1. Introduction
Spain was one of the countries more severely affected by the first COVID-19 wave [
1]. To accommodate the unprecedented stress to treat the unexpected and extraordinarily high number of patients during the first wave in March 2020, hospitals had to quickly re-organize, dedicating almost all hospital resources to treating patients with SARS-CoV-2 and canceling most programmed admissions. The immediate consequence was a reduction even in cases requiring emergency interventions [
2]. Prioritization among patients with heart diseases requiring coronary revascularizations has represented a difficult issue during the COVID-19 pandemic [
3]. After that first wave, hospitals established new COVID-19-negative units for the care of patients requiring non-COVID-19 related care, including coronary revascularization for the delivery of safe and effective care even in the epicenter of the pandemic. The late effects of the postponement of coronary revascularizations are not clearly determined [
4,
5].
Percutaneous coronary intervention (PCI) and coronary artery bypass grafts (CABG) are the two main techniques used for revascularization procedures for patients with chronic coronary artery disease. Both procedures have been showing different trends in their utilization in Spain in recent years: on the one hand, in the last two decades, PCI showed a three times increase, whereas, on the other hand, the proportions of CABG reduced by 27% [
6].
Interrupted time series (ITS) analysis has been proposed as a robust design to evaluate the impact of interventions when their implementation occurs at a concrete moment in time [
7,
8]. For this, it is necessary to have the observed data of the variable of interest during a period (time series) that includes measurements both before and after the application of the intervention, which is the moment of interruption of the series. The effects of the intervention are assessed by changes in the level and slope of the time series, as well as by the statistical significance of the different model parameters.
Given the uncontrolled COVID-19 epidemiological situation, on 14 March 2020, the government approved declaring a state of alarm throughout the Spanish territory to deal with the health emergency caused by COVID-19. The state of alarm was extended until 00:00 on 21 June 2020 [
9]. After the first period of the pandemic, hospitals were returning to usual care.
This work aims to explore the effect that the COVID-19 pandemic had on the use of revascularization procedures in Spain, both in utilization rates and also assessing the risk profiles of patients receiving both PCI and CABG, comparing the periods before and after March 2020, when the Spanish government introduced the state of alarm.
2. Materials and Methods
2.1. Study Design and Population
We conducted a descriptive epidemiological study using the SNHDD. The SNHDD is an administrative database managed by the Spanish Ministry of Health (SMH) that collects information from all private and public hospitals. These hospitals are required by law to provide data from all subjects hospitalized for at least 24 h. The following variables for each patient are included in the SNHDD: age, sex, place of residence, dates of admission and discharge, discharge destination, primary diagnosis, secondary diagnosis (up to a maximum of 19), and procedures (therapeutic or diagnostic) conducted during the hospitalization period (up to a maximum of 20). The SNHDD applies the International Classification of Disease Tenth Revision (ICD10) to codify diagnoses and procedures. Details on the SNHDD can be found online [
10]. In this work, we evaluated patients registered in the Spanish National Hospital Discharge Database (SNHDD) with a code indicating they underwent PCI or CABG during the 5-year period, from January 2016 to December 2020.
2.2. Statistical Analysis
An ITS analysis was performed with the data. First, a descriptive analysis of the data was conducted. The risk profile of each individual patient is based on the predicted probability of death in patients who underwent CABG and PCI. The analysis was conducted on two cohorts: patients who underwent PCI and CABG separately. The risk profile was determined by estimating the probability of death for each patient obtained through a logistic regression model, using the patient discharge status (dead or alive) as an outcome variable. The variables included in those models to estimate the risk of death were age, sex, admission to ICU, severity, mortality risk, and Elixhauser Comorbidity Index. The Elixhauser Comorbidity Index is a system for classifying a patient’s comorbidities using ICD diagnosis codes from administrative data sources, such as hospital abstracts. The categories are binary and indicate the presence or absence of a comorbidity. The index can be used to anticipate hospital resource utilization and in-hospital death rates [
11]. This statistical analysis was performed via IBM SPSS Statistics, version 26.
The time intervals were 60 months in a five-year period from 2016 to 2020. Segmented regression analysis was used as a method of modeling the time series. First, time series were checked for seasonality and were non-stationary. The patterns of each are clearly seen on the decomposition plots in
Figure 1. The seasonality of the series was controlled using the “seasonal” adjustment function in RStudio during the plot construction. However, an ordinary least squares function with the addition of dummy variables for months from January to November was used to adjust the model for seasonality in order to determine the coefficients. The general time series model was as follows:
where t refers to month t;
deathprobt is the estimated probability of death;
emergencyt is a dummy variable equal to 0 until March 2020, but equal to 1 from April 2020 onward;
β0 is the intercept and corresponds to the death probability in January 2016;
β1 is the slope of the trend before the intervention;
β2 is the change in the level caused by the intervention;
β3 is the change in the trend of the slope, caused by the intervention;
The interrupted time series analysis was conducted in the RStudio 2022.07.1 + 554.
3. Results
Data from 306,910 patients who underwent PCI or CABG during the 5-year period from January 2016 to December 2020 were included in this analysis. The overall PCI and CABG procedures analyzed in this study are shown in
Figure 1. The main characteristics of the patients receiving either procedure are shown in the
Supplementary Table.
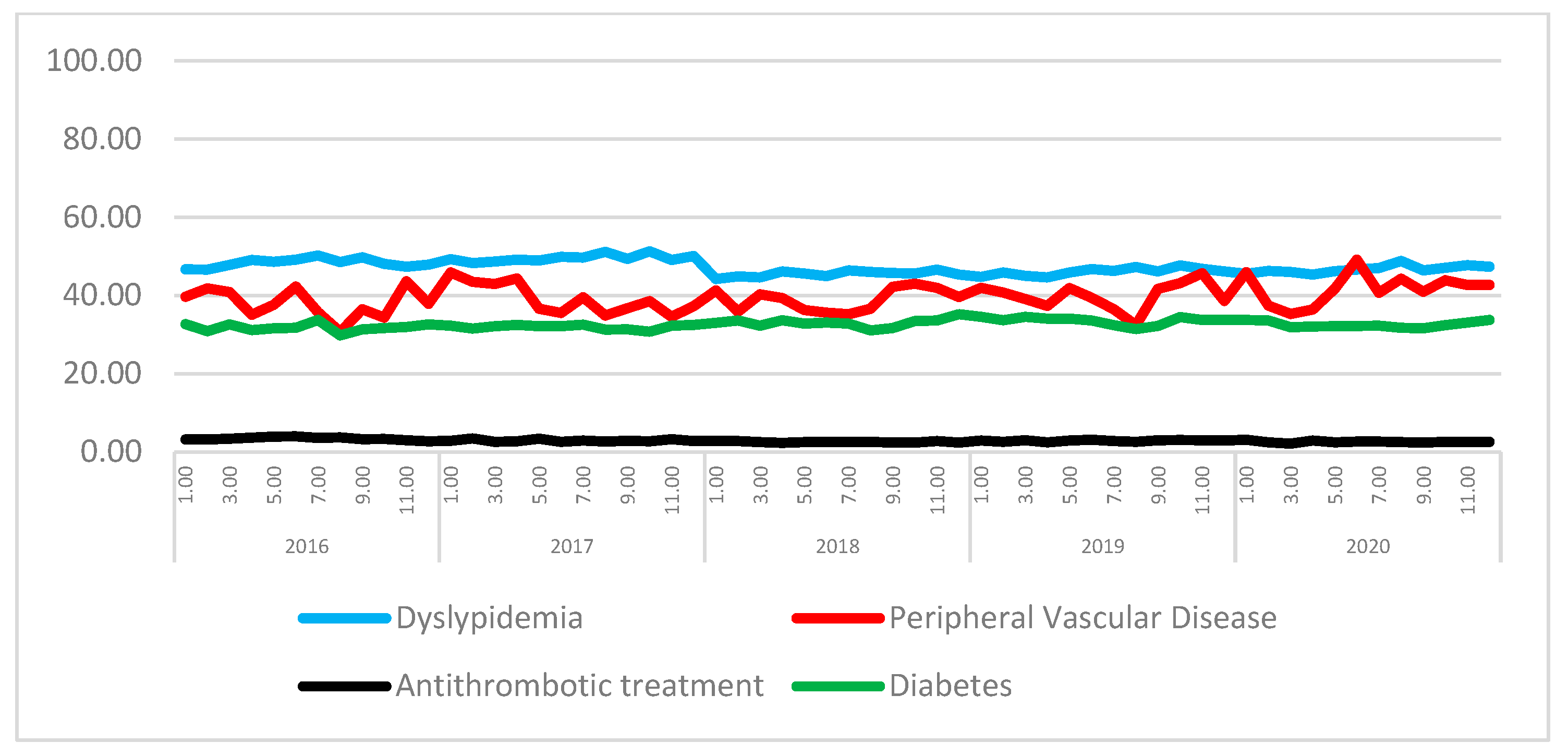
Figure 2 shows the time trend of significant coronary factors, including the antithrombotic treatment of patients with coronary revascularizations.
The logistic regression model to determine the risk profile for PCI was overall statistically significant, ( (8) = 17,520.740, p < 0.001), explained with 42.3% (Nagelkerke R2), and correctly predicted 97.5% of cases. Age (p < 0.001), gender (p < 0.001), severity (p < 0.001), risk mortality, and Elixhauser comorbidity index were all significant in the predicted probability of death in PCI patients.
Turning to the predicted probability of death in CABG patients, the model was overall statistically significant, ( (8) = 3180.226, p < 0.001), explained with 32.3% (Nagelkerke R2), and correctly predicted 95.6% of cases. Age (p < 0.001), gender (p < 0.001), severity (p < 0.001), risk mortality, and Elixhauser Comorbidity Index were all significant but admission to ICU (p = 0.116) was not.
It was found that time series had seasonality and were non-stationary. The patterns of each are clearly seen on the decomposition plots in
Figure 3.
General models of segmented regression equations:
It is clearly seen graphically from
Figure 4, that the predicted probability of death among the CABG patients rose slightly during the period of five years from January 2016 to December 2020, from 0.028 to 0.038, respectively. After adjusting for seasonality, the model shows that there was a statistically significant change in level by 2.512 × 10
−3 after the introduction of the lockdown (estimate = 2.512 × 10
−3; Std. error = 1.056 × 10
−3; t value = 2.379; Pr(>|t|) = 0.02164) (
Table 1).
The joint hypothesis test robust to autocorrelation and heteroskedasticity rejected the null hypothesis for both CABG (4.204 × 10
−7) and PCI (3.531 × 10
−7) (
Table 2). Thus, dummy variables in the unrestricted models statistically significantly enhance the general fit of the model.
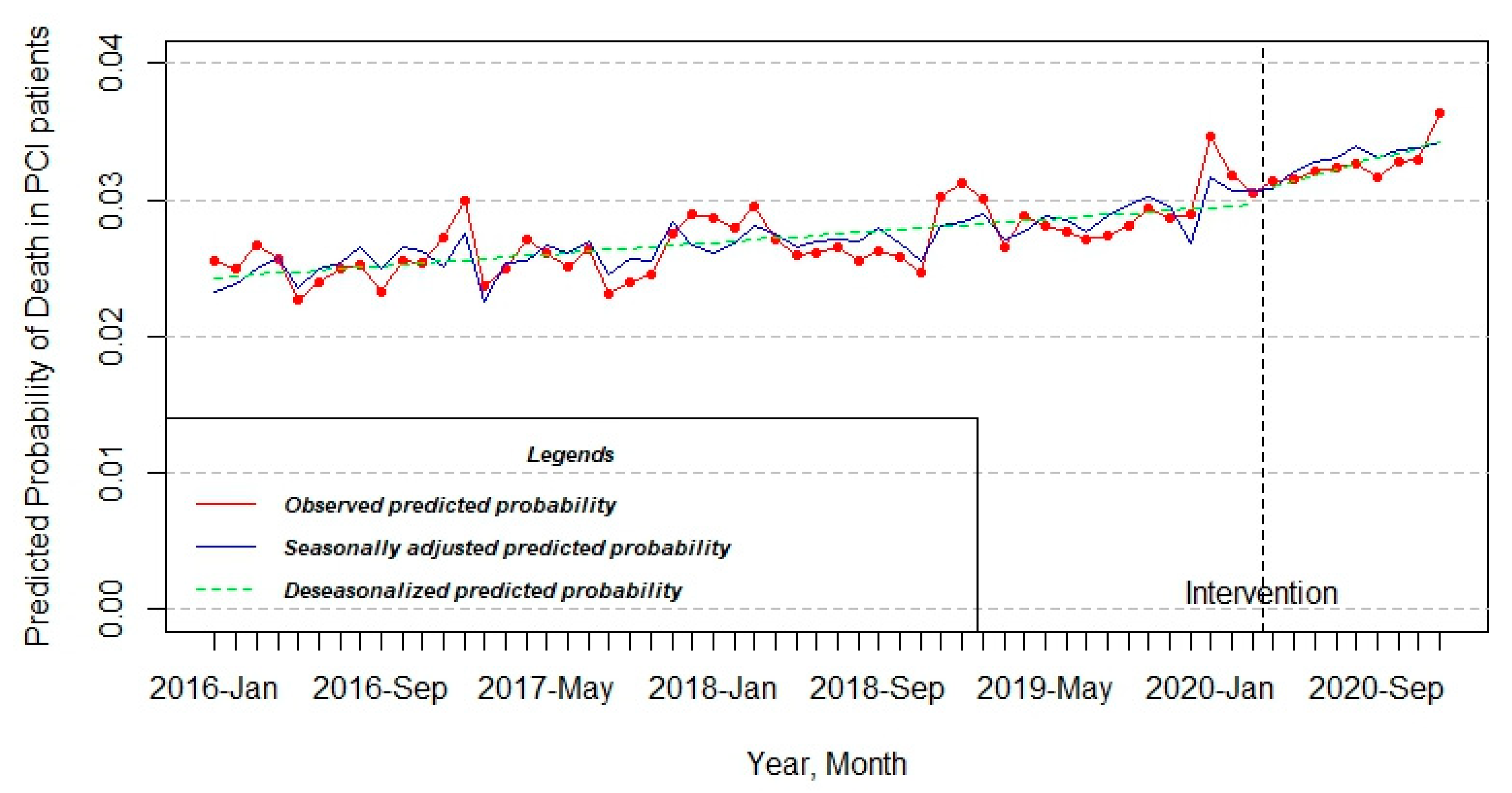
The pattern of the PCI model also experienced a little increase in the observed predicted probability throughout half a decade from 0.025 to 0.036. On the other hand, the change at that level was not statistically significant after the approval of intervention (estimate = 1.747 × 10
−3; Std. error = 1.089 × 10
−3; t value = 1.604; Pr(>|t|) = 0.115772) (
Table 1 and
Figure 5).
4. Discussion
The main finding of this work is that the outbreak of COVID-19 in Spain did have an initial significant reduction in the volume of coronary revascularizations but did not influence the risk profile of patients admitted for PCI, and it showed a small, although significant, level effect in the risk profile of CABG in Spanish hospitals.
With the first wave of COVID-19 cases, hospitals were forced to abruptly reduce admissions for the care of non-COVID-19 patients, including patients with chronic ischemic disease [
12], but our data suggest that the reduction was not associated with lower severity of cases for PCI, whereas it showed an increase for patients admitted for surgical revascularizations associated with the abrupt COVID-19 hospital reorganizations.
The results from ITS models reveal, interestingly, that already before the March 2020 surge in COVID-19 cases and the introduction of lockdowns and state of alarm in Spain, there was an increase in patients’ risk profiles receiving either PCI or CABG. The significant time effect observed reflects that cardiologists’ and cardiac surgeons’ decision-making regarding indications for both revascularization procedures were already selecting more severe at-risk patients.
What is also quite an interesting finding is the seasonality of time series in both the PCI and CABG models. Specifically, our study uncovers seasonality in the risk profiles of treated patients. A study by Stewart et al. (2017) supports our finding by mentioning that the majority of studies state higher hospitalization and mortality frequency during the winter months in comparison to summer periods. They also suggest that the reason behind this issue is multifactorial and may be related to physiological responses to cold and heat, behavioral changes in particular seasons, vitamin D deficiency, ambient air pollutants, and susceptibility to infectious diseases [
13].
ITS represents a valuable study design to assess the effect of population-based interventions when randomization is not possible or feasible. Natural experiments could be considered for evaluating health or other outcomes where exposure to the event of the intention of interest has not been manipulated by the researcher [
14]. Natural experiments require clever approaches to analyzing data, such as comparing what happened before and after lockdowns using methods that could include interrupted time series, or between a population that was subject to lockdown and another that was not, which can serve as a control [
15].
The pandemic has created a natural experiment of unprecedented proportions. The COVID-19 pandemic has resulted in considerable delays and affected the patients’ clinical profiles due to the implementation of restrictive measures in cardiac revascularization units [
16], but it also provided this opportunity to assess the dynamics of the risk profile of patients receiving coronary revascularizations.
A common finding observed during the COVID-19 pandemic is a reduction in revascularization volumes, whereas some authors have found higher risk-adjusted mortality [
17] and others have not [
18]. This study did not aim to explore the mortality of patients and has some limitations. The most important is that the post-COVID-19 period includes only nine observations. Another relevant limitation is the capacity of administrative data to capture appropriate clinical variables reflecting the severity of chronic coronary patients. Additionally, this study analyzes national data, and the observed effects may have regional or local differences.
5. Conclusions
The abrupt reorganization of hospital care that represented the first wave of COVID–19 in March 2020 in Spain led to a reduction in cases, which was accompanied by an increase in the risk profile of CABG patients but not PCI. On the other hand, the risk profile of both coronary revascularization procedures began before the pandemic, showing a significant temporal trend toward an increase in the risk profile. Further efforts should be aimed at studying and validating our results and evaluating other databases, regions, or countries.
Author Contributions
Conceptualization, A.S.-S. and A.A.; validation, A.S.-S. and A.P.; formal analysis, A.P. and D.Y.; data curation, A.S.-S., D.Y., A.P. and A.A.; writing—original draft preparation, A.S.-S. and A.P.; writing—review and editing, A.A., M.A.O., D.Y. and S.Z.; visualization, A.S.-S. and A.P.; supervision, A.S.-S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Nazarbayev University, grant number 021220CRP0822.
Institutional Review Board Statement
This study did not require ethical approval.
Informed Consent Statement
As this study relied on a fully anonymized dataset, it did not require full committee review, ongoing review, or informed consent.
Data Availability Statement
The data used to support the findings of the present study are available from the corresponding author upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Artiga-Sainz, L.M.; Sarria-Santamera, A.; Martínez-Alés, G.; Quintana-Díaz, M. New Approach to Managing the COVID-19 Pandemic in a Complex Tertiary Care Medical Center in Madrid, Spain. Disaster Med. Public Health Prep. 2022, 16, 2097–2102. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, S.; Shin, J.-H.; Morishita, T.; Takada, D.; Kunisawa, S.; Imanaka, Y. Medium-term impact of the coronavirus disease 2019 pandemic on the practice of percutaneous coronary interventions in Japan. J. Atheroscler. Thromb. 2021, 29, 1571–1587. [Google Scholar] [CrossRef] [PubMed]
- Keskin, G.; Khalil, E.; Uysal, A. Should we postpone elective cardiovascular procedures and percutaneous coronary interventions during the COVID-19 Pandemic? Heart Surg. Forum 2021, 24, E022–E030. [Google Scholar] [CrossRef] [PubMed]
- Ball, S.; Banerjee, A.; Berry, C.; Boyle, J.R.; Bray, B.; Bradlow, W.; Chaudhry, A.; Crawley, R.; Danesh, J.; Denniston, A.; et al. Monitoring indirect impact of COVID-19 pandemic on services for cardiovascular diseases in the UK. Heart 2020, 106, 1890–1897. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, M.O.; Banerjee, A.; Clarke, S.; de Belder, M.; Patwala, A.; Goodwin, A.T.; Kwok, C.S.; Rashid, M.; Gale, C.P.; Curzen, N.; et al. Impact of COVID-19 on cardiac procedure activity in England and associated 30-day mortality. Eur. Heart, J. Qual. Care Clin. Outcomes 2021, 7, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Carnero Alcazar, M.; Hernandez-Vaquero, D.; Cubero-Gallego, H.; Menendez, J.L.; Piñon, M.; Martin, J.A.; Caballero, G.C.; Carnicer, J.C.; Villamor, C.; Forteza, A.; et al. Retrospective cohort analysis of Spanish national trends of coronary artery bypass grafting and percutaneous coronary intervention from 1998 to 2017. BMJ Open 2021, 11, e046141. [Google Scholar] [CrossRef] [PubMed]
- Penfold, R.B.; Zhang, F. Use of Interrupted Time Series Analysis in Evaluating Health Care Quality Improvements. Acad. Pediatr. 2013, 13 (Suppl. S6), S38–S44. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2017, 46, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Real Decreto 463/2020, de 14 de Marzo, Por el Que se Declara el Estado de Alarma Para la Gestión de la Situación de Crisis Sanitaria Ocasionada Por el COVID-19. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-2020-3692 (accessed on 2 November 2022).
- Ministerio de Sanidad, Consumo y Bienestar Social. Spanish Register of Specialized Care-Basic Minimum Database [Registro de Actividad de Atención Especializada. RAE-CMBD]. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/cmbdhome.htm (accessed on 2 November 2022).
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity measures for use with administrative data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef] [PubMed]
- Tam, D.Y.; Qiu, F.; Manoragavan, R.; Fremes, S.E.; Hassan, A.; Ko, D.T.; Lauck, S.B.; Naimark, D.; Ouzounian, M.; Sander, B.; et al. The Impact of the COVID-19 Pandemic on Cardiac Procedure Wait List Mortality in Ontario, Canada. Can. J. Cardiol. 2021, 37, 1547–1554. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Keates, A.K.; Redfern, A.; McMurray, J.J. Seasonal variations in cardiovascular disease. Nat. Rev. Cardiol. 2017, 14, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Cooper, C.; Gunnell, D.; Haw, S.; Lawson, K.; Macintyre, S.; Ogilvie, D.; Petticrew, M.; Reeves, B.; Sutton, M.; et al. Using natural experiments to evaluate population health interventions: New medical research council guidance. J. Epidemiol. Commun. Health 2012, 66, 1182–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, J. Pandemic upheaval offers a huge natural experiment. Nature 2021, 596, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Roussakis, A.; Boumpoulis, K.; Nenekidis, I.; Gavalaki, A.; Petsios, K.; Dimopoulos, S.; Bisiadis, I.; Rellia, P.; Perreas, K. Trends regarding the profile of cardiac surgery patients during the first wave of COVID-19 pandemic in Greece. Braz. J. Cardiovasc. Surg. 2022, 37, 418–421. [Google Scholar] [CrossRef] [PubMed]
- Azzalini, L.; Seth, M.; Sukul, D.; Valle, J.A.; Daher, E.; Wanamaker, B.; Tucciarone, M.T.; Zaitoun, A.; Madder, R.D.; Gurm, H.S. Trends and outcomes of percutaneous coronary intervention during the COVID-19 pandemic in Michigan. PLoS ONE 2022, 17, e0273638. [Google Scholar] [CrossRef]
- Ramzy, J.; Martin, C.A.; Burgess, S.; Gooley, R.; Zaman, S. COVID-19 Pandemic Impact on Percutaneous Coronary Intervention for Acute Coronary Syndromes: An Australian Tertiary Centre Experience. Heart Lung Circ. 2022, 31, 787–794. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}