

Limited versus Radical Resection in Mitral Valve Infective Endocarditis Surgery
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Operative Technique
2.3. Postoperative Care
2.4. Endpoints and Definitions
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Operative Characteristics
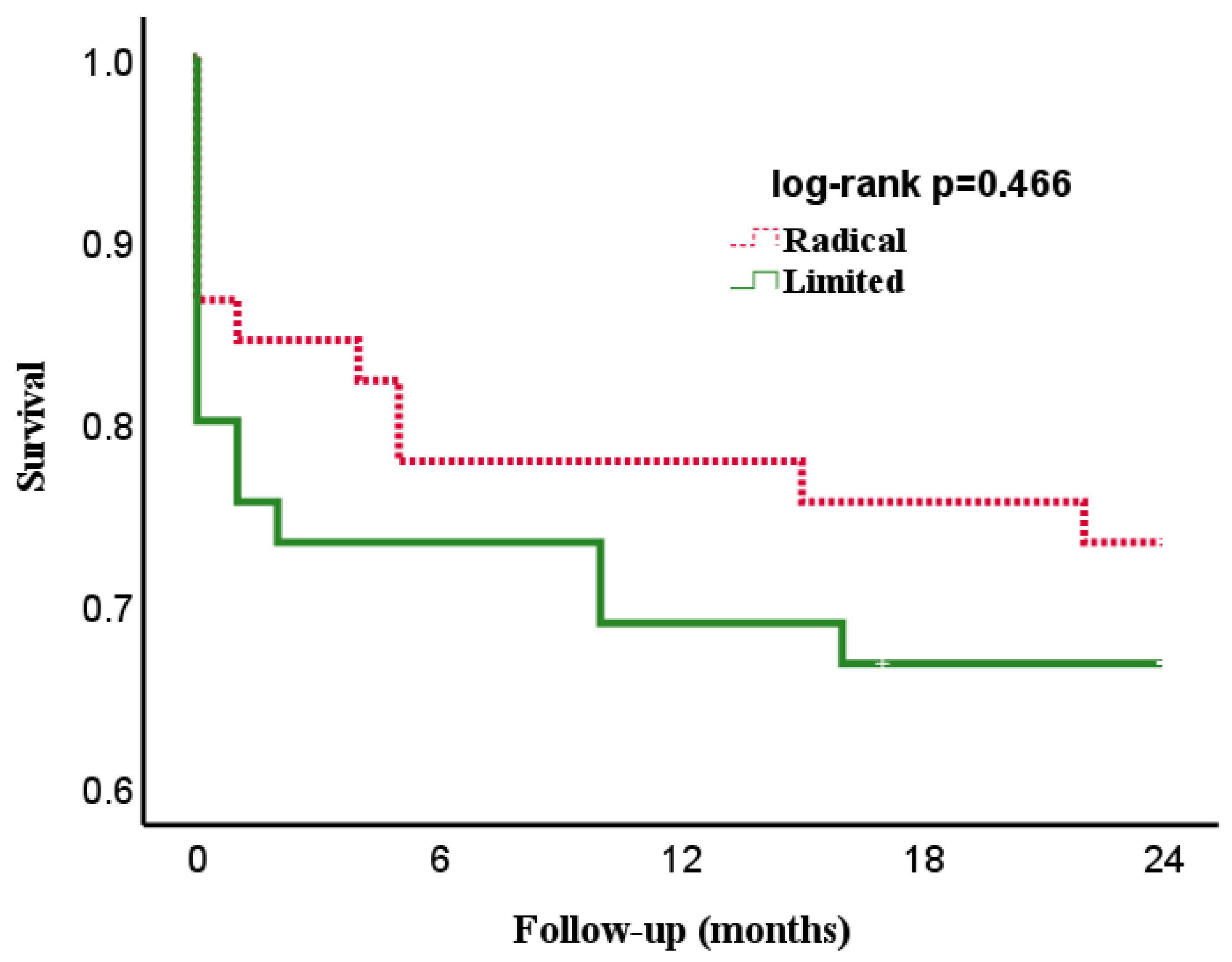
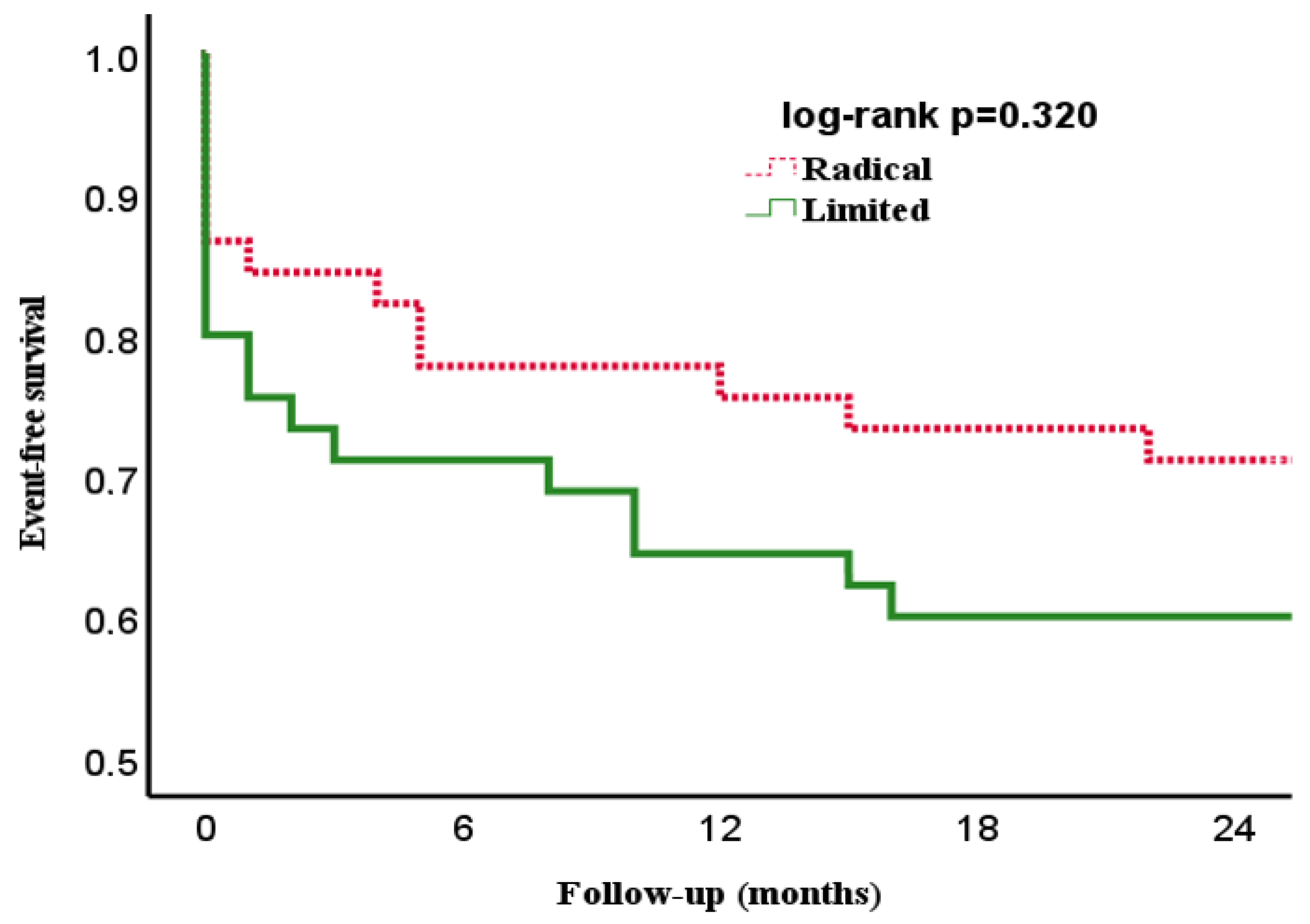
3.3. Endpoints
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhao, D.; Zhang, B. Are valve repairs associated with better outcomes than replacements in patients with native active valve endocarditis? Interact. Cardiovasc. Thorac. Surg. 2014, 19, 1036–1039. [Google Scholar] [CrossRef] [PubMed]
- Okada, Y.; Nakai, T.; Kitai, T. Role of Mitral Valve Repair for Mitral Infective Endocarditis. Cardiol. Clin. 2021, 39, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.M.; Shapiro, L.M.; Wells, F.C. Conservative Operation for Infective Endocarditis of the Mitral Valve. Ann. Thorac. Surg. 1998, 65, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Zegdi, R.; Debièche, M.; Latrémouille, C.; Lebied, D.; Chardigny, C.; Grinda, J.-M.; Chauvaud, S.; Deloche, A.; Carpentier, A.; Fabiani, J.-N. Long-Term Results of Mitral Valve Repair in Active Endocarditis. Circulation 2005, 111, 2532–2536. [Google Scholar] [CrossRef] [Green Version]
- Rostagno, C.; Carone, E.; Stefàno, P.L. Role of mitral valve repair in active infective endocarditis: Long term results. J. Cardiothorac. Surg. 2017, 12, 29. [Google Scholar] [CrossRef] [Green Version]
- Feringa, H.H.; Shaw, L.J.; Poldermans, D.; Hoeks, S.; van der Wall, E.E.; Dion, R.A.; Bax, J.J. Mitral Valve Repair and Replacement in Endocarditis: A Systematic Review of Literature. Ann. Thorac. Surg. 2007, 83, 564–570. [Google Scholar] [CrossRef]
- Alexiou, C.; Langley, S.M.; Stafford, H.; Haw, M.P.; Livesey, S.A.; Monro, J.L. Surgical treatment of infective mitral valve endocarditis: Predictors of early and late outcome. J. Heart Valve Dis. 2000, 9, 327–334. [Google Scholar]
- Muehrcke, D.D.; Cosgrove, D.M., 3rd; Lytle, B.W.; Taylor, P.C.; Burgar, A.M.; Durnwald, C.P. Is there an advantage to repairing infected mitral valves? Ann Thorac Surg. 1997, 63, 1718–1724. [Google Scholar] [CrossRef]
- Evans, C.F.; Gammie, J.S. Surgical Management of Mitral Valve Infective Endocarditis. Semin. Thorac. Cardiovasc. Surg. 2011, 23, 232–240. [Google Scholar] [CrossRef]
- Toyoda, N.; Itagaki, S.; Egorova, N.N.; Tannous, H.; Anyanwu, A.C.; El-Eshmawi, A.; Adams, D.H.; Chikwe, J. Real-world outcomes of surgery for native mitral valve endocarditis. J. Thorac. Cardiovasc. Surg. 2017, 154, 1906–1912.e9. [Google Scholar] [CrossRef] [Green Version]
- Solari, S.; De Kerchove, L.; Tamer, S.; Aphram, G.; Baert, J.; Borsellino, S.; Mastrobuoni, S.; Navarra, E.; Noirhomme, P.; Astarci, P.; et al. Active infective mitral valve endocarditis: Is a repair-oriented surgery safe and durable? Eur. J. Cardiothorac. Surg. 2019, 55, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Solari, S.; Navarra, E.; de Kerchove, L.; El Khoury, G. Mitral valve repair for endocarditis. J. Card. Surg. 2022, 37, 4097–4102. [Google Scholar] [CrossRef] [PubMed]
- Dreyfus, G.; Serraf, A.; Jebara, V.A.; Deloche, A.; Chauvaud, S.; Couetil, J.P.; Carpentier, A. Valve repair in acute endocarditis. Ann. Thorac. Surg. 1990, 49, 706–713. [Google Scholar] [CrossRef]
- Omoto, T.; Tedoriya, T.; Oi, M.; Nagai, N.; Miyauchi, T.; Ishikawa, N. Significance of mitral valve repair for active-phase infective endocarditis. Asian Cardiovasc. Thorac. Ann. 2011, 19, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Shomura, Y.; Okada, Y.; Nasu, M.; Koyama, T.; Yuzaki, M.; Murashita, T.; Fukunaga, N.; Konishi, Y. Late Results of Mitral Valve Repair With Glutaraldehyde-Treated Autologous Pericardium. Ann. Thorac. Surg. 2013, 95, 2000–2005. [Google Scholar] [CrossRef]
- Mihos, C.G.; Pineda, A.M.; Capoulade, R.; Santana, O. A Systematic Review of Mitral Valve Repair With Autologous Pericardial Leaflet Augmentation for Rheumatic Mitral Regurgitation. Ann. Thorac. Surg. 2016, 102, 1400–1405. [Google Scholar] [CrossRef] [Green Version]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, V.G., Jr.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed Modifications to the Duke Criteria for the Diagnosis of Infective Endocarditis. Clin. Infect. Dis. 2000, 30, 633–638. [Google Scholar] [CrossRef]
- El Gabry, M.; Haidari, Z.; Mourad, F.; Nowak, J.; Tsagakis, K.; Thielmann, M.; Wendt, D.; Jakob, H.; Shehada, S.E. Outcomes of mitral valve repair in acute native mitral valve infective endocarditis. Interact. Cardiovasc. Thorac. Surg. 2019, 29, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar]
- Habib, G.; Hoen, B.; Tornos, P.; Thuny, F.; Prendergast, B.; Vilacosta, I.; Moreillon, P.; de Jesus Antunes, M.; Thilen, U.; Lekakis, J. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): The Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur. Heart J. 2009, 30, 2369–2413. [Google Scholar]
- Shang, E.; Forrest, G.N.; Chizmar, T.; Chim, J.; Brown, J.M.; Zhan, M.; Zoarski, G.H.; Griffith, B.P.; Gammie, J.S. Mitral Valve Infective Endocarditis: Benefit of Early Operation and Aggressive Use of Repair. Ann. Thorac. Surg. 2009, 87, 1728–1734. [Google Scholar] [CrossRef]
- Harky, A.; Hof, A.; Garner, M.; Froghi, S.; Bashir, M. Mitral valve repair or replacement in native valve endocarditis? Systematic review and meta-analysis. J. Card. Surg. 2018, 33, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.-K.; Nesser, J.; Punzengruber, C.; Pachinger, O.; Auer, J.; Franke, H.; Hartl, P. Valvuloplasty with glutaraldehyde-treated autologous pericardium in patients with complex mitral valve pathology. Ann. Thorac. Surg. 2001, 71, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Chauvaud, S.; Jebara, V.; Chachques, J.-C.; El Asmar, B.; Mihaileanu, S.; Perier, P.; Dreyfus, G.; Relland, J.; Couetil, J.-P.; Carpentier, A. Valve extension with glutaraldehyde-preserved autologous pericardium. J. Thorac. Cardiovasc. Surg. 1991, 102, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Mayer, K.; Aicher, D.; Feldner, S.; Kunihara, T.; Schäfers, H.-J. Repair versus replacement of the aortic valve in active infective endocarditis. Eur. J. Cardio-Thoracic. Surg. 2012, 42, 122–127. [Google Scholar] [CrossRef]
- Nierhaus, A.; Morales, J.; Wendt, D.; Scheier, J.; Gutzler, D.; Jarczak, D.; Born, F.; Hagl, C.; Deliargyris, E.; Mehta, Y. Comparison of the CytoSorb((R)) 300 mL and Jafron HA380 hemoadsorption devices: An in vitro study. Minim. Invasive Ther. Allied Technol. 2022, 31, 1058–1065. [Google Scholar] [CrossRef]
- Haidari, Z.; Wendt, D.; Thielmann, M.; Mackowiak, M.; Neuhäuser, M.; Jakob, H.; Ruhparwar, A.; El-Gabry, M. Intraoperative Hemoadsorption in Patients With Native Mitral Valve Infective Endocarditis. Ann. Thorac. Surg. 2020, 110, 890–896. [Google Scholar] [CrossRef]
- Haidari, Z.; Demircioglu, E.; Boss, K.; Tyczynski, B.; Thielmann, M.; Schmack, B.; Kribben, A.; Weymann, A.; El Gabry, M.; Ruhparwar, A.; et al. Intraoperative hemoadsorption in high-risk patients with infective endocarditis. PLoS ONE 2022, 17, e0266820. [Google Scholar] [CrossRef]
- Kalisnik, J.M.; Leiler, S.; Mamdooh, H.; Zibert, J.; Bertsch, T.; Vogt, F.A.; Bagaev, E.; Fittkau, M.; Fischlein, T. Single-Centre Retrospective Evaluation of Intraoperative Hemoadsorption in Left-Sided Acute Infective Endocarditis. J. Clin. Med. 2022, 11, 3954. [Google Scholar] [CrossRef]
- Diab, M.; Lehmann, T.; Bothe, W.; Akhyari, P.; Platzer, S.; Wendt, D.; Deppe, A.-C.; Strauch, J.; Hagel, S.; Günther, A.; et al. Cytokine Hemoadsorption During Cardiac Surgery Versus Standard Surgical Care for Infective Endocarditis (REMOVE): Results From a Multicenter Randomized Controlled Trial. Circulation 2022, 145, 959–968. [Google Scholar] [CrossRef]
- Haidari, Z.; Leiler, S.; Mamdooh, H.; Fittkau, M.; Boss, K.; Tyczynski, B.; Thielmann, M.; Bagaev, E.; El Gabry, M.; Wendt, D.; et al. Effect of intraoperative hemoadsorption therapy in cardiac surgery for active infective endocarditis with confirmed staphylococcus aureus bacteremia. Interdiscip. CardioVascular Thorac. Surgery 2023, 36, ivad010. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Limited-Resection n = 45 | Radical-Resection n = 45 | p |
|---|---|---|---|
| Demographics | |||
| Age, years ± SD | 60 ± 14 | 62 ± 13 | 0.446 |
| Gender, female, n (%) | 15 (33) | 16 (36) | 0.824 |
| Diabetes, n (%) | 10 (22) | 12 (27) | 0.624 |
| Drug abuse, n (%) | 3 (7) | 1 (2) | 0.616 |
| Previous stroke, n (%) | 18 (40) | 16 (36) | 0.664 |
| - Endocarditis related, n | 17 | 15 | 0.660 |
| - Neurologic dysfunction, n | 13 | 12 | 0.814 |
| CAD, n (%) | 10 (22) | 11 (24) | 0.803 |
| Atrial fibrillation, n (%) | 12 (27) | 13 (29) | 0.814 |
| Pulmonary disease, n (%) | 6 (13) | 6 (13) | >0.999 |
| Dialysis, n (%) | 4 (9) | 7 (16) | 0.334 |
| Liver disease, n (%) | 4 (9) | 2 (4) | 0.677 |
| PVD, n (%) | 6 (13) | 7 (16) | 0.764 |
| Previous CABG, n (%) | 3 (7) | 3 (7) | >0.999 |
| Previous PCI, n (%) | 2 (4) | 3 (7) | >0.999 |
| Previous valve surgery, n (%) | 3 (7) | 4 (9) | >0.999 |
| EuroSCORE II, mean ± SEM | 10 ± 2 | 11 ± 2 | 0.642 |
| Clinical status | |||
| NYHA fc III-IV, n (%) | 25 (56) | 21 (47) | 0.399 |
| Intubated, n (%) | 5 (11) | 4 (9) | 0.725 |
| Vasopressor need, n (%) | 5 (11) | 5 (11) | >0.999 |
| Surgical delay, days ± SD | 16 ± 2 | 17 ± 3 | 0.940 |
| Inflammatory status | |||
| CRP, mg/dL (IQR) | 4.90 (1.95–10.25) | 5.00 (1.95–8.55) | 0.692 |
| PCT, ng/mL (IQR) | 0.21 (0.08–0.36) | 0.28 (0.14–0.61) | 0.199 |
| WBC, 109/L (IQR) | 8.24 (5.56–11.52) | 8.60 (6.56–12.27) | 0.169 |
| Echocardiographic parameters | |||
| LVEF > 50%, n (%) | 35 (78) | 39 (87) | 0.270 |
| Severe MR, n (%) | 24 (53) | 33 (73) | 0.049 |
| Concomitant AV IE, n (%) | 8 | 12 | 0.310 |
| Concomitant TV IE, n (%) | 3 | 2 | >0.999 |
| Variables | Limited-Resection n = 45 | Radical-Resection n = 45 | p |
|---|---|---|---|
| Causative microorganism | |||
| Staphylococcus species, n (%) | 19 (42) | 11 (24) | 0.074 |
| - Staphylococcus aureus, n | 13 | 8 | 0.213 |
| Streptococcus species, n (%) | 5 (11) | 12 (27) | 0.059 |
| Enterococcus species, n (%) | 5 (11) | 6 (13) | 0.748 |
| Others, n (%) | 4 (9) | 4 (9) | >0.999 |
| Negative, n (%) | 12 (27) | 12 (27) | >0.999 |
| Indication for surgery | |||
| Heart failure, n (%) | 8 (18) | 16 (36) | 0.057 |
| Large or embolized vegetation, n (%) | 28 (62) | 19 (42) | 0.058 |
| Uncontrolled infection, n (%) | 8 (18) | 8 (18) | >0.999 |
| Valvular disease, n (%) | 1 (2) | 2 (4) | >0.999 |
| Timing of surgery | |||
| Elective (>7 days), n (%) | 34 (76) | 31 (69) | 0.480 |
| Urgent (2–7 days), n (%) | 7 (15) | 8 (18) | 0.777 |
| Emergent (<2 days), n (%) | 4 (9) | 6 (13) | 0.502 |
| Variables | Limited-Resection n = 45 | Radical-Resection n = 45 | p |
|---|---|---|---|
| Isolated mitral valve surgery, n (%) | 24 (53) | 16 (36) | 0.090 |
| Concomitant CABG, n (%) | 4 (9) | 7 (16) | 0.334 |
| Concomitant AV surgery, n (%) | 13 (29) | 15 (33) | 0.649 |
| Concomitant TV surgery, n (%) | 5 (11) | 7 (16) | 0.535 |
| Minimally invasive, n (%) | 2 (4) | 6 (13) | 0.266 |
| CPB time, minutes (IQR) | 92 (73–117) | 128 (111–172) | <0.001 |
| ACC time, minutes (IQR) | 59 (45–78) | 84 (73–121) | <0.001 |
| Variables | Limited-Resection n = 45 | Radical-Resection n = 45 | p |
|---|---|---|---|
| Primary | |||
| Repair rate, n (%) | 38 (84) | 8 (18) | <0.001 |
| Mortality (30-Day), n (%) | 11 (24) | 6 (13) | 0.178 |
| - Sepsis-related, n | 6 | 6 | >0.999 |
| Secondary | |||
| Mortality (2-Year), n (%) | 15 (33) | 12 (26) | 0.490 |
| Re-endocarditis, n (%) | 2 (4) | 4 (9) | 0.677 |
| Re-operation, n (%) | 3 (7) | - | 0.242 |
| Postoperative IABP, n (%) | 2 (4) | 2 (4) | >0.999 |
| Postoperative ECMO, n (%) | - | 2 (4) | 0.494 |
| Dialysis, n (%) | 9 (20) | 11 (24) | 0.612 |
| Reintubation, n (%) | 5 (11) | 13 (29) | 0.035 |
| ICU-stay, days (IQR) | 5 (2–10) | 6 (4–11) | 0.129 |
| Hospital stay, days (IQR) | 13 (10–21) | 14 (9–20) | 0.771 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haidari, Z.; Wendt, D.; Thielmann, M.; Jakob, H.; Ruhparwar, A.; El-Gabry, M. Limited versus Radical Resection in Mitral Valve Infective Endocarditis Surgery. J. Cardiovasc. Dev. Dis. 2023, 10, 146. https://doi.org/10.3390/jcdd10040146
Haidari Z, Wendt D, Thielmann M, Jakob H, Ruhparwar A, El-Gabry M. Limited versus Radical Resection in Mitral Valve Infective Endocarditis Surgery. Journal of Cardiovascular Development and Disease. 2023; 10(4):146. https://doi.org/10.3390/jcdd10040146
Chicago/Turabian StyleHaidari, Zaki, Daniel Wendt, Matthias Thielmann, Heinz Jakob, Arjang Ruhparwar, and Mohamed El-Gabry. 2023. "Limited versus Radical Resection in Mitral Valve Infective Endocarditis Surgery" Journal of Cardiovascular Development and Disease 10, no. 4: 146. https://doi.org/10.3390/jcdd10040146