
Long-Term Renal Function after Catheter Ablation of Atrial Fibrillation
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
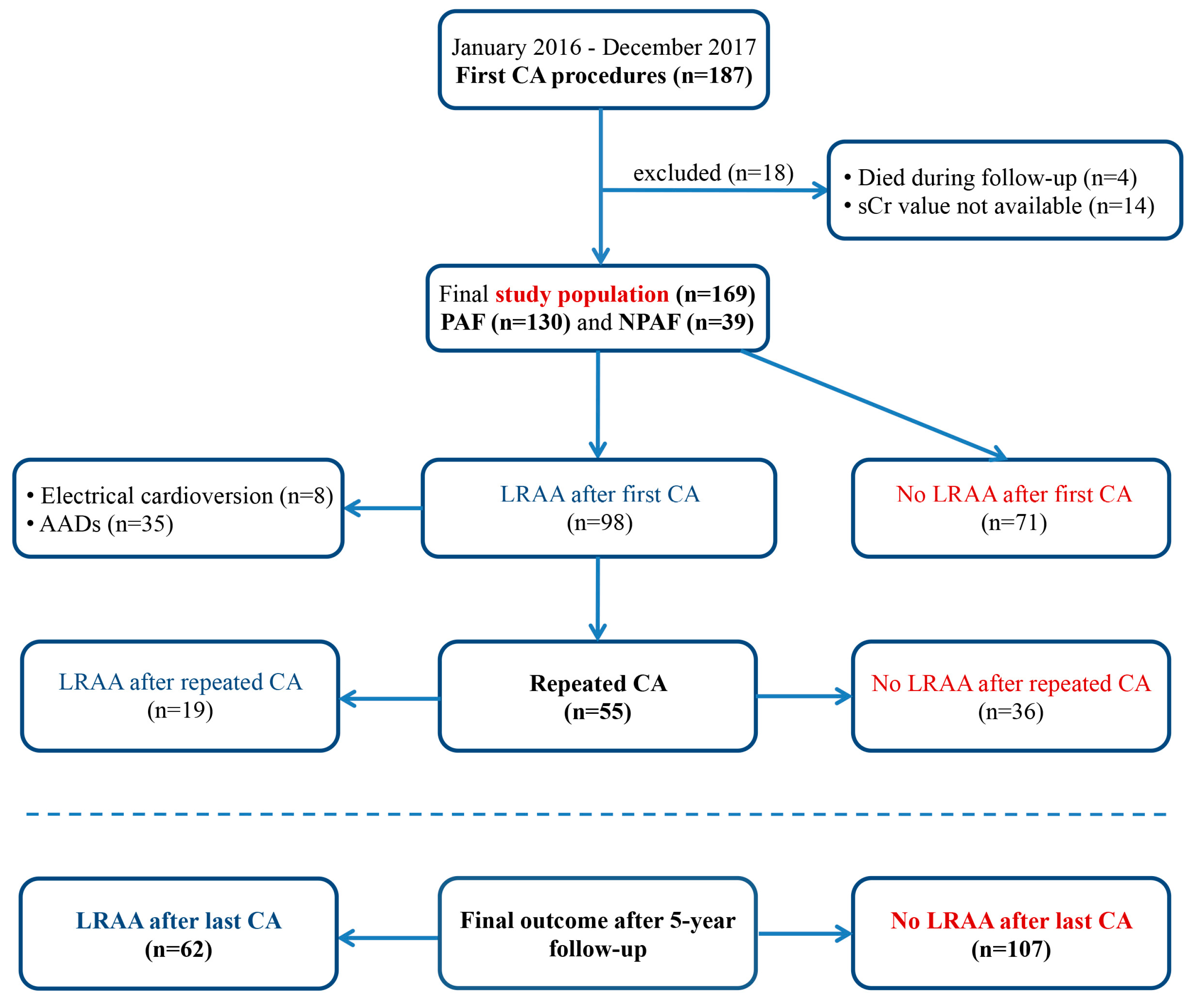
2.1. Study Population
2.2. Pre-Ablation Work Up
2.3. Evaluation of Renal Function
2.4. Ablation Procedure
2.5. Post-Ablation Follow-Up
2.6. Statistical Analysis
3. Results
3.1. Study Population
3.2. Baseline Renal Function
3.3. Changes in Renal Function According to the Rhythm Outcome after CA
3.4. Renal Function after 5-Year Follow-Up
3.5. Changes in eGFR Categories
3.6. The Risk Factors for Rapid CKD Progression
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.S.; Bilous, R.W.; Coresh, J. Chapter 1: Definition and classification of CKD. Kidney Int. Suppl. 2013, 3, 19–62. [Google Scholar] [CrossRef] [Green Version]
- Major, R.W.; Cheng, M.R.I.; Grant, R.A.; Shantikumar, S.; Xu, G.; Oozeerally, I.; Brunskill, N.J.; Gray, L.J. Cardiovascular disease risk factors in chronic kidney disease: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0192895. [Google Scholar] [CrossRef]
- Ding, W.Y.; Gupta, D.; Wong, C.F.; Lip, G.Y.H. Pathophysiology of atrial fibrillation and chronic kidney disease. Cardiovasc. Res. 2021, 117, 1046–1059. [Google Scholar] [CrossRef]
- Bansal, N.; Fan, D.; Hsu, C.Y.; Ordonez, J.D.; Marcus, G.M.; Go, A.S. Incident atrial fibrillation and risk of end-stage renal disease in adults with chronic kidney disease. Circulation 2013, 127, 569–574. [Google Scholar] [CrossRef] [Green Version]
- Carrero, J.J.; Trevisan, M.; Sood, M.M.; Barany, P.; Xu, H.; Evans, M.; Friberg, L.; Szummer, K. Incident Atrial Fibrillation and the Risk of Stroke in Adults with Chronic Kidney Disease: The Stockholm CREAtinine Measurements (SCREAM) Project. Clin. J. Am. Soc. Nephrol. 2018, 13, 1314–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Y.; Gao, J.; Ye, P.; Xing, A.; Wu, Y.; Wu, S.; Luo, Y. Comparison of atrial fibrillation in CKD and non-CKD populations: A cross-sectional analysis from the Kailuan study. Int. J. Cardiol. 2019, 277, 125–129. [Google Scholar] [CrossRef]
- Watanabe, H.; Tanabe, N.; Watanabe, T.; Darbar, D.; Roden, D.M.; Sasaki, S.; Aizawa, Y. Metabolic syndrome and risk of development of atrial fibrillation: The Niigata preventive medicine study. Circulation 2008, 117, 1255–1260. [Google Scholar] [CrossRef] [Green Version]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: Executive summary. Europace 2018, 20, 157–208. [Google Scholar] [CrossRef]
- Mujovic, N.; Marinkovic, M.; Lenarczyk, R.; Tilz, R.; Potpara, T.S. Catheter Ablation of Atrial Fibrillation: An Overview for Clinicians. Adv. Ther. 2017, 34, 1897–1917. [Google Scholar] [CrossRef] [Green Version]
- Mujovic, N.; Marinkovic, M.; Markovic, N.; Stankovic, G.; Lip, G.Y.H.; Blomstrom-Lundqvist, C.; Bunch, T.J.; Potpara, T.S. Persistency of left atrial linear lesions after radiofrequency catheter ablation for atrial fibrillation: Data from an invasive follow-up electrophysiology study. J. Cardiovasc. Electrophysiol. 2017, 28, 1403–1414. [Google Scholar] [CrossRef] [PubMed]
- Aviles, R.J.; Martin, D.O.; Apperson-Hansen, C.; Houghtaling, P.L.; Rautaharju, P.; Kronmal, R.A.; Tracy, R.P.; Van Wagoner, D.R.; Psaty, B.M.; Lauer, M.S.; et al. Inflammation as a risk factor for atrial fibrillation. Circulation 2003, 108, 3006–3010. [Google Scholar] [CrossRef] [Green Version]
- Ehrlich, J.R.; Hohnloser, S.H.; Nattel, S. Role of angiotensin system and effects of its inhibition in atrial fibrillation: Clinical and experimental evidence. Eur. Heart J. 2006, 27, 512–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Solus, J.; Chen, Q.; Rho, Y.H.; Milne, G.; Stein, C.M.; Darbar, D. Role of inflammation and oxidative stress in atrial fibrillation. Heart Rhythm 2010, 7, 438–444. [Google Scholar] [CrossRef] [Green Version]
- Park, J.W.; Yang, P.S.; Bae, H.J.; Yang, S.Y.; Yu, H.T.; Kim, T.H.; Uhm, J.S.; Joung, B.; Lee, M.H.; Pak, H.N. Five-Year Change in the Renal Function After Catheter Ablation of Atrial Fibrillation. J. Am. Heart Assoc. 2019, 8, e013204. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Lee, S.; Kim, Y.; Lee, Y.; Kang, M.W.; Kim, K.; Kim, Y.C.; Han, S.S.; Lee, H.; Lee, J.P.; et al. Atrial fibrillation and kidney function: A bidirectional Mendelian randomization study. Eur. Heart J. 2021, 42, 2816–2823. [Google Scholar] [CrossRef]
- Takahashi, Y.; Takahashi, A.; Kuwahara, T.; Okubo, K.; Fujino, T.; Takagi, K.; Nakashima, E.; Kamiishi, T.; Hikita, H.; Hirao, K.; et al. Renal function after catheter ablation of atrial fibrillation. Circulation 2011, 124, 2380–2387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawaji, T.; Shizuta, S.; Aizawa, T.; Yamagami, S.; Takeji, Y.; Yoshikawa, Y.; Kato, M.; Yokomatsu, T.; Miki, S.; Ono, K.; et al. Renal function and outcomes in atrial fibrillation patients after catheter ablation. PLoS ONE 2020, 15, e0241449. [Google Scholar] [CrossRef]
- Deng, H.; Shantsila, A.; Xue, Y.; Bai, Y.; Guo, P.; Potpara, T.S.; Zhan, X.; Fang, X.; Liao, H.; Wu, S.; et al. Renal function and outcomes after catheter ablation of patients with atrial fibrillation: The Guangzhou atrial fibrillation ablation registry. Arch. Cardiovasc. Dis. 2019, 112, 420–429. [Google Scholar] [CrossRef]
- Kornej, J.; Hindricks, G.; Banerjee, A.; Arya, A.; Sommer, P.; Rolf, S.; Husser, D.; Lip, G.Y.; Bollmann, A. Changes in renal function after catheter ablation of atrial fibrillation are associated with CHADS2 and CHA2DS2-VASc scores and arrhythmia recurrences. Heart 2015, 101, 126–131. [Google Scholar] [CrossRef]
- Base, E. Chapter 2: Definition, identification, and prediction of CKD progression. Kidney Int. Suppl. 2013, 3, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Eriksen, B.O.; Ingebretsen, O.C. The progression of chronic kidney disease: A 10-year population-based study of the effects of gender and age. Kidney Int. 2006, 69, 375–382. [Google Scholar] [CrossRef] [Green Version]
- Halbesma, N.; Kuiken, D.S.; Brantsma, A.H.; Bakker, S.J.; Wetzels, J.F.; De Zeeuw, D.; De Jong, P.E.; Gansevoort, R.T. Macroalbuminuria is a better risk marker than low estimated GFR to identify individuals at risk for accelerated GFR loss in population screening. J. Am. Soc. Nephrol. 2006, 17, 2582–2590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, E.; Horio, M.; Yamagata, K.; Iseki, K.; Hara, S.; Ura, N.; Kiyohara, Y.; Makino, H.; Hishida, A.; Matsuo, S. Slower decline of glomerular filtration rate in the Japanese general population: A longitudinal 10-year follow-up study. Hypertens. Res. 2008, 31, 433–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, A.; Djurdjev, O.; Beaulieu, M.; Er, L. Variability and risk factors for kidney disease progression and death following attainment of stage 4 CKD in a referred cohort. Am. J. Kidney Dis. 2008, 52, 661–671. [Google Scholar] [CrossRef]
- Rohla, M.; Pecen, L.; Cemin, R.; Patti, G.; Siller-Matula, J.M.; Schnabel, R.B.; Huber, K.; Kirchhof, P.; De Caterina, R. Reclassification, Thromboembolic, and Major Bleeding Outcomes Using Different Estimates of Renal Function in Anticoagulated Patients With Atrial Fibrillation: Insights From the PREFER-in-AF and PREFER-in-AF Prolongation Registries. Circ. Cardiovasc. Qual. Outcomes 2021, 14, e006852. [Google Scholar] [CrossRef]
- Carrero, J.J.; Hecking, M.; Chesnaye, N.C.; Jager, K.J. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat. Rev. Nephrol. 2018, 14, 151–164. [Google Scholar] [CrossRef]
- Halbesma, N.; Brantsma, A.H.; Bakker, S.J.; Jansen, D.F.; Stolk, R.P.; De Zeeuw, D.; De Jong, P.E.; Gansevoort, R.T.; PREVEND Study Group. Gender differences in predictors of the decline of renal function in the general population. Kidney Int. 2008, 74, 505–512. [Google Scholar] [CrossRef] [Green Version]
- Jafar, T.H.; Schmid, C.H.; Stark, P.C.; Toto, R.; Remuzzi, G.; Ruggenenti, P.; Marcantoni, C.; Becker, G.; Shahinfar, S.; De Jong, P.E.; et al. The rate of progression of renal disease may not be slower in women compared with men: A patient-level meta-analysis. Nephrol. Dial. Transplant. 2003, 18, 2047–2053. [Google Scholar] [CrossRef]
- Barrera-Chimal, J.; Girerd, S.; Jaisser, F. Mineralocorticoid receptor antagonists and kidney diseases: Pathophysiological basis. Kidney Int. 2019, 96, 302–319. [Google Scholar] [CrossRef]
- Koos, R.; Krueger, T.; Westenfeld, R.; Kuhl, H.P.; Brandenburg, V.; Mahnken, A.H.; Stanzel, S.; Vermeer, C.; Cranenburg, E.C.; Floege, J.; et al. Relation of circulating Matrix Gla-Protein and anticoagulation status in patients with aortic valve calcification. Thromb. Haemost. 2009, 101, 706–713. [Google Scholar] [PubMed] [Green Version]
- Nigwekar, S.U.; Bloch, D.B.; Nazarian, R.M.; Vermeer, C.; Booth, S.L.; Xu, D.; Thadhani, R.I.; Malhotra, R. Vitamin K-Dependent Carboxylation of Matrix Gla Protein Influences the Risk of Calciphylaxis. J. Am. Soc. Nephrol. 2017, 28, 1717–1722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, M.T.; Chen, Y.Y.; Chang, W.J.; Li, S.Y. Warfarin accelerated vascular calcification and worsened cardiac dysfunction in remnant kidney mice. J. Chin. Med. Assoc. 2018, 81, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, S.V.; Nadasdy, T.; Rovin, B.H.; Satoskar, A.A.; Nadasdy, G.M.; Wu, H.M.; Bhatt, U.Y.; Hebert, L.A. Warfarin-related nephropathy occurs in patients with and without chronic kidney disease and is associated with an increased mortality rate. Kidney Int. 2011, 80, 181–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, S.; Szeki, I.; Nash, M.J.; Thachil, J. Anticoagulation in chronic kidney disease patients-the practical aspects. Clin. Kidney J. 2014, 7, 442–449. [Google Scholar] [CrossRef] [Green Version]
- Potpara, T.S.; Ferro, C.J.; Lip, G.Y.H. Use of oral anticoagulants in patients with atrial fibrillation and renal dysfunction. Nat. Rev. Nephrol. 2018, 14, 337–351. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, T.; Zhao, J.; Li, G. Warfarin-related nephropathy: Prevalence, risk factors and prognosis. Int. J. Cardiol. 2014, 176, 1297–1298. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All Patients, n = 169 | No LRAA after Last CA, n = 107 (63.3%) | LRAA after Last CA, n = 62 (36.7%) | p-Value | |
|---|---|---|---|---|
| Age, y | 59.6 ± 10.1 | 58.8 ± 10.7 | 61.0 ± 8.8 | 0.181 |
| Male patients | 104 (61.5%) | 71 (66.4%) | 33 (53.2%) | 0.091 |
| BMI, kg/m2 | 27.1 ± 4.0 | 26.7 ± 4.1 | 27.7 ± 3.7 | 0.107 |
| NPAF | 39 (23.1%) | 16 (15%) | 23 (37.1%) | 0.001 * |
| History of AF before CA, y | 4.0 (2.0–7.0) | 4.0 (2.0–7.0) | 4.0 (2.0–7.0) | 0.971 |
| Failed AADs, n | 1.6 ± 0.7 | 1.5 ± 0.7 | 1.7 ± 0.7 | 0.139 |
| Hypertension | 117 (69.2%) | 72 (67.3%) | 45 (72.6%) | 0.473 |
| Diabetes mellitus | 17 (10.1%) | 9 (8.4%) | 8 (12.9%) | 0.349 |
| Congestive heart failure | 10 (5.9%) | 5 (4.7%) | 5 (8.1%) | 0.368 |
| Stroke | 12 (7.1%) | 6 (5.6%) | 6 (9.7%) | 0.321 |
| Coronary artery disease | 13 (7.7%) | 6 (5.6%) | 7 (11.3%) | 0.181 |
| BUN (mmol/L) | 6.1 ± 1.9 | 6.2 ± 1.8 | 6.0 ± 2.1 | 0.431 |
| Serum creatinine (µmol/L) | 86.1 ± 20.6 | 87.8 ± 20.5 | 83.3 ± 20.5 | 0.175 |
| Baseline eGFR (CKD-EPI), mL/min per 1.73 m2 | 78.7 ± 17.3 | 78.7 ± 17.3 | 78.8 ± 17.3 | 0.973 |
| GFR category 1 | 44 (26%) | 29 (27.1%) | 15 (24.2%) | 0.678 |
| GFR category 2 | 103 (61%) | 65 (60.8%) | 38 (61.3%) | 0.944 |
| CKD (GFR category ≥ 3) | 22 (13%) | 13 (12.1%) | 9 (14.5%) | 0.659 |
| CHA2DS2-VASc score | 1.8 ± 1.3 | 1.6 ± 1.1 | 2.2 ± 1.5 | 0.016 * |
| ΔCHA2DS2-VASc score | 0.4 ± 0.7 | 0.4 ± 0.7 | 0.4 ± 0.6 | 0.563 |
| LA diameter, mm | 41.6 ± 4.8 | 40.7 ± 4.8 | 43.0 ± 4.6 | 0.002 * |
| LV EDD, mm | 52.7 ± 4.3 | 52.8 ± 4.1 | 52.7 ± 4.6 | 0.900 |
| LV EF, % | 59.7 ± 7.3 | 60.3 ± 6.6 | 58.6 ± 8.3 | 0.154 |
| LV EF < 50% | 13 (7.7%) | 6 (5.6%) | 7 (11.3%) | 0.181 |
| Cardiac CT scan before ablation | 149 (88.2%) | 92 (86%) | 57 (91.9%) | 0.248 |
| VKA | 44 (26%) | 20 (18.7%) | 24 (38.7%) | 0.004 * |
| DOACs | 62 (36.7%) | 30 (28%) | 32 (51.6%) | 0.002 * |
| Amiodarone | 44 (26%) | 15 (14%) | 29 (46.8%) | <0.001 * |
| Propafenone | 26 (15.4%) | 12 (11.2%) | 14 (22.6%) | 0.048 * |
| Flecainide | 36 (21.3%) | 16 (15%) | 20 (32.3%) | 0.008 * |
| Beta blockers | 137 (81.1%) | 84 (78.5%) | 53 (85.5%) | 0.264 |
| ACEi | 84 (49.7%) | 49 (45.8%) | 35 (56.5%) | 0.182 |
| ARB | 19 (11.2%) | 12 (11.2%) | 7 (11.3%) | 0.988 |
| Thiazide diuretics | 36 (21.3%) | 23 (21.5%) | 13 (21%) | 0.936 |
| Loop diuretics | 21 (12.4%) | 12 (11.2%) | 9 (14.5%) | 0.531 |
| MRA | 16 (9.5%) | 9 (8.4%) | 7 (11.3%) | 0.538 |
| statins | 50 (29.6%) | 27 (25.2%) | 23 (37.1%) | 0.103 |
| Renal Function | LRAA after Last CA | Before CA | Post CA | p-Value (Post CA vs. before CA) | Δ (Post CA– before CA), n (95% CI) | p-Value (LRAA vs. No LRAA) |
|---|---|---|---|---|---|---|
| CKD-EPI eGFR, mL/min per 1.73 m2 | LRAA | 78.8 ± 17.3 | 72.0 ± 18.5 | <0.001 * | −6.8 (−10.2 to −3.4) | <0.001 * |
| No LRAA | 78.7 ± 17.3 | 79.4 ± 17.4 | 0.555 | 0.7 (−1.8 to 3.3) | ||
| MDRD eGFR, mL/min per 1.73 m2 | LRAA | 74.8 ± 18.2 | 69.4 ± 19.5 | 0.006 * | −5.4 (−9.2 to 1.6) | <0.001 * |
| No LRAA | 74.1 ± 17.0 | 77.4 ± 19.6 | 0.029 * | 3.3 (0.4 to 6.3) | ||
| Creatinine clearence, mL/min | LRAA | 98.2 ± 31.2 | 87.6 ± 31.3 | <0.001 * | −10.6 (−15.8 to −5.3) | <0.001 * |
| No LRAA | 94.0 ± 24.7 | 94.8 ± 26.2 | 0.624 | 0.8 (−2.5 to 4.1) | ||
| Serum creatinine (µmol/L) | LRAA | 83.3 ± 20.5 | 89.2 ± 26.1 | 0.006 * | 5.9 (1.7 to 10.2) | <0.001 * |
| No LRAA | 87.8 ± 20.5 | 83.8 ± 19.0 | 0.023 * | −4.0 (−7.4 to −0.6) | ||
| BUN (mmol/L) | LRAA | 6.0 ± 2.1 | 6.5 ± 2.7 | 0.078 | 0.5 (−0.1 to 1.1) | 0.006 * |
| No LRAA | 6.2 ± 1.8 | 5.8 ± 1.6 | 0.038 * | −0.3 (−0.7 to −0.1) |
| All Patients, n = 169 | No LRAA after Last CA, n = 107 (63.3%) | LRAA after Last CA, n = 62 (36.7%) | p-Value | |
|---|---|---|---|---|
| Certain rise | 14 (8.3%) | 13 (12.2%) | 1 (1.6%) | 0.019 * |
| Uncertain rise | 17 (10.1%) | 12 (11.2%) | 5 (8.1%) | 0.512 |
| Stable | 105 (62.1%) | 65 (60.7%) | 40 (64.5%) | 0.626 |
| Uncertain drop | 19 (11.2%) | 13 (12.2%) | 6 (9.7%) | 0.624 |
| Certain drop | 14 (8.3%) | 4 (3.7%) | 10 (16.1%) | 0.008 * |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age | 1.04 (0.98–1.09) | 0.197 | ||
| Female patients | 3.31 (1.30–8.44) | 0.012 * | 3.05 (1.13–8.20) | 0.027 * |
| BMI | 1.02 (0.92–1.13) | 0.743 | ||
| NPAF | 1.17 (0.42–3.27) | 0.763 | ||
| Hypertension | 1.46 (0.52–4.05) | 0.451 | ||
| Diabetes mellitus | 1.74 (0.50–5.98) | 0.378 | ||
| Coronary artery disease | 2.18 (0.49–9.62) | 0.303 | ||
| CHA2DS2-VASc score | 1.16 (0.84–1.59) | 0.360 | ||
| ΔCHA2DS2-VASc score | 1.38 (0.75–2.56) | 0.299 | ||
| baseline eGFR (CKD-EPI), mL/min per 1.73 m2 | 1.02 (0.99–1.04) | 0.219 | ||
| LA diameter, mm | 1.02 (0.93–1.12) | 0.638 | ||
| LV EDD, mm | 0.95 (0.85–1.06) | 0.376 | ||
| LV EF, % | 1.01 (0.94–1.08) | 0.889 | ||
| LV EF < 50% | 0.90 (0.12–6.81) | 0.917 | ||
| VKA | 3.52 (1.41–8.75) | 0.007 * | 3.32 (1.28–8.58) | 0.013 * |
| DOACs | 1.15 (0.45–2.93) | 0.766 | ||
| Amiodarone | 2.59 (1.05–6.39) | 0.038 * | 1.14 (0.44–2.99) | 0.785 |
| Propafenone | 1.86 (0.67–5.16) | 0.237 | ||
| Flecainide | 1.51 (0.54–4.20) | 0.432 | ||
| Beta blockers | 1.10 (0.36–3.34) | 0.862 | ||
| ACEi | 1.08 (0.44–2.66) | 0.870 | ||
| ARB | 2.67 (0.96–7.43) | 0.060 | ||
| ACEi/ARB | 2.09 (0.75–5.84) | 0.157 | ||
| Thiazide diuretics | 0.90 (0.29–2.72) | 0.846 | ||
| Loop diuretics | 3.22 (1.22–8.50) | 0.018 * | 1.55 (0.41–5.83) | 0.516 |
| MRA | 3.99 (1.43–11.15) | 0.008 * | 3.28 (1.13–9.54) | 0.029 * |
| statins | 1.04 (0.40–2.75) | 0.934 | ||
| LRAA after last CA | 4.54 (1.72–11.98) | 0.002 * | 3.36 (1.25–9.06) | 0.016 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovačević, V.; Marinković, M.M.; Kocijančić, A.; Isailović, N.; Simić, J.; Mihajlović, M.; Vučićević, V.; Potpara, T.S.; Mujović, N.M. Long-Term Renal Function after Catheter Ablation of Atrial Fibrillation. J. Cardiovasc. Dev. Dis. 2023, 10, 151. https://doi.org/10.3390/jcdd10040151
Kovačević V, Marinković MM, Kocijančić A, Isailović N, Simić J, Mihajlović M, Vučićević V, Potpara TS, Mujović NM. Long-Term Renal Function after Catheter Ablation of Atrial Fibrillation. Journal of Cardiovascular Development and Disease. 2023; 10(4):151. https://doi.org/10.3390/jcdd10040151
Chicago/Turabian StyleKovačević, Vladan, Milan M. Marinković, Aleksandar Kocijančić, Nikola Isailović, Jelena Simić, Miroslav Mihajlović, Vera Vučićević, Tatjana S. Potpara, and Nebojša M. Mujović. 2023. "Long-Term Renal Function after Catheter Ablation of Atrial Fibrillation" Journal of Cardiovascular Development and Disease 10, no. 4: 151. https://doi.org/10.3390/jcdd10040151