

The Contributions of Knee Extension Strength and Hand Grip Strength to Factors Relevant to Physical Frailty: The Tanno-Sobetsu Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
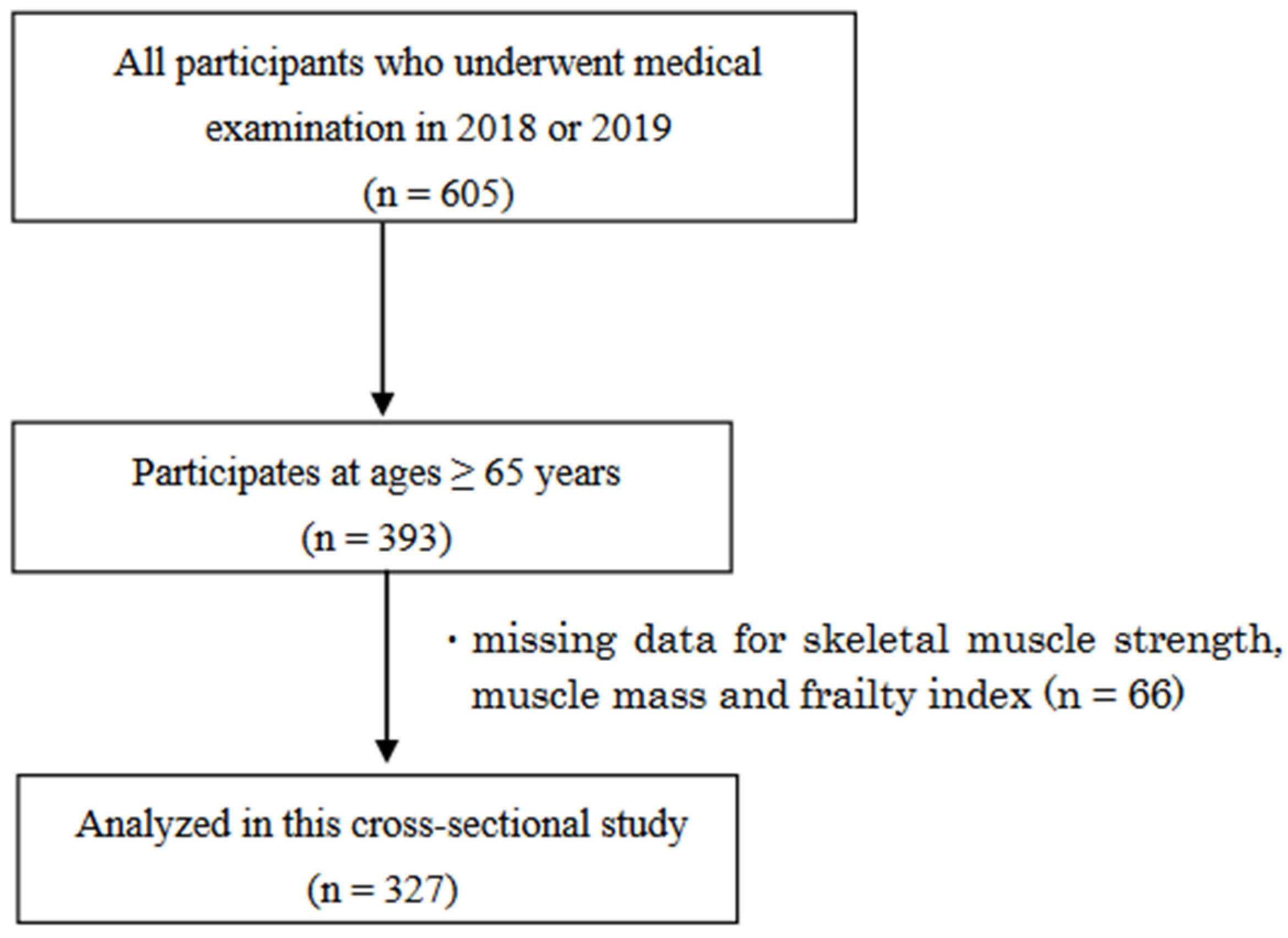
2.1. Study Population
2.2. Assessment of Frailty
2.3. Muscle Strength and Muscle Mass Measurements
2.4. Other Measurements
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Associations between Physical Frailty and the Muscle Indices
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cabinet Office, Government of Japan. The Aging Society White Paper in 2022. Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2022/html/zenbun/s1_1_1.html (accessed on 2 February 2023).
- Abellan van Kan, G.; Rolland, Y.; Bergman, H.; Morley, J.E.; Kritchevsky, S.B.; Vellas, B. The I.A.N.A Task Force on frailty assessment of older people in clinical practice. J. Nutr. Health Aging 2008, 12, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Yamada, M.; Fukutani, N.; Adachi, D.; Tashiro, Y.; Hotta, T.; Morino, S.; Shirooka, H.; Nozaki, Y.; Hirata, H.; et al. Differential association of frailty with cognitive decline and sarcopenia in community-dwelling older adults. J. Am. Med. Dir. Assoc. 2015, 16, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Pourhassan, M.; Norman, K.; Müller, M.J.; Dziewas, R.; Wirth, R. Impact of Sarcopenia on One-Year Mortality among Older Hospitalized Patients with Impaired Mobility. J. Frailty Aging 2018, 7, 40–46. [Google Scholar] [CrossRef]
- Manini, T.M.; Clark, B.C. Dynapenia and aging: An update. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2012, 67, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Skelton, D.A.; Greig, C.A.; Davies, J.M.; Young, A. Strength, power and related functional ability of healthy people aged 65–89 years. Age Ageing 1994, 23, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.C.; Tsou, H.H.; Yang, R.S.; Tsauo, J.Y.; Chen, C.Y.; Hsiung, C.A.; Kuo, K.N. A pilot randomized controlled trial to improve geriatric frailty. BMC Geriatr. 2012, 12, 58. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty Reversal Among Older Adults: A Randomized Controlled Trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef]
- Kim, H.; Suzuki, T.; Kim, M.; Kojima, N.; Ota, N.; Shimotoyodome, A.; Hase, T.; Hosoi, E.; Yoshida, H. Effects of exercise and milk fat globule membrane (MFGM) supplementation on body composition, physical function, and hematological parameters in community-dwelling frail Japanese women: A randomized double blind, placebo-controlled, follow-up trial. PLoS ONE 2015, 10, e0116256. [Google Scholar] [CrossRef]
- Luger, E.; Dorner, T.E.; Haider, S.; Kapan, A.; Lackinger, C.; Schindler, K. Effects of a Home-Based and Volunteer-Administered Physical Training, Nutritional, and Social Support Program on Malnutrition and Frailty in Older Persons: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2016, 17, 671.e9–671.e16. [Google Scholar] [CrossRef]
- Serra-Prat, M.; Sist, X.; Domenich, R.; Jurado, L.; Saiz, A.; Roces, A.; Palomera, E.; Tarradelles, M.; Papiol, M. Effectiveness of an intervention to prevent frailty in pre-frail community-dwelling older people consulting in primary care: A randomised controlled trial. Age Ageing 2017, 46, 401–407. [Google Scholar] [CrossRef]
- Losa-Reyna, J.; Baltasar-Fernandez, I.; Alcazar, J.; Navarro-Cruz, R.; Garcia-Garcia, F.J.; Alegre, L.M.; Alfaro-Acha, A. Effect of a short multicomponent exercise intervention focused on muscle power in frail and pre frail elderly: A pilot trial. Exp. Gerontol. 2019, 115, 114–121. [Google Scholar] [CrossRef]
- Bollwein, J.; Volkert, D.; Diekmann, R.; Kaiser, M.J.; Uter, W.; Vidal, K.; Sieber, C.C.; Bauer, J.M. Nutritional status according to the mini nutritional assessment (MNA®) and frailty in community dwelling older persons: A close relationship. J. Nutr. Health Aging 2013, 17, 351–356. [Google Scholar] [CrossRef]
- Peterson, M.J.; Giuliani, C.; Morey, M.C.; Pieper, C.F.; Evenson, K.R.; Mercer, V.; Cohen, H.J.; Visser, M.; Brach, J.S.; Kritchevsky, S.B.; et al. Physical activity as a preventative factor for frailty: The health, aging, and body composition study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2009, 64, 61–68. [Google Scholar] [CrossRef]
- García-Esquinas, E.; Andrade, E.; Martínez-Gómez, D.; Caballero, F.F.; López-García, E.; Rodríguez-Artalejo, F. Television viewing time as a risk factor for frailty and functional limitations in older adults: Results from 2 European prospective cohorts. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 54. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, L.; Corbin, A.L.; Goveas, J.S. Depression and frailty in later life: A systematic review. Clin. Interv. Aging 2015, 10, 1947–1958. [Google Scholar] [CrossRef] [PubMed]
- García-Esquinas, E.; Graciani, A.; Guallar-Castillón, P.; López-García, E.; Rodríguez-Mañas, L.; Rodríguez-Artalejo, F. Diabetes and risk of frailty and its potential mechanisms: A prospective cohort study of older adults. J. Am. Med. Dir. Assoc. 2015, 16, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Afilalo, J.; Karunananthan, S.; Eisenberg, M.J.; Alexander, K.P.; Bergman, H. Role of frailty in patients with cardiovascular disease. Am. J. Cardiol. 2009, 103, 1616–1621. [Google Scholar] [CrossRef]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Suzuki, T. Impact of physical frailty on disability in community-dwelling older adults: A prospective cohort study. BMJ Open 2015, 5, e008462. [Google Scholar] [CrossRef]
- Matsumoto, T.; Ohnishi, H.; Sato, T.; Miki, T.; Akasaka, H.; Hanawa, N.; Koyama, M.; Saitoh, S.; Miura, T. Insulin Resistance is Associated with Longitudinal Changes of Cardiac Repolarization Heterogeneity in Apparently Healthy Subjects. Cardiol. Ther. 2019, 8, 239–251. [Google Scholar] [CrossRef]
- Satake, S.; Shimada, H.; Yamada, M.; Kim, H.; Yoshida, H.; Gondo, Y.; Matsubayashi, K.; Matsushita, E.; Kuzuya, M.; Kozaki, K.; et al. Prevalence of frailty among community-dwellers and outpatients in Japan as defined by the Japanese version of the Cardiovascular Health Study criteria. Geriatr. Gerontol. Int. 2017, 17, 2629–2634. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.L. Grip strength reference values for Canadians aged 6 to 79: Canadian Health Measures Survey, 2007 to 2013. Health Rep. 2016, 27, 3–10. [Google Scholar] [PubMed]
- Bohannon, R.W.; Bubela, D.J.; Magasi, S.R.; Gershon, R.C. Relative reliability of three objective tests of limb muscle strength. Isokinet. Exerc. Sci. 2011, 19, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Suwa, M.; Imoto, T.; Kida, A.; Iwase, M.; Yokochi, T. Age-related reduction and independent predictors of toe flexor strength in middle-aged men. J. Foot Ankle Res. 2017, 10, 15. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Shinkai, S.; Murayama, H.; Mori, S. Comparison of segmental multifrequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for the assessment of body composition in a community-dwelling older population. Geriatr. Gerontol. Int. 2015, 15, 1013–1022. [Google Scholar] [CrossRef]
- Batista, F.S.; Gomes, G.A.; D’Elboux, M.J.; Cintra, F.A.; Neri, A.L.; Guariento, M.E.; Rosário de Souza Mda, L. Relationship between lower-limb muscle strength and functional independence among elderly people according to frailty criteria: A cross-sectional study. Sao Paulo Med. J. 2014, 132, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Vellas, B.; van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef]
- Osawa, Y.; Chiles Shaffer, N.; Shardell, M.D.; Studenski, S.A.; Ferrucci, L. Changes in knee extension peak torque and body composition and their relationship with change in gait speed. J. Cachexia Sarcopenia Muscle 2019, 10, 1000–1008. [Google Scholar] [CrossRef]
- Rantanen, T.; Guralnik, J.M.; Ferrucci, L.; Penninx, B.W.; Leveille, S.; Sipila, S.; Fried, L.P. Coimpairments as predictors of severe walking disability in older women. J. Am. Geriatr. Soc. 2001, 49, 21–27. [Google Scholar] [CrossRef]
- Newman, A.B.; Kupelian, V.; Visser, M.; Simonsick, E.M.; Goodpaster, B.H.; Kritchevsky, S.B.; Tylavsky, F.A.; Rubin, S.M.; Harris, T.B. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 72–77. [Google Scholar] [CrossRef]
- Delmonico, M.J.; Harris, T.B.; Visser, M.; Park, S.W.; Conroy, M.B.; Velasquez-Mieyer, P.; Boudreau, R.; Manini, T.M.; Nevitt, M.; Newman, A.B.; et al. Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am. J. Clin. Nutr. 2009, 90, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- Seko, T.; Akasaka, H.; Koyama, M.; Himuro, N.; Saitoh, S.; Miura, T.; Mori, M.; Ohnishi, H. Preserved Lower Limb Muscle Mass Prevents Insulin Resistance Development in Nondiabetic Older Adults. J. Am. Med. Dir. Assoc. 2023, 24, 376–381.e1. [Google Scholar] [CrossRef] [PubMed]
- Seko, T.; Akasaka, H.; Koyama, M.; Himuro, N.; Saitoh, S.; Miura, T.; Mori, M.; Ohnishi, H. Lower limb muscle mass is associated with insulin resistance more than lower limb muscle strength in non-diabetic older adults. Geriatr. Gerontol. Int. 2019, 19, 1254–1259. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Non-Frail (n = 70) | Pre-Frail (n = 64) | Frail (n = 9) | Pairwise Comparison |
|---|---|---|---|---|
| Age (years) | 73.7 (5.5) | 75.7 (6.8) | 82.7 (6.3) | b, c |
| Height (cm) | 163.9 (5.9) | 162.0 (5.7) | 159.4 (7.9) | p = 0.08 |
| Weight (kg) | 64.3 (9.5) | 63.6 (12.8) | 52.8 (11.9) | b, c |
| BMI (kg/m2) | 23.9 (3.0) | 24.1 (4.2) | 20.6 (3.5) | b, c |
| Systolic BP (mmHg) | 137.5 (17.0) | 140.4 (17.3) | 140.1 (21.4) | p = 0.39 |
| Diastolic BP (mmHg) | 74.9 (8.9) | 76.1 (10.6) | 71.3 (12.0) | p = 0.17 |
| Medical history, n (%) | ||||
| Type2 diabetes | 12 (17) | 10 (16) | 2 (22) | p = 0.41 |
| Cardiovascular disease | 11 (16) | 18 (28) | 3 (33) | p = 0.16 |
| Muscle strength | ||||
| Hand grip strength (kg) | 38.5 (6.8) | 34.3 (8.1) | 24.9 (12.3) | a, b, c |
| Knee extension strength (Nm) | 108.0 (34.2) | 100.1 (31.4) | 49.8 (31.3) | b, c |
| Toe grip strength (kg) | 14.0 (4.8) | 12.8 (5.4) | 7.7 (6.8) | b, c |
| Skeletal muscle mass | ||||
| Appendicular muscle mass (kg) | 20.3 (2.8) | 19.1 (2.8) | 15.5 (4.6) | a, b, c |
| Walking speed | ||||
| Comfortable speed (m/s) | 1.23 (0.16) | 1.12 (0.23) | 0.85 (0.10) | a, b, c |
| Biochemical data | ||||
| Albumin (g/dL) | 4.41 (0.22) | 4.32 (0.26) | 4.35 (0.30) | p = 0.17 |
| HbA1c (%) | 5.7 (5.4–5.9) | 5.6 (5.3–6.0) | 5.5 (5.3–5.7) | p = 0.42 |
| Variable | Non-Frail (n = 101) | Pre-Frail (n = 68) | Frail (n = 15) | Pairwise Comparison |
|---|---|---|---|---|
| Age (years) | 73.6 (6.0) | 76.2 (7.0) | 74.9 (6.5) | a |
| Height (cm) | 149.7 (6.1) | 148.2 (5.6) | 145.1 (6.1) | b |
| Weight (kg) | 51.1 (8.4) | 50.0 (8.5) | 54.5 (11.2) | p = 0.20 |
| BMI (kg/m2) | 22.7 (3.4) | 22.8 (3.8) | 25.8 (5.1) | b |
| Systolic BP (mmHg) | 141.3 (21.3) | 138.8 (21.2) | 129.2 (16.3) | p = 0.74 |
| Diastolic BP (mmHg) | 74.7 (11.1) | 70.8 (12.0) | 71.5 (12.9) | p = 0.09 |
| Medical history, n (%) | ||||
| Type2 diabetes | 9 (9) | 9 (13) | 4 (27) | p = 0.15 |
| Cardiovascular disease | 4 (5) | 11 (16) | 2 (13) | p = 0.049 |
| Muscle strength | ||||
| Hand grip strength (kg) | 23.9 (4.0) | 21.4 (4.7) | 19.2 (4.8) | a, b |
| Knee extension strength (Nm) | 67.1 (18.8) | 56.0 (20.0) | 49.5 (15.8) | a, b |
| Toe grip strength (kg) | 10.5 (3.9) | 8.9 (3.9) | 7.5 (2.9) | a, b |
| Skeletal muscle mass | ||||
| Appendicular muscle mass (kg) | 13.6 (2.2) | 12.8 (1.9) | 12.9 (2.3) | p = 0.06 |
| Walking speed | ||||
| Comfortable speed (m/s) | 1.25 (0.15) | 1.04 (0.25) | 0.88 (0.22) | a, b, c |
| Biochemical data | ||||
| Albumin (g/dL) | 4.40 (0.20) | 4.41 (0.25) | 4.26 (0.26) | p = 0.07 |
| HbA1c (%) | 5.6 (5.4–5.8) | 5.6 (5.4–5.9) | 5.7 (5.4–5.9) | p = 0.48 |
| Weight Loss | Low Activity Level | Exhaustion | Weakness | Slowness | ||
|---|---|---|---|---|---|---|
| Pre-frail (n = 132) | n (%) | 37 (28) | 32 (24) | 38 (29) | 23 (17) | 40 (30) |
| Frail (n = 24) | n (%) | 13 (54) | 16 (66) | 15 (62) | 12 (50) | 20 (83) |
| Robust = 171 vs. Pre-Frailty = 132 | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| OR (95%CI) | OR (95%CI) | OR (95%CI) | |
| Hand grip strength (kg) | 0.92 (0.88–0.97) | 0.93 (0.88–0.98) | 0.92 (0.87–0.97) |
| p = 0.005 | p = 0.006 | p = 0.005 | |
| Knee extension strength (Nm) | 0.99 (0.98–1.01) | 0.99 (0.98–1.01) | 0.99 (0.98–1.01) |
| p = 0.36 | p = 0.36 | p = 0.82 | |
| Toe grip strength (kg) | 1.01 (0.94–1.09) | 1.01 (0.94–1.10) | 1.06 (0.98–1.14) |
| p = 0.63 | p = 0.64 | p = 0.13 | |
| Appendicular muscle mass (kg) | 0.96 (0.85–1.09) | 0.96 (0.85–1.09) | 0.92 (0.81–1.05) |
| p = 0.59 | p = 0.57 | p = 0.25 |
| Pre-Frailty = 132 vs. Frailty = 24 | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| OR (95%CI) | OR (95%CI) | OR (95%CI) | |
| Hand grip strength (kg) | 0.93 (0.84–1.03) | 0.93 (0.85–1.03) | 0.93 (0.84–1.03) |
| p = 0.18 | p = 0.19 | p = 0.18 | |
| Knee extension strength (Nm) | 0.95 (0.92–0.98) | 0.95 (0.92–0.98) | 0.95 (0.92–0.99) |
| p = 0.005 | p = 0.005 | p = 0.021 | |
| Toe grip strength (kg) | 0.99 (0.84–1.17) | 0.99 (0.84–1.17) | 1.03 (0.86–1.23) |
| p = 0.95 | p = 0.96 | p = 0.72 | |
| Appendicular muscle mass (kg) | 1.18 (0.92–1.50) | 1.17 (0.91–1.50) | 1.13 (0.85–1.45) |
| p = 0.18 | p = 0.21 | p = 0.43 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seko, T.; Akasaka, H.; Koyama, M.; Himuro, N.; Saitoh, S.; Ogawa, S.; Miura, S.; Mori, M.; Ohnishi, H. The Contributions of Knee Extension Strength and Hand Grip Strength to Factors Relevant to Physical Frailty: The Tanno-Sobetsu Study. Geriatrics 2024, 9, 9. https://doi.org/10.3390/geriatrics9010009
Seko T, Akasaka H, Koyama M, Himuro N, Saitoh S, Ogawa S, Miura S, Mori M, Ohnishi H. The Contributions of Knee Extension Strength and Hand Grip Strength to Factors Relevant to Physical Frailty: The Tanno-Sobetsu Study. Geriatrics. 2024; 9(1):9. https://doi.org/10.3390/geriatrics9010009
Chicago/Turabian StyleSeko, Toshiaki, Hiroshi Akasaka, Masayuki Koyama, Nobuaki Himuro, Shigeyuki Saitoh, Shunichi Ogawa, Sayo Miura, Mitsuru Mori, and Hirofumi Ohnishi. 2024. "The Contributions of Knee Extension Strength and Hand Grip Strength to Factors Relevant to Physical Frailty: The Tanno-Sobetsu Study" Geriatrics 9, no. 1: 9. https://doi.org/10.3390/geriatrics9010009