
The Use of the Cryopreserved Aortic Homograft for Aortic Valve Replacement: Is It Still an Option?
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Oversight, Patient Population, Definitions, and Endpoints
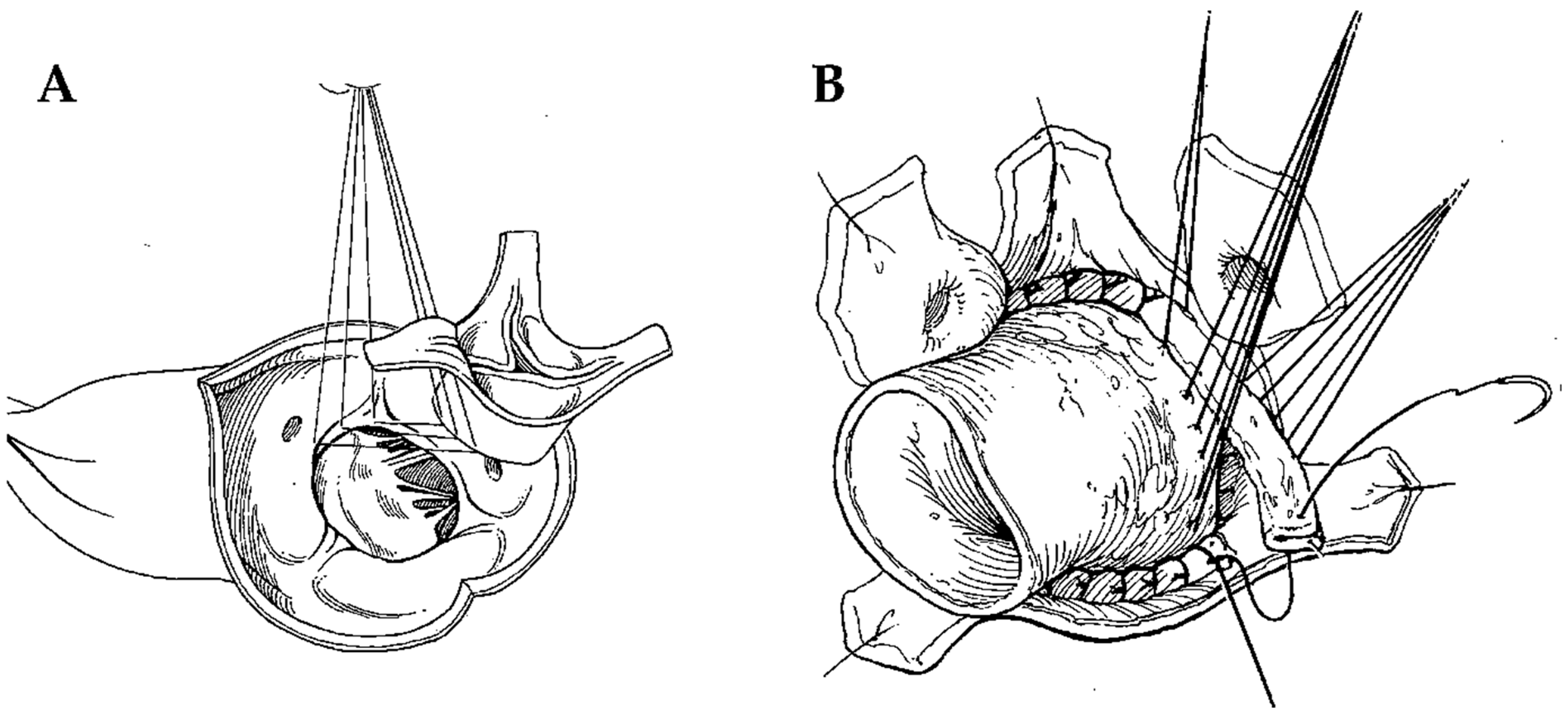
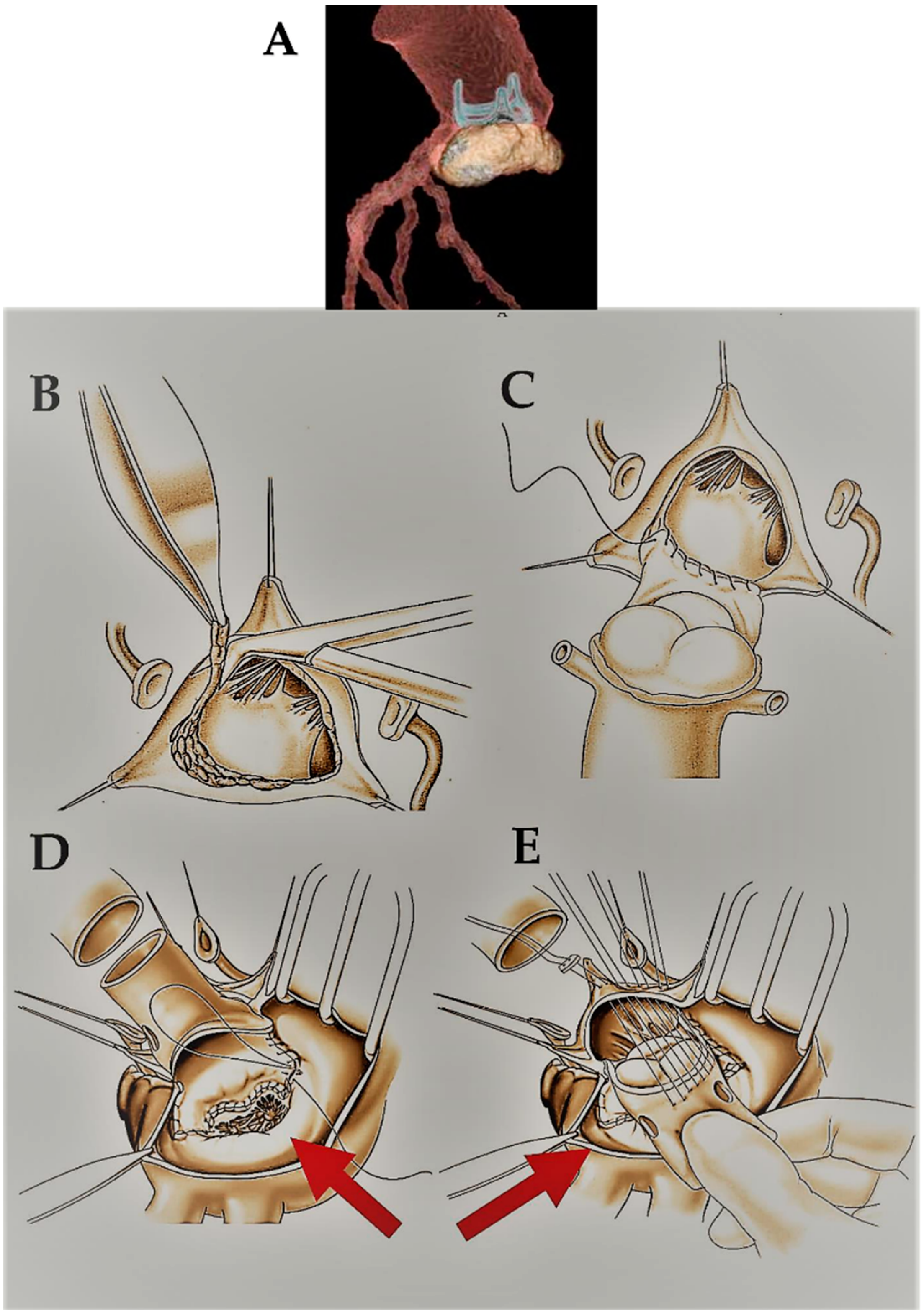
2.2. Surgical Technique
2.3. Clinical Follow-Up
2.4. Echocardiography
2.5. Structural Valve Degeneration
2.6. Statistical Analysis
3. Results
3.1. Patients and Surgical Data
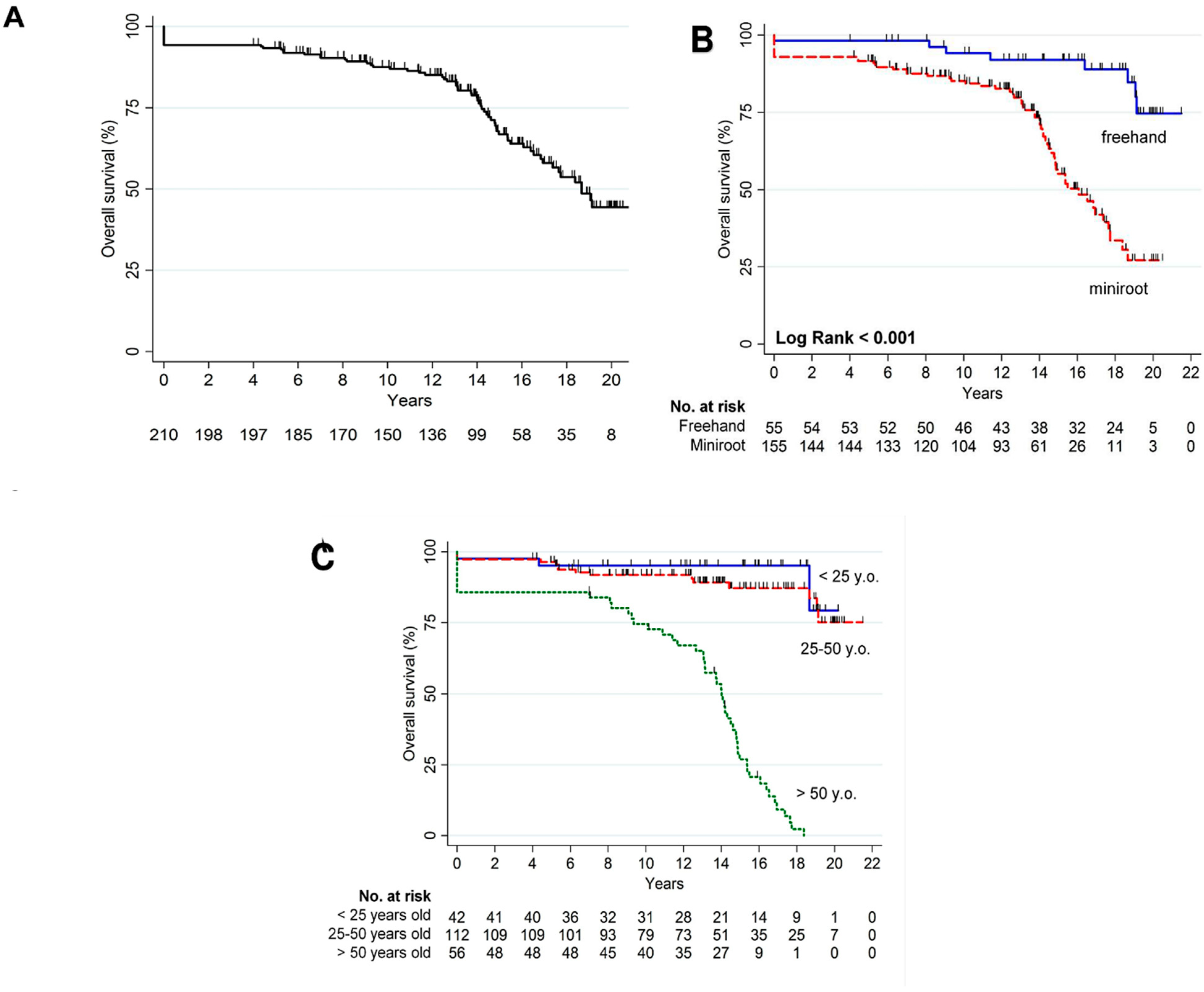
3.2. Overall Mortality
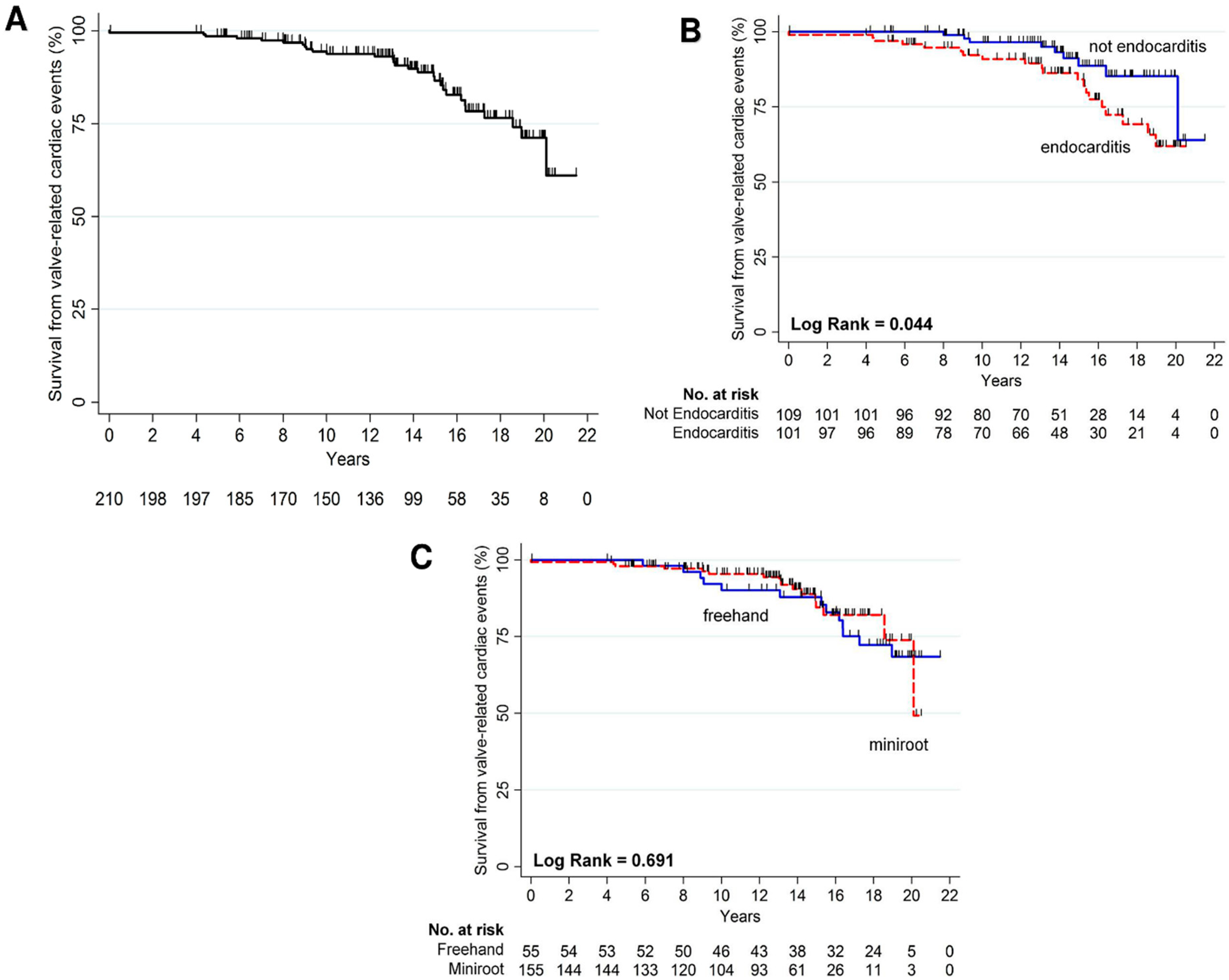
3.3. Cardiac Mortality Related to Structural Valve Degeneration
3.4. Structural Valve Degeneration
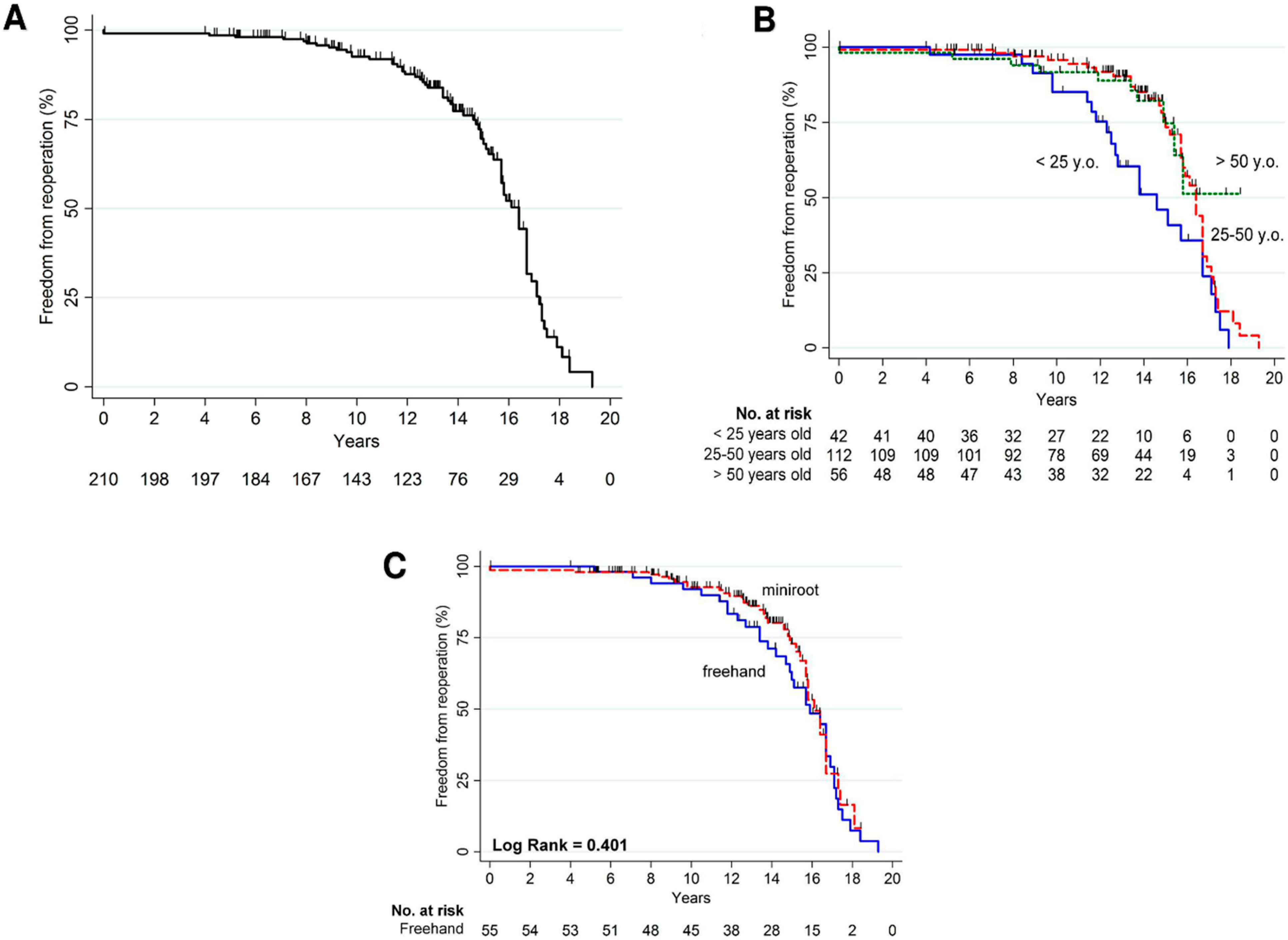
3.5. Reoperation
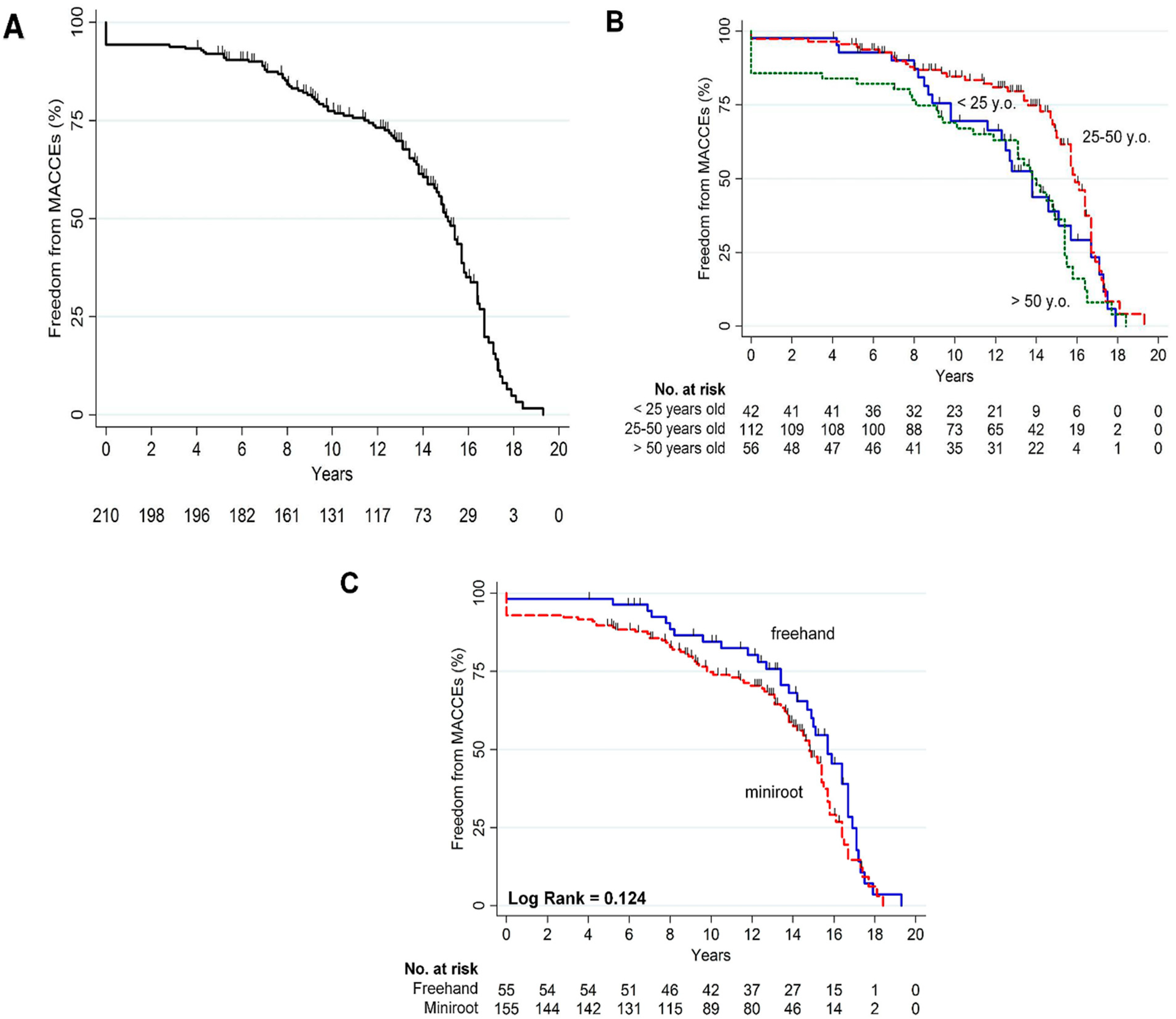
3.6. Composite Cardiac End Point and Echocardiographic Data
3.7. Outcomes in Childbearing Age
4. Discussion
5. Limitations
6. Conclusions
7. Perspectives
7.1. Competency in Medical Knowledge
7.2. Competency in Patient Care
7.3. Translational Outlook
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AUC | area under the ROC curve |
| CAH | cryopreserved aortic homograft |
| MACCEs | major adverse cardiac and cerebrovascular events |
| NYHA | New York Heart Association |
| SVD | structural valve degeneration |
References
- Witten, J.C.; Houghtaling, P.L.; Shrestha, N.K.; Gordon, S.M.; Jaber, W.; Blackstone, E.H.; Pettersson, G.B.; Durbak, E.; Hussain, S.T.; Unai, S.; et al. Aortic allograft infection risk. J. Thorac. Cardiovasc. Surg. 2023, 165, 1303–1315.e9. [Google Scholar]
- Fukushima, S.; Tesar, P.J.; Pearse, B.; Jalali, H.; Sparks, L.; Fraser, J.F.; Pohlner, P.G. Long-term clinical outcomes after aortic valve replacement using cryopreserved aortic allograft. J. Thorac. Cardiovasc. Surg. 2014, 148, 65–72.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romeo, J.L.; Takkenberg, J.J.; Roos-Hesselink, J.W.; Hanif, M.; Cornette, J.M.; van Leeuwen, W.J.; van Dijk, A.; Bogers, A.J.; Mokhles, M.M. Outcomes of Pregnancy After Right Ventricular Outflow Tract Reconstruction with an Allograft Conduit. J. Am. Coll. Cardiol. 2018, 71, 2656–2665. [Google Scholar] [CrossRef] [PubMed]
- Arabkhani, B.; Bekkers, J.A.; Andrinopoulou, E.-R.; Roos-Hesselink, J.W.; Takkenberg, J.J.; Bogers, A.J. Allografts in aortic position: Insights from a 27-year, single-center prospective study. J. Thorac. Cardiovasc. Surg. 2016, 152, 1572–1579.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jassar, A.S.; Bavaria, J.E.; Szeto, W.Y.; Moeller, P.J.; Maniaci, J.; Milewski, R.K.; Gorman, J.H., III; Desai, N.D.; Gorman, R.C.; Pochettino, A. Graft selection for aortic root replacement in complex active endocarditis: Does it matter? Ann. Thorac. Surg. 2012, 93, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Musci, M.; Weng, Y.; Hübler, M.; Amiri, A.; Pasic, M.; Kosky, S.; Stein, J.; Siniawski, H.; Hetzer, R. Homograft aortic root replacement in native or prosthetic active infective endocarditis: Twenty-year single-center experience. J. Thorac. Cardiovasc. Surg. 2010, 139, 665–673. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.B.; Ejiofor, J.I.; Yammine, M.; Camuso, J.M.; Walsh, C.W.; Ando, M.; Melnitchouk, S.I.; Rawn, J.D.; Leacche, M.; MacGillivray, T.E.; et al. Are homografts superior to conventional prosthetic valves in the setting of infective endocarditis involving the aortic valve? J. Thorac. Cardiovasc. Surg. 2016, 151, 1239–1248.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nappi, F.; Nenna, A.; Petitti, T.; Spadaccio, C.; Gambardella, I.; Lusini, M.; Chello, M.; Acar, C. Long-term outcome of cryopreserved allograft for aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2018, 156, 1357–1365.e6. [Google Scholar] [CrossRef]
- Kowert, A.; Vogt, F.; Beiras-Fernandez, A.; Reichart, B.; Kilian, E. Outcome after homograft redo operation in aortic position. Eur. J. Cardio-Thorac. Surg. 2012, 41, 404–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, D.R.; Soltesz, E.G.; Vakil, N.; Rajeswaran, J.; Roselli, E.E.; Sabik, J.F.; Smedira, N.G.; Svensson, L.G.; Lytle, B.W.; Blackstone, E.H. Long-Term Durability of Bioprosthetic Aortic Valves: Implications from 12,569 Implants. Ann. Thorac. Surg. 2015, 99, 1239–1247. [Google Scholar] [CrossRef] [Green Version]
- Bourguignon, T.; Bouquiaux-Stablo, A.-L.; Candolfi, P.; Mirza, A.; Loardi, C.; May, M.-A.; El-Khoury, R.; Marchand, M.; Aupart, M. Very Long-Term Outcomes of the Carpentier-Edwards Perimount Valve in Aortic Position. Ann. Thorac. Surg. 2015, 99, 831–837. [Google Scholar] [CrossRef]
- Flameng, W.; Herregods, M.C.; Vercalsteren, M.; Herijgers, P.; Bogaerts, K.; Meuris, B. Prosthesis-patient mismatch predicts structural valve degeneration in bio-prosthetic heart valves. Circulation 2010, 121, 2123–2129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palka, P.; Harrocks, S.; Lange, A.; Burstow, D.; O’brien, M. Primary aortic valve replacement with cryopreserved aortic allograft. An echocardiographic follow-up study of 570 patients. ACC Curr. J. Rev. 2002, 105, 61–66. [Google Scholar] [CrossRef]
- Folesani, G.; Calcara, G.; Minniti, G.; Polesel, E. Reoperation for aortic homograft failure using an Edwards Intuity valve. Interact. Cardiovasc. Thorac. Surg. 2016, 22, 378–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danesi, T.H.; Minniti, G.; Cresce, G.D.; Favaro, A.; Magagna, P.; Auriemma, S.; Micciolo, M.; Mirone, S.; Polesel, E.; Salvador, L. Redo after Failure of Aortic Homografts with a Rapid Deployment Valve. Ann. Thorac. Surg. 2016, 102, e281–e282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kieffer, E.; Bahnini, A.; Koskas, F.; Ruotolo, C.; Le Blevec, D.; Plissonnier, D. In situ allograft replacement of infected infrarenal aortic prosthetic grafts: Results in forty-three patients. J. Vasc. Surg. 1993, 17, 349–355; discussion 55–56. [Google Scholar] [CrossRef] [Green Version]
- Nappi, F.; Spadaccio, C.; Acar, C. Use of allogeneic tissue to treat infective valvular disease: Has everything been said? J. Thorac. Cardiovasc. Surg. 2017, 153, 824–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- David, T.E.; Regesta, T.; Gavra, G.; Armstrong, S.; Maganti, M.D. Surgical treatment of paravalvular abscess: Long-term results. Eur. J. Cardio-Thorac. Surg. 2007, 31, 43–48. [Google Scholar] [CrossRef]
- Hussain, S.T.; Blackstone, E.H.; Gordon, S.M.; Griffin, B.; LeMaire, S.A.; Woc-Colburn, L.E.; Coselli, J.S.; Pettersson, G.B. Randomized clinical trials of surgery for infective endocarditis: Reality versus expectations! J. Thorac. Cardiovasc. Surg. 2018, 155, 74–75.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lytle, B.W.; Sabik, J.F.; Blackstone, E.H.; Svensson, L.G.; Pettersson, G.B.; Cosgrove, D.M. Reoperative cryopreserved root and ascending aorta replacement for acute aortic prosthetic valve endocarditis. Ann. Thorac. Surg. 2002, 74, S1754–S1757. [Google Scholar] [CrossRef] [PubMed]
- Navia, J.L.; Elgharably, H.; Hakim, A.H.; Witten, J.C.; Haupt, M.J.; Germano, E.; Houghtaling, P.L.; Bakaeen, F.G.; Pettersson, G.B.; Lytle, B.W.; et al. Long-term Outcomes of Surgery for Invasive Valvular Endocarditis Involving the Aortomitral Fibrosa. Ann. Thorac. Surg. 2019, 108, 1314–1323. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Acar, C. Monobloc or Separate Aortic and Mitral Homografts for Endocarditis of the Intervalvular Fibrosa? Ann. Thorac. Surg. 2021, 112, 1382–1383. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Spadaccio, C.; Dreyfus, J.; Attias, D.; Acar, C.; Bando, K. Mitral endocarditis: A new management framework. J. Thorac. Cardiovasc. Surg. 2018, 156, 1486–1495.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirklin, J.K. Challenging homografts as the holy grail for aortic valve endocarditis. J. Thorac. Cardiovasc. Surg. 2016, 151, 1230–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nappi, F.; Singh, S.S.A.; Spadaccio, C.; Acar, C. Revisiting the guidelines and choice the ideal substitute for aortic valve endocarditis. Ann. Transl. Med. 2020, 8, 952. [Google Scholar] [CrossRef] [PubMed]
- Mokhles, M.M.; Rajeswaran, J.; Bekkers, J.A.; Borsboom, G.J.; Roos-Hesselink, J.W.; Steyerberg, E.W.; Bogers, A.J.; Takkenberg, J.J.; Blackstone, E.H. Capturing echocardiographic allograft valve function over time after allograft aortic valve or root replacement. J. Thorac. Cardiovasc. Surg. 2014, 148, 1921–1928.e3. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, S.; Yagihara, T.; Kobayashi, J.; Nakajima, H.; Toda, K.; Fujita, T.; Ichikawa, H.; Ogino, H.; Nakatani, T.; Taniguchi, S. Mid- to long-term outcomes of cardiovascular tissue replacements utilizing homografts harvested and stored at Japanese institutional tissue banks. Surg. Today 2011, 41, 500–509. [Google Scholar] [CrossRef]
- El-Hamamsy, I.; Yacoub, M.H.; Chester, A.H. Neuronal regulation of aortic valve cusps. Curr. Vasc. Pharmacol. 2009, 7, 40–46. [Google Scholar] [CrossRef]
- Hung, L.; Rahimtoola, S.H. Prosthetic Heart Valves and Pregnancy. Circulation 2003, 107, 1240–1246. [Google Scholar] [CrossRef] [Green Version]
- Heuvelman, H.J.; Arabkhani, B.; Cornette, J.M.; Pieper, P.G.; Bogers, A.J.; Takkenberg, J.; Roos-Hesselink, J.W. Pregnancy Outcomes in Women with Aortic Valve Substitutes. Am. J. Cardiol. 2013, 111, 382–387. [Google Scholar] [CrossRef]
- Kebed, K.Y.; Bishu, K.; Al Adham, R.I.; Baddour, L.M.; Connolly, H.M.; Sohail, M.R.; Steckelberg, J.M.; Wilson, W.R.; Murad, M.H.; Anavekar, N.S. Pregnancy and postpartum infective endocarditis: Asystematic review. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2014; Volume 89, pp. 1143–1152. [Google Scholar]
- El-Hamamsy, I.; Clark, L.; Stevens, L.M.; Sarang, Z.; Melina, G.; Takkenberg, J.J.; Yacoub, M.H. Late Outcomes Following Freestyle Versus Homograft Aortic Root Replacement: Results from a Prospective Randomized Trial. J. Am. Coll. Cardiol. 2010, 55, 368–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nappi, F.; Singh, S.S.A.; Spadaccio, C.; Acar, C. Ross operation 23 years after surgery: It should not be a “forgotten” option. J. Card. Surg. 2020, 35, 952–956. [Google Scholar] [CrossRef] [PubMed]
- Mazine, A.; El-Hamamsy, I.; Verma, S.; Peterson, M.D.; Bonow, R.O.; Yacoub, M.H.; David, T.E.; Bhatt, D.L. Ross Procedure in Adults for Cardiologists and Cardiac Surgeons: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 2761–2777. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Spadaccio, C.; Acar, C.; El-Hamamsy, I. Lights and Shadows on the Ross Procedure: Biological Solutions for Biological Problems. In Seminars in Thoracic and Cardiovascular Surgery; WB Saunders: Philadelphia, PA, USA, 2020; Volume 32, pp. 815–822. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Patients |
|---|---|
| Patients | 210 (100%) |
| Male sex | 125 (59.5%) |
| Mean age (range) | 40.1 ± 17.9 (10–77) |
| Age groups | |
| <25 years | 42 (20.0%) |
| 25–50 years | 112 (53.3%) |
| >50 years | 56 (26.7%) |
| Smoking history | 21 (10.0%) |
| Hypertension | 24 (11.4%) |
| Dyslipidemia | 6 (2.8%) |
| Diabetes | 4 (1.9%) |
| Chronic obstructive pulmonary disease | 12 (5.7%) |
| Chronic kidney disease | 5 (2.4%) |
| Preoperative NYHA class | |
| 1 | 0 (0.0%) |
| 2 | 64 (30.5%) |
| 3 | 83 (39.5%) |
| 4 | 63 (30.0%) |
| Etiology | |
| Endocarditis | 101 (48.1%) |
| <25 years | 27 |
| 25–50 years | 67 |
| >50 years | 7 |
| Rheumatic | 57 (27.1%) |
| <25 years | 13 |
| 25–50 years | 24 |
| >50 years | 20 |
| Congenital | 35 (16.7%) |
| <25 years | 2 |
| 25–50 years | 16 |
| >50 years | 17 |
| Other | 17 (8.1%) |
| <25 years | 0 |
| 25–50 years | 5 |
| >50 years | 12 |
| Surgical indication | |
| Isolated aortic stenosis | 46 (21.9%) |
| Isolated aortic regurgitation | 85 (40.5%) |
| Mixed aortic stenosis and regurgitation | 79 (37.6%) |
| Previous cardiac surgery | 48 (22.8%) |
| Aortic valve replacement, mechanical | 23 (10.9%) |
| Aortic valve replacement, biological | 13 (6.2%) |
| Homograft | 10 (4.8%) |
| Other | 2 (0.9%) |
| Repeated cardiac surgery | 48 (22.8%) |
| Redux | 42 (20.0%) |
| Tridux | 5 (2.4%) |
| Quadridux | 1 (0.5%) |
| Operative Data | Patients |
| Concomitant procedure | 49 (23.3%) |
| Myocardial revascularization | 19 (9.0%) |
| Mitral valve homograft | 10 (4.8%) |
| Tricuspid valve repair | 9 (4.3%) |
| Mitral homograft valve repair | 8 (3.8%) |
| Tricuspid valve replacement | 3 (1.4%) |
| Technical procedure | |
| Freehand | 55 (26.2%) |
| By etiology | |
| Endocarditis | 35 |
| Rheumatic | 10 |
| Congenital | 8 |
| Other | 2 |
| By age | |
| <25 years | 16 |
| 25–50 years | 34 |
| >50 years | 5 |
| Miniroot | 155 (73.8%) |
| By etiology | |
| Endocarditis | 66 |
| Rheumatic | 47 |
| Congenital | 27 |
| Other | 15 |
| By age | |
| <25 years | 26 |
| 25–50 years | 78 |
| >50 years | 51 |
| Allograft mean size | |
| Freehand, mean-SD/median-IQR | 22.6 ± 1.5, 22 (20–24) |
| Miniroot, mean-SD/median-IQR | 22.5 ± 1.8, 22 (20–24) |
| Severe aortic annular calcification | 32 (15.2%) |
| Donor age (range) | 44.1 ± 7.1 (5–61) |
| Donor age > 50 years | 68 (32.3%) |
| Donor annulus, mean-SD/median-IQR | 25.2 ± 3.6, 25 (22–28) |
| Gender mismatch | 92 (43.8%) |
| Annular size mismatch (>5 mm) | 11 (5.2%) |
| Blood group mismatch | 109 (51.9%) |
| Rh antigen mismatch | 34 (16.2%) |
| Outcome | Patients | p Value |
|---|---|---|
| Early mortality | 12 (5.7%) | |
| By age | 0.005 y | |
| <25 years | 1 (2.4%) | |
| 25–50 years | 3 (2.7%) | |
| >50 years | 8 (14.3%) | |
| By etiology | 0.165 | |
| Endocarditis | 9 (8.9%) | |
| Rheumatic | 3 (5.3%) * | |
| Congenital | 0 (0%) | |
| Other | 0 (0%) | |
| By technical procedure | 0.147 | |
| Freehand | 1 (1.8%) | |
| Miniroot | 11 (7.1%) | |
| By cardiac procedure | <0.001 z | |
| First | 7 (4.3%) | |
| Second | 2 (4.8%) | |
| Third | 2 (40.0%) | |
| Fourth | 1 (100.0%) | |
| Overall mortality | 68 (32.4%) | |
| By age | ||
| <25 years | 3 (7.1%) | <0.001 x |
| 25–50 years | 15 (13.4%) | |
| >50 years | 50 (89.3%) | |
| By etiology | ||
| Endocarditis | 22 (21.8%) | <0.001 jj |
| Rheumatic | 22 (38.6%) | |
| Congenital | 16 (45.7%) | |
| Other | 8 (47.0%) | |
| By technical procedure | ||
| Freehand | 8 (14.5%) | <0.001 |
| Miniroot | 60 (38.7%) | |
| Valve related cardiac mortality | 29 (13.8%) | |
| By age | ||
| <25 years | 3 (7.1%) | 0.276 |
| 25–50 years | 15 (13.4%) | |
| >50 years | 11 (19.6%) | |
| By etiology | ||
| Endocarditis | 20 (19.8%) | 0.044 |
| Rheumatic | 6 (10.5%) | |
| Congenital | 2 (5.7%) | |
| Other | 1 (5.9%) | |
| By technical procedure | ||
| Freehand | 5 (9.1%) | 0.691 |
| Miniroot | 24 (15.5%) | |
| Not valve related cardiac mortality | 19 (9.0%) | |
| Not cardiac mortality | 20 (9.5%) |
| Outcome | Patients | p Value |
|---|---|---|
| Structural valve degeneration By age <25 years 25–50 years >50 years By etiology Endocarditis Rheumatic Congenital Other By technical procedure Freehand Miniroot | 57 (27.1%) 22 (52.4%) 30 (26.8%) 5 (8.9%) 31 (30.7%) 15 (26.3%) 7 (20.0%) 4 (23.5%) 27 (49.1%) 30 (19.3%) | <0.001 * 0.642 <0.001 |
| Reoperation By age <25 years 25–50 years >50 years By etiology Endocarditis Rheumatic Congenital Other By technical procedure Freehand Miniroot Reoperation type Aortic valve replacement (mechanical) Aortic allograft Bentall procedure Aortic valve replacement (biologic) Ascending aorta | 71 (33.8%) 23 (54.8%) 38 (33.9%) 10 (17.8%) 38 (37.6%) 19 (33.3%) 9 (25.7%) 5 (29.4%) 34 (61.8%) 37 (23.9%) 36 (50.7%) 13 (18.3%) 12 (16.9%) 8 (11.3%) 2 (2.8%) | 0.001 y 0.787 0.401 |
| MACCEs By age <25 years 25–50 years >50 years By etiology Endocarditis Rheumatic Congenital Other By technical procedure Freehand Miniroot | 115 (54.8%) 26 (61.9%) 49 (43.7%) 40 (71.4%) 51 (50.5%) 31 (54.4%) 21 (60.0%) 12 (70.6%) 36 (65.4%) 79 (51.0%) | <0.001 z 0.914 0.124 |
| NYHA class Preoperative (mean ± SD) 1 2 3 4 After 6 months from surgery (mean ± SD) 1 2 3 4 After 1 year from surgery (mean ± SD) 1 2 3 4 After 5 years from surgery (mean ± SD) 1 2 3 4 After 10 years from surgery (mean ± SD) 1 2 3 4 | 3.0 ± 0.8 0 64 83 63 1.4 ± 0.5 127 66 5 0 1.3 ± 0.5 144 51 2 1 1.3 ± 0.5 147 47 3 1 1.4 ± 0.6 97 50 1 2 | <0.001 x 0.002 x 0.562 x <0.001 x |
| Univariate Analysis | |||
|---|---|---|---|
| Variable | Significance | Hazard Ratio | 95%CI |
| Miniroot | <0.001 | 0.25 | 0.13–0.48 |
| Age | <0.001 | 0.94 | 0.92–0.97 |
| Endocarditis | 0.166 | 1.41 | 0.77–1.60 |
| Allograft dimension | 0.027 | 0.82 | 0.68–0.98 |
| Etiology Rheumatic Congenital Other | 0.561 0.228 0.551 | 0.81 0.56 0.69 | 0.39–1.67 0.22–1.43 0.21–2.30 |
| Male sex | 0.094 | 1.73 | 0.91–3.30 |
| Hypertension | 0.228 | 0.50 | 0.16–1.54 |
| Smoking history | 0.074 | 0.26 | 0.06–1.14 |
| Diabetes | 0.923 | 0.89 | 0.09–8.76 |
| Multivariable Analysis | |||
| Variable | Significance | Hazard Ratio | 95%CI |
| Age Miniroot Endocarditis Allograft dimension Constant | <0.001 0.001 0.222 0.249 0.043 | 0.95 0.30 0.64 0.89 89.89 | 0.92–0.97 0.14–0.62 0.31–1.31 0.43–1.08 1.16–6945.78 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nappi, F.; Nenna, A.; Spadaccio, C.; Avtaar Singh, S.S.; Almazil, A.; Acar, C. The Use of the Cryopreserved Aortic Homograft for Aortic Valve Replacement: Is It Still an Option? J. Cardiovasc. Dev. Dis. 2023, 10, 248. https://doi.org/10.3390/jcdd10060248
Nappi F, Nenna A, Spadaccio C, Avtaar Singh SS, Almazil A, Acar C. The Use of the Cryopreserved Aortic Homograft for Aortic Valve Replacement: Is It Still an Option? Journal of Cardiovascular Development and Disease. 2023; 10(6):248. https://doi.org/10.3390/jcdd10060248
Chicago/Turabian StyleNappi, Francesco, Antonio Nenna, Cristiano Spadaccio, Sanjeet Singh Avtaar Singh, Almothana Almazil, and Christophe Acar. 2023. "The Use of the Cryopreserved Aortic Homograft for Aortic Valve Replacement: Is It Still an Option?" Journal of Cardiovascular Development and Disease 10, no. 6: 248. https://doi.org/10.3390/jcdd10060248