
Bempedoic Acid: An Emerging Therapy for Uncontrolled Low-Density Lipoprotein (LDL) Cholesterol
 , and
, and
Abstract
:1. Introduction
2. Role of LDL-C in Development of ASCVD
3. Role of Statins for CVD Prevention
4. LDL-C Goals Revision as per ESC 2019 (vs. ESC 2016)
- An updated Systematic Coronary Risk Evaluation (SCORE) risk assessment chart was introduced, which was also applicable to individuals above age 65 years.
- Class I/A recommendations for statin therapy were expanded by lowering the untreated LDL-C levels eligible for treatment.
- Finally, Class I/A statin recommendation was also provided for individuals aged 66–75 years.
5. Poor LDL-C Goals Attainment Based on Revised Guidelines: DA VINCI and DYSIS II
6. Residual Cardiovascular (CV) Risk Post Statin Therapy
7. Optimization of Uncontrolled LDL-C Management through Non-Statin Therapy
8. Bempedoic Acid: A Novel Non-Statin Lipid-Lowering Therapy
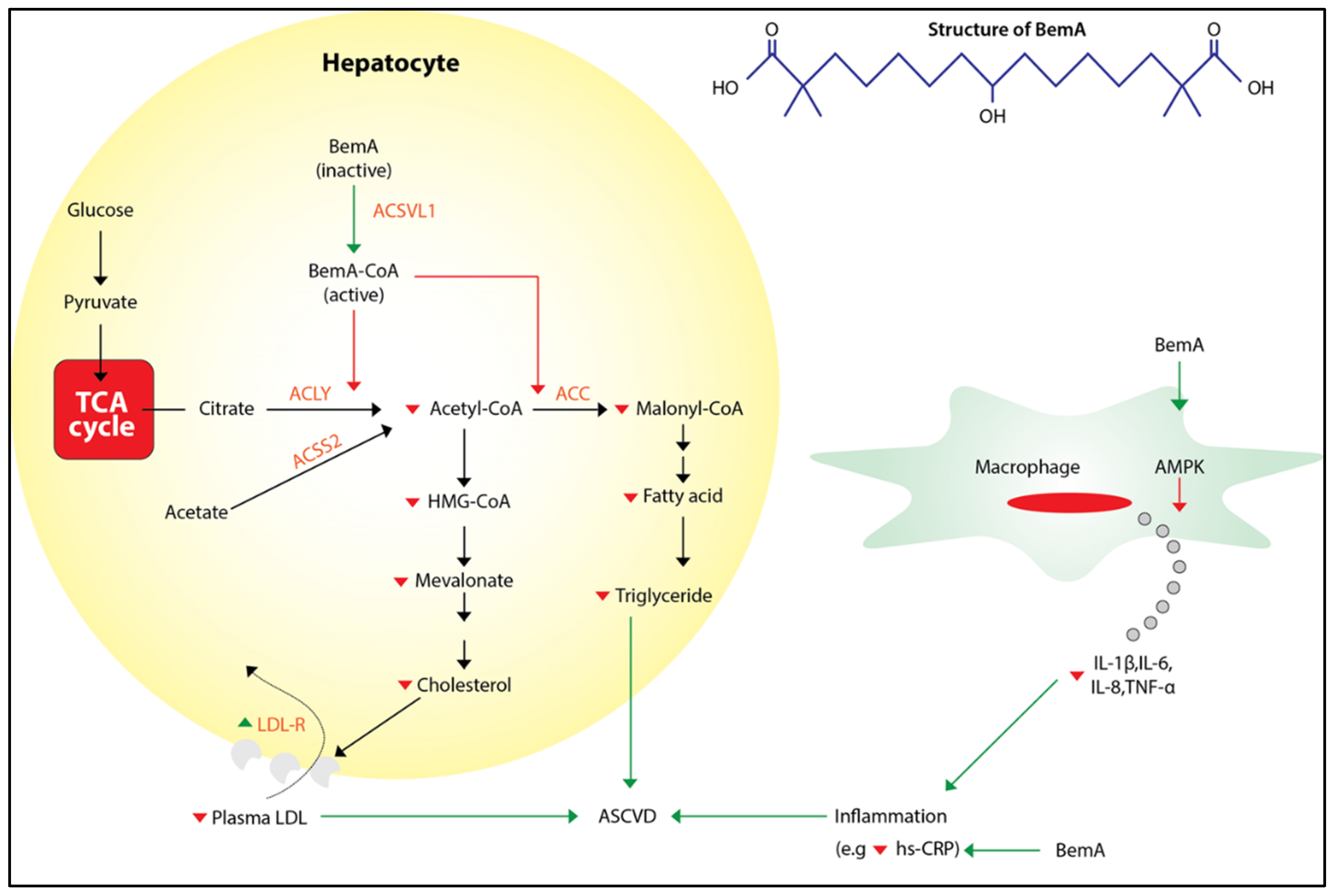
9. Mechanism of Action of Bempedoic Acid
10. Pharmacokinetics of Bempedoic Acid
11. Bempedoic Acid—Efficacy Analysis from Clinical Trials
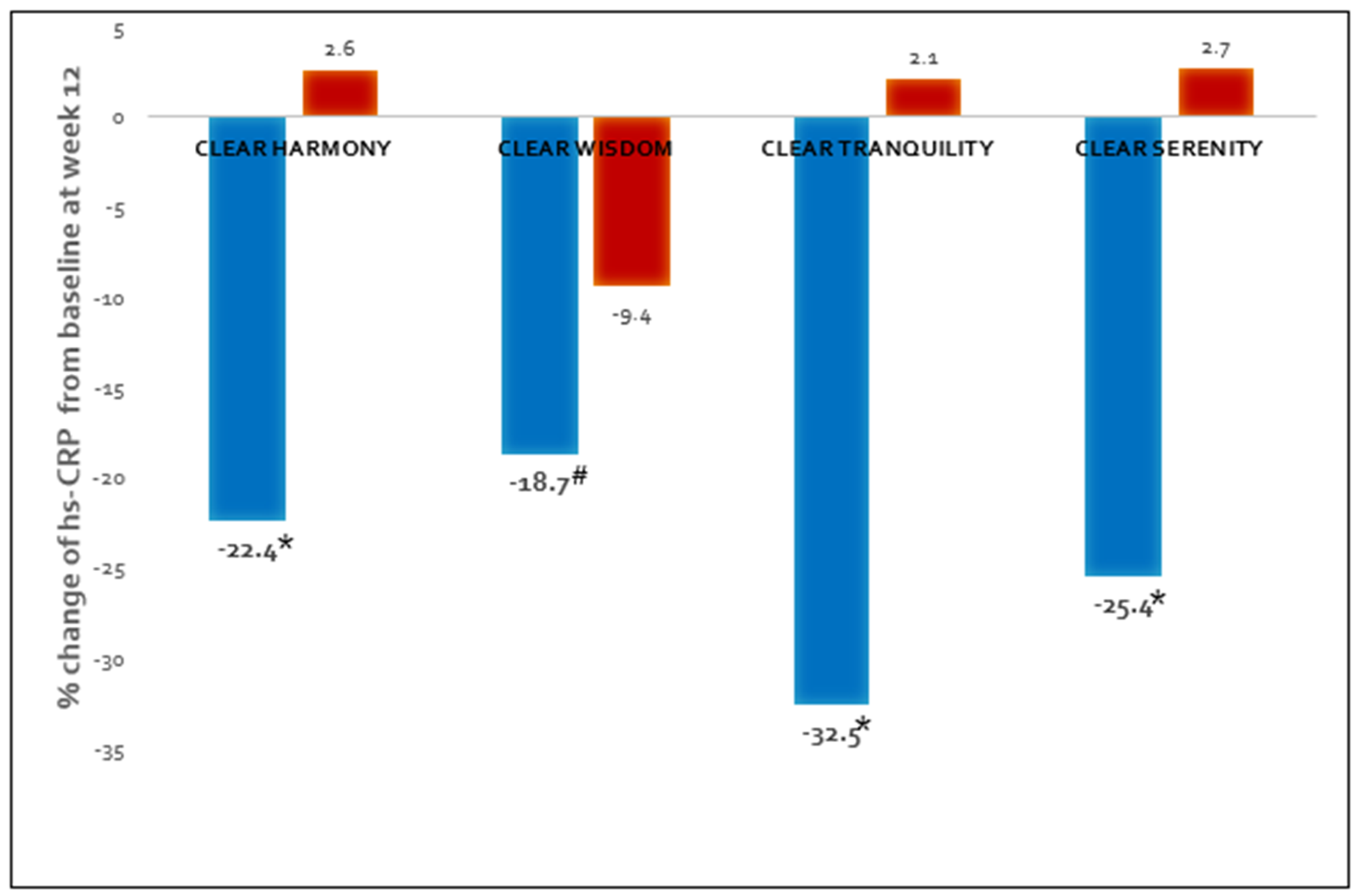
12. Effect of Bempedoic Acid on Atherogenic Lipids and Inflammation
13. Bempedoic Acid Safety Analysis
14. Effect of Bempedoic Acid on Glycemic Status
15. Use of Bempedoic Acid along with Other Statins
16. Effect of Bempedoic Acid on Uric Acid Level
17. Bempedoic Acid in Patients with CKD and Hypertension
18. Bempedoic Acid—Long Term Cardiovascular Outcome Trial
19. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Puri, R.; Mehta, V.; Iyengar, S.S.; Narasingan, S.N.; Duell, P.B.; Sattur, G.B.; Vijayaraghavan, K.; Mohan, J.C.; Wangnoo, S.K.; Dalal, J.; et al. Lipid Association of India Expert Consensus Statement on Management of Dyslipidemia in Indians 2020: Part III. J. Assoc. Physicians India 2020, 68, 8–9. [Google Scholar] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. ESC Scientific Document Group. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Haq, I.; Bilitou, A.; Aguiar, C.; Arca, M.; Connolly, D.L.; Eriksson, M.; Ferrières, J.; Hildebrandt, P.; Laufs, U.; et al. Evaluation of contemporary treatment of high- and very high-risk patients for the prevention of cardiovascular events in Europe—Methodology and rationale for the multi-national observational SANTORINI study. Atheroscler. Plus 2021, 43, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Enas, E.A.; Varkey, B.; Gupta, R. Expanding statin use for prevention of ASCVD in Indians: Reasoned and simplified proposals. Indian Heart J. 2020, 72, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Ginsberg, H.N.; Davidson, M.H.; Pordy, R.; Bessac, L.; Minini, P.; Eckel, R.H.; Cannon, C.P. Reductions in Atherogenic Lipids and Major Cardiovascular Events. Circulation 2016, 134, 1931–1943. [Google Scholar] [CrossRef] [PubMed]
- Baigent, C.; Blackwell, L.; Emberson, J.; Holland, L.E.; Reith, C.; Bhala, N.; Collins, R.; Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170 000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar] [CrossRef]
- Wang, Q.; Liang, C. Role of Lipid-Lowering Therapy in Low-Density Lipoprotein Cholesterol Goal attainment: Focus on Patients With Acute Coronary Syndrome. J. Cardiovasc. Pharmacol. 2020, 76, 658. [Google Scholar] [CrossRef]
- Mortensen, M.B.; Nordestgaard, B.G. 2019 vs. 2016 ESC/EAS statin guidelines for primary prevention of atherosclerotic cardi-ovascular disease. Eur. Heart J. 2020, 41, 3005–3015. [Google Scholar] [CrossRef]
- Puri, R.; Mehta, V.; Duell, P.B.; Nair, D.; Mohan, J.C.; Yusuf, J.; Dalal, J.J.; Mishra, S.; Kasliwal, R.R.; Agarwal, R.; et al. Proposed low-density lipoprotein cholesterol goals for secondary prevention and familial hypercholesterolemia in India with focus on PCSK9 inhibitor monoclonal antibodies: Expert consensus statement from Lipid Association of India. J. Clin. Lipidol. 2020, 14, e1–e13. [Google Scholar] [CrossRef]
- Ray, K.K.; Molemans, B.; Schoonen, W.M.; Giovas, P.; Bray, S.; Kiru, G.; Murphy, J.; Banach, M.; De Servi, S.; Gaita, D.; et al. EU-Wide Cross-Sectional Observational Study of Lipid-Modifying Therapy Use in Secondary and Primary Care: The DA VINCI study. Eur. J. Prev. Cardiol. 2021, 28, 1279–1289. [Google Scholar] [CrossRef]
- Buddhari, W.; Uerojanaungkul, P.; Sriratanasathavorn, C.; Sukonthasarn, A.; Ambegaonkar, B.; Brudi, P.; Horack, M.; Lautsch, D.; Vyas, A.; Gitt, A.K. Low-Density Lipoprotein Cholesterol Target Attainment in Patients Surviving an Acute Coronary Syndrome in Thailand: Results From the Dyslipidaemia International Study (DYSIS) II. Heart Lung Circ. 2020, 29, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Sampson, U.K.; Fazio, S.; Linton, M.F. Residual Cardiovascular Risk Despite Optimal LDL Cholesterol Reduction with Statins: The Evidence, Etiology, and Therapeutic Challenges. Curr. Atheroscler. Rep. 2012, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yao, T.; Lu, W.; Ke, J.; Zhang, H.; Zhao, X.; Song, B.; Liu, T.; Ke, Q.; Liu, C. Residual Risk of Coronary Atherosclerotic Heart Disease and Severity of Coronary Atherosclerosis Assessed by ApoB and LDL-C in Participants With Statin Treatment: A Retrospective Cohort Study. Front. Endocrinol. 2022, 13, 865863. [Google Scholar] [CrossRef] [PubMed]
- Niman, S.; Rana, K.; Reid, J.; Sheikh-Ali, M.; Lewis, T.; Choksi, R.R.; Goldfaden, R.F. A Review of the Efficacy and Tolerability of Bempedoic Acid in the Treatment of Hypercholesterolemia. Am. J. Cardiovasc. Drugs 2020, 20, 535–548. [Google Scholar] [CrossRef] [PubMed]
- Nexletol (Bempedoic Acid) Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/211616s000lbl.pdf (accessed on 2 December 2022).
- Nilemdo (Bempedoic Acid) Summary of Product Characteristics (SmPC). Available online: https://www.ema.europa.eu/en/documents/smop-initial/chmp-summary-positive-opinion-nilemdo_en.pdf (accessed on 2 December 2022).
- Ballantyne, C.M.; Bays, H.; Catapano, A.L.; Goldberg, A.; Ray, K.K.; Saseen, J.J. Role of Bempedoic Acid in Clinical Practice. Cardiovasc. Drugs Ther. 2021, 35, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Wichaiyo, S.; Supharattanasitthi, W. Bempedoic Acid: A New Non-statin Drug for the Treatment of Dyslipidemia. Clin. Drug Investig. 2021, 41, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Bays, H.E.; Catapano, A.L.; Lalwani, N.D.; Bloedon, L.T.; Sterling, L.R.; Robinson, P.L.; Ballantyne, C.M.; CLEAR Harmony Trial. Safety and Efficacy of Bempedoic Acid to Reduce LDL Cholesterol. N. Engl. J. Med. 2019, 380, 1022–1032. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.C.; Leiter, L.A.; Stroes, E.S.G.; Baum, S.J.; Hanselman, J.C.; Bloedon, L.T.; Lalwani, N.D.; Patel, P.M.; Zhao, X.; Duell, P.B. Effect of Bempedoic Acid vs Placebo Added to Maximally Tolerated Statins on Low-Density Lipoprotein Cholesterol in Patients at High Risk for Cardiovascular Disease: The CLEAR Wisdom Randomized Clinical Trial. JAMA 2019, 322, 1780–1788. [Google Scholar] [CrossRef]
- Laufs, U.; Banach, M.; Mancini, G.B.J.; Gaudet, D.; Bloedon, L.T.; Sterling, L.R.; Kelly, S.; Stroes, E.S.G. Efficacy and Safety of Bempedoic Acid in Patients With Hypercholesterolemia and Statin Intolerance. J. Am. Heart Assoc. 2019, 8, e011662. [Google Scholar] [CrossRef]
- Ballantyne, C.M.; Banach, M.; Mancini, G.J.; Lepor, N.E.; Hanselman, J.C.; Zhao, X.; Leiter, L.A. Efficacy and safety of bempedoic acid added to ezetimibe in statin-intolerant patients with hypercholesterolemia: A randomized, placebo-controlled study. Atherosclerosis 2018, 277, 195–203. [Google Scholar] [CrossRef]
- Dai, L.; Zuo, Y.; You, Q.; Zeng, H.; Cao, S. Efficacy and safety of bempedoic acid in patients with hypercholesterolemia: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Prev. Cardiol. 2021, 28, 825–833. [Google Scholar] [CrossRef] [PubMed]
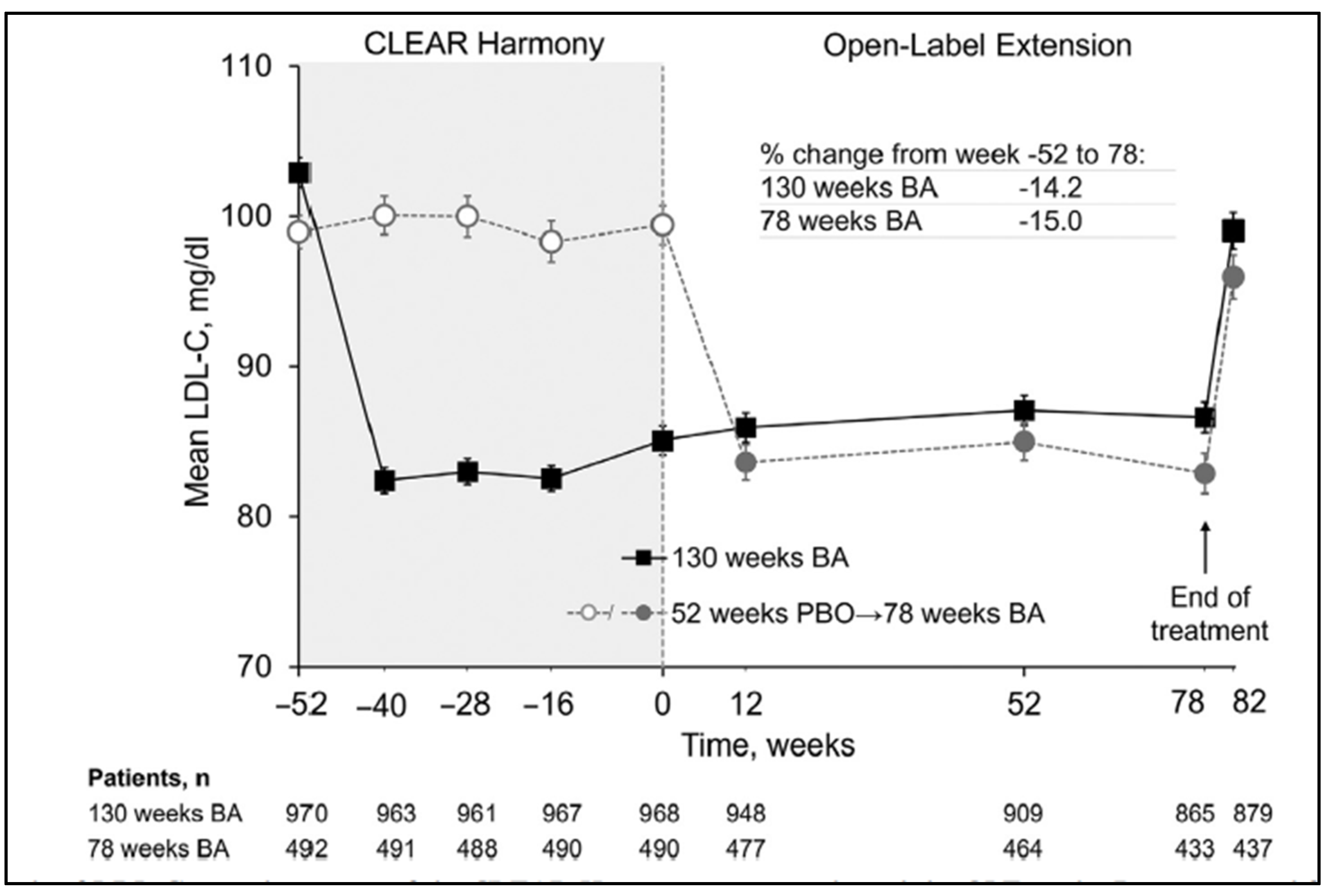
- Ballantyne, C.M.; Banach, M.; Bays, H.E.; Catapano, A.L.; Laufs, U.; Stroes, E.S.; Robinson, P.; Lei, L.; Ray, K.K. Long-Term Safety and Efficacy of Bempedoic Acid in Patients With Atherosclerotic Cardiovascular Disease and/or Heterozygous Familial Hypercholesterolemia (from the CLEAR Harmony Open-Label Extension Study). Am. J. Cardiol. 2022, 174, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ballantyne, C.M.; Laufs, U.; Ray, K.K.; Leiter, L.A.; Bays, H.E.; Goldberg, A.C.; Stroes, E.S.; MacDougall, D.; Zhao, X.; Catapano, A.L. Bempedoic acid plus ezetimibe fixed-dose combination in patients with hypercholesterolemia and high CVD risk treated with maximally tolerated statin therapy. Eur. J. Prev. Cardiol. 2019, 27, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Parco, C.; Karathanos, A.; Krieger, T.; Schulze, V.; Chernyak, N.; Icks, A.; Kelm, M.; Brockmeyer, M.; Wolff, G. Clinical efficacy and safety outcomes of bempedoic acid for LDL-C lowering therapy in patients at high cardiovascular risk: A systematic review and meta-analysis. BMJ Open 2022, 12, e048893. [Google Scholar] [CrossRef] [PubMed]
- Ballantyne, C.M.; Bays, H.E.; Louie, M.J.; Smart, J.; Zhang, Y.; Ray, K.K. Factors Associated With Enhanced Low-Density Lipoprotein Cholesterol Lowering With Bempedoic Acid. J. Am. Heart Assoc. 2022, 11, e024531. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Morris, P.B.; Ballantyne, C.M.; Birtcher, K.K.; Covington, A.M.; DePalma, S.M.; Minissian, M.B.; Orringer, C.E.; Smith, S.C.; Waring, A.A.; et al. 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2022, 80, 1366–1418. [Google Scholar] [CrossRef]
- Mehta, V.; Puri, R.; Duell, P.B.; Iyengar, S.S.; Wong, N.D.; Yusuf, J.; Mukhopadhyay, S.; Pradhan, A.; Muruganathan, A.; Wangnoo, S.K.; et al. Unmet Need for Further LDL-C Lowering in India despite Statin Therapy: Lipid Association of India Recommendations for the Use of Bempedoic Acid. J. Assoc. Physicians India 2022, 70, 67–75. [Google Scholar] [CrossRef]
- Banach, M.; Burchardt, P.; Chlebus, K.; Dobrowolski, P.; Dudek, D.; Dyrbuś, K.; Gąsior, M.; Jankowski, P.; Jóźwiak, J.; Kłosiewicz-Latoszek, L.; et al. PoLA/CFPiP/PCS/PSLD/PSD/PSH guidelines on diagnosis and therapy of lipid disorders in Poland 2021. Arch. Med. Sci. 2021, 17, 1447–1547. [Google Scholar] [CrossRef]
- Masson, W.; Lobo, M.; Lavalle-Cobo, A.; Molinero, G. Effect of Bempedoic Acid on atherogenic lipids and inflammation: A meta-analysis. Clin. Investig. Arterioscler. 2021, 33, 117–126. [Google Scholar] [CrossRef]
- Bays, H.E.; Banach, M.; Catapano, A.L.; Duell, P.B.; Gotto, A.M.; Laufs, U.; Leiter, L.A.; Mancini, G.B.J.; Ray, K.K.; Bloedon, L.T.; et al. Bempedoic acid safety analysis: Pooled data from four phase 3 clinical trials. J. Clin. Lipidol. 2020, 14, 649–659.e6. [Google Scholar] [CrossRef]
- Pirillo, A.; Catapano, A.L. New insights into the role of bempedoic acid and ezetimibe in the treatment of hypercholesterolemia. Curr. Opin. Endocrinol. Diabetes 2022, 29, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Leiter, L.A.; Banach, M.; Catapano, A.L.; Duell, P.B.; Gotto, A.M., Jr.; Laufs, U.; Mancini, G.B.J.; Ray, K.K.; Hanselman, J.C.; Ye, Z.; et al. Bempedoic acid in patients with type 2 diabetes mellitus, prediabetes, and normoglycaemia: A post hoc analysis of efficacy and glycaemic control using pooled data from phase 3 clinical trials. Diabetes Obes. Metab. 2022, 24, 868–880. [Google Scholar] [CrossRef] [PubMed]
- Shriver, K. Bempedoic Acid: A Novel LDL Cholesterol–Lowering Agent. Clin. Diabetes 2020, 38, 405–407. [Google Scholar] [CrossRef]
- Catapano, A.; Helms, B.; Lei, L.; Louie, M.; Bakris, G.; Toth, P. Safety and Efficacy of Bempedoic Acid in Patients with Renal Impairment. J. Clin. Lipidol. 2022, 16, e56. [Google Scholar] [CrossRef]
- Ferdinand, K.C.; Michos, E.D.; Everett, P.B.; Lei, L.; Sanganalmath, S.; Karlais, D.G. Safety and efficacy of bempedoic acid in patients with hypertension. J. Am. Coll. Cardiol. 2022, 79, 1566. [Google Scholar] [CrossRef]
- Nissen, S.E.; Lincoff, A.M.; Brennan, D.; Ray, K.K.; Mason, D.; Kastelein, J.J.; Thompson, P.D.; Libby, P.; Cho, L.; Plutzky, J.; et al. Bempedoic Acid and Cardiovascular Outcomes in Statin-Intolerant Patients. N. Engl. J. Med. 2023. epub ahead of print. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2016 ESC/EAS Guidelines | 2019 ESC/EAS Guidelines |
|---|---|
| Lipid-based: | Lipid-based: |
| LDL-C > 6 mmol/L (232 mg/dL) | LDL-C > 4.9 mmol/L (190 mg/dL) |
| or | or |
| TC > 8 mmol/L (309 mg/dL) | TC > 8 mmol/L (309 mg/dL) |
| Risk-based: | Risk-based: |
| Age 40–65 years | Age 40–75 years |
| LDL-C ≥ 4.0 mmol/L (155 mg/dL) | LDL-C ≥ 2.6 mmol/L (100 mg/dL) |
| SCORE 5% to <10% | SCORE 5% to <10% |
| Or | Or |
| Age 40–65 years | Age 40–75 years |
| LDL-C ≥ 2.6 mmol/L (100 mg/dL) | LDL-C ≥ 1.8 mmol/L (70 mg/dL) |
| SCORE ≥10% | SCORE ≥10% |
| Or | Or |
| Diabetes | Diabetes |
| Or | Or |
| Non-dialysis dependent CKD and eGFR <60 mL/min/1.73 m2 | Non-dialysis dependent CKD and eGFR <60 mL/min/1.73 m2 |
| Study Name | Population Studied | Intervention | LDL-C Reduction (Placebo Corrected Difference) at 12 Weeks |
|---|---|---|---|
| Bempedoic acid add-on to statin | |||
| CLEAR Harmony | ASCVD and/or HeFH Taking maximally tolerated statin with or without other lipid-lowering agents # LDL-C ≥ 70 mg/dL | Bempedoic acid 180 mg (n = 1488) versus placebo (n = 742) | −18.1% |
| CLEAR Wisdom | ASCVD and/or HeFH Taking maximally tolerated lipid lowering therapy LDL-C ≥ 70 mg/dL | Bempedoic acid 180 mg (n = 522) versus placebo (n = 257) | −17.4% |
| Bempedoic acid in statin-intolerant patients | |||
| CLEAR Serenity | History of statin intolerance to ≥ 2 statin LDL-C ≥ 130 mg/dL for primary prevention LDL-C ≥ 100 mg/dL for secondary prevention in ASCVD or for HeFH | Bempedoic acid 180 mg (n = 234) versus placebo (n = 111) Using low-dose statin (10%) Using other lipid-lowering agents (30%) Never used lipid-lowering agents (57%) | −21.4% |
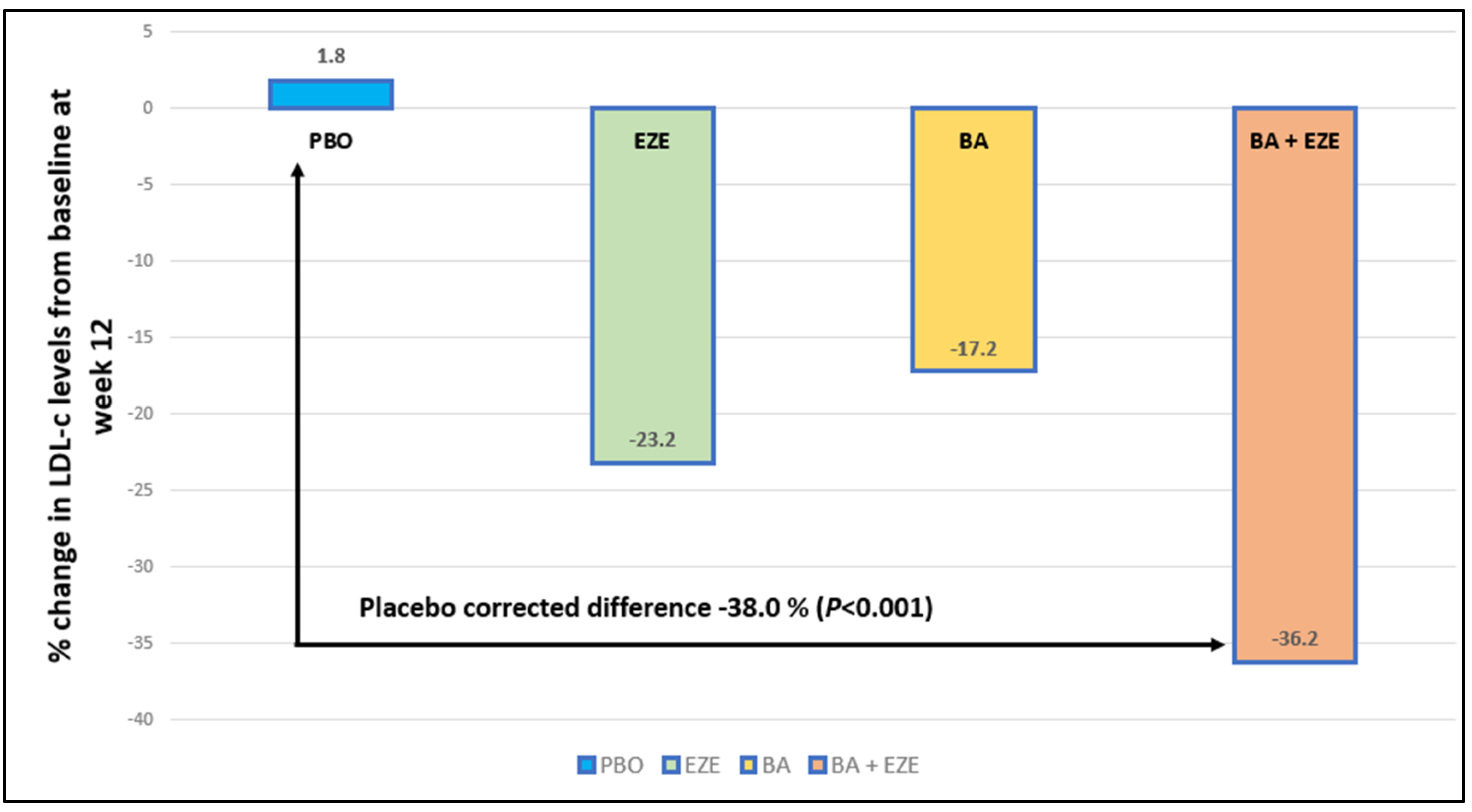
| CLEAR Tranquility | History of statin intolerance with or without use of low low-dose statin LDL ≥ 100 mg/dL | Bempedoic acid 180 mg plus ezetimibe 10 mg (n = 181) versus placebo plus ezetimibe 10 mg (n = 88) Using low-dose statin (30%) | −28.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pradhan, A.; Bhandari, M.; Vishwakarma, P.; Singh, A.; Perrone, M.A.; Sethi, R. Bempedoic Acid: An Emerging Therapy for Uncontrolled Low-Density Lipoprotein (LDL) Cholesterol. J. Cardiovasc. Dev. Dis. 2023, 10, 195. https://doi.org/10.3390/jcdd10050195
Pradhan A, Bhandari M, Vishwakarma P, Singh A, Perrone MA, Sethi R. Bempedoic Acid: An Emerging Therapy for Uncontrolled Low-Density Lipoprotein (LDL) Cholesterol. Journal of Cardiovascular Development and Disease. 2023; 10(5):195. https://doi.org/10.3390/jcdd10050195
Chicago/Turabian StylePradhan, Akshyaya, Monika Bhandari, Pravesh Vishwakarma, Abhishek Singh, Marco Alfonso Perrone, and Rishi Sethi. 2023. "Bempedoic Acid: An Emerging Therapy for Uncontrolled Low-Density Lipoprotein (LDL) Cholesterol" Journal of Cardiovascular Development and Disease 10, no. 5: 195. https://doi.org/10.3390/jcdd10050195