
Objective Quantification of Bilateral Bubble Contrast Echocardiography Correlates with Systemic Oxygenation in Patients with Single Ventricle Circulation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
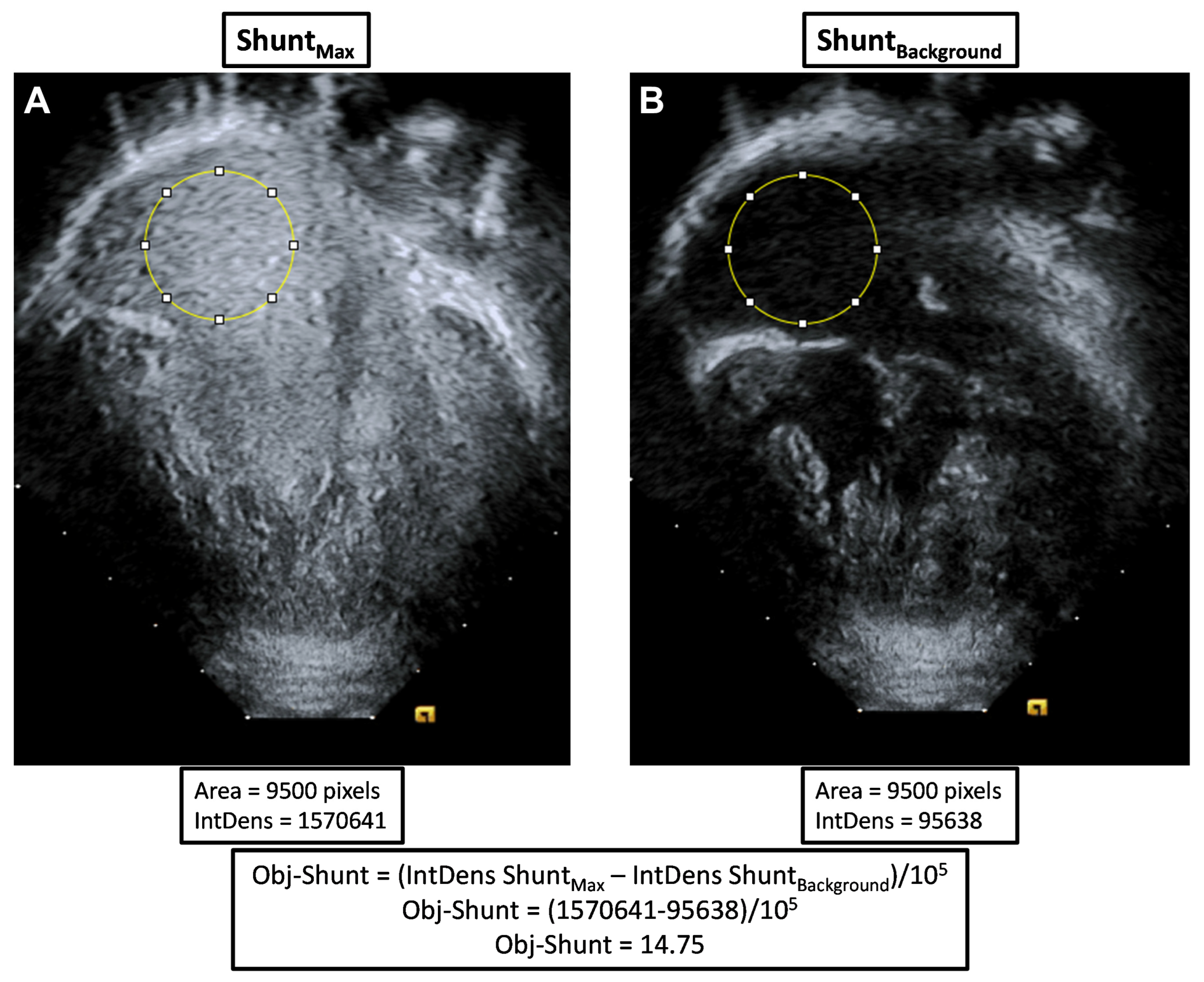
2.2. Bubble Echocardiograms
2.3. Measures of Oxygenation
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
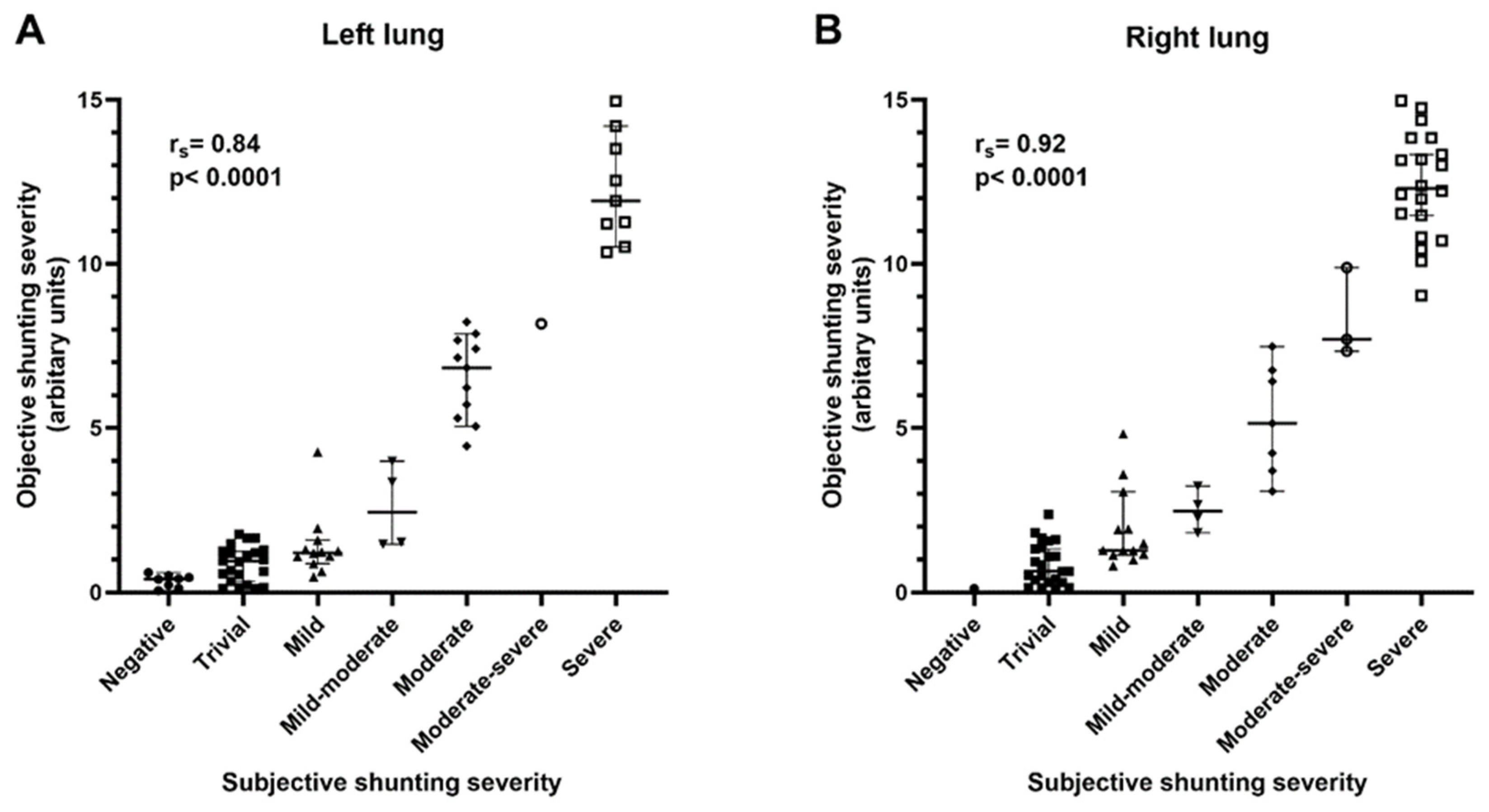
3.2. Objective Quantification of Bubble Echocardiograms
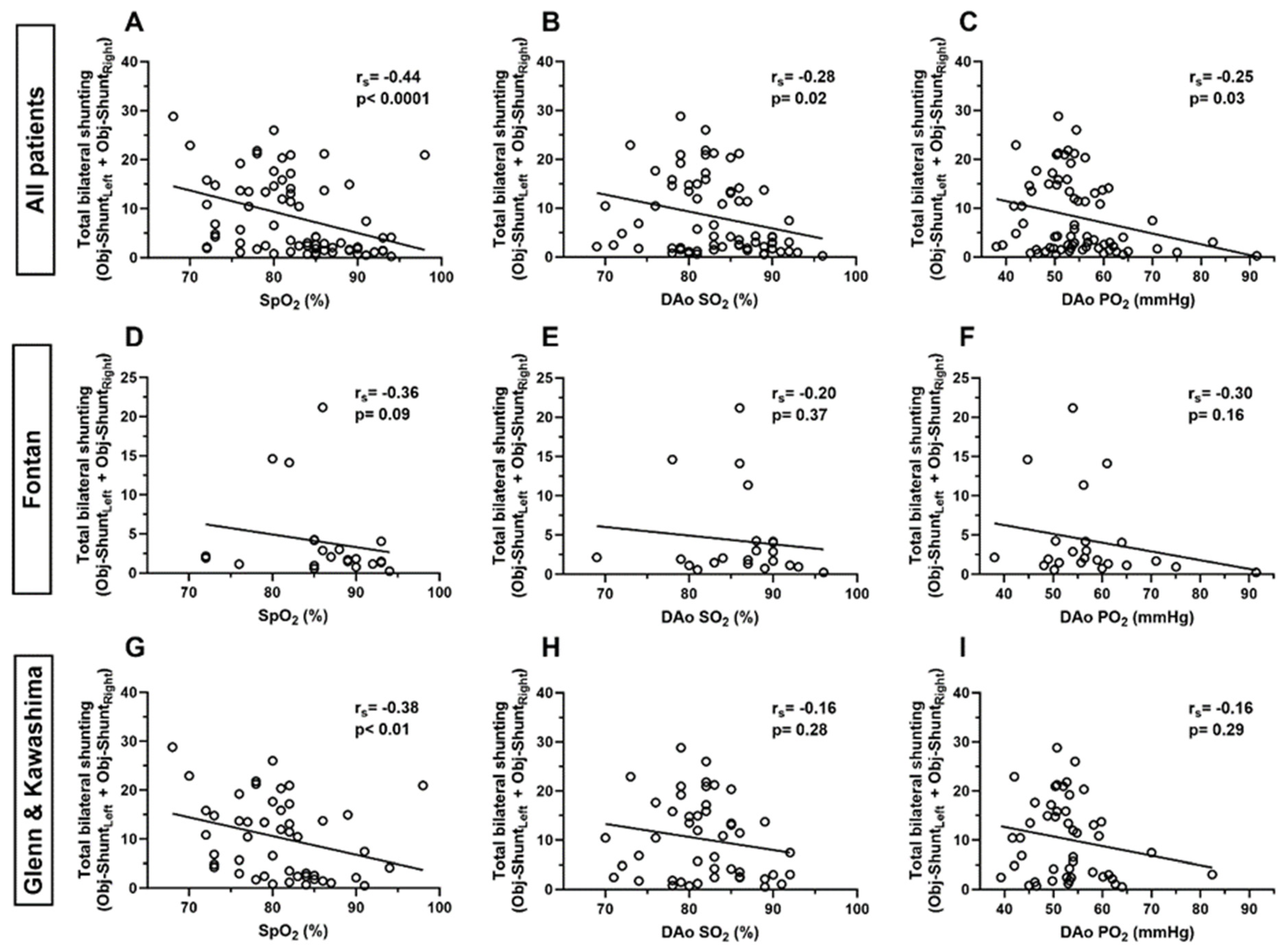
3.3. Correlation of Total Bilateral Intrapulmonary Shunting and Systemic Oxygenation
3.4. Correlation of Unilateral Intrapulmonary Shunting and Pulmonary Vein Oxygenation
3.5. Relationship between Total Intrapulmonary Shunting and Clinical Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bernstein, H.S.; Brook, M.M.; Silverman, N.H.; Bristow, J. Development of pulmonary arteriovenous fistulae in children after cavopulmonary shunt. Circulation 1995, 92, II309–II314. [Google Scholar] [CrossRef]
- Vettukattil, J.J.; Slavik, Z.; Lamb, R.K.; Monro, J.L.; Keeton, B.R.; Tsang, V.T.; Aldous, A.J.; Zivanovic, A.; Johns, S.; Lewington, V.; et al. Intrapulmonary arteriovenous shunting may be a universal phenomenon in patients with the superior cavopulmonary anastomosis: A radionuclide study. Heart 2000, 83, 425–428. [Google Scholar] [CrossRef] [PubMed]
- Mathur, M.; Glenn, W.W.L. Long-term evaluation of cava-pulmonary artery anastomosis. Surgery 1973, 74, 899–916. [Google Scholar] [PubMed]
- McFaul, R.C.; Tajik, A.J.; Mair, D.D.; Danielson, G.K.; Seward, J.B. Development of pulmonary arteriovenous shunt after superior vena cava-right pulmonary artery (Glenn) anastomosis: Report of four cases. Circulation 1977, 55, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Spearman, A.D.; Ginde, S. Pulmonary vascular sequalae of palliated single ventricle circulation: Arteriovenous malformations and aortopulmonary collaterals. J. Cardiovasc. Dev. Dis. 2022, 9, 309. [Google Scholar] [PubMed]
- Velthuis, S.; Buscarini, E.; Gossage, J.R.; Snijder, R.J.; Mager, J.J.; Post, M.C. Clinical implications of pulmonary shunting on saline contrast echocardiography. J. Am. Soc. Echocardiogr. 2015, 28, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.K.R.; Alejos, J.C.; Atkinson, D.; Jensen, R.; Drant, S.; Galindo, A.; Laks, H. Bubble contrast echocardiography in detecting pulmonary arteriovenous shunting in children with univentricular heart after cavopulmonary anastomosis. J. Am. Coll. Cardiol. 1999, 33, 2052–2058. [Google Scholar] [CrossRef] [PubMed]
- Larsson, E.S.; Solymar, L.; Eriksson, B.O.; de Wahl Granelli, A.; Mellander, M. Bubble contrast echocardiography in detecting pulmonary arteriovenous malformations after modified Fontan operations. Cardiol. Young 2001, 11, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, J.A.; Moore, P.; Rosenthal, D.N.; Puchalski, M.; Brook, M.M. Comparison of contrast echocardiography versus cardiac catheterization for detection of pulmonary arteriovenous malformations. Am. J. Cardiol. 2002, 89, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Asada, D.; Morishita, Y.; Kawai, Y.; Kajiyama, Y.; Ikeda, K. Efficacy of bubble contrast echocardiography in detecting pulmonary arteriovenous fistulas in children with univentricular heart after total cavopulmonary connection. Cardiol. Young 2020, 30, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Kartik, S.V.; Sasidharan, B.; Gopalakrishnan, A.; Kurup, H.K.N.; Krishnamoorthy, K.M.; Sasikumar, D.; Thulaseedharan, J.V.; Valaparambil, A.; Tharakan, J. A comparative study of invasive modalities for evaluation of pulmonary arteriovenous fistula after bidirectional Glenn shunt. Pediatr. Cardiol. 2021, 42, 1818–1825. [Google Scholar] [CrossRef] [PubMed]
- Barzilai, B.; Waggoner, A.D.; Spessert, C.; Picus, D.; Goodenberger, D. Two-dimensional contrast echocardiography in the detection and follow-up of congenital pulmonary arteriovenous malformations. Am. J. Cardiol. 1991, 68, 1507–1510. [Google Scholar] [CrossRef] [PubMed]
- Gazzaniga, P.; Buscarini, E.; Leando, G.; Reduzzi, L.; Grosso, M.; Pongiglione, G. Contrast echocardiography for pulmonary arteriovenous malformations screening: Does any bubble matter? Eur. J. Echocardiogr. 2009, 10, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Kroon, S.; Van Thor, M.C.J.; Vorselaars, V.M.M.; Hosman, A.E.; Swaans, M.J.; Snijder, R.J.; Mager, H.J.; Post, M.C. The use of echo density to quantify pulmonary right-to-left shunt in transthoracic contrast echocardiography. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 1190–1196. [Google Scholar] [CrossRef] [PubMed]
- Rantner, B. The correlation coefficient: Its values range between +1/-1, or do they? J. Target. Meas. Anal. Mark. 2009, 17, 139–142. [Google Scholar] [CrossRef]
- Shah, M.J.; Rychik, J.; Fogel, M.A.; Murphy, J.D.; Jacobs, M.L. Pulmonary AV malformations after superior cavopulmonary connection: Resolution after inclusion of hepatic veins in the pulmonary circulation. Ann. Thorac. Surg. 1997, 63, 960–963. [Google Scholar] [CrossRef] [PubMed]
- McElhinney, D.B.; Kreutzer, J.; Lang, P.; Mayer, J.E.; del Nido, P.J.; Lock, J.E. Incorporation of the hepatic veins into the cavopulmonary circulation in patients with heterotaxy and pulmonary arteriovenous malformations after a Kawashima procedure. Ann. Thorac. Surg. 2005, 80, 1597–1603. [Google Scholar] [CrossRef] [PubMed]
- Vollebregt, A.; Pushparajah, K.; Rizvi, M.; Hoschtitzky, A.; Anderson, D.; Austin, C.; Tibby, S.M.; Simpson, J. Outcomes following the Kawashima procedure for single-ventricle palliation in left atrial isomerism. Eur. J. Cardiothorac. Surg. 2012, 41, 574–579. [Google Scholar] [CrossRef]
- Spearman, A.D.; Kindel, S.J.; Woods, R.K.; Ginde, S. Arteriovenous fistula creation for hypoxia after single ventricle palliation: A single-institution experience and literature review. Congenit. Heart Dis. 2019, 14, 1199–1206. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cohort Demographics | n = 72 | |
|---|---|---|
| Age (years) | 12.5 [9.8, 19.1] | |
| Male sex | 41 (56.9) | |
| Primary cardiac diagnosis | AVSD | 19 (26.4) |
| DILV | 12 (16.7) | |
| DORV | 9 (12.5) | |
| HLHS | 27 (37.5) | |
| PA IVS | 1 (1.4) | |
| TA | 4 (5.5) | |
| Heterotaxy | 26 (36.1) | |
| Interrupted IVC | 13 (18.1) | |
| Bilateral Glenn | 15 (20.8) | |
| Major blood group | A | 21 (29.1) |
| B | 12 (16.7) | |
| AB | 1 (1.4) | |
| O | 38 (52.8) | |
| Circulatory stage at catheterization | Glenn | 41 |
| Kawashima | 8 | |
| Fontan | 23 | |
| Duration post-Glenn (years) # | 1.9 [1.2, 2.9] | |
| Duration post-Kawashima (years) $ | 2.6 [1.7, 3.6] | |
| Duration post-Fontan (years) ^ | 11.7 [5.2, 15.8] | |
| Any pulmonary vein data obtained (Glenn circulation only) | 30 (71.4) | |
| Cohort | Oxygen Measurement | Number of Measurements | Correlation Coefficient (rs) | p-Value |
|---|---|---|---|---|
| Glenn | LUPV SO2 | 17 | 0.00 | >0.99 |
| LUPV PO2 | 16 | −0.05 | 0.86 | |
| RUPV SO2 | 19 | 0.07 | 0.76 | |
| RUPV PO2 | 18 | 0.07 | 0.78 | |
| LLPV SO2 | 11 | −0.04 | 0.91 | |
| LLPV PO2 | 11 | −0.20 | 0.56 | |
| RLPV SO2 | 9 | −0.47 | 0.21 | |
| RLPV PO2 | 8 | −0.55 | 0.16 |
| Patient | Objective Shunting Left | Objective Shunting Right | Inhaled Supplemental O2 | LUPV | LLPV | RUPV | RLPV |
|---|---|---|---|---|---|---|---|
| Glenn-1 | 1.30 | 1.14 | 21% | 124 mmHg | 156 mmHg | 121 mmHg | 93 mmHg |
| 99% | 99% | 99% | 96% | ||||
| - | - | - | - | - | |||
| - | - | - | - | ||||
| Glenn-2 | 10.52 | 12.38 | 35% | 229 mmHg | 41 mmHg | - | 43 mmHg |
| 99% | 71% | - | 75% | ||||
| - | - | - | - | - | |||
| - | - | - | - | ||||
| Glenn-3 | 7.41 | 13.84 | 25% | 146 mmHg | 122 mmHg | 138 mmHg | 55 mmHg |
| 99% | 98% | 98% | 86% | ||||
| - | - | - | - | - | |||
| - | - | - | - | ||||
| Glenn-4 | 0.34 | 13.33 | 21% | 96 mmHg | - | - | - |
| 99% | - | - | - | ||||
| 100% | 437 mmHg | - | 461 mmHg | 106 mmHg | |||
| 100% | - | 100% | 96% |
| Cohort | Clinical Variable | p-Value |
|---|---|---|
| All patients (n = 72) | Sex | 0.43 |
| Primary cardiac diagnosis | 0.79 | |
| Heterotaxy | 0.49 | |
| Interrupted IVC | <0.01 | |
| Bilateral BDG | 0.69 | |
| Major blood group | 0.88 | |
| Fontan (n = 23) | Sex | 0.74 |
| Primary cardiac diagnosis | 0.44 | |
| Heterotaxy | 0.60 | |
| Interrupted IVC | 0.08 | |
| Bilateral BDG | 0.66 | |
| Major blood group | 0.74 | |
| Glenn + Kawashima (n = 49) | Sex | 0.35 |
| Primary cardiac diagnosis | 0.36 | |
| Heterotaxy | 0.93 | |
| Interrupted IVC | 0.08 | |
| Bilateral BDG | 0.78 | |
| Major blood group | 0.51 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phimister, A.; Bushee, C.; Merbach, M.; Challa, S.A.; Pan, A.Y.; Spearman, A.D. Objective Quantification of Bilateral Bubble Contrast Echocardiography Correlates with Systemic Oxygenation in Patients with Single Ventricle Circulation. J. Cardiovasc. Dev. Dis. 2024, 11, 84. https://doi.org/10.3390/jcdd11030084
Phimister A, Bushee C, Merbach M, Challa SA, Pan AY, Spearman AD. Objective Quantification of Bilateral Bubble Contrast Echocardiography Correlates with Systemic Oxygenation in Patients with Single Ventricle Circulation. Journal of Cardiovascular Development and Disease. 2024; 11(3):84. https://doi.org/10.3390/jcdd11030084
Chicago/Turabian StylePhimister, Ashley, Chana Bushee, Monica Merbach, Sai Alekha Challa, Amy Y. Pan, and Andrew D. Spearman. 2024. "Objective Quantification of Bilateral Bubble Contrast Echocardiography Correlates with Systemic Oxygenation in Patients with Single Ventricle Circulation" Journal of Cardiovascular Development and Disease 11, no. 3: 84. https://doi.org/10.3390/jcdd11030084