
Concomitant Use of Antiplatelet Agents and Proton-Pump Inhibitors Increases the Risk of Adverse Cardiovascular Events: A Nationwide Population-Based Cohort Study Using Balanced Operational Definitions

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Dataset
2.2. Study Setting and Participants
2.3. Outcome Variables
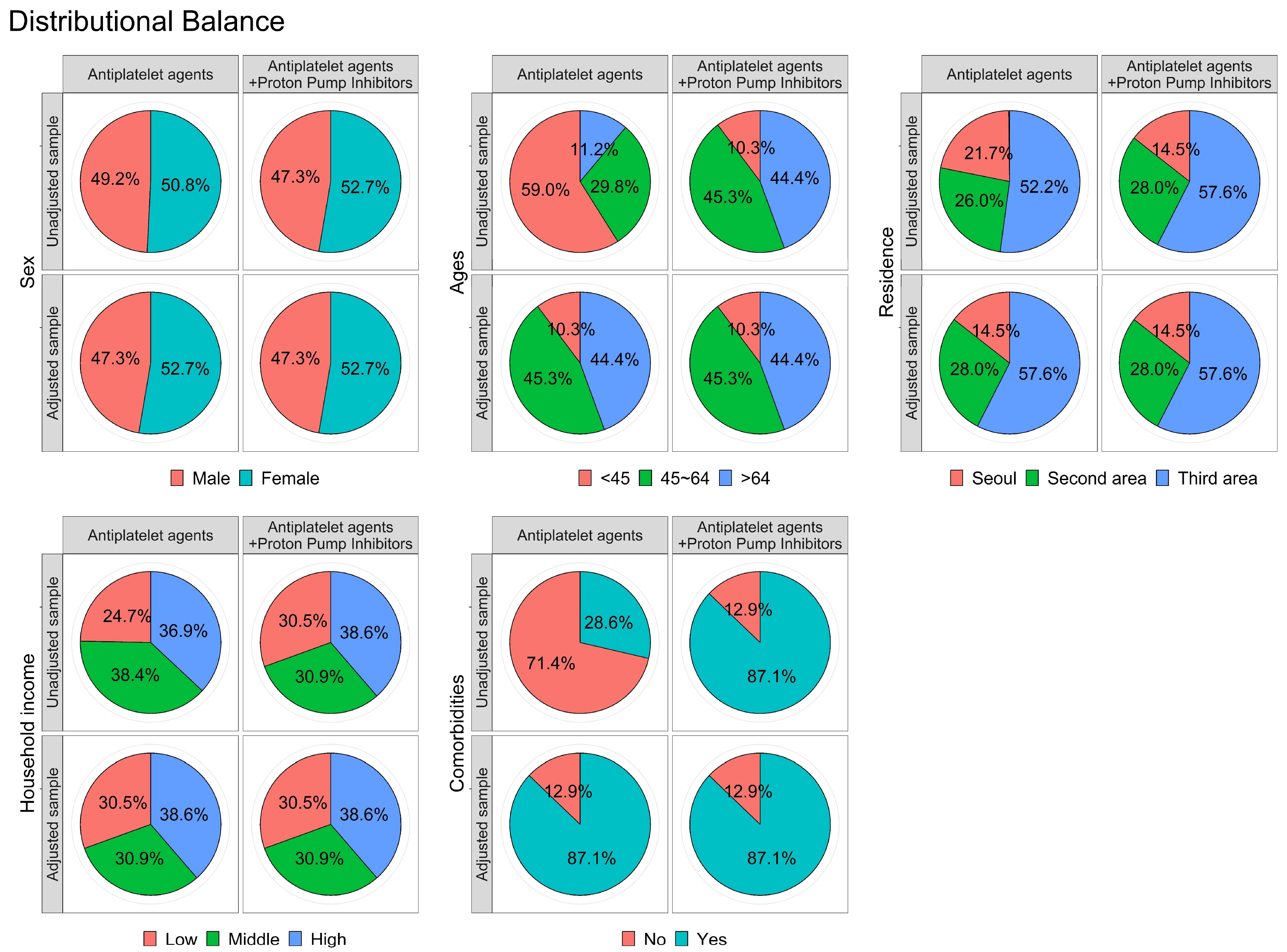
2.4. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Incidence and Risk Ratio
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, D.L.; Scheiman, J.; Abraham, N.S.; Antman, E.M.; Chan, F.K.L.; Furberg, C.D.; Johnson, D.A.; Mahaffey, K.W.; Quigley, E.M. American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents ACCF/ACG/AHA 2008 Expert Consensus Document on Reducing the Gastrointestinal Risks of Antiplatelet Therapy and NSAID Use: A Report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. Circulation 2008, 118, 1894–1909. [Google Scholar] [CrossRef] [Green Version]
- Hallas, J.; Dall, M.; Andries, A.; Andersen, B.S.; Aalykke, C.; Hansen, J.M.; Andersen, M.; Lassen, A.T. Use of single and combined antithrombotic therapy and risk of serious upper gastrointestinal bleeding: Population based case-control study. BMJ 2006, 333, 726. [Google Scholar] [CrossRef] [Green Version]
- Kwok, C.S.; Nijjar, R.S.; Loke, Y.K. Effects of Proton Pump Inhibitors on Adverse Gastrointestinal Events in Patients Receiving Clopidogrel: Systematic Review and Meta-analysis. Drug Saf. 2011, 34, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.W.Y.; Lau, W.; Leung, W.K.; Mok, M.; He, Y.; Tong, T.S.; Wong, I.C. Prevention of Dabigatran-Related Gastrointestinal Bleeding with Gastroprotective Agents: A Population-Based Study. Gastroenterology 2015, 149, 586–595.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ray, W.A.; Chung, C.P.; Murray, K.T.; Smalley, W.E.; Daugherty, J.R.; Dupont, W.D.; Stein, C.M. Association of Oral Anticoagulants and Proton Pump Inhibitor Cotherapy with Hospitalization for Upper Gastrointestinal Tract Bleeding. JAMA 2018, 320, 2221–2230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moayyedi, P.; Eikelboom, J.W.; Bosch, J.; Connolly, S.J.; Dyal, L.; Shestakovska, O.; Leong, D.; Anand, S.S.; Störk, S.; Branch, K.R.; et al. Pantoprazole to Prevent Gastroduodenal Events in Patients Receiving Rivaroxaban and/or Aspirin in a Randomized, Double-Blind, Placebo-Controlled Trial. Gastroenterology 2019, 157, 403–412.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, K.C.; Lam, S.K.; Chu, K.M.; Wong, B.C.; Hui, W.M.; Hu, W.H.; Lau, G.K.; Wong, W.M.; Yuen, M.F.; Chan, A.O.; et al. Lansoprazole for the Prevention of Recurrences of Ulcer Complications from Long-Term Low-Dose Aspirin Use. N. Engl. J. Med. 2002, 346, 2033–2038. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, D.L.; Scheiman, J.; Abraham, N.S.; Antman, E.M.; Chan, F.K.; Furberg, C.D.; Johnson, D.A.; Mahaffey, K.W.; Quigley, E.M.; Harrington, R.A.; et al. ACCF/ACG/AHA 2008 Expert Consensus Document on Reducing the Gastrointestinal Risks of Antiplatelet Therapy and NSAID Use: A Report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. J. Am. Coll. Cardiol. 2008, 52, 1502–1517. [Google Scholar] [CrossRef] [Green Version]
- Serbin, M.A.; Guzauskas, G.F.; Veenstra, D.L. Clopidogrel-Proton Pump Inhibitor Drug-Drug Interaction and Risk of Adverse Clinical Outcomes Among PCI-Treated ACS Patients: A Meta-analysis. J. Manag. Care Spec. Pharm. 2016, 22, 939–947. [Google Scholar] [CrossRef] [PubMed]
- Bhurke, S.M.; Martin, B.C.; Li, C.; Franks, A.M.; Bursac, Z.; Said, Q. Effect of the Clopidogrel-Proton Pump Inhibitor Drug Interaction on Adverse Cardiovascular Events in Patients with Acute Coronary Syndrome. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2012, 32, 809–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chua, D.; Shalansky, S.J.; Legal, M.G.; Jung, J. Conflicting Evidence Surrounding the Clopidogrel and Proton Pump Inhibitor Drug Interaction. Arch. Intern. Med. 2010, 170, 1501–1510. [Google Scholar] [CrossRef]
- Wu, W.; Liu, J.; Yu, H.; Jiang, Z. Antiplatelet therapy with or without PPIs for the secondary prevention of cardiovascular diseases in patients at high risk of upper gastrointestinal bleeding: A systematic review and meta-analysis. Exp. Ther. Med. 2020, 19, 3595–3603. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, J.S.; Park, S.-H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service–National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef] [Green Version]
- Rassen, J.A.; Shelat, A.A.; Myers, J.; Glynn, R.J.; Rothman, K.J.; Schneeweiss, S. One-to-many propensity score matching in cohort studies. Pharmacoepidemiol. Drug Saf. 2012, 21, 69–80. [Google Scholar] [CrossRef]
- Massel, D.; Little, S.H. Risks and benefits of adding anti-platelet therapy to warfarin among patients with prosthetic heart valves: A meta-analysis. J. Am. Coll. Cardiol. 2001, 37, 569–578. [Google Scholar] [CrossRef] [Green Version]
- Steinhubl, S.R.; Berger, P.B.; Mann, J.T.M., III; Fry, E.T.A.; Delago, A.; Wilmer, C.; Topol, E.; for the CREDO Investigators. Early and Sustained Dual Oral Antiplatelet Therapy Following Percutaneous Coronary Intervention: A Randomized Controlled Trial. JAMA 2002, 288, 2411–2420. [Google Scholar] [CrossRef] [Green Version]
- Van Es, R.F.; Jonker, J.J.; Verheugt, F.W.; Deckers, J.W.; Grobbee, D.E. Aspirin and coumadin after acute coronary syndromes (the ASPECT-2 study): A randomised controlled trial. Lancet 2002, 360, 109–113. [Google Scholar] [CrossRef]
- Hurlen, M.; Abdelnoor, M.; Smith, P.; Erikssen, J.; Arnesen, H. Warfarin, Aspirin, or Both After Myocardial Infarction. N. Engl. J. Med. 2002, 347, 969–974. [Google Scholar] [CrossRef]
- Farrell, B.; Godwin, J.; Richards, S.; Warlow, C. The United Kingdom transient ischaemic attack (UK-TIA) aspirin trial: Final results. J. Neurol. Neurosurg. Psychiatry 1991, 54, 1044–1054. [Google Scholar] [CrossRef]
- Dutch TIA Trial Study Group; van Gijn, J.; Algra, A.; Kappelle, J.; Koudstaal, P.J.; van Latum, A. A Comparison of Two Doses of Aspirin (30 mg vs. 283 mg a Day) in Patients after a Transient Ischemic Attack or Minor Ischemic Stroke. N. Engl. J. Med. 1991, 325, 1261–1266. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Andersson, T.B.; Ahlström, M.; Weidolf, L. Comparison of inhibitory effects of the proton pump-inhibiting drugs omeprazole, esomeprazole, lansoprazole, pantoprazole, and rabeprazole on human cytochrome p450 activities. Drug Metab. Dispos. 2004, 32, 821–827. [Google Scholar] [CrossRef]
- Zvyaga, T.; Chang, S.-Y.; Chen, C.; Yang, Z.; Vuppugalla, R.; Hurley, J.; Thorndike, D.; Wagner, A.; Chimalakonda, A.; Rodrigues, A.D. Evaluation of Six Proton Pump Inhibitors as Inhibitors of Various Human Cytochromes P450: Focus on Cytochrome P450 2C19. Drug Metab. Dispos. 2012, 40, 1698–1711. [Google Scholar] [CrossRef] [Green Version]
- Ma, T.K.; Lam, Y.-Y.; Tan, V.P.; Kiernan, T.J.; Yan, B.P. Impact of genetic and acquired alteration in cytochrome P450 system on pharmacologic and clinical response to clopidogrel. Pharmacol. Ther. 2010, 125, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Morath, T.; Stegherr, J.; Braun, S.; Vogt, W.; Hadamitzky, M.; Schömig, A.; Kastrati, A.; von Beckerath, N.; Sibbing, D. Impact of proton pump inhibitors on the antiplatelet effects of clopidogrel. Thromb. Haemost. 2009, 101, 714–719. [Google Scholar] [CrossRef] [Green Version]
- Ogilvie, B.W.; Yerino, P.; Kazmi, F.; Buckley, D.B.; Rostami-Hodjegan, A.; Paris, B.L.; Toren, P.; Parkinson, A. The Proton Pump Inhibitor, Omeprazole, but Not Lansoprazole or Pantoprazole, Is a Metabolism-Dependent Inhibitor of CYP2C19: Implications for Coadministration with Clopidogrel. Drug Metab. Dispos. 2011, 39, 2020–2033. [Google Scholar] [CrossRef] [Green Version]
- Cuisset, T.; Frere, C.; Quilici, J.; Poyet, R.; Gaborit, B.; Bali, L.; Brissy, O.; Morange, P.-E.; Alessi, M.-C.; Bonnet, J.-L. Comparison of Omeprazole and Pantoprazole Influence on a High 150-mg Clopidogrel Maintenance Dose: The PACA (Proton Pump Inhibitors and Clopidogrel Association) Prospective Randomized Study. J. Am. Coll. Cardiol. 2009, 54, 1149–1153. [Google Scholar] [CrossRef] [Green Version]
- Bundhun, P.K.; Teeluck, A.R.; Bhurtu, A.; Huang, W.-Q. Is the concomitant use of clopidogrel and Proton Pump Inhibitors still associated with increased adverse cardiovascular outcomes following coronary angioplasty? A systematic review and meta-analysis of recently published studies (2012–2016). BMC Cardiovasc. Disord. 2017, 17, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, Y.-W.; Wen, Y.-W.; Huang, W.-F.; Chen, P.-F.; Kuo, K.N.; Hsiao, F.-Y. Cardiovascular and gastrointestinal events of three antiplatelet therapies: Clopidogrel, clopidogrel plus proton-pump inhibitors, and aspirin plus proton-pump inhibitors in patients with previous gastrointestinal bleeding. J. Gastroenterol. 2010, 46, 39–45. [Google Scholar] [CrossRef]
- Hsiao, F.-Y.; Tsai, Y.-W.; Huang, W.-F.; Wen, Y.-W.; Chen, P.-F.; Chang, P.-Y.; Kuo, K.N. A comparison of aspirin and clopidogrel with or without proton pump inhibitors for the secondary prevention of cardiovascular events in patients at high risk for gastrointestinal bleeding. Clin. Ther. 2009, 31, 2038–2047. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, F.-Y.; Mullins, C.D.; Wen, Y.-W.; Huang, W.-F.; Chen, P.-F.; Tsai, Y.-W. Relationship between cardiovascular outcomes and proton pump inhibitor use in patients receiving dual antiplatelet therapy after acute coronary syndrome. Pharmacoepidemiol. Drug Saf. 2011, 20, 1043–1049. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Antiplatelet Agents (Clopidogrel) (n = 1244) | Antiplatelet Agents and Proton-Pump Inhibitors (n = 311) | p-Value |
|---|---|---|---|
| Sex | 1.000 | ||
| Male | 588 (47.3%) | 147 (47.3%) | |
| Female | 656 (52.7%) | 164 (52.7%) | |
| Ages (years) | 1.000 | ||
| <45 | 128 (10.3%) | 32 (10.3%) | |
| 45–64 | 564 (45.3%) | 141 (45.3%) | |
| >64 | 552 (44.4%) | 138 (44.4%) | |
| Residence | 1.000 | ||
| Seoul | 180 (14.5%) | 45 (14.5%) | |
| Second area | 348 (28.0%) | 87 (28.0%) | |
| Third area | 716 (57.6%) | 179 (57.6%) | |
| Household income | 1.000 | ||
| Low (0–30%) | 380 (30.5%) | 95 (30.5%) | |
| Mid (30–70%) | 384 (30.9%) | 96 (30.9%) | |
| High (70–100%) | 480 (38.6%) | 120 (38.6%) | |
| Comorbidities | 1.000 | ||
| No | 160 (12.9%) | 40 (12.9%) | |
| Yes | 1084 (87.1%) | 271 (87.1%) | |
| Hypertension | 0.106 | ||
| No | 347 (27.9%) | 72 (23.2%) | |
| Yes | 897 (72.1%) | 239 (76.8%) | |
| Type 2 diabetes | 0.005 | ||
| No | 794 (63.8%) | 171 (55.0%) | |
| Yes | 450 (36.2%) | 140 (45.0%) | |
| Chronic kidney disease | <0.001 | ||
| No | 1212 (97.4%) | 288 (92.6%) | |
| Yes | 32 (2.6%) | 23 (7.4%) | |
| Variables | n | Case | Person/Year | Incidence | Unadjusted HR (95% CI) | Adjusted HR (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|
| Total Death | |||||||
| Antiplatelet agent (clopidogrel) | 1244 | 163 | 8820.1 | 18.48 | 1.00 (ref) | 1.00 (ref) | |
| Antiplatelet agents and proton-pump inhibitors | 311 | 58 | 1814.1 | 31.97 | 1.68 (1.25–2.28) *** | 1.77 (1.30–2.40) *** | <0.001 |
| Myocardial Infarction | |||||||
| Antiplatelet agent (clopidogrel) | 1244 | 10 | 8798.9 | 1.14 | 1.00 (ref) | 1.00 (ref) | |
| Antiplatelet agents and proton-pump inhibitors | 311 | 8 | 1795.6 | 4.46 | 3.77 (1.47–9.63) ** | 3.52 (1.34–9.22) * | 0.010 |
| Coronary Revascularization | |||||||
| Antiplatelet agent (clopidogrel) | 1244 | 12 | 8798.1 | 1.36 | 1.00 (ref) | 1.00 (ref) | |
| Antiplatelet agents and proton-pump inhibitors | 311 | 12 | 1780.7 | 6.74 | 5.53 (2.45–12.45) *** | 4.74 (2.03–11.05) *** | <0.001 |
| Total Deaths | Myocardial Infarction | Coronary Revascularization | |
|---|---|---|---|
| Event | 221 | 18 | 24 |
| Antiplatelet agent (clopidogrel) | 163 | 10 | 12 |
| Antiplatelet agents and proton-pump inhibitors | 58 | 8 | 12 |
| Total censored (no event) | 1334 | 1537 | 1531 |
| Antiplatelet agent (clopidogrel) | 1081 | 1234 | 1232 |
| Antiplatelet agents and proton-pump inhibitors | 253 | 303 | 299 |
| Termination of study | 1270 | 1260 | 1248 |
| Antiplatelet agent (clopidogrel) | 1031 | 1025 | 1020 |
| Antiplatelet agents and proton-pump inhibitors | 239 | 235 | 228 |
| Loss to follow-up/drop-out | 64 | 277 | 283 |
| Antiplatelet agent (clopidogrel) | 50 | 209 | 212 |
| Antiplatelet agents and proton-pump inhibitors | 14 | 68 | 71 |
| Ages | <45 | 45–64 | >64 | |||
|---|---|---|---|---|---|---|
| Antiplatelet Agent (Clopidogrel) | Antiplatelet Agents and Proton-Pump Inhibitors | Antiplatelet Agent (Clopidogrel) | Antiplatelet Agents and Proton-Pump Inhibitors | Antiplatelet Agent (Clopidogrel) | Antiplatelet Agents and Proton-Pump Inhibitors | |
| Total Deaths | ||||||
| Unadjusted HR (95% CI) | 1.00 (ref) | - | 1.00 (ref) | 2.28 (1.10–4.70) * | 1.00 (ref) | 1.75 (1.25–2.44) ** |
| Adjusted HR (95% CI) | 1.00 (ref) | - | 1.00 (ref) | 2.08 (0.97–4.46) | 1.00 (ref) | 1.77 (1.26–2.49) *** |
| Myocardial Infarction | ||||||
| Unadjusted HR (95% CI) | 1.00 (ref) | - | 1.00 (ref) | 25.01 (2.64–237.30) ** | 1.00 (ref) | 2.02 (1.62–6.57) * |
| Adjusted HR (95% CI) | 1.00 (ref) | - | 1.00 (ref) | 16.79 (1.81–156.10) * | 1.00 (ref) | 2.09 (1.63–6.89) * |
| Coronary Revascularization | ||||||
| Unadjusted HR (95% CI) | 1.00 (ref) | - | 1.00 (ref) | 17.12 (4.52–64.88) *** | 1.00 (ref) | 1.95 (1.52–7.31) * |
| Adjusted HR (95% CI) | 1.00 (ref) | - | 1.00 (ref) | 13.64 (3.41–54.51) *** | 1.00 (ref) | 1.74 (1.45–6.72) * |
| Time (Year) | Myocardial Infarction | Coronary Revascularization |
|---|---|---|
| Adjusted HR (95% CI) | Adjusted HR (95% CI) | |
| 1 | 3.56 (0.32–39.47) | No events |
| 2 | 4.16 (0.98–17.63) | 9.44 (1.51–59.03) * |
| 3 | 6.02 (1.86–19.51) ** | 15.33 (3.08–76.34) *** |
| 4 | 3.69 (1.31–10.43) * | 7.35 (2.07–26.07) ** |
| 5 | 3.69 (1.31–10.43) * | 5.54 (1.87–16.36) ** |
| 6 | 3.69 (1.31–10.43) * | 4.45 (1.55–12.76) ** |
| 7 | 3.17 (1.18–8.52) * | 4.65 (1.83–11.87) ** |
| 8 | 3.17 (1.18–8.52) * | 4.61 (1.93–11.01) *** |
| 9 | 3.17 (1.18–8.52) * | 4.46 (1.90–10.50) *** |
| 10 | 3.52 (1.34–9.22) * | 4.74 (2.03–11.05) *** |
| 11 | 3.52 (1.34–9.22) * | 4.74 (2.03–11.05) *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, H.G.; Kim, D.-K. Concomitant Use of Antiplatelet Agents and Proton-Pump Inhibitors Increases the Risk of Adverse Cardiovascular Events: A Nationwide Population-Based Cohort Study Using Balanced Operational Definitions. J. Cardiovasc. Dev. Dis. 2023, 10, 264. https://doi.org/10.3390/jcdd10060264
Yang HG, Kim D-K. Concomitant Use of Antiplatelet Agents and Proton-Pump Inhibitors Increases the Risk of Adverse Cardiovascular Events: A Nationwide Population-Based Cohort Study Using Balanced Operational Definitions. Journal of Cardiovascular Development and Disease. 2023; 10(6):264. https://doi.org/10.3390/jcdd10060264
Chicago/Turabian StyleYang, Hee Gyu, and Dong-Kyu Kim. 2023. "Concomitant Use of Antiplatelet Agents and Proton-Pump Inhibitors Increases the Risk of Adverse Cardiovascular Events: A Nationwide Population-Based Cohort Study Using Balanced Operational Definitions" Journal of Cardiovascular Development and Disease 10, no. 6: 264. https://doi.org/10.3390/jcdd10060264