 0.68 (OR) | [0.40, 1.17], p = 0.16 | 46.85 | 0.0648 | |
| Pacemaker Insertion | 17 | 9878 | 1.26 (OR) | [1.06, 1.50], p = 0.01 | 37.33 | 0.5568 | |
| Acute Kidney Injury | 14 | 7485 | 1.09 (OR) | [0.93, 1.29], p = 0.28 | 0 | 0.2912 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, J.; Li, W.; Safiriyu, I.; Kharawala, A.; Nagraj, S.; Tahir, A.; Doundoulakis, I.; Koliastasis, L.; Rios, S.; Palaiodimos, L.; et al. A Meta-Analysis on the Impact of High BMI in Patients Undergoing Transcatheter Aortic Valve Replacement. J. Cardiovasc. Dev. Dis. 2022, 9, 386. https://doi.org/10.3390/jcdd9110386
Seo J, Li W, Safiriyu I, Kharawala A, Nagraj S, Tahir A, Doundoulakis I, Koliastasis L, Rios S, Palaiodimos L, et al. A Meta-Analysis on the Impact of High BMI in Patients Undergoing Transcatheter Aortic Valve Replacement. Journal of Cardiovascular Development and Disease. 2022; 9(11):386. https://doi.org/10.3390/jcdd9110386
Chicago/Turabian StyleSeo, Jiyoung, Weijia Li, Israel Safiriyu, Amrin Kharawala, Sanjana Nagraj, Arooj Tahir, Ioannis Doundoulakis, Leonidas Koliastasis, Saul Rios, Leonidas Palaiodimos, and et al. 2022. "A Meta-Analysis on the Impact of High BMI in Patients Undergoing Transcatheter Aortic Valve Replacement" Journal of Cardiovascular Development and Disease 9, no. 11: 386. https://doi.org/10.3390/jcdd9110386