
Lower Limit of Normality of Segmental Multilayer Longitudinal Strain in Healthy Adult Subjects
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Two-Dimensional Echocardiographic Imaging and Measurements
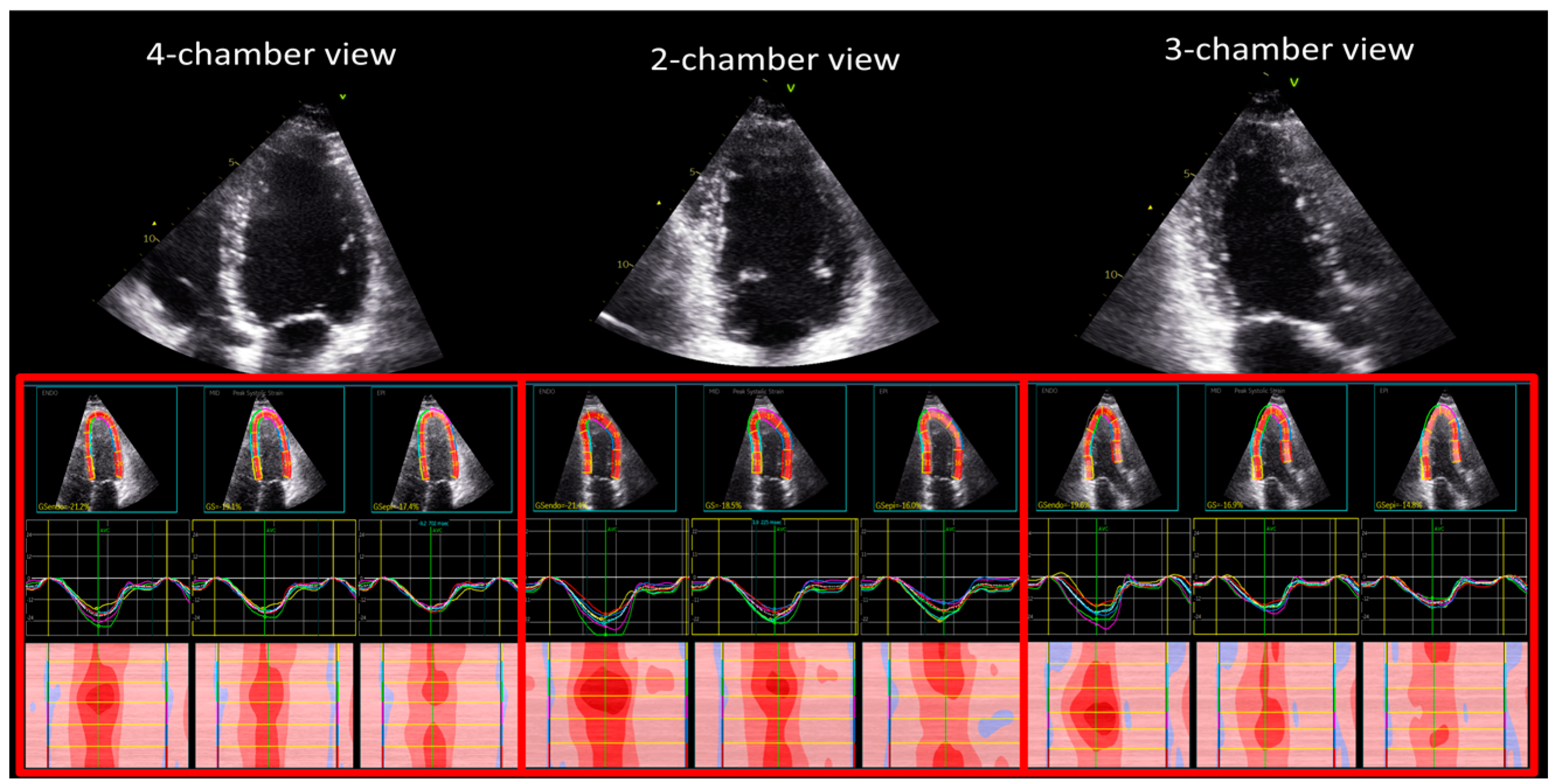
2.2. Two-Dimensional Echocardiographic Strain Measurements
2.3. Statistical Analysis
3. Results
3.1. Demographic and Standard Echocardiographic Characteristics
3.2. Global Longitudinal Strain
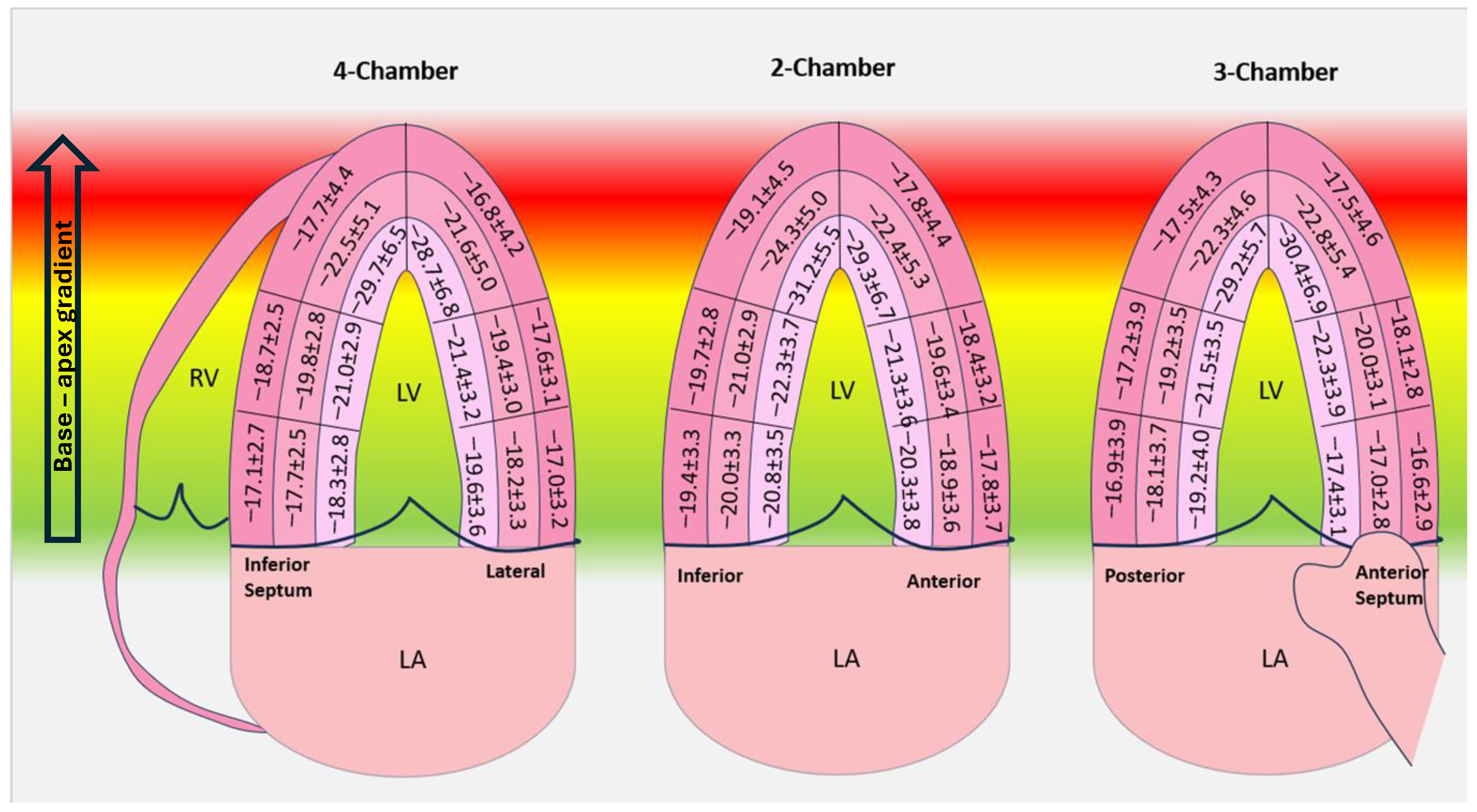
3.3. Segmental Longitudinal Strain
3.4. Reproducibility of the Measurements
4. Discussion
4.1. Global Longitudinal Strain
4.2. Segmental Longitudinal Strain
4.3. Study Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. J. Am. Soc. Echocardiogr. 2015, 28, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Kalam, K.; Otahal, P.; Marwick, T.H. Prognostic implications of global LV dysfunction: A systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart 2014, 100, 1673–1680. [Google Scholar] [CrossRef] [PubMed]
- Phelan, D.; Collier, P.; Thavendiranathan, P.; Popović, Z.B.; Hanna, M.; Plana, J.C.; Marwick, T.H.; Thomas, J.D. Relative apical sparing of longitudinal strain using two-dimensional speckle-tracking echocardiography is both sensitive and specific for the diagnosis of cardiac amyloidosis. Heart 2012, 98, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Risum, N.; Jons, C.; Olsen, N.T.; Fritz-Hansen, T.; Bruun, N.E.; Hojgaard, M.V.; Valeur, N.; Kronborg, M.B.; Kisslo, J.; Sogaard, P. Simple regional strain pattern analysis to predict response to cardiac resynchronization therapy: Rationale, initial results, and advantages. Am. Heart J. 2012, 163, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Edvardsen, T.; Skulstad, H.; Aakhus, S.; Urheim, S.; Ihlen, H. Regional myocardial systolic function during acute myocardial ischemia assessed by strain Doppler echocardiography. J. Am. Coll. Cardiol. 2001, 37, 726–730. [Google Scholar] [CrossRef]
- Uppu, S.C.; Shah, A.; Weigand, J.; Nielsen, J.C.; Ko, H.H.; Parness, I.A.; Srivastava, S. Two-Dimensional Speckle-Tracking-Derived Segmental Peak Systolic Longitudinal Strain Identifies Regional Myocardial Involvement in Patients with Myocarditis and Normal Global Left Ventricular Systolic Function. Pediatr. Cardiol. 2015, 36, 950–959. [Google Scholar] [CrossRef] [PubMed]
- Sperlongano, S.; D’Amato, A.; Tagliamonte, E.; Russo, V.; Desiderio, A.; Ilardi, F.; Muscogiuri, G.; Esposito, G.; Pontone, G.; Esposito, G.; et al. Acute myocarditis: Prognostic role of speckle tracking echocardiography and comparison with cardiac magnetic resonance features. Heart Vessel. 2022, 37, 121–131. [Google Scholar] [CrossRef]
- Mirea, O.; Pagourelias, E.; Duchenne, J.; Bogaert, J.; Thomas, J.D.; Badano, L.P.; Voigt, J.-U.; on behalf of the EACVI-ASE-Industry Standardization Task Force. Intervendor Differences in the Accuracy of Detecting Regional Functional Abnormalities: A Report From the EACVI-ASE Strain Standardization Task Force. J. Am. Coll. Cardiol. Imaging 2018, 11, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart. J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- Liao, J.J.; Capen, R.C.; Schofield, T.L. Assessing the reproducibility of an analytical method. J. Chromatogr. Sci. 2006, 44, 119–122. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef]
- Ho, S.Y. Anatomy and myoarchitecture of the left ventricular wall in normal and in disease. Eur. J. Echocardiogr. 2009, 10, iii3–iii7. [Google Scholar] [CrossRef] [PubMed]
- Smiseth, O.A.; Torp, H.; Opdahl, A.; Haugaa, K.H.; Urheim, S. Myocardial strain imaging: How useful is it in clinical decision making? Eur. Heart J. 2016, 37, 1196–1207. [Google Scholar] [CrossRef] [PubMed]
- Edvardsen, T.; Helle-Valle, T.; Smiseth, O.A. Systolic Dysfunction in Heart Failure with Normal Ejection Fraction: Speckle-Tracking Echocardiography. Prog. Cardiovasc. Dis. 2006, 49, 207–214. [Google Scholar] [CrossRef]
- Ewe, S.H.; Haeck, M.L.; Ng, A.C.; Witkowski, T.G.; Auger, D.; Leong, D.P.; Abate, E.; Marsan, N.A.; Holman, E.R.; Schalij, M.J.; et al. Detection of subtle left ventricular systolic dysfunction in patients with significant aortic regurgitation and preserved left ventricular ejection fraction: Speckle tracking echocardiographic analysis. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 992–999. [Google Scholar] [CrossRef] [PubMed]
- Nakai, H.; Takeuchi, M.; Nishikage, T.; Lang, R.M.; Otsuji, Y. Subclinical left ventricular dysfunction in asymptomatic diabetic patients assessed by two-dimensional speckle tracking echocardiography: Correlation with diabetic duration. Eur. J. Echocardiogr. 2009, 10, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Ono, S.; Waldman, L.K.; Yamashita, H.; Covell, J.W.; Ross, J., Jr. Effects of coronary artery reperfusion on transmural myocardial remodeling in dogs. Circulation 1995, 91, 1143–1153. [Google Scholar] [CrossRef]
- Altiok, E.; Neizel, M.; Tiemann, S.; Krass, V.; Kuhr, K.; Becker, M.; Zwicker, C.; Koos, R.; Lehmacher, W.; Kelm, M. Quantitative analysis of endocardial and epicardial left ventricular myocardial deformation-comparison of strain-encoded cardiac magnetic resonance imaging with two-dimensional speckle-tracking echocardiography. J. Am. Soc. Echocardiogr. 2012, 25, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Dalen, H.; Thorstensen, A.; Aase, S.A.; Ingul, C.B.; Torp, H.; Vatten, L.J.; Stoylen, A. Segmental and global longitudinal strain and strain rate based on echocardiography of 1266 healthy individuals: The HUNT study in Norway. Eur. J. Echocardiogr. 2010, 11, 176–183. [Google Scholar] [CrossRef]
- Shi, J.; Pan, C.; Kong, D.; Cheng, L.; Shu, X. Left Ventricular Longitudinal and Circumferential Layer-Specific Myocardial Strains and Their Determinants in Healthy Subjects. Echocardiography 2016, 33, 510–518. [Google Scholar] [CrossRef]
- Alcidi, G.M.; Esposito, R.; Evola, V.; Santoro, C.; Lembo, M.; Sorrentino, R.; Lo Iudice, F.; Borgia, F.; Novo, G.; Trimarco, B.; et al. Normal reference values of multilayer longitudinal strain according to age decades in a healthy population: A single-centre experience. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1390–1396. [Google Scholar] [CrossRef] [PubMed]
- Aygen, M.; Popp, R.L. Influence of the orientation of myocardial fibers on echocardiographic images. Am. J. Cardiol. 1987, 60, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Huttin, O.; Xhaard, C.; Dandine-Roulland, C.; Le Floch, E.; Bacq-Daian, D.; Lamiral, Z.; Bozec, E.; Deleuze, J.-F.; Zannad, F.; Rossignol, P.; et al. Layer myocardial strain is the most heritable echocardiographic trait. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 1394–1403. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, T.; Dulgheru, R.; Bernard, A.; Ilardi, F.; Contu, L.; Addetia, K.; Caballero, L.; Akhaladze, N.; Athanassopoulos, G.D.; Barone, D.; et al. Echocardiographic reference ranges for normal left ventricular 2D strain: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, J.; Jakobsen, E.O.; Østvik, A.; Holte, E.; Stølen, S.; Lovstakken, L.; Grenne, B.; Dalen, H. Echocardiographic Reference Ranges of Global Longitudinal Strain for All Cardiac Chambers Using Guideline-Directed Dedicated Views. JACC Cardiovasc. Imaging 2023, 16, 1516–1531. [Google Scholar] [CrossRef] [PubMed]
- Anan, R.; Imoto, T.; Onizuka, K.; Watanabe, H.; Mori, W.; Murakoso, M. Concentric hypertrophy geometry is a significant determinant of impaired global longitudinal strain in patients with normal cardiac structure and function. Heliyon 2023, 9, e16252. [Google Scholar] [CrossRef]
- Mirea, O.; Pagourelias, E.D.; Duchenne, J.; Bogaert, J.; Thomas, J.D.; Badano, L.P.; Voigt, J.U. EACVI-ASE-Industry Standardization Task Force. Variability and Reproducibility of Segmental Longitudinal Strain Measurement: A Report From the EACVI-ASE Strain Standardization Task Force. JACC Cardiovasc. Imaging 2018, 11, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Forsha, D.; Risum, N.; Rajagopal, S.; Dolgner, S.; Hornik, C.; Barnhart, H.; Kisslo, J.; Barker, P. The influence of angle of insonation and target depth on speckle-tracking strain. J. Am. Soc. Echocardiogr. 2015, 28, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Bière, L.; Donal, E.; Terrien, G.; Kervio, G.; Willoteaux, S.; Furber, A.; Prunier, F. Longitudinal strain is a marker of microvascular obstruction and infarct size in patients with acute ST-segment elevation myocardial infarction. PLoS ONE 2014, 9, e86959. [Google Scholar] [CrossRef]
- Nardozza, M.; Chiodi, E.; Mele, D. Left Ventricle Relative Apical Sparing in Cardiac Amyloidosis. J. Cardiovasc. Echogr. 2017, 27, 141–142. [Google Scholar]
- Wali, E.; Gruca, M.; Singulane, C.; Cotella, J.; Guile, B.; Johnson, R.; Mor-Avi, V.; Addetia, K.; Lang, R.M. How Often Does Apical Sparing of Longitudinal Strain Indicate the Presence of Cardiac Amyloidosis? Am. J. Cardiol. 2023, 202, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Lagies, R.; Beck, B.B.; Hoppe, B.; Sreeram, N.; Udink Ten Cate, F.E. Apical sparing of longitudinal strain, left ventricular rotational abnormalities, and short-axis dysfunction in primary hyperoxaluria type 1. Circ. Heart Fail. 2013, 6, e45–e47. [Google Scholar] [CrossRef] [PubMed]
- Abecasis, J.; Lopes, P.; Santos, R.R.; Maltês, S.; Guerreiro, S.; Ferreira, A.; Freitas, P.; Ribeiras, R.; Andrade, M.J.; Manso, R.T.; et al. Prevalence and significance of relative apical sparing in aortic stenosis: Insights from an echo and cardiovascular magnetic resonance study of patients referred for surgical aortic valve replacement. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 1033–1042. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Unit | Mean ± STDEV |
|---|---|---|
| Age | (years) | 37 ± 11 |
| Gender, males/females | (%) | 65/35 |
| BSA | (m2) | 1.8 ± 0.2 |
| BMI | (kg/m2) | 23 ± 4 |
| Heart Rate | (bpm) | 81 ± 14 |
| SBP | (mmHg) | 118 ± 9 |
| DBP | (mmHg) | 68 ± 7 |
| IVSd | (mm) | 8.4 ± 1.6 |
| PWd | (mm) | 8.3 ± 1.5 |
| LVMi | (g/m2) | 68 ± 15 |
| LV EDVi | (mL/m2) | 50 ± 11 |
| LV ESVi | (mL/m2) | 20 ± 5 |
| LV SVi | (mL/m2) | 32 ± 9 |
| LV EF | (%) | 59 ± 5 |
| LV E wave | (cm/s) | 83 ± 17 |
| LV Edt | (ms) | 157 ± 28 |
| LV E/A | 1.6 ± 0.5 | |
| LV s | (cm/s) | 10 ± 2 |
| LV E’ | (cm/s) | 16 ± 4 |
| LV E/E’ | 5.3 ± 1 | |
| LA ESVi | (mL/m2) | 22 ± 6 |
| TAPSE | (cm) | 23 ± 3 |
| RV-EDAi | (cm/m2) | 9 ± 2 |
| RV-ESAi | (cm/m2) | 5 ± 1 |
| FAS | (%) | 45 ± 9 |
| Parameter | Unit | Males (n = 130) | Females (n = 70) |
|---|---|---|---|
| Age | (years) | 35 ± 11 | 37 ± 12 |
| BSA | (m2) | 1.9 ± 0.2 | 1.6 ± 0.2 * |
| BMI | (kg/m2) | 23 ± 4 | 21 ± 3 * |
| Heart Rate | (bpm) | 79 ± 13 | 83 ± 14 |
| SBP | (mmHg) | 119 ± 9 | 116 ± 9 |
| DBP | (mmHg) | 68 ± 7 | 68 ± 8 |
| IVSd | (mm) | 9.0 ± 1.6 | 8.0 ± 1.5 * |
| PWd | (mm) | 9.0 ± 1.5 | 8.0 ± 1.8 * |
| LVMi | (g/m2) | 72 ± 14 | 61 ± 15 * |
| LV EDVi | (mL/m2) | 52 ± 11 | 50 ± 11 |
| LV ESVi | (mL/m2) | 18 ± 4 | 21 ± 6 * |
| LV SVi | (mL/m2) | 31 ± 8 | 32 ± 10 |
| LV EF | (%) | 59 ± 5 | 59 ± 5 |
| LV E wave | (cm/s) | 85 ± 16 | 81 ± 18 |
| LV Edt | (ms) | 156 ± 27 | 159 ± 28 |
| LV E/A | 1.6 ± 0.5 | 1.6 ± 0.5 | |
| LV s | (cm/s) | 9 ± 2 | 10 ± 2 |
| LV E’ | (cm/s) | 16 ± 3 | 15 ± 3 |
| LV E/E’ | 5.5 ± 1 | 5.2 ± 1 | |
| LA ESVi | (mL/m2) | 21 ± 6 | 22 ± 6 |
| TAPSE | (cm) | 22 ± 3 | 22 ± 3 |
| RV-EDAi | (cm/m2) | 9 ± 2 | 9 ± 2 |
| RV-ESAi | (cm/m2) | 5 ± 1 | 5 ± 1 |
| FAS | (%) | 46 ± 7 | 44 ± 9 |
| Layer | Basal | Mid | Apical |
|---|---|---|---|
| Endocardial | −19.3 ± 3.6 | −21.6 ± 3.5 * | −29.8 ± 6.4 *,§ |
| Mid-myocardial | −18.3 ± 3.3 | −19.9 ± 3.2 * | −22.7 ± 5.1 *,§ |
| Epicardial | −17.5 ± 3.4 | −18.3 ± 3.1 * | −17.7 ± 4.4 *,§ |
| Endocardial | Mid-Myocardial | Epicardial | ||||
|---|---|---|---|---|---|---|
| Basal | Mean ± SD | (Max, Min) | Mean ± SD | (Max, Min) | Mean ± SD | (Max, Min) |
| Anterior | −20.3 ± 3.8 | (−30, −11) | −18.9 ± 3.7 | (−28, −10) | −17.8 ± 3.7 | (−28, −9) |
| Anterior septum | −17.4 ± 3.1 | (−26, −10) | −17.0 ± 2.8 | (−25, −10) | −16.6 ± 2.9 | (−25, −9) |
| Inferior septum | −18.3 ± 2.8 | (−25, −12) | −17.7 ± 2.5 | (−23, −11) | −17.1 ± 2.7 | (−24, −10) |
| Inferior | −20.8 ± 3.5 | (−30, −12) | −20.0 ± 3.3 | (−28, −11) | −19.4 ± 3.3 | (−28, −10) |
| Posterior | −19.2 ± 4.0 | (−30, −10) | −18.0 ± 3.7 | (−28, −10) | −16.9 ± 3.9 | (−27, −9) |
| Lateral | −19.6 ± 3.5 | (−28, −11) | −18.2 ± 3.3 | (−26, −10) | −17.0 ± 3.2 | (−25, −8) |
| Mid | ||||||
| Anterior | −21.3 ± 3.6 | (−32, −12) | −19.6 ± 3.4 | (−29, −10) | −18.4 ± 3.2 | (−28, −10) |
| Anterior septum | −22.3 ± 3.9 | (−34, −14) | −20.0 ± 3.1 | (−30, −14) | −18.1 ± 2.8 | (−27, −8) |
| Inferior septum | −21.0 ± 2.9 | (−28, −15) | −19.8 ± 2.8 | (−35, −14) | −18.7 ± 2.5 | (−28, −12) |
| Inferior | −22.3 ± 3.7 | (−32, −12) | −21.1 ± 2.9 | (−29, −14) | −19.7 ± 2.8 | (−28, −12) |
| Posterior | −21.5 ± 3.5 | (−32, −13) | −19.2 ± 3.5 | (−30, −10) | −17.2 ± 3.9 | (−27, −8) |
| Lateral | −21.4 ± 3.2 | (−30, −13) | −19.4 ± 3.0 | (−26, −12) | −17.6 ± 3.1 | (−25, −10) |
| Apical | ||||||
| Anterior | −29.9 ± 6.7 | (−46, −14) | −22.4 ± 5.3 | (−36, −10) | −17.8 ± 4.4 | (−29, −9) |
| Anterior septum | −30.4 ± 6.9 | (−50, −17) | −22.8 ± 5.4 | (−40, −12) | −17.5 ± 4.6 | (−31, −8) |
| Inferior septum | −29.17 ± 6.5 | (−47, −15) | −22.5 ± 5.1 | (−35, −11) | −17.7 ± 4.4 | (−31, −8) |
| Inferior | −31.1 ± 5.5 | (−45, −16) | −24.3 ± 5.0 | (−39, −12) | −19.1 ± 4.5 | (−30, −8) |
| Posterior | −29.2 ± 5.7 | (−46, −15) | −22.3 ± 4.6 | (−36, −12) | −17.5 ± 4.3 | (−30, −8) |
| Lateral | −28.7 ± 6.8 | (−46, −15) | −21.6 ± 5.0 | (−35, −12) | −16.8 ± 4.2 | (−28, −8) |
| Endocardial | Mid-Myocardial | Epicardial | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |
| Inferior septum | −23.0 ± 6.6 | −20.0 ± 4.2 | −17.9 ± 3.4 |
| Lateral | −23.2 ± 6.2 | −19.7 ± 4.1 | −17.1 ± 3.6 |
| Inferior | −24.8 ± 6.3 | −21.8 ± 4.2 | −19.4 ± 3.6 |
| Anterior | −23.6 ± 6.3 | −20.3 ± 4.4 | −18.0 ± 3.8 |
| Posterior | −23.4 ± 6.2 | −19.9 ± 4.4 | −17.2 ± 4.0 |
| Anterior septum | −23.4 ± 7.3 | −19.9 ± 4.6 | −17.4 ± 3.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moraru, L.; Mirea, O.; Toader, D.; Berceanu, M.; Soldea, S.; Munteanu, A.; Donoiu, I.; Raicea, V. Lower Limit of Normality of Segmental Multilayer Longitudinal Strain in Healthy Adult Subjects. J. Cardiovasc. Dev. Dis. 2024, 11, 102. https://doi.org/10.3390/jcdd11040102
Moraru L, Mirea O, Toader D, Berceanu M, Soldea S, Munteanu A, Donoiu I, Raicea V. Lower Limit of Normality of Segmental Multilayer Longitudinal Strain in Healthy Adult Subjects. Journal of Cardiovascular Development and Disease. 2024; 11(4):102. https://doi.org/10.3390/jcdd11040102
Chicago/Turabian StyleMoraru, Liviu, Oana Mirea, Despina Toader, Mihaela Berceanu, Sorina Soldea, Alexandru Munteanu, Ionuț Donoiu, and Victor Raicea. 2024. "Lower Limit of Normality of Segmental Multilayer Longitudinal Strain in Healthy Adult Subjects" Journal of Cardiovascular Development and Disease 11, no. 4: 102. https://doi.org/10.3390/jcdd11040102