
Burden from Study Questionnaire on Patient Fatigue in Qualitative Congestive Heart Failure Research


Abstract
:1. Introduction
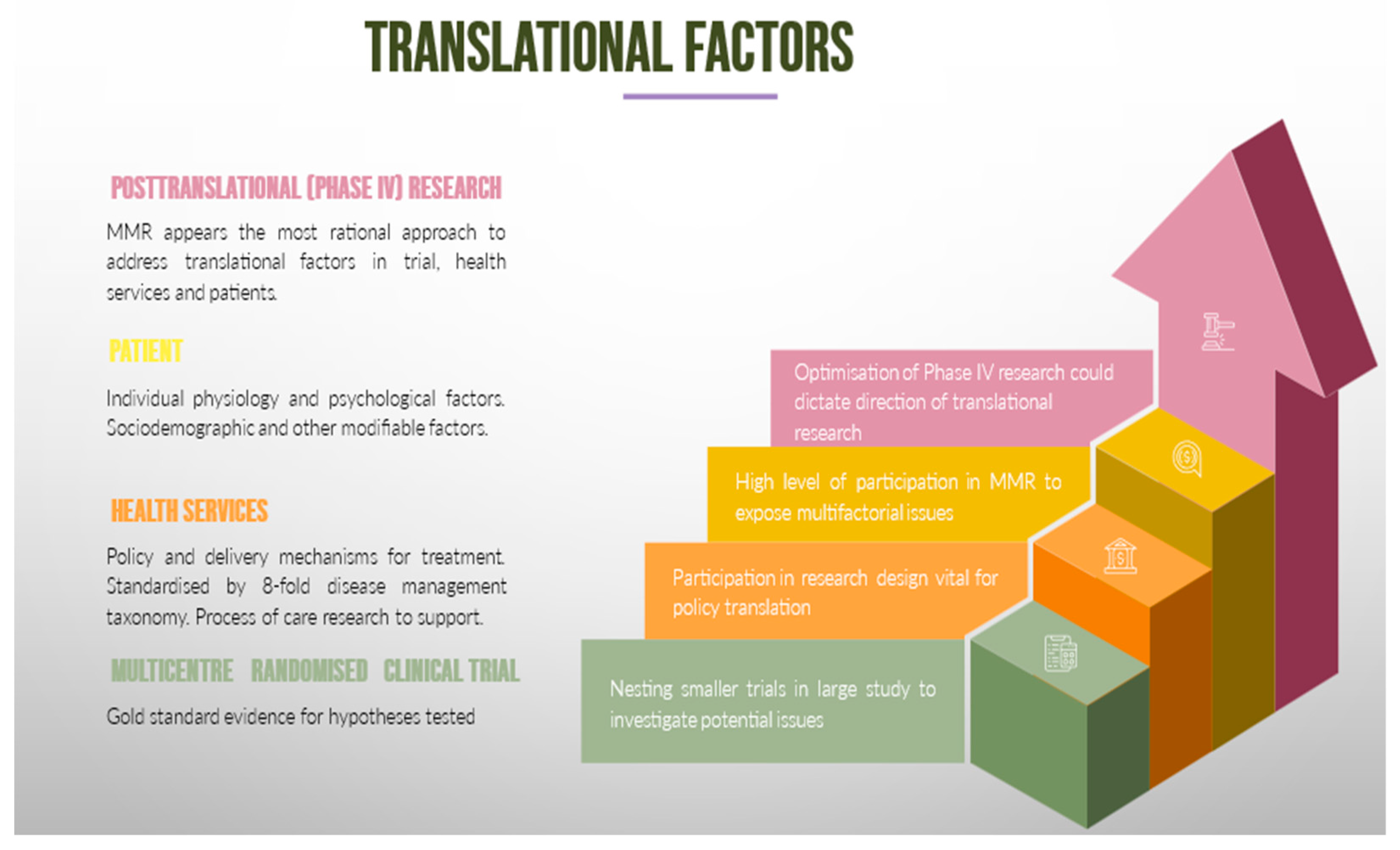
2. Mixed Method Research in Translating CVD and CHF Guidelines
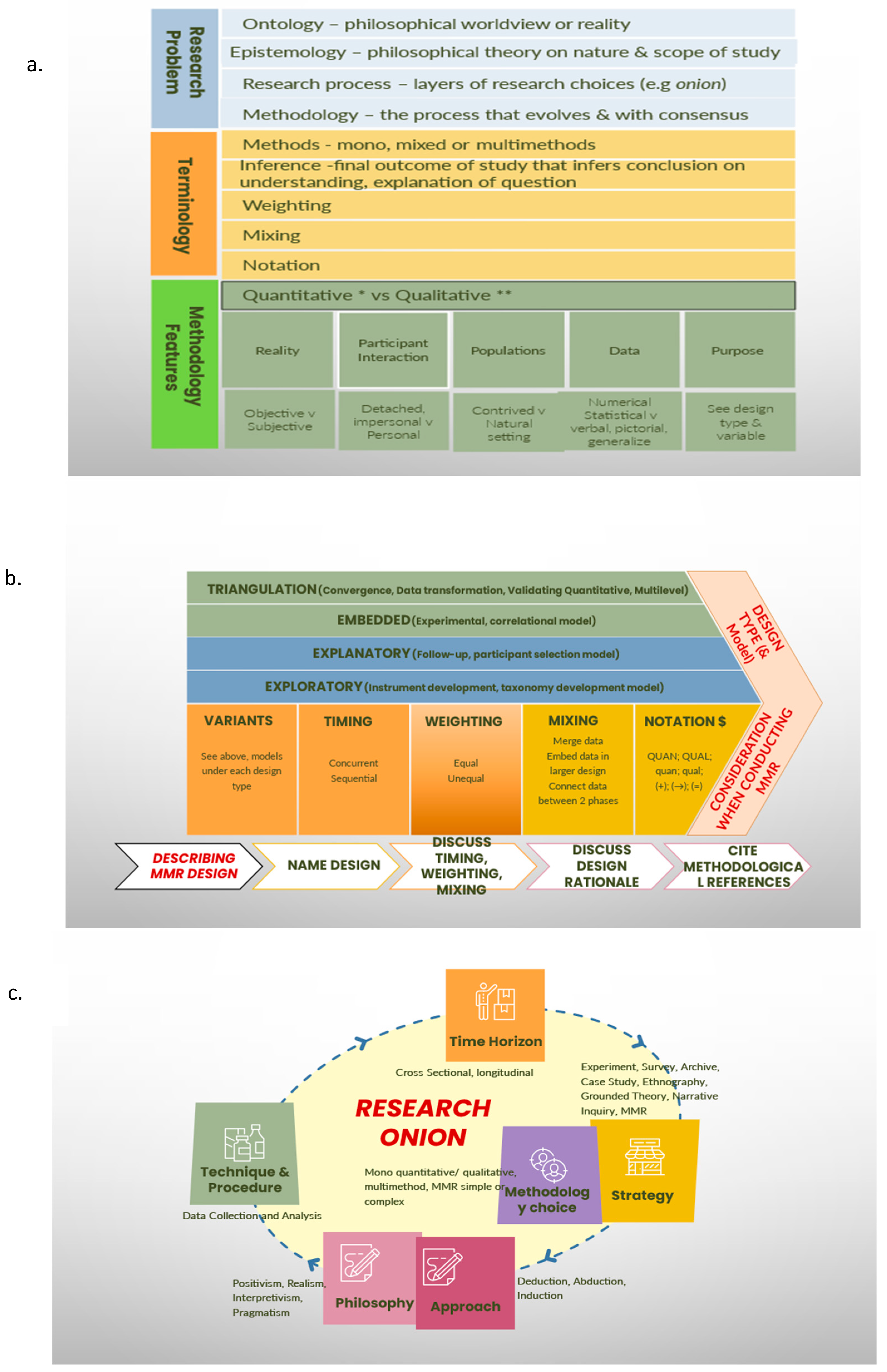
2.1. Foundations of Combining Research Methodologies
2.2. What Are the Issues with Translating Gold Standard Evidence?
2.3. Incidental Post-Trial Population-Level Patient Factors in Congestive Heart Failure
3. Data Accumulation and Patient Fatigue
3.1. Subjective Questionnaires in Medical Research
- Economical and efficient means to collect information, attitudes and opinions from many people or monitor a program’s progress.
- A high level of skill and knowledge is required to design and conduct quality surveys. These skills include knowledge on how to design surveys to answer a focused research question, understanding how to design survey items and response options that will yield interpretable and usable results, understanding survey structures such that the individual items contribute to answers on the research question coherently, and understanding the shortfalls of surveys within the context of the population that they study, including sampling errors, coverage errors, non-response errors, measurement errors, processing errors and transparency indexes [41].
- To understand the ethical and general considerations for the whole spectrum of the population, risk burdens and benefits, vulnerable groups and individuals.
- To be able to draw a conclusion on these subjective points, meaning that surveys must be representative of the population.
3.2. Patient Reported Measures and Subjective Questionnaires in Heart Failure
3.3. Patient Fatigue
3.4. Future Areas of Study to Improve Qualitative Research in Heart Failure

{kind=link}
{kind=link}
| Tool | Type of Measure | Summary of Instrument/Tool | Dimensions |
|---|---|---|---|
| ACIC | Health Systems | The components of ACIC were derived after specific evidence-based interventions from the six components of the Chronic Care Model. Thus, similar to this model, the ACIC addresses the main elements for improving chronic illness care at the community, organisation, practice and patient levels. | Many measures were considered:
|
| PACIC | Patient Satisfaction | 20- or 26-item patient report instruments were used to rate chronic illness care over a 6-month period. They cover 5 dimensions of care. | Many measures were considered:
|
| PSQ-18 | Patient satisfaction | Short form of PSQ-III using a Likert scale questionnaire evaluating 18 items from 7 dimensions of patient satisfaction directed toward doctors. | Many measures were considered:
|
| CAHPS | Patient satisfaction | Survey for consumers and patients to report on and evaluate their experiences with health care across 12 dimensions. | Many measures were considered:
|
| SF-36v2 | Patient reported outcomes | Patient-reported 5-point survey covering mental and physical health over eight scaled scores. Each question has equal weight, with final score from 0 to 100 scale. Lower scores are associated with greater disability. | Many measures were considered:
|
| EQ-5D | Patient reported outcomes | The most used self-administered survey, being available in >70 languages, that can be completed within minutes. Scoring based on a 3-point descriptive questionnaire and 20 cm vertical visual analogue scale with best (top) or worst health (bottom). | Many measures were considered:
|
| QWB-SA | Patient reported outcomes | Survey of an interview with 71 items scored from 0 (death) to 1.0 (full function) taking 10–15 min. It can be translated into QALY. It requires training. | Many measures were considered:
|
| HUI | Patient reported outcomes | A family of generic health profiles and preference-based systems measuring health status, reporting health-related quality of life, and producing utility scores. It explores the following: (1) experience of patients undergoing therapy; (2) long-term outcomes of disease or therapy; (3) the efficacy, effectiveness, and efficiency of interventions; and (4) health status of general populations. Each HUI attribute (dimension) has 3–6 levels of discrimination and is very responsive to changes in health caused by treatment therapies or other influences. | Three measures were considered:
|
| KCCQ | Disease specific QOL | The Kansas City Cardiomyopathy Questionnaire (KCCQ) is a new, self-administered, 23-item questionnaire developed to provide a better description of HRQoL in patients with CHF. It quantifies, in a disease-specific fashion, physical limitation, symptoms (frequency, severity and recent change over time), QoL, social interference, and self-efficacy. | Many measures were considered:
|
| MLHFQ | Disease specific QOL | A self-administered, 5–10 min, 21-item 5-point Likert variable used to measure the effects of symptoms, functional limitations, and psychological distress on an individual’s quality of life, the MLHF questionnaire asks each person to indicate using a 6-point, zero to five, Likert scale on how much each of 21 facets prevented them from living as they desired. The MLHFQ is designed to measure the effects of heart failure and its treatments on an individual’s quality of life. MLHFQ measures the effects of symptoms, functional limitations, and psychological distress on an individual’s quality of life. It consists of questions that assess the impacts of frequent physical symptoms, the effects of heart failure on physical/social functions, and side effects of treatments, hospital stays, and costs of care. | |
| NYHA | Disease specific QOL | A standardised health care provider assessment of heart failure severity. Dyspnoea grading with varying states of rest and exercise. Range of 0–4. Higher scores are worse. | One component—Universal. |
| CFPI | Understanding self-care and goals | Partners in Health Scale tests self-efficacy for managing chronic disease using a 6-item scale, Energy/Fatigue Scale, Cue and Response Score, and Problems and Goals Score. Training required for use. | Three testing methods were used:
|
| EHFScBS | CHF self-care | The EHFScBS is a 12-item questionnaire that measures 3 aspects of health maintenance behaviours: compliance with their management regimen, asking for help, and adapting daily activities. Responses are on a 5-point Likert-type scale indicating how often each behaviour is performed, ranging from “I completely agree” to “I don’t agree at all”. Scores are summed. Lower scores indicate better self-care. The instrument has subsequently been revised into a 9-item instrument. | Translated into 14 languages:
|
| SCHFI | CHF self-care | The SCHFI consists of 15 items that measure 3 subscales: behaviours undertaken to maintain clinical stability (self-care maintenance), the decision-making process with regard to symptom changes (self-care management), and the confidence to manage symptoms and evaluate any actions implemented (self-care confidence). Self-care management can only be computed if patients have been symptomatic in the past month. Summary scores for the 3 subscales are used by transforming each subscale into a scale from 0 to 100. Adequate scores are more than 70 on any subscale. | Officially translated into Spanish and Thai languages and requests to use it in 24 other countries:
|
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421, Correction in J. Am. Coll. Cardiol. 2023, 81, 1551. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [PubMed]
- Iyngkaran, P.; Usmani, W.; Hanna, F.; de Courten, M. Challenges of Health Data Use in Multidisciplinary Chronic Disease Care: Perspective from Heart Failure Care. J. Cardiovasc. Dev. Dis. 2023, 10, 486. [Google Scholar] [CrossRef] [PubMed]
- Ezekowitz, J.; Mentz, R.J.; Westerhout, C.M.; Sweitzer, N.K.; Givertz, M.M.; Piña, I.L.; O’Connor, C.M.; Greene, S.J.; McMullan, C.; Roessig, L.; et al. Participation in a Heart Failure Clinical Trial. Perspectives and Opportunities From the VICTORIA Trial and VICTORIA Simultaneous Registry. Circ. Heart Fail. 2021, 14, e008242. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S.; Ou, F.S.; Newby, L.K.; Sutton, V.; Adams, P.; Felker, G.M.; Wang, T.Y. Patient- and trial-specific barriers to participation in cardiovascular randomized clinical trials. J. Am. Coll. Cardiol. 2013, 61, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, A.; Tonks, R.W.; Adams, P.A.; Felker, G.M.; Patel, C.B.; Mentz, R.J. Enrollment in Heart Failure Clinical Trials: Insights into Which Entry Criteria Exclude Patients. J. Card. Fail. 2015, 21, 608–609. [Google Scholar] [CrossRef]
- Kamiya, K.; Sato, Y.; Takahashi, T.; Tsuchihashi-Makaya, M.; Kotooka, N.; Ikegame, T.; Takura, T.; Yamamoto, T.; Nagayama, M.; Goto, Y.; et al. Multidisciplinary Cardiac Rehabilitation and Long-Term Prognosis in Patients with Heart Failure. Circ. Heart Fail. 2020, 13, e006798. [Google Scholar] [CrossRef]
- Bozkurt, B.; Fonarow, G.C.; Goldberg, L.R.; Guglin, M.; Josephson, R.A.; Forman, D.E.; Lin, G.; Lindenfeld, J.; O’Connor, C.; Panjrath, G.; et al. ACC’s Heart Failure and Transplant Section and Leadership Council. Cardiac Rehabilitation for Patients with Heart Failure: JACC Expert Panel. J. Am. Coll. Cardiol. 2021, 77, 1454–1469. [Google Scholar] [CrossRef]
- Taylor, R.S.; Dalal, H.M.; McDonagh, S.T.J. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat. Rev. Cardiol. 2022, 19, 180–194. [Google Scholar] [CrossRef]
- Chen, Z.; Li, M.; Yin, C.; Fang, Y.; Zhu, Y.; Feng, J. Effects of cardiac rehabilitation on elderly patients with Chronic heart failure: A meta-analysis and systematic review. PLoS ONE 2022, 17, e0273251. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Stough, W.G.; Abraham, W.T.; Albert, N.M.; Gheorghiade, M.; Greenberg, B.H.; O’Connor, C.M.; Sun, J.L.; Yancy, C.W.; Young, J.B.; et al. Characteristics, Treatments, and Outcomes of Patients with Preserved Systolic Function Hospitalized for Heart Failure. J. Am. Coll. Cardiol. 2007, 50, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Fonarow, G.C.; Breathett, K.; Jurgens, C.Y.; Pisani, B.A.; Pozehl, B.J.; Spertus, J.A.; Taylor, K.G.; Thibodeau, J.T.; Yancy, C.W.; et al. 2020 ACC/AHA Clinical Performance and Quality Measures for Adults with Heart Failure. A Report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e000099. [Google Scholar] [CrossRef] [PubMed]
- Leech, N.; Onwuegbuzie, A. A typology of mixed methods research designs. Qual. Quant. 2008, 43, 265–275. [Google Scholar] [CrossRef]
- Iyngkaran, P.; Liew, D.; McDonald, P.; Thomas, M.C.; Reid, C.; Chew, D.; Hare, D.L. Phase 4 Studies in Heart Failure—What is Done and What is Needed? Curr. Cardiol. Rev. 2016, 12, 216–230. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Fetters, M.D. The Mixed Methods Research Workbook: Activities for Designing, Implementing, and Publishing Projects; Sage: Thousand Oaks, CA, USA, 2020. [Google Scholar]
- Fàbregues, S.; Escalante-Barrios, E.L.; Molina-Azorin, J.F.; Hong, Q.N.; Verd, J.M. Taking a critical stance towards mixed methods research: A cross-disciplinary qualitative secondary analysis of researchers’ views. PLoS ONE 2021, 16, e0252014. [Google Scholar] [CrossRef]
- Plano Clark, V.L.; Ivankova, N.V. Mixed Methods Research: A Guide to the Field; Sage: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Tashakkori, A.; Teddlie, C. (Eds.) Epilogue: Current developments and emerging trends in integrated research methodology. In The SAGE Handbook of Mixed Methods in Social and Behavioral Research, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2010; pp. 803–826. [Google Scholar]
- Creswell, J.W. Controversies in mixed methods research. In The SAGE Handbook of Qualitative Research, 4th ed.; Denzin, N.K., Lincoln, Y., Eds.; Sage: Thousand Oaks, CA, USA, 2011; pp. 269–283. [Google Scholar]
- Andrew, S.; Halcomb, E.J. Mixed methods research is an effective method of enquiry for community health research. Adv. Contemp. Nurse 2006, 23, 145–153. [Google Scholar] [CrossRef]
- Greene, J.C.; Caracelli, V.J.; Graham, W.F. Toward a conceptual framework for mixed methods evaluation design. Educ. Eval. Policy Anal. 1989, 11, 255–274. [Google Scholar] [CrossRef]
- Heneghan, C.; Goldacre, B.; Mahtani, K.R. Why clinical trial outcomes fail to translate into benefits for patients. Trials 2017, 18, 122. [Google Scholar] [CrossRef]
- Krumholz, H.M.; Currie, P.M.; Riegel, B.; Phillips, C.O.; Peterson, E.D.; Smith, R.; Yancy, C.W.; Faxon, D.P. American Heart Association Disease Management Taxonomy Writing Group. A taxonomy for disease management: A scientific statement from the American Heart Association Disease Management Taxonomy Writing Group. Circulation 2006, 114, 1432–1445. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Albert, N.M.; Curtis, A.B.; Gheorghiade, M.; Heywood, J.T.; Liu, Y.; Mehra, M.R.; O’Connor, C.M.; Reynolds, D.; Walsh, M.N.; et al. Associations between outpatient heart failure process-of-care measures and mortality. Circulation 2011, 123, 1601–1610. [Google Scholar] [CrossRef]
- Schjødt, I.; Johnsen, S.P.; Strömberg, A.; DeVore, A.D.; Valentin, J.B.; Løgstrup, B.B. Evidence-Based Process Performance Measures and Clinical Outcomes in Patients with Incident Heart Failure with Reduced Ejection Fraction: A Danish Nationwide Cohort Study. Circ. Cardiovasc. Qual. Outcomes 2022, 15, e007973. [Google Scholar] [CrossRef] [PubMed]
- Al-Mohammad, A. Hydralazine and nitrates in the treatment of heart failure with reduced ejection fraction. ESC Heart Fail. 2019, 6, 878–883. [Google Scholar] [CrossRef] [PubMed]
- Iyngkaran, P.; Thomas, M.C.; Johnson, R.; French, J.; Ilton, M.; McDonald, P.; Hare, D.L.; Fatkin, D. Contextualizing Genetics for Regional Heart Failure Care. Curr. Cardiol. Rev. 2016, 12, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Gu, A.; Yue, Y.; Desai Raj, P.; Argulian, E. Racial and ethnic differences in antihypertensive medication use and blood pressure control among US adults with hypertension. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003166. [Google Scholar] [CrossRef]
- Iyngkaran, P.; Majoni, W.; Cass, A.; Sanders, P.; Ronco, C.; Brady, S.; Kangaharan, N.; Ilton, M.; Hare, D.L.; Thomas, M.C. Northern Territory perspectives on heart failure with comorbidities—Understanding trial validity and exploring collaborative opportunities to broaden the evidence base. Heart Lung Circ. 2015, 24, 536–543. [Google Scholar] [CrossRef]
- Bibbins-Domingo, K.; Pletcher, M.J.; Lin, F.; Vittinghoff, E.; Gardin, J.M.; Arynchyn, A.; Lewis, C.E.; Williams, O.D.; Hulley, S.B. Racial differences in incident heart failure among young adults. N. Engl. J. Med. 2009, 360, 1179–1190. [Google Scholar] [CrossRef]
- Morris, A.A.; Patel, R.S.; Binongo, J.N.; Poole, J.; Al Mheid, I.; Ahmed, Y.; Stoyanova, N.; Vaccarino, V.; Din-Dzietham, R.; Gibbons, G.H.; et al. Racial differences in arterial stiffness and microcirculatory function between Black and White Americans. J. Am. Heart Assoc. 2013, 2, e002154. [Google Scholar] [CrossRef]
- Xu, H.; Dorn, G.W.; Shetty, A.; Parihar, A.; Dave, T.; Robinson, S.W.; Gottlieb, S.S.; Donahue, M.P.; Tomaselli, G.F.; Kraus, W.E.; et al. A genome-wide association study of idiopathic dilated cardiomyopathy in African Americans. J. Pers. Med. 2018, 8, 11. [Google Scholar] [CrossRef]
- Myers, V.D.; Gerhard, G.S.; McNamara, D.M.; Tomar, D.; Madesh, M.; Kaniper, S.; Ramsey, F.V.; Fisher, S.G.; Ingersoll, R.G.; Kasch-Semenza, L.; et al. Association of variants in BAG3 with cardiomyopathy outcomes in African American Individuals. JAMA Cardiol. 2018, 3, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Irizarry, O.C.; Levine, L.D.; Lewey, J.; Boyer, T.; Riis, V.; Elovitz, M.A.; Arany, Z. Comparison of clinical characteristics and outcomes of peripartum cardiomyopathy between African American and Non-African American Women. JAMA Cardiol. 2017, 2, 1256–1260. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.K.; de Lemos, J.A.; Ayers, C.R.; Berry, J.D.; Wang, T.J. Racial differences in natriuretic peptide levels: The dallas heart study. JACC Heart Fail. 2015, 3, 513–519. [Google Scholar] [CrossRef]
- Morris, A.A.; Nayak, A.; Ko, Y.-A.; D’Souza, M.; Felker, G.M.; Redfield, M.M.; Tang, W.H.W.; Testani, J.M.; Butler, J. Racial differences in diuretic efficiency, plasma renin, and rehospitalization in subjects with acute heart failure. Circ. Heart Fail. 2020, 13, e006827. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.I.; Freedman, B.I.; Ellison, D.H.; Rodriguez, C.J. Salt sensitivity: A review with a focus on non-Hispanic blacks and Hispanics. J. Am. Soc. Hypertens. 2013, 7, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Nayak, A.; Hicks, A.J.; Morris, A.A. Understanding the Complexity of Heart Failure Risk and Treatment in Black Patients. Circ. Heart Fail. 2020, 13, e007264. [Google Scholar] [CrossRef]
- Fowler, F.J. Improving Survey Questions: Design and Evaluation; Applied Social Research Methods Series; Sage Publishing: Thousand Oaks, CA, USA, 1995; Volume 38. [Google Scholar]
- VanGeest, J.B.; Johnson, T.P.; Welch, V.L. Methodologies for improving response rates in surveys of physicians: A systematic review. Eval. Health Prof. 2007, 30, 303–321. [Google Scholar] [CrossRef]
- Audibert, C.; Glass, D.; Johnson, T.P. Method and transparency of online physician surveys: An overview. Surv. Methods Insights Field 2020. [Google Scholar] [CrossRef]
- Cunningham, C.T.; Quan, H.; Hemmelgarn, B.; Noseworthy, T.; A Beck, C.; Dixon, E.; Samuel, S.; A Ghali, W.; Sykes, L.L.; Jetté, N. Exploring physician specialist response rates to web-based surveys. BMC Med. Res. Methodol. 2015, 15, 32. [Google Scholar] [CrossRef] [PubMed]
- Bennett, C.; Khangura, S.; Brehaut, J.C.; Graham, I.D.; Moher, D.; Potter, B.K.; Grimshaw, J.M. Reporting Guidelines for Survey Research: An Analysis of Published Guidance and Reporting Practices. PLoS Med. 2011, 8, e1001069. [Google Scholar] [CrossRef]
- Wolfe, A. Institute of Medicine Report: Crossing the Quality Chasm: A New Health Care System for the 21st Century. Policy Politics Nurs. Pract. 2001, 2, 233–235. [Google Scholar] [CrossRef]
- Cella, D.; Hahn, E.A.; Jensen, S.E.; Butt, Z.; Nowinski, C.J.; Rothrock, N.; Lohr, K.N. Patient-Reported Outcomes in Performance Measurement; RTI Press: Research Triangle Park, NC, USA, 2015. [Google Scholar]
- US Food and Drug Administration. Guidance for Industry: Patientreported Outcome Measures: Use in Medical Product Development to Support Labeling Claims. December 2009. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/patientreported-outcome-measures-use-medical-product-developmentsupport-labeling-claims (accessed on 12 March 2023).
- Agarwal, A.; Pain, T.; Levesque, J.F.; Girgis, A.; Hoffman, A.; Karnon, J.; King, M.T.; Shah, K.K.; Morton, R.L.; HSRAANZ PROMs Special Interest Group. Patient-reported outcome measures (PROMs) to guide clinical care: Recommendations and challenges. Med. J. Aust. 2022, 216, 9–11. [Google Scholar] [CrossRef]
- Kelkar, A.A.; Spertus, J.; Pang, P.; Pierson, R.F.; Cody, R.J.; Pina, I.L.; Hernandez, A.; Butler, J. Utility of Patient-Reported Outcome Instruments in Heart Failure. JACC Heart Fail. 2016, 4, 165–175. [Google Scholar] [CrossRef]
- Psotka, M.A.; von Maltzahn, R.; Anatchkova, M.; Agodoa, I.; Chau, D.; Malik, F.I.; Patrick, D.L.; Spertus, J.A.; Wiklund, I.; Teerlink, J.R. Patient-Reported Outcomes in Chronic Heart Failure: Applicability for Regulatory Approval. JACC Heart Fail. 2016, 4, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Rolstad, S.; Adler, J.; Rydén, A. Response burden and questionnaire length: Is shorter better? A review and meta-analysis. Value Health 2011, 14, 1101–1108. [Google Scholar] [CrossRef]
- Edwards, P.; Roberts, I.; Sandercock, P.; Frost, C. Follow-up by mail in clinical trials: Does questionnaire length matter? Control. Clin. Trials 2004, 25, 31–52. [Google Scholar] [CrossRef]
- Hatch, R.; Young, D.; Barber, V.; Harrison, D.A.; Watkinson, P. The effect of postal questionnaire burden on response rate and answer patterns following admission to intensive care: A randomised controlled trial. BMC Med. Res. Methodol. 2017, 17, 49. [Google Scholar] [CrossRef]
- Edwards, P.; Roberts, I.; Clarke, M.; DiGuiseppi, C.; Pratap, S.; Wentz, R.; Kwan, I.; Cooper, R. Methods to increase response rates to postal questionnaires. Cochrane Database Syst. Rev. 2007, 2, MR000008, Update in Cochrane Database Syst. Rev. 2009, 3, MR000008. [Google Scholar] [CrossRef]
- Nakash, R.A.; Hutton, J.L.; Jørstad-Stein, E.C.; Gates, S.; Lamb, S.E. Maximising response to postal questionnaires--a systematic review of randomised trials in health research. BMC Med. Res. Methodol. 2006, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Iyngkaran, P.; Hanna, F.; Andrew, S.; Horowitz, J.D.; Battersby, M.; De Courten, M.P. Comparison of Short and Long Form Flinders Program of Chronic Disease SELF-MANagement on Participants starting SGLT-2 Inhibitors for Congestive Heart Failure (SELFMAN-HF): Protocol for a prospective, observational study. Front. Med. 2023, 10, 1059735. [Google Scholar] [CrossRef] [PubMed]
- Rubio, R.; Palacios, B.; Varela, L.; Fernández, R.; Correa, S.C.; Estupiñan, M.F.; Calvo, E.; José, N.; Muñoz, M.R.; Yun, S.; et al. Quality of life and disease experience in patients with heart failure with reduced ejection fraction in Spain: A mixed-methods study. BMJ Open 2021, 11, e053216. [Google Scholar] [CrossRef]
- Patel, K.K.; Veenstra, D.L.; Patrick, D.L. A review of selected patient-generated outcome measures and their application in clinical trials. Value Health 2003, 6, 595–603. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, Version 6.3; Updated February 2022. Cochrane; 2022. Available online: www.training.cochrane.org/handbook (accessed on 2 November 2023).
- Iyngkaran, P.; Toukhsati, S.R.; Harris, M.; Connors, C.; Kangaharan, N.; Ilton, M.; Nagel, T.; Moser, D.K.; Battersby, M. Self Managing Heart Failure in Remote Australia—Translating Concepts into Clinical Practice. Curr. Cardiol. Rev. 2016, 12, 270–284. [Google Scholar] [CrossRef]
- Goh, F.Q.; Kong, W.K.F.; Wong, R.C.C.; Chong, Y.F.; Chew, N.W.S.; Yeo, T.-C.; Sharma, V.K.; Poh, K.K.; Sia, C.-H. Cognitive Impairment in Heart Failure—A Review. Biology 2022, 11, 179. [Google Scholar] [CrossRef]
- Ventoulis, I.; Arfaras-Melainis, A.; Parissis, J.; Polyzogopoulou, E. Cognitive Impairment in Acute Heart Failure: Narrative Review. J. Cardiovasc. Dev. Dis. 2021, 8, 184. [Google Scholar] [CrossRef] [PubMed]
- John, J.E.; Claggett, B.; Skali, H.; Solomon, S.D.; Cunningham, J.W.; Matsushita, K.; Konety, S.H.; Kitzman, D.W.; Mosley, T.H.; ClarkIII, D.; et al. Coronary Artery Disease and Heart Failure with Preserved Ejection Fraction: The ARIC Study. J. Am. Heart Assoc. 2022, 11, e021660. [Google Scholar] [CrossRef] [PubMed]
- Hegyi, B.; Hernandez, J.M.; Ko, C.Y.; Hong, J.; Shen, E.Y.; Spencer, E.R.; Smoliarchuk, D.; Navedo, M.F.; Bers, D.M.; Bossuyt, J. Diabetes and Excess Aldosterone Promote Heart Failure with Preserved Ejection Fraction. J. Am. Heart Assoc. 2022, 11, e027164. [Google Scholar] [CrossRef] [PubMed]
- Omar, A.M.S.; Rahman, M.A.A.; Rifaie, O.; Bella, J.N. Atrial Fibrillation in Heart Failure with Preserved Left Ventricular Systolic Function: Distinct Elevated Risk for Cardiovascular Outcomes in Women Compared to Men. J. Cardiovasc. Dev. Dis. 2022, 9, 417. [Google Scholar] [CrossRef] [PubMed]
- Tamirisa, K.P.; Dye, C.; Bond, R.M.; Hollier, L.M.; Marinescu, K.; Vaseghi, M.; Russo, A.M.; Gulati, M.; Volgman, A.S. Arrhythmias and Heart Failure in Pregnancy: A Dialogue on Multidisciplinary Collaboration. J. Cardiovasc. Dev. Dis. 2022, 9, 199. [Google Scholar] [CrossRef]
- Horodinschi, R.N.; Diaconu, C.C. Heart Failure and Atrial Fibrillation: Diastolic Function Differences Depending on Left Ventricle Ejection Fraction. Diagnostics 2022, 12, 839. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iyngkaran, P.; Usmani, W.; Bahmani, Z.; Hanna, F. Burden from Study Questionnaire on Patient Fatigue in Qualitative Congestive Heart Failure Research. J. Cardiovasc. Dev. Dis. 2024, 11, 96. https://doi.org/10.3390/jcdd11040096
Iyngkaran P, Usmani W, Bahmani Z, Hanna F. Burden from Study Questionnaire on Patient Fatigue in Qualitative Congestive Heart Failure Research. Journal of Cardiovascular Development and Disease. 2024; 11(4):96. https://doi.org/10.3390/jcdd11040096
Chicago/Turabian StyleIyngkaran, Pupalan, Wania Usmani, Zahra Bahmani, and Fahad Hanna. 2024. "Burden from Study Questionnaire on Patient Fatigue in Qualitative Congestive Heart Failure Research" Journal of Cardiovascular Development and Disease 11, no. 4: 96. https://doi.org/10.3390/jcdd11040096