
The Predictive Value of Different Nutritional Indices Combined with the GRACE Score in Predicting the Risk of Long-Term Death in Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Calculation of Nutritional Indices and GRACE Scores
2.4. Follow-Up for All-Cause Death
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
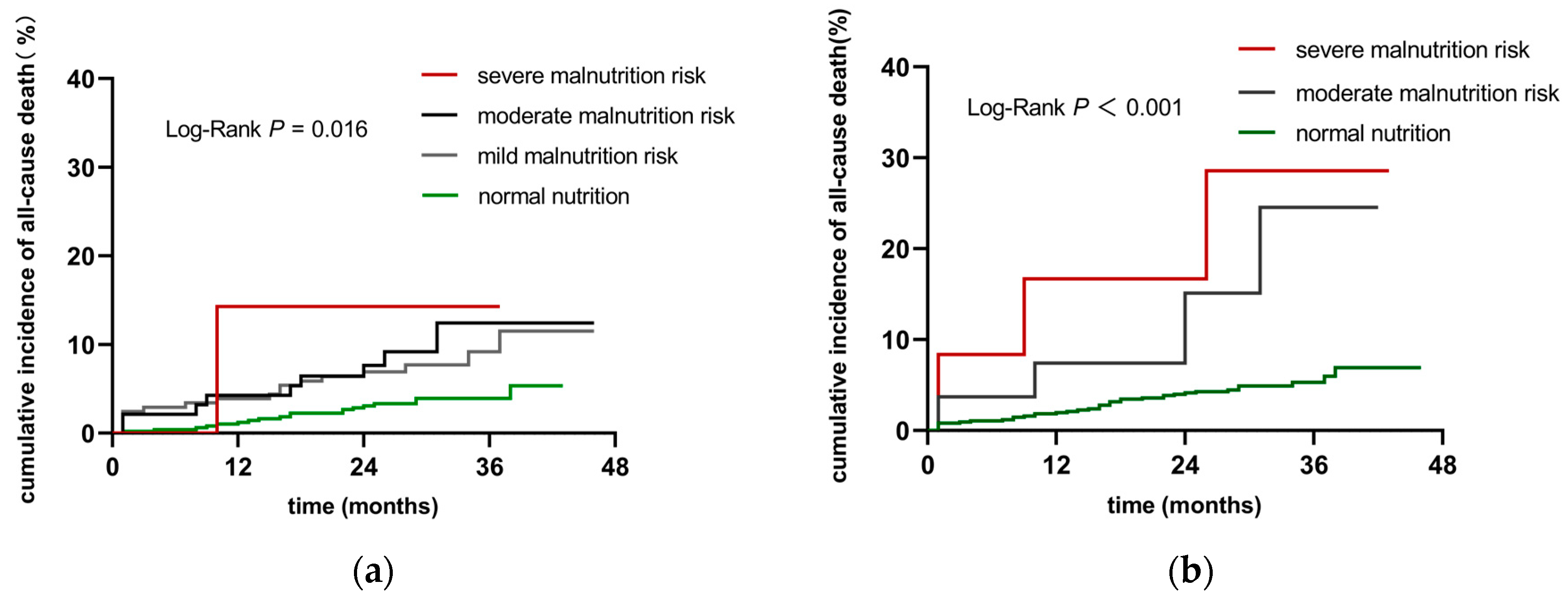
3.2. Cumulative Incidence of All-Cause Death in Patients in Different Nutritional Risk Groups
3.3. The Relationship between Different Nutritional Indices and All-Cause Mortality
3.4. Additional Predictive Values of the Nutritional Indices in the GRACE Risk Prediction Model
4. Discussion
4.1. Predictive Value of Serum Albumin for All-Cause Death
4.2. Predictive Value of Weight Loss for All-Cause Death
4.3. Predictive Value of Total Lymphocyte Counts for All-Cause Death
4.4. Predictive Value of the PNI Combined with the GRACE Score for All-Cause Death
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2021 Update: A Report from the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef] [PubMed]
- Global Use of Strategies to Open Occluded Coronary Arteries in Acute Coronary Syndromes (GUSTO IIb) Angioplasty Substudy Investigators. A clinical trial comparing primary coronary angioplasty with tissue plasminogen activator for acute myocardial infarction. N. Engl. J. Med. 1997, 336, 1621–1628. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, U.; Brejt, J.A.; Schulman-Marcus, J.; Swaminathan, R.V.; Feldman, D.N.; Goyal, P.; Wong, S.C.; Minutello, R.M.; Bergman, G.; Singh, H.; et al. Temporal Trends in the Clinical Acuity of Patients with ST-Segment Elevation Myocardial Infarction. Am. J. Med. 2018, 131, 100.e9–100.e20. [Google Scholar] [CrossRef] [PubMed]
- Eagle, K.A.; Lim, M.J.; Dabbous, O.H.; Pieper, K.S.; Goldberg, R.J.; Van de Werf, F.; Goodman, S.G.; Granger, C.B.; Steg, P.G.; Gore, J.M.; et al. A validated prediction model for all forms of acute coronary syndrome: Estimating the risk of 6-month postdischarge death in an international registry. JAMA 2004, 291, 2727–2733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradshaw, P.J.; Ko, D.T.; Newman, A.M.; Donovan, L.R.; Tu, J.V. Validity of the GRACE (Global Registry of Acute Coronary Events) acute coronary syndrome prediction model for six month post-discharge death in an independent data set. Heart 2006, 92, 905–909. [Google Scholar] [CrossRef]
- Tang, E.W.; Wong, C.K.; Herbison, P. Global Registry of Acute Coronary Events (GRACE) hospital discharge risk score accurately predicts long-term mortality post acute coronary syndrome. Am. Heart J. 2007, 153, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2020, 42, 1289–1367. [Google Scholar] [CrossRef]
- Raposeiras Roubín, S.; Abu Assi, E.; Cespón Fernandez, M.; Barreiro Pardal, C.; Lizancos Castro, A.; Parada, J.A.; Pérez, D.D.; Blanco Prieto, S.; Rossello, X.; Ibanez, B.; et al. Prevalence and Prognostic Significance of Malnutrition in Patients with Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2020, 76, 828–840. [Google Scholar] [CrossRef]
- Ando, T.; Yoshihisa, A.; Kimishima, Y.; Kiko, T.; Shimizu, T.; Yamaki, T.; Kunii, H.; Nakazato, K.; Takeishi, Y. Prognostic impacts of nutritional status on long-term outcome in patients with acute myocardial infarction. Eur. J. Prev. Cardiol. 2020, 27, 2229–2231. [Google Scholar] [CrossRef] [PubMed]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Wada, H.; Dohi, T.; Miyauchi, K.; Doi, S.; Naito, R.; Konishi, H.; Tsuboi, S.; Ogita, M.; Kasai, T.; Hassan, A.; et al. Prognostic Impact of the Geriatric Nutritional Risk Index on Long-Term Outcomes in Patients Who Underwent Percutaneous Coronary Intervention. Am. J. Cardiol. 2017, 119, 1740–1745. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Zhang, T.Y.; Cheng, Y.J.; Ma, Y.; Xu, Y.K.; Yang, J.Q.; Zhou, Y.J. Impacts of geriatric nutritional risk index on prognosis of patients with non-ST-segment elevation acute coronary syndrome: Results from an observational cohort study in China. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1685–1696. [Google Scholar] [CrossRef]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar]
- Keskin, M.; Hayıroğlu, M.I.; Keskin, T.; Kaya, A.; Tatlısu, M.A.; Altay, S.; Uzun, A.O.; Börklü, E.B.; Güvenç, T.S.; Avcı, I.I.; et al. A novel and useful predictive indicator of prognosis in ST-segment elevation myocardial infarction, the prognostic nutritional index. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Lee, H.W.; Lee, H.C.; Kim, H.J.; Seong, E.Y.; Song, S.H. Impact of nutritional index on contrast-associated acute kidney injury and mortality after percutaneous coronary intervention. Sci. Rep. 2021, 11, 7123. [Google Scholar] [CrossRef] [PubMed]
- Chinese Society of Cardiology. CSC guidelines for thediagnosis and treatment of acute myocardial infarction in patients presenting with ST-segment elevation. Chin. J. Cardiol. 2015, 43, 380–393. [Google Scholar]
- Chinese Society of Cardiology. CSC guidelines for the diagnosis and treatment of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Chin. J. Cardiol. 2017, 45, 359–376. [Google Scholar]
- Sze, S.; Pellicori, P.; Kazmi, S.; Rigby, A.; Cleland, J.G.F.; Wong, K.; Clark, A.L. Prevalence and Prognostic Significance of Malnutrition Using 3 Scoring Systems Among Outpatients with Heart Failure: A Comparison With Body Mass Index. JACC Heart Fail. 2018, 6, 476–486. [Google Scholar] [CrossRef] [PubMed]
- Doi, S.; Iwata, H.; Wada, H.; Funamizu, T.; Shitara, J.; Endo, H.; Naito, R.; Konishi, H.; Tsuboi, S.; Ogita, M.; et al. A novel and simply calculated nutritional index serves as a useful prognostic indicator in patients with coronary artery disease. Int. J. Cardiol. 2018, 262, 92–98. [Google Scholar] [CrossRef]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Kolodgie, F.D.; Virmani, R.; Burke, A.P.; Farb, A.; Weber, D.K.; Kutys, R.; Finn, A.V.; Gold, H.K. Pathologic assessment of the vulnerable human coronary plaque. Heart 2004, 90, 1385–1391. [Google Scholar] [CrossRef] [Green Version]
- Navar, A.M. The Evolving Story of Triglycerides and Coronary Heart Disease Risk. JAMA 2019, 321, 347–349. [Google Scholar] [CrossRef] [PubMed]
- Don, B.R.; Kaysen, G. Serum albumin: Relationship to inflammation and nutrition. Semin. Dial. 2004, 17, 432–437. [Google Scholar] [CrossRef]
- Wada, H.; Dohi, T.; Miyauchi, K.; Shitara, J.; Endo, H.; Doi, S.; Naito, R.; Konishi, H.; Tsuboi, S.; Ogita, M.; et al. Impact of serum albumin levels on long-term outcomes in patients undergoing percutaneous coronary intervention. Heart Vessel. 2017, 32, 1085–1092. [Google Scholar] [CrossRef]
- Djoussé, L.; Rothman, K.J.; Cupples, L.A.; Levy, D.; Ellison, R.C. Serum albumin and risk of myocardial infarction and all-cause mortality in the Framingham Offspring Study. Circulation 2002, 106, 2919–2924. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; He, Y.M.; Cai, D.P.; Yang, X.J.; Xu, H.F. Risk burdens of modifiable risk factors incorporating lipoprotein (a) and low serum albumin concentrations for first incident acute myocardial infarction. Sci. Rep. 2016, 6, 35463. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.; Chen, M.; Lin, X. Serum albumin level for prediction of all-cause mortality in acute coronary syndrome patients: A meta-analysis. Biosci. Rep. 2020, 40, BSR20190881. [Google Scholar] [CrossRef] [Green Version]
- Arques, S. Human serum albumin in cardiovascular diseases. Eur. J. Intern. Med. 2018, 52, 8–12. [Google Scholar] [CrossRef]
- Merker, M.; Felder, M.; Gueissaz, L.; Bolliger, R.; Tribolet, P.; Kägi-Braun, N.; Gomes, F.; Hoess, C.; Pavlicek, V.; Bilz, S.; et al. Association of baseline inflammation with effectiveness of nutritional support among patients with disease-related malnutrition: A secondary analysis of a randomized clinical trial. JAMA Netw. Open 2020, 3, e200663. [Google Scholar] [CrossRef] [PubMed]
- Polat, N.; Oylumlu, M.; Işik, M.A.; Arslan, B.; Özbek, M.; Demir, M.; Kaya, H.; Toprak, N. Prognostic Significance of Serum Albumin in Patients with Acute Coronary Syndrome. Angiology 2020, 71, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.J.; Zhou, Y.J.; Galper, B.Z.; Gao, F.; Yeh, R.W.; Mauri, L. Association of body mass index with mortality and cardiovascular events for patients with coronary artery disease: A systematic review and meta-analysis. Heart 2015, 101, 1631–1638. [Google Scholar] [CrossRef] [PubMed]
- Abou Ghayda, R.; Duck-Young Park, D.; Lee, J.Y.; Kim, J.Y.; Lee, K.H.; Hong, S.H.; Yang, J.W.; Kim, J.S.; Jeong, G.H.; Kronbichler, A.; et al. Body mass index and mortality in patients with cardiovascular disease: An umbrella review of meta-analyses. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 273–286. [Google Scholar]
- Madjid, M.; Awan, I.; Willerson, J.T.; Casscells, S.W. Leukocyte count and coronary heart disease: Implications for risk assessment. J. Am. Coll. Cardiol. 2004, 44, 1945–1956. [Google Scholar] [CrossRef] [Green Version]
- Grönberg, C.; Nilsson, J.; Wigren, M. Recent advances on CD4+ T cells in atherosclerosis and its implications for therapy. Eur. J. Pharmacol. 2017, 816, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, S.; Zernecke, A. CD8+ T Cells in Atherosclerosis. Cells 2020, 10, 37. [Google Scholar] [CrossRef]
- Upadhye, A.; Sturek, J.M.; McNamara, C.A. 2019 Russell Ross Memorial Lecture in Vascular Biology: B Lymphocyte-Mediated Protective Immunity in Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 309–322. [Google Scholar] [CrossRef]
- Shumilah, A.M.; Othman, A.M.; Al-Madhagi, A.K. Accuracy of neutrophil to lymphocyte and monocyte to lymphocyte ratios as new inflammatory markers in acute coronary syndrome. BMC Cardiovasc. Disord. 2021, 21, 422. [Google Scholar] [CrossRef]
- Ji, H.; Li, Y.; Fan, Z.; Zuo, B.; Jian, X.; Li, L.; Liu, T. Monocyte/lymphocyte ratio predicts the severity of coronary artery disease: A syntax score assessment. BMC Cardiovasc. Disord. 2017, 17, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Wang, J.; Cao, D.; Han, L. Correlation of neutrophil-to-lymphocyte ratio with the prognosis of non-ST-segment elevation in patients with acute coronary syndrome undergoing selective percutaneous coronary intervention. J. Int. Med. Res. 2020, 48, 300060520959510. [Google Scholar] [CrossRef]
- Zhao, W.M.; Tao, S.M.; Liu, G.L. Neutrophil-to-lymphocyte ratio in relation to the risk of all-cause mortality and cardiovascular events in patients with chronic kidney disease: A systematic review and meta-analysis. Ren. Fail. 2020, 42, 1059–1066. [Google Scholar] [CrossRef]
- Song, F.H.; Zheng, Y.Y.; Tang, J.N.; Wang, W.; Guo, Q.Q.; Zhang, J.C.; Bai, Y.; Wang, K.; Cheng, M.D.; Jiang, L.Z.; et al. A Correlation Between Monocyte to Lymphocyte Ratio and Long-Term Prognosis in Patients with Coronary Artery Disease After PCI. Clin. Appl. Thromb. Hemost. 2021, 27, 1076029621999717. [Google Scholar] [CrossRef]
- Kim, C.; Sung, J.; Lee, J.H.; Kim, W.S.; Lee, G.J.; Jee, S.; Jung, I.Y.; Rah, U.W.; Kim, B.O.; Choi, K.H.; et al. Clinical Practice Guideline for Cardiac Rehabilitation in Korea: Recommendations for Cardiac Rehabilitation and Secondary Prevention after Acute Coronary Syndrome. Korean Circ. J. 2019, 49, 1066–1111. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | All Subjects (n = 799) | All-Cause Death (n = 46) | Survival (n = 753) | p Value |
|---|---|---|---|---|
| Male, n (%) | 578 (72.3) | 30 (65.2) | 548 (72.8) | 0.266 |
| PNI | 47.53 ± 5.79 | 43.86 ± 5.35 | 47.76 ± 5.74 | <0.001 |
| GNRI | 100.22 (95.01, 103.94) | 96.94 (92.33, 101.71) | 100.37 (95.23, 104.09) | 0.002 |
| Serum albumin, g/L | 39.60 (36.60, 42.10) | 38.10 (34.60, 40.30) | 39.60 (36.80, 42.20) | 0.001 |
| Total lymphocyte count, ×109/L | 1.55 (1.17, 1.98) | 1.23 (0.89, 1.70) | 1.56 (1.19, 2.00) | 0.001 |
| Weight loss, n (%) | 176 (22.0) | 9 (19.6) | 167 (22.2) | 0.678 |
| BMI, kg/m2 | 24.24 (22.58, 26.67) | 24.44 (23.10, 26.49) | 24.24 (22.54, 26.67) | 0.875 |
| GRACE score | 106 (85, 131) | 134 (114, 153) | 104 (85, 129) | <0.001 |
| Age, years | 66.26 ± 11.34 | 73.41 ± 10.50 | 65.82 ± 11.25 | <0.001 |
| HR, bpm | 76.00 (67.00, 85.00) | 75.50 (67.00, 88.50) | 76.00 (67.00, 85.00) | 0.752 |
| SBP, mmHg | 130.00 (119.00, 144.00) | 132.00 (114.75, 149.25) | 130.00 (119.50, 144.00) | 0.998 |
| Scr, umol/L | 75.90 (64.10, 89.80) | 77.60 (60.53, 110.48) | 75.70 (64.30, 88.90) | 0.301 |
| Congestive heart failure, n (%) | 274 (34.3) | 27 (58.7) | 247 (32.8) | <0.001 |
| History of MI, n (%) | 49 (6.1) | 5 (10.9) | 44 (5.8) | 0194 |
| ST-Segment Depression, n (%) | 374 (46.8) | 25 (54.3) | 349 (46.3) | 0.291 |
| Elevated Cardiac Enzymes, n (%) | 533 (66.7) | 38 (82.6) | 495 (65.7) | 0.018 |
| Smoking, n (%) | 317 (39.7) | 10 (21.7) | 307 (40.8) | 0.010 |
| Previous CAD, n (%) | 180 (22.6) | 16 (34.8) | 164 (21.8) | 0.041 |
| Previous PCI, n (%) | 63 (7.9) | 4 (8.7) | 59 (7.8) | 0.778 |
| Atrial fibrillation, n (%) | 51 (6.4) | 10 (21.7) | 41 (5.4) | <0.001 |
| Hypertension, n (%) | 505 (63.2) | 33 (71.7) | 472 (62.7) | 0.216 |
| Diabetes, n (%) | 270 (33.8) | 22 (47.8) | 248 (32.9) | 0.038 |
| Previous Stroke, n (%) | 24 (3.0) | 1 (2.2) | 23 (3.1) | 1.000 |
| Renal dysfunction, n (%) | 50 (6.3) | 6 (13.0) | 44 (5.8) | 0.060 |
| Hs-TnT, pg/mL | 42.05 (11.55, 916.10) | 137.10 (27.72, 1780.50) | 38.71 (11.28, 859.50) | 0.025 |
| Uric acid, μmol/L | 366.50 (308.10, 439.10) | 400.25 (324.65, 478.95) | 365.35 (307.43, 435.78) | 0.053 |
| TG, mmol/L | 1.45 (1.06, 2.19) | 1.22 (0.97, 1.66) | 1.47 (1.07, 2.24) | 0.017 |
| TC, mmol/L | 4.34 (3.62, 5.20) | 4.33 (3.49, 5.08) | 4.34 (3.63, 5.21) | 0.853 |
| LDL-C, mmol/L | 2.66 (2.15, 3.31) | 2.68 (2.07, 3.38) | 2.66 (2.16, 3.31) | 0.843 |
| HDL-C, mmol/L | 1.10 (0.95, 1.30) | 1.13 (0.97, 1.37) | 1.10 (0.95, 1.29) | 0.486 |
| Blood glucose, mmol/L | 5.82 (5.01, 7.38) | 6.19 (5.20, 8.26) | 5.79 (5.01, 7.37) | 0.107 |
| Haemoglobin, g/L | 137.00 (124.00, 148.00) | 128.50 (117.75, 140.25) | 137.00 (124.00, 148.00) | 0.002 |
| Haematocrit, % | 41.30 (37.80, 44.20) | 39.00 (35.05, 42.65) | 41.40 (38.00, 44.30) | 0.002 |
| LVEF, % | 58 (51, 62) | 50 (40, 58) | 58 (52, 62) | <0.001 |
| MVD, n (%) | 468 (63.7) | 32 (76.2) | 436 (62.9) | 0.082 |
| LM or LAD, n (%) | 528 (71.2) | 34 (81.0) | 494 (70.6) | 0.149 |
| Discharge medication, n (%) | ||||
| Dual antiplatelet therapy | 778 (97.5) | 40 (87.0) | 738 (98.1) | 0.001 |
| Statins | 783 (98.1) | 46 (100.0) | 737 (98.0) | 1.000 |
| β-blockers | 561 (70.4) | 35 (76.1) | 526 (70.0) | 0.506 |
| ACEI/ARB | 331 (41.5) | 24 (52.2) | 307 (40.9) | 0.131 |
| CCB | 176 (22.1) | 11 (23.9) | 165 (22.0) | 0.762 |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Male | 1.410 | 0.769 to 2.587 | 0.267 | |||
| Smoking | 0.420 | 0.208 to 0.846 | 0.015 | 0.791 | 0.375 to 1.672 | 0.540 |
| GRACE score | 1.027 | 1.017 to 1.037 | <0.001 | 1.017 | 1.006 to 1.029 | 0.002 |
| Previous CAD | 1.886 | 1.028 to 3.459 | 0.041 | 1.651 | 0.877 to 3.108 | 0.120 |
| Atrial fibrillation | 4.658 | 2.308 to 9.401 | <0.001 | 2.249 | 1.007 to 5.024 | 0.048 |
| Diabetes | 1.790 | 1.003 to 3.193 | 0.049 | 1.437 | 0.769 to 2.683 | 0.256 |
| Hypertension | 1.501 | 0.790 to 2.851 | 0.215 | |||
| Uric acid | 1.003 | 1.001 to 1.006 | 0.007 | 1.002 | 1.000 to 1.005 | 0.054 |
| TG | 0.642 | 0.438 to 0.940 | 0.023 | 0.757 | 0.522 to 1.097 | 0.142 |
| TC | 0.993 | 0.788 to 1.253 | 0.956 | |||
| LDL-C | 1.024 | 0.753 to 1.394 | 0.879 | |||
| HDL-C | 1.107 | 0.414 to 2.961 | 0.839 | |||
| MVD | 1.887 | 0.927 to 3.840 | 0.080 | |||
| LM or LAD | 1.770 | 0.819 to 3.824 | 0.146 | |||
| Haematocrit | 0.921 | 0.881 to 0.963 | <0.001 | 0.960 | 0.908 to 1.016 | 0.159 |
| Dual antiplatelet therapy | 0.145 | 0.062 to 0.343 | <0.001 | 0.493 | 0.179 to 1.354 | 0.170 |
| Statins | 20.685 | 0.002 to 262,630.802 | 0.530 | |||
| β-blockers | 1.353 | 0.687 to 2.664 | 0.382 | |||
| ACEI/ARB | 1.563 | 0.876 to 2.788 | 0.130 | |||
| CCB | 1.094 | 0.555 to 2.153 | 0.796 | |||
| Variable | HR | 95% CI | p Value | |
|---|---|---|---|---|
| Serum albumin | 0.918 | 0.844 | 0.998 | 0.044 |
| Total lymphocyte count | 0.676 | 0.379 | 1.206 | 0.185 |
| Weight loss | 0.956 | 0.447 | 2.043 | 0.907 |
| PNI | 0.926 | 0.867 | 0.989 | 0.022 |
| GNRI | 0.952 | 0.907 | 1.001 | 0.053 |
| Model | All-Cause Mortality | |||||
|---|---|---|---|---|---|---|
| C-Index (95% CI) | p Value | IDI (95% CI) | p Value | NRI (95% CI) | p Value | |
| GRACE score | 0.722 (0.644, 0.799) | Ref. | Ref. | Ref. | Ref. | Ref. |
| GRACE score + GNRI | 0.736 (0.661, 0.810) | 0.198 | 0.000 (0.000, 0.010) | 0.286 | 0.070 (0.004, 0.187) | <0.001 |
| GRACE score + PNI | 0.740 (0.669, 0.812) | 0.027 | 0.006 (0.000, 0.014) | <0.001 | 0.095 (0.004, 0.147) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, X.; Xiong, S.; Chen, Y.; Cheng, L.; Chen, Q.; Yang, S.; Qi, L.; Liu, H.; Cai, L. The Predictive Value of Different Nutritional Indices Combined with the GRACE Score in Predicting the Risk of Long-Term Death in Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention. J. Cardiovasc. Dev. Dis. 2022, 9, 358. https://doi.org/10.3390/jcdd9100358
Chen X, Xiong S, Chen Y, Cheng L, Chen Q, Yang S, Qi L, Liu H, Cai L. The Predictive Value of Different Nutritional Indices Combined with the GRACE Score in Predicting the Risk of Long-Term Death in Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention. Journal of Cardiovascular Development and Disease. 2022; 9(10):358. https://doi.org/10.3390/jcdd9100358
Chicago/Turabian StyleChen, Xu, Shiqiang Xiong, Yingzhong Chen, Lianchao Cheng, Qiang Chen, Siqi Yang, Lingyao Qi, Hanxiong Liu, and Lin Cai. 2022. "The Predictive Value of Different Nutritional Indices Combined with the GRACE Score in Predicting the Risk of Long-Term Death in Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention" Journal of Cardiovascular Development and Disease 9, no. 10: 358. https://doi.org/10.3390/jcdd9100358