

Revolutionizing the Management of Large-Core Ischaemic Strokes: Decoding the Success of Endovascular Therapy in the Recent Stroke Trials
 , , , ,
, , , ,
Abstract
:1. Defining the Role of EVT in Large Infarct Core Strokes
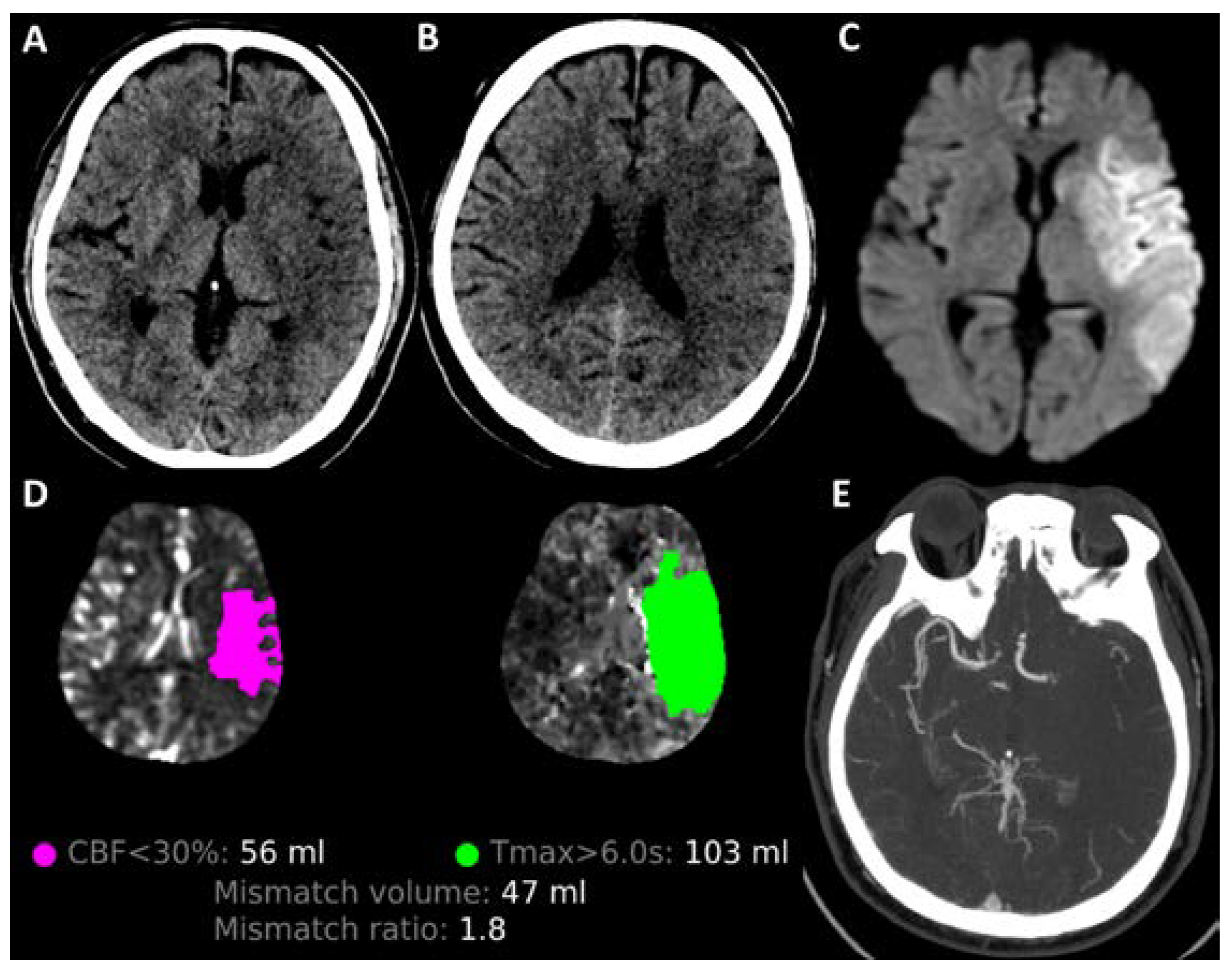
2. Imaging Considerations in Large Infarct Core Strokes
3. HERMES Pooled Data and Meta-Analysis Preceding the RCTs
4. RESCUE-Japan LIMIT RCT
5. ANGEL-ASPECT RCT
6. SELECT2 RCT
7. TENSION RCT
8. TESLA RCT
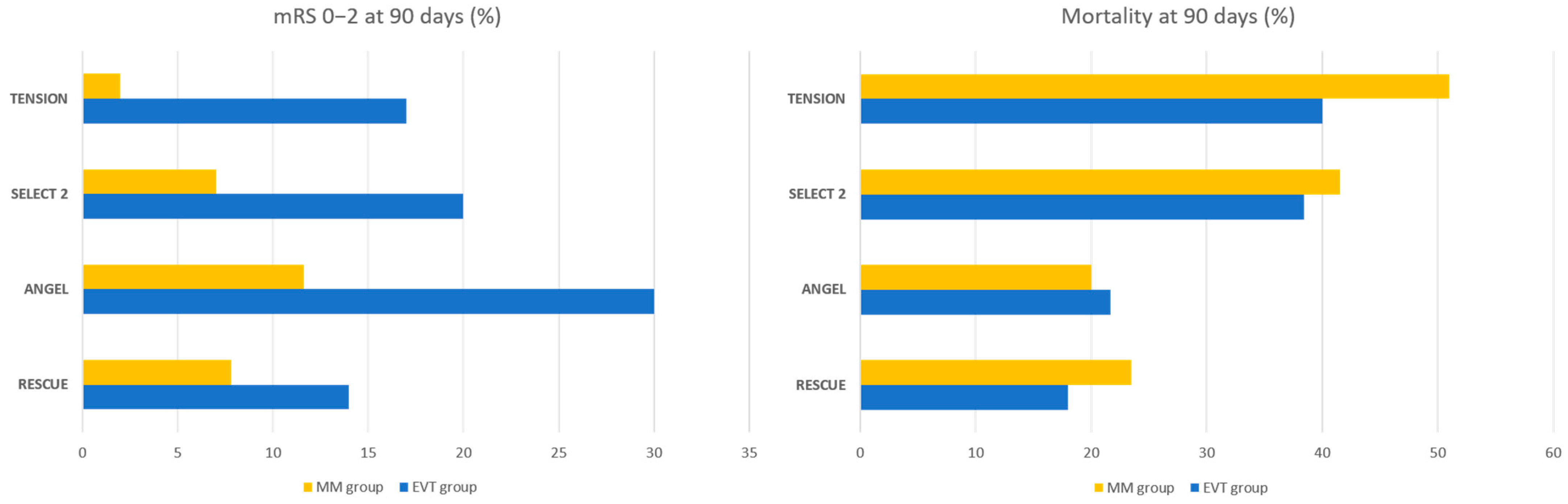
9. Summary and Discussion of Key Findings
10. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berkhemer, O.A.; Fransen, P.S.S.; Beumer, D.; van den Berg, L.A.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.H.; et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.C.V.; Mitchell, P.J.; Kleinig, T.J.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.J.; Parsons, M.W.; Oxley, T.J.; et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; de Miquel, M.A.; Molina, C.A.; Rovira, A.; Román, L.S.; Serena, J.; Abilleira, S.; Ribó, M.; et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef]
- Saver, J.L.; Goyal, M.; Bonafe, A.; Diener, H.-C.; Levy, E.I.; Pereira, V.M.; Albers, G.W.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N. Engl. J. Med. 2015, 372, 2285–2295. [Google Scholar] [CrossRef] [PubMed]
- Emberson, J.; Lees, K.R.; Lyden, P.; Blackwell, L.; Albers, G.; Bluhmki, E.; Brott, T.; Cohen, G.; Davis, S.; Donnan, G.; et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: A meta-analysis of individual patient data from randomised trials. Lancet 2014, 384, 1929–1935. [Google Scholar] [CrossRef]
- Bracard, S.; Ducrocq, X.; Mas, J.L.; Soudant, M.; Oppenheim, C.; Moulin, T.; Guillemin, F.; THRACE investigators. Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke (THRACE): A randomised controlled trial. Lancet Neurol. 2016, 15, 1138–1147. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.J.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.L.M.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N. Engl. J. Med. 2018, 378, 708–718. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef]
- Sarraj, A.; Hassan, A.E.; Savitz, S.; Sitton, C.; Grotta, J.; Chen, P.; Cai, C.; Cutter, G.; Imam, B.; Redd, S.; et al. Outcomes of Endovascular Thrombectomy vs Medical Management Alone in Patients with Large Ischemic Cores: A Secondary Analysis of the Optimizing Patient’s Selection for Endovascular Treatment in Acute Ischemic Stroke (SELECT) Study. JAMA Neurol. 2019, 76, 1147–1156. [Google Scholar] [CrossRef] [PubMed]
- Rebello, L.C.; Bouslama, M.; Haussen, D.C.; Dehkharghani, S.; Grossberg, J.A.; Belagaje, S.; Frankel, M.R.; Nogueira, R.G. Endovascular Treatment for Patients with Acute Stroke Who Have a Large Ischemic Core and Large Mismatch Imaging Profile. JAMA Neurol. 2017, 74, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Román, L.S.; Menon, B.K.; Blasco, J.; Hernández-Pérez, M.; Dávalos, A.; Majoie, C.B.L.M.; Campbell, B.C.V.; Guillemin, F.; Lingsma, H.; Anxionnat, R.; et al. Imaging features and safety and efficacy of endovascular stroke treatment: A meta-analysis of individual patient-level data. Lancet Neurol. 2018, 17, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Mourand, I.; Abergel, E.; Mantilla, D.; Ayrignac, X.; Sacagiu, T.; Eker, O.F.; Gascou, G.; Dargazanli, C.; Riquelme, C.; Moynier, M.; et al. Favorable revascularization therapy in patients with ASPECTS ≤ 5 on DWI in anterior circulation stroke. J. Neurointerv. Surg. 2018, 10, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Mokin, M.; Primiani, C.T.; Siddiqui, A.H.; Turk, A.S. ASPECTS (Alberta Stroke Program Early CT Score) Measurement Using Hounsfield Unit Values When Selecting Patients for Stroke Thrombectomy. Stroke 2017, 48, 1574–1579. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, J.M.; Farrall, A.J.; Perry, D.; von Kummer, R.; Mielke, O.; Moulin, T.; Ciccone, A.; Hill, M.; Acute Cerebral CT Evaluation of Stroke Study (ACCESS) Study Group. Factors Influencing the Detection of Early CT Signs of Cerebral Ischemia. Stroke 2007, 38, 1250–1256. [Google Scholar] [CrossRef]
- Nezu, T.; Koga, M.; Nakagawara, J.; Shiokawa, Y.; Yamagami, H.; Furui, E.; Kimura, K.; Hasegawa, Y.; Okada, Y.; Okuda, S.; et al. Early ischemic change on CT versus diffusion-weighted imaging for patients with stroke receiving intravenous recombinant tissue-type plasminogen activator therapy: Stroke acute management with urgent risk-factor assessment and improvement (SAMURAI) rt-PA registry. Stroke 2011, 42, 2196–2200. [Google Scholar] [CrossRef]
- Fiebach, J.B.; Schellinger, P.D.; Jansen, O.; Meyer, M.; Wilde, P.; Bender, J.; Schramm, P.; Jüttler, E.; Oehler, J.; Hartmann, M.; et al. CT and diffusion-weighted MR imaging in randomized order: Diffusion-weighted imaging results in higher accuracy and lower interrater variability in the diagnosis of hyperacute ischemic stroke. Stroke 2002, 33, 2206–2210. [Google Scholar] [CrossRef]
- Hoelter, P.; Muehlen, I.; Goelitz, P.; Beuscher, V.; Schwab, S.; Doerfler, A. Automated ASPECT scoring in acute ischemic stroke: Comparison of three software tools. Neuroradiology 2020, 62, 1231–1238. [Google Scholar] [CrossRef]
- Sundaram, V.K.; Goldstein, J.; Wheelwright, D.; Aggarwal, A.; Pawha, P.S.; Doshi, A.; Fifi, J.T.; De Leacy, R.; Mocco, J.; Puig, J.; et al. Automated ASPECTS in Acute Ischemic Stroke: A Comparative Analysis with CT Perfusion. Am. J. Neuroradiol. 2019, 40, 2033. [Google Scholar] [CrossRef]
- Broocks, G.; Meyer, L.; McDonough, R.; Bechstein, M.; Hanning, U.; Fiehler, J.; Kemmling, A. The Benefit of Thrombectomy in Patients with Low ASPECTS Is a Matter of Shades of Gray-What Current Trials May Have Missed. Front. Neurol. 2021, 12, 718046. [Google Scholar] [CrossRef] [PubMed]
- Broocks, G.; Flottmann, F.; Scheibel, A.; Aigner, A.; Faizy, T.D.; Hanning, U.; Leischner, H.; Broocks, S.I.; Fiehler, J.; Gellissen, S.; et al. Quantitative Lesion Water Uptake in Acute Stroke Computed Tomography Is a Predictor of Malignant Infarction. Stroke 2018, 49, 1906–1912. [Google Scholar] [CrossRef] [PubMed]
- Demeestere, J.; Wouters, A.; Christensen, S.; Lemmens, R.; Lansberg, M.G. Review of Perfusion Imaging in Acute Ischemic Stroke. Stroke 2020, 51, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Boned, S.; Padroni, M.; Rubiera, M.; Tomasello, A.; Coscojuela, P.; Romero, N.; Muchada, M.; Rodríguez-Luna, D.; Flores, A.; Rodríguez, N.; et al. Admission CT perfusion may overestimate initial infarct core: The ghost infarct core concept. J. NeuroIntervent Surg. 2017, 9, 66. [Google Scholar] [CrossRef] [PubMed]
- García-Tornel, Á.; Campos, D.; Rubiera, M.; Boned, S.; Olivé-Gadea, M.; Requena, M.; Ciolli, L.; Muchada, M.; Pagola, J.; Rodriguez-Luna, D.; et al. Ischemic Core Overestimation on Computed Tomography Perfusion. Stroke 2021, 52, 1751–1760. [Google Scholar] [CrossRef]
- Nagaraja, N.; Forder, J.R.; Warach, S.; Merino, J.G. Reversible diffusion-weighted imaging lesions in acute ischemic stroke. Neurology 2020, 94, 571. [Google Scholar] [CrossRef]
- Gautheron, V.; Xie, Y.; Tisserand, M.; Raoult, H.; Soize, S.; Naggara, O.; Bourcier, R.; Richard, S.; Guillemin, F.; Bracard, S.; et al. Outcome After Reperfusion Therapies in Patients with Large Baseline Diffusion-Weighted Imaging Stroke Lesions: A THRACE Trial (Mechanical Thrombectomy After Intravenous Alteplase Versus Alteplase Alone After Stroke) Subgroup Analysis. Stroke 2018, 49, 750–753. [Google Scholar] [CrossRef]
- Campbell, B.C.V.; Majoie, C.B.L.M.; Albers, G.W.; Menon, B.K.; Yassi, N.; Sharma, G.; van Zwam, W.H.; van Oostenbrugge, R.J.; Demchuk, A.M.; Guillemin, F.; et al. Penumbral imaging and functional outcome in patients with anterior circulation ischaemic stroke treated with endovascular thrombectomy versus medical therapy: A meta-analysis of individual patient-level data. Lancet Neurol. 2019, 18, 46–55. [Google Scholar] [CrossRef]
- Cagnazzo, F.; Derraz, I.; Dargazanli, C.; Lefevre, P.-H.; Gascou, G.; Riquelme, C.; Bonafe, A.; Costalat, V. Mechanical thrombectomy in patients with acute ischemic stroke and ASPECTS ≤ 6: A meta-analysis. J. Neurointerv. Surg. 2020, 12, 350–355. [Google Scholar] [CrossRef]
- Sarraj, A.; Grotta, J.C.; Pujara, D.K.; Shaker, F.; Tsivgoulis, G. Triage imaging and outcome measures for large core stroke thrombectomy—A systematic review and meta-analysis. J. Neurointerv. Surg. 2020, 12, 1172–1179. [Google Scholar] [CrossRef]
- Yoshimura, S.; Uchida, K.; Sakai, N.; Yamagami, H.; Inoue, M.; Toyoda, K.; Matsumaru, Y.; Matsumoto, Y.; Kimura, K.; Ishikura, R.; et al. Randomized Clinical Trial of Endovascular Therapy for Acute Large Vessel Occlusion with Large Ischemic Core (RESCUE-Japan LIMIT): Rationale and Study Protocol. Neurol. Med. Chir. 2022, 62, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Huo, X.; Ma, G.; Tong, X.; Zhang, X.; Pan, Y.; Nguyen, T.N.; Yuan, G.; Han, H.; Chen, W.; Wei, M.; et al. Trial of Endovascular Therapy for Acute Ischemic Stroke with Large Infarct. N. Engl. J. Med. 2023, 388, 1272–1283. [Google Scholar] [CrossRef] [PubMed]
- Sarraj, A.; Hassan, A.E.; Abraham, M.G.; Ortega-Gutierrez, S.; Kasner, S.E.; Hussain, M.S.; Chen, M.; Blackburn, S.; Sitton, C.W.; Churilov, L.; et al. Trial of Endovascular Thrombectomy for Large Ischemic Strokes. N. Engl. J. Med. 2023, 388, 1259–1271. [Google Scholar] [CrossRef] [PubMed]
- Ballout, A.A. Endovascular thrombectomy of large ischemic strokes: Reimagining the boundaries of reperfusion. Interv. Neuroradiol. 2023, 29, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Bendszus, M.; Fiehler, J.; Subtil, F.; Bonekamp, S.; Aamodt, A.H.; Fuentes, B.; Gizewski, E.R.; Hill, M.D.; Krajina, A.; Pierot, L.; et al. Endovascular thrombectomy for acute ischaemic stroke with established large infarct: Multicentre, open-label, randomised trial. Lancet 2023, 402, 1753–1763. [Google Scholar] [CrossRef]
- Zaidat, O.O.; Yoo, A.J.; on behalf of TESLA investigators. TESLA trial: Primary results. In Proceedings of the European Stroke Organisation Conference 2023, Munich, Germany, 26 May 2023. [Google Scholar]
- Palaiodimou, L.; Sarraj, A.; Safouris, A.; Magoufis, G.; Lemmens, R.; Sandset, E.C.; Turc, G.; Psychogios, M.; Tsivgoulis, G. Endovascular treatment for large-core ischaemic stroke: A meta-analysis of randomised controlled clinical trials. J. Neurol. Neurosurg. Psychiatry 2023, 94, 781. [Google Scholar] [CrossRef]
- Kobeissi, H.; Adusumilli, G.; Ghozy, S.; Kadirvel, R.; Brinjikji, W.; Albers, G.W.; Heit, J.J.; Kallmes, D.F. Endovascular thrombectomy for ischemic stroke with large core volume: An updated, post-TESLA systematic review and meta-analysis of the randomized trials. Interv. Neuroradiol, 2023; online ahead of print. [Google Scholar] [CrossRef]
- Hao, Y.; Yang, D.; Wang, H.; Zi, W.; Zhang, M.; Geng, Y.; Zhou, Z.; Wang, W.; Xu, H.; Tian, X. Predictors for Symptomatic Intracranial Hemorrhage After Endovascular Treatment of Acute Ischemic Stroke. Stroke 2017, 48, 1203–1209. [Google Scholar] [CrossRef]
- Ren, Z.; Huo, X.; Kumar, J.; Jadhav, A.P.; Costalat, V.; Fiehler, J.; Bendszus, M.; Yoshimura, S.; Ma, G.; Tong, X.; et al. Review of Current Large Core Volume Stroke Thrombectomy Clinical Trials: Controversies and Progress. Stroke Vasc. Interv. Neurol. 2022, 2, e000330. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Trial | RESCUE-Japan LIMIT | ANGEL-ASPECTS | SELECT2 | TENSION | TESLA (Unpublished) |
|---|---|---|---|---|---|
| Country(ies) | Japan | China | United States, Canada, Europe | Canada, Europe | United States |
| Size | 101 EVT, 102 MM | 231 EVT, 225 MM | 178 EVT, 174 MM | 125 EVT, 128 MM | 152 EVT, 148 MM |
| NIHSS score | ≥6 | 6–30 | ≥6 | <26 | ≥6 |
| Age | >18 | 18–80 | 18–85 | >18 | 18–85 |
| Imaging criteria | 1. NCCT or DWI-MRI ASPECTS 3–5
| 1. NCCT ASPECTS 3–5 or 2. NCCT ASPECTS > 5 (>6 h) and infarct core 70–100 mL or 3. ASPECTS < 3 and infarct core 70–100 mL
| 1. NCCT ASPECTS ≥ 6 and infarct core ≥ 50 mL 2. NCCT ASPECTS 3–5 and infarct core ≥ 50 mL or 3. NCCT ASPECTS 3–5 and infarct core < 50 mL or
| 1. NCCT or DWI-MRI ASPECTS 3–5
| 1. NCCT ASPECTS 2–5 |
| Thrombolysis | 56/203 (27%) given alteplase | 129/455 (28%) given alteplase (1 given urokinase) | 67/351 (19%) given alteplase | 93/253 (36%) given alteplase | Yes, unclear how many |
| Time window | Within 6 h from LKW or within 6 to 24 h from LKW (FLAIR-) Most presented within 4.5 h | Within 0 to 24 h from LKW Most presented within 6–12 h | Within 0 to 24 h from LKW Median time interval—9 h from LKW | Within 0 to 12 h from LKW Median time from symptom onset to groin puncture 4.2 h | Within 24 h of stroke onset |
| Key outcomes |
|
|
|
|
|
| Key safety outcomes |
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, G.Z.; Lai, J.Y.; Seet, C.Y.H.; Tham, C.H.; Venketasubramanian, N.; Tan, B.Y.Q.; Jing, M.; Yeo, J.Y.P.; Myint, M.Z.; Sia, C.-H.; et al. Revolutionizing the Management of Large-Core Ischaemic Strokes: Decoding the Success of Endovascular Therapy in the Recent Stroke Trials. J. Cardiovasc. Dev. Dis. 2023, 10, 499. https://doi.org/10.3390/jcdd10120499
Lim GZ, Lai JY, Seet CYH, Tham CH, Venketasubramanian N, Tan BYQ, Jing M, Yeo JYP, Myint MZ, Sia C-H, et al. Revolutionizing the Management of Large-Core Ischaemic Strokes: Decoding the Success of Endovascular Therapy in the Recent Stroke Trials. Journal of Cardiovascular Development and Disease. 2023; 10(12):499. https://doi.org/10.3390/jcdd10120499
Chicago/Turabian StyleLim, Gareth Zigui, Jonathan Yexian Lai, Christopher Ying Hao Seet, Carol Huilian Tham, Narayanaswamy Venketasubramanian, Benjamin Yong Qiang Tan, Mingxue Jing, Joshua Yee Peng Yeo, May Zin Myint, Ching-Hui Sia, and et al. 2023. "Revolutionizing the Management of Large-Core Ischaemic Strokes: Decoding the Success of Endovascular Therapy in the Recent Stroke Trials" Journal of Cardiovascular Development and Disease 10, no. 12: 499. https://doi.org/10.3390/jcdd10120499