
Influence of Potentially Inappropriate Medication Use on Older Australians’ Admission to Emergency Department Short Stay

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Setting
2.2. Inclusion Criteria
2.3. Data Sources and Collection
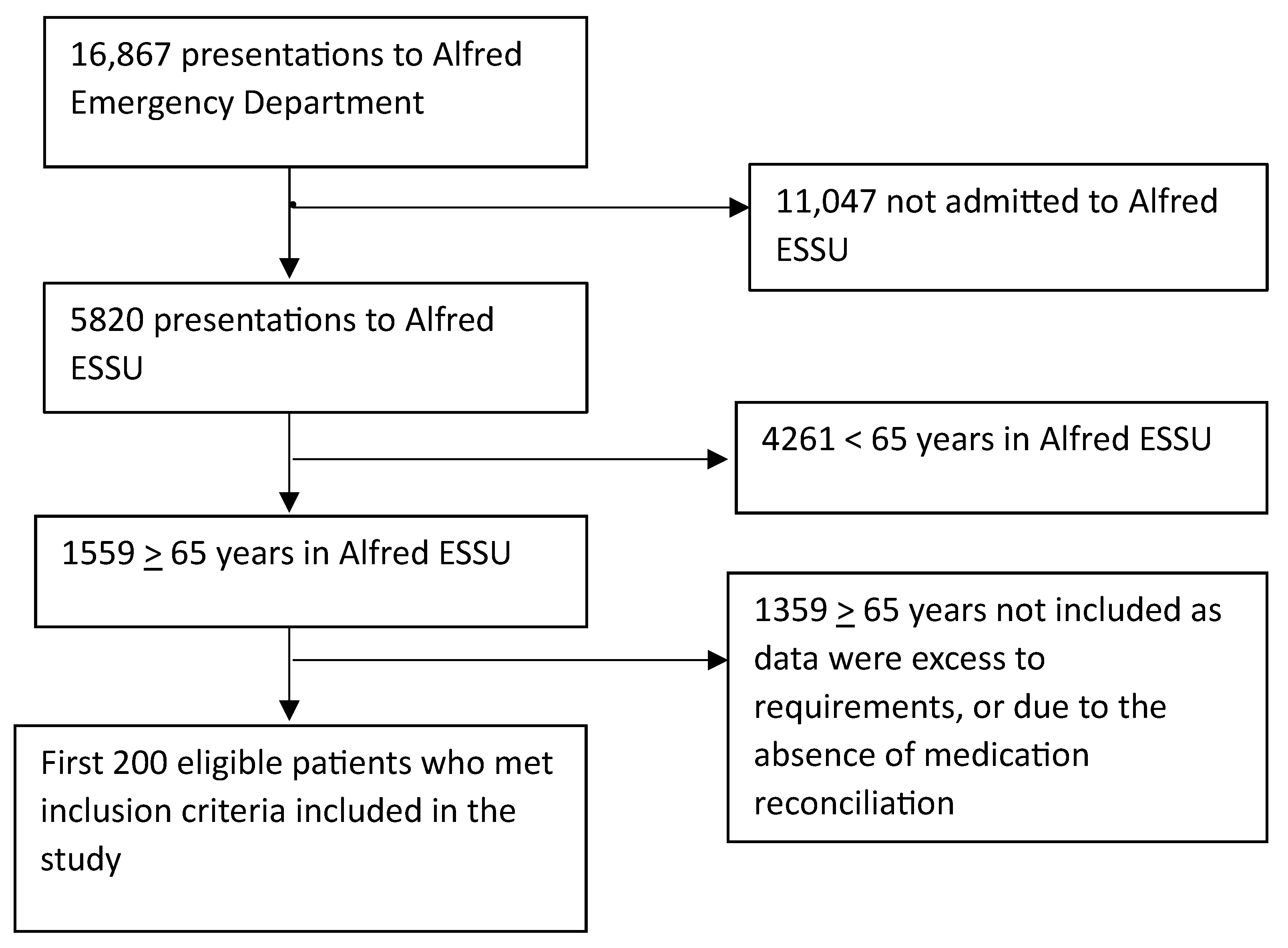
2.4. Sample Size
2.5. Data Analysis
3. Results
3.1. Demographics
3.2. Potentially Inappropriate Medications Identified Using STOPP/START Criteria
3.3. Potential ESSU Admissions Related to PIMs
4. Discussion
- Comprehensive medication reviews by EM pharmacists: EM pharmacists can play a pivotal role in conducting thorough medication reviews, identifying PIMs, and initiating deprescribing interventions [45,46]. Interventions made by EM pharmacists such as medication reconciliation and providing deprescribing suggestions to at-risk patients have led to a ten-fold increase in deprescribing of PIMs by primary care physicians [47].
- Education on deprescribing: Providing education to healthcare professionals, including pharmacists and doctors, is essential to empower them with the knowledge and skills needed for effective deprescribing [43,44]. Education interventions provided to patients and their caregivers may lead to a reduction in medication use and need to be targeted to prevent admission to ED [48,49].
- Computer-based decision support (CDS) tools: Computer-based decision support tools have been demonstrated to enhance prescribing practice for older individuals in the ED. These improve recommended dose administrations, promote deprescribing of PIMs, and reduce the incidence of inappropriate prescriptions [50].
- Inclusion of geriatricians in ED: Involving geriatricians in ED can provide specialized input in medication decisions for older patients [51].
- Collaboration and follow-up with community-based providers: Collaborative efforts and effective communication with community-based doctors and pharmacists are crucial to ensure seamless transitions in patient care and medication management [52]
- Utilization of Home Medication Review (HMR) or Hospital-Initiated Medication Review (HIMR): These services can be valuable in reviewing and optimizing medication use [53]. According to data from the Australian Commission on Safety and Quality in Health Care, only about 5.4% of people aged 75 years and over had at least one government-subsidized service for a Residential Medication Management Review (RMMR) or a Home Medicine Review (HMR) in 2018–19 [54]. There is a pressing need to enhance access to these services and develop strategies to improve the uptake of pharmacist recommendations. The Society of Hospital Pharmacists (SHPA) has also established a pathway for HMR referrals for patients seen in the ED [55].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| D5. Benzodiazepines for ≥4 weeks. K1. Benzodiazepines (sedative, may cause reduced sensorium, impair balance). | 31 (15.5%) |
| A1. Any drug prescribed without an evidence-based clinical indication. | 22 (11%) |
| A3. Any duplicate drug class prescription, e.g., two concurrent NSAIDs, SSRIs, loop diuretics, ACE inhibitors, or anticoagulants (optimisation of monotherapy within a single drug class should be observed prior to considering a new agent). | 11 (5.5%) |
| L2. Use of regular (as distinct from PRN) opioids without concomitant laxative (risk of severe constipation). | 7 (3.5%) |
| D1. TriCyclic Antidepressants (TCAs) with dementia, narrow angle glaucoma, cardiac conduction abnormalities, prostatism, or prior history of urinary retention (risk of worsening these conditions). | 5 (2.5%) |
| L3. Long-acting opioids without short-acting opioids for break-through pain (risk of persistence of severe pain) | 4 (2%) |
| A2. Any drug prescribed beyond the recommended duration, where treatment duration is well defined. | 3 (1.5%) |
| D14. First-generation antihistamines (safer, less toxic antihistamines now widely available). | 3 (1.5%) |
| E6. Metformin if eGFR < 30 mL/min/1.73 m2 (risk of lactic acidosis). | 3 (1.5%) |
| F2. PPI for uncomplicated peptic ulcer disease or erosive peptic oesophagitis at full therapeutic dosage for >8 weeks (dose reduction or earlier discontinuation indicated). | 3 (1.5%) |
| I2. Pneumococcal vaccine at least once after age 65 according to national guidelines. | 142 (71%) |
| I1. Seasonal trivalent influenza vaccine annually. | 84 (42%) |
| E3. Vitamin D and calcium supplement in patients with known osteoporosis and/or previous fragility fracture(s) and/or bone mineral density T-scores more than −2.5 in multiple sites. | 59 (29.5%) |
| E2. Bisphosphonates and vitamin D and calcium in patients taking long-term systemic corticosteroid therapy. | 16 (8%) |
| A3. Antiplatelet therapy (aspirin or clopidogrel or prasugrel or ticagrelor) with a documented history of coronary, cerebral, or peripheral vascular disease. | 12 (6%) |
| A7. Beta-blocker with ischaemic heart disease. | 11 (5.5%) |
| B1. Regular inhaled b2 agonist or antimuscarinic bronchodilator (e.g., ipratropium, tiotropium) for mild to moderate asthma or COPD. | 11 (5.5%) |
| C3. Acetylcholinesterase inhibitor (e.g., donepezil, rivastigmine, galantamine) for mild-moderate Alzheimer’s dementia or Lewy body dementia (rivastigmine). | 11 (5.5%) |
| E4. Bone anti-resorptive or anabolic therapy (e.g., bisphosphonate, strontium ranelate, teriparatide, denosumab) in patients with documented osteoporosis, where no pharmacological or clinical status contraindication exists (bone mineral density T-scores -> | 11 (5.5%) |
| A6. Angiotensin converting enzyme (ACE) inhibitor with systolic heart failure and/or documented coronary artery disease. | 9 (4.5%) |
| E5. Vitamin D supplement in older people who are housebound or experiencing falls or with osteopenia (bone mineral density T-score is >−1.0 but <−2.5 in multiple sites). | 8 (4%) |
| A5. Statin therapy with a documented history of coronary, cerebral, or peripheral vascular disease, unless the patient’s status is end-of-life or age is >85 years. | 7 (3.5%) |
| A8. Appropriate beta-blocker (bisoprolol, nebivolol, metoprolol or carvedilol) with stable systolic heart failure. | 6 (3%) |
| A1. Vitamin K antagonists or direct thrombin inhibitors or factor Xa inhibitors in the presence of chronic atrial fibrillation. | 5 (2.5%) |
| STOPP/ START PIM (Y/N) | Risk Rating (Assessed by Expert Panel) | |
|---|---|---|
| Y | Moderate |
| Y | Moderate |
| Y | High |
| Y | High |
| Y | Moderate |
| Y | Low |
| Y | High/Low |
| Y | Low |
| Y | High |
| Y | Low |
| Y | High |
| Y | High |
| Y | Low |
| Y | High |
| Y | High |
| Y | Low |
| Y | Low |
| Y | Moderate/Moderate |
| Y | Low |
References
- Australian Institute of Health and Welfare. Emergency Department Care 2020–21: Australian Hospital Statistics; Australian Institute of Health and Welfare: Canberra, Australia, 2021. Available online: https://www.aihw.gov.au/reports-data/myhospitals/sectors/emergency-department-care (accessed on 5 December 2021).
- Chan, T.; Arendts, G.; Stevens, M. Variables that predict admission to hospital from an emergency department observation unit. Emerg. Med. Australas. 2008, 20, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Ross, M.A.; Compton, S.; Richardson, D.; Jones, R.; Nittis, T.; Wilson, A. The use and effectiveness of an emergency department observation unit for elderly patients. Ann. Emerg. Med. 2003, 41, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Salvi, F.; Rossi, L.; Lattanzio, F.; Cherubini, A. Is polypharmacy an independent risk factor for adverse outcomes after an emergency department visit? Intern. Emerg. Med. 2017, 12, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Tong, E.Y.; Roman, C.; Mitra, B.; Yip, G.; Gibbs, H.; Newnham, H.; Smit, D.P.; Galbraith, K.; Dooley, M.J. Partnered pharmacist charting on admission in the General Medical and Emergency Short-stay Unit—A cluster-randomised controlled trial in patients with complex medication regimens. J. Clin. Pharm. Ther. 2016, 41, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Cahir, C.; Fahey, T.; Teeling, M.; Teljeur, C.; Feely, J.; Bennett, K. Potentially inappropriate prescribing and cost outcomes for older people: A national population study. Br. J. Clin. Pharmacol. 2010, 69, 543–552. [Google Scholar] [CrossRef] [PubMed]
- WHO. Medication Safety in Polypharmacy; (WHO/UHC/SDS/2019.11). Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Australian Commission on Safety and Quality in Health Care. Medication without Harm WHO Global Patient Safety Challenge—Australia’s Response; Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2022.
- Australian Commision on Safty and Quality in Healthcare. The Fourth Atlas of Healthcare Variation 2020—Medicines Use in Older People—Full Chapter. 2021. Available online: https://www.safetyandquality.gov.au/publications-and-resources/resource-library/fourth-atlas-healthcare-variation-2020-medicines-use-older-people-full-chapter (accessed on 18 November 2022).
- Banerjee, A.; Mbamalu, D.; Ebrahimi, S.; Khan, A.A.; Chan, T.F. The prevalence of polypharmacy in elderly attenders to an emergency department—A problem with a need for an effective solution. Int. J. Emerg. Med. 2011, 4, 22. [Google Scholar] [CrossRef] [PubMed]
- Almodóvar, A.S.; Nahata, M.C. Associations Between Chronic Disease, Polypharmacy, and Medication-Related Problems Among Medicare Beneficiaries. J. Manag. Care Spec. Pharm. 2019, 25, 573–577. [Google Scholar] [CrossRef]
- O’Mahony, D.; Gallagher, P.F. Inappropriate prescribing in the older population: Need for new criteria. Age Ageing 2008, 37, 138–141. [Google Scholar] [CrossRef]
- Ni Chroinin, D.; Neto, H.M.; Xiao, D.; Sandhu, A.; Brazel, C.; Farnham, N.; Perram, J.; Roach, T.S.; Sutherland, E.; Day, R. Potentially inappropriate medications (PIMs) in older hospital in-patients: Prevalence, contribution to hospital admission and documentation of rationale for continuation. Australas. J. Ageing 2016, 35, 262–265. [Google Scholar] [CrossRef]
- Liew, T.M.; Lee, C.S.; Goh Shawn, K.L.; Chang, Z.Y. Potentially Inappropriate Prescribing Among Older Persons: A Meta-Analysis of Observational Studies. Ann. Fam. Med. 2019, 17, 257–266. [Google Scholar] [CrossRef]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. Tools for Assessment of the Appropriateness of Prescribing and Association with Patient-Related Outcomes: A Systematic Review. Drugs Aging 2018, 35, 43–60. [Google Scholar] [CrossRef] [PubMed]
- 2019 American Geriatrics Society Beers Criteria® Update Expert Panel; Fick, D.M.; Semla, T.P.; Steinman, M.; Beizer, J.; Brandt, N.; Dombrowski, R.; DuBeau, C.E.; Pezzullo, L.; Epplin, J.J.; et al. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef]
- O’Mahony, D. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2015, 44, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Hill-Taylor, B.; Walsh, K.A.; Stewart, S.; Hayden, J.; Byrne, S.; Sketris, I.S. Effectiveness of the STOPP/START (Screening Tool of Older Persons’ potentially inappropriate Prescriptions/Screening Tool to Alert doctors to the Right Treatment) criteria: Systematic review and meta-analysis of randomized controlled studies. J. Clin. Pharm. Ther. 2016, 41, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Santolaya-Perrín, R.; Calderón-Hernanz, B.; Jiménez-Díaz, G.; Galán-Ramos, N.; Moreno-Carvajal, M.; Rodríguez-Camacho, J.; Serra-Simó, P.; García-Ortiz, J.; Tarradas-Torras, J.; Ginés-Palomares, A. The efficacy of a medication review programme conducted in an emergency department. Int. J. Clin. Pharm. 2019, 41, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Houlind, M.B.; Andersen, A.L.; Treldal, C.; Jørgensen, L.M.; Kannegaard, P.N.; Castillo, L.S.; Christensen, L.D.; Tavenier, J.; Rasmussen, L.J.H.; Ankarfeldt, M. A Collaborative Medication Review Including Deprescribing for Older Patients in an Emergency Department: A Longitudinal Feasibility Study. J. Clin. Med. 2020, 9, 348. [Google Scholar] [CrossRef]
- Atey, T.M.; Peterson, G.M.; Salahudeen, M.S.; Wimmer, B.C. The impact of partnered pharmacist medication charting in the emergency department on the use of potentially inappropriate medications in older people. Front. Pharmacol. 2023, 14, 1273655. [Google Scholar] [CrossRef]
- Atey, T.M.; Peterson, G.M.; Salahudeen, M.S.; Bereznicki, L.R.; Simpson, T.; Boland, C.M.; Anderson, E.; Burgess, J.R.; Huckerby, E.J.; Tran, V.; et al. Impact of Partnered Pharmacist Medication Charting (PPMC) on Medication Discrepancies and Errors: A Pragmatic Evaluation of an Emergency Department-Based Process Redesign. Int. J. Environ. Res. Public Health 2023, 20, 1452. [Google Scholar] [CrossRef]
- Alfred Health Annual Report 2020–2021; Alfred Health: Melbourne, Australia, 2021; Available online: https://www.alfredhealth.org.au/images/resources/corporate-publications/Annual-Report/Alfred_Health_Annual_Report_2020_2021.pdf (accessed on 5 July 2022).
- Abetz, J.W.; Adams, N.G.; Newnham, H.; Smit, D.V.; Mitra, B. Transfer of care and overstay in the management of cellulitis in the emergency short stay unit: A retrospective cohort study. Emerg. Med. Australas. 2017, 29, 143–148. [Google Scholar] [CrossRef]
- Taylor, G.; Leversha, A.; Archer, C.; Boland, C.; Dooley, M.; Fowler, P.; Gordon-Croal, S.; Fitch, J.; Marotti, S.; McKenzie, A.O.; et al. Standards of practice for clinical pharmacy services. J. Pharm. Pract. Res. 2013, 43, S2–S69. [Google Scholar] [CrossRef]
- Triage: Australasian College for Emergency Medicine. Available online: https://acem.org.au/Content-Sources/Advancing-Emergency-Medicine/Better-Outcomes-for-Patients/Triage (accessed on 4 December 2023).
- Baré, M.; Lleal, M.; Ortonobes, S.; Gorgas, M.Q.; Sevilla-Sánchez, D.; Carballo, N.; De Jaime, E.; Herranz, S.; on behalf of the MoPIM study group. Factors associated to potentially inappropriate prescribing in older patients according to STOPP/START criteria: MoPIM multicentre cohort study. BMC Geriatr. 2022, 22, 44. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.E.; Thomas, B.C. A Systematic Review of Studies of the STOPP/START 2015 and American Geriatric Society Beers 2015 Criteria in Patients ≥ 65 Years. Curr. Aging Sci. 2019, 12, 121–154. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, A.; Redley, B.; Crawford, K.; Jones, S.; de Courten, B.; Manias, E. Associations between hyper-polypharmacy and potentially inappropriate prescribing with clinical and functional outcomes in older adults. Expert Opin. Drug Saf. 2022, 21, 985–994. [Google Scholar] [CrossRef] [PubMed]
- Manias, E.; Maier, A.; Krishnamurthy, G. Inappropriate medication use in hospitalised oldest old patients across transitions of care. Aging Clin. Exp. Res. 2019, 31, 1661–1673. [Google Scholar] [CrossRef]
- Woolcott, J.C.; Richardson, K.J.; Wiens, M.O.; Patel, B.; Marin, J.; Khan, K.M.; Marra, C.A. Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Arch. Intern. Med. 2009, 169, 1952–1960. [Google Scholar] [CrossRef] [PubMed]
- Zetsen, S.P.G.; Schellekens, A.F.A.; Paling, E.P.; Kan, C.C.; Kessels, R.P.C. Cognitive Functioning in Long-Term Benzodiazepine Users. Eur. Addict. Res. 2022, 28, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Inderjeeth, C.A.; Glennon, D.A.; Poland, K.E.; Ingram, K.V.; Prince, R.L.; Van, V.R.; Holman, C.D.A.J. A multimodal intervention to improve fragility fracture management in patients presenting to emergency departments. Med. J. Aust. 2010, 193, 149–153. [Google Scholar] [CrossRef]
- Weng, M.C.; Tsai, C.F.; Sheu, K.L.; Lee, Y.T.; Lee, H.C.; Tzeng, S.L.; Ueng, K.C.; Chen, C.C.; Chen, S.C. The impact of number of drugs prescribed on the risk of potentially inappropriate medication among outpatient older adults with chronic diseases. QJM Int. J. Med. 2013, 106, 1009–1015. [Google Scholar] [CrossRef]
- Perpétuo, C.; Plácido, A.I.; Rodrigues, D.; Aperta, J.; Piñeiro-Lamas, M.; Figueiras, A.; Herdeiro, M.T.; Roque, F. Prescription of potentially inappropriate medication in older inpatients of an internal medicine ward: Concordance and overlap among the EU (7)-PIM list and Beers and STOPP criteria. Front. Pharmacol. 2021, 12, 676020. [Google Scholar] [CrossRef]
- Lau, D.T.; Mercaldo, N.D.; Harris, A.T.; Trittschuh, E.; Shega, J.; Weintraub, S. Polypharmacy and potentially inappropriate medication use among community-dwelling elders with dementia. Alzheimer Dis. Assoc. Disord. 2010, 24, 56–63. [Google Scholar] [CrossRef]
- Bao, Y.; Shao, H.; Bishop, T.F.; Schackman, B.R.; Bruce, M.L. Inappropriate medication in a national sample of US elderly patients receiving home health care. J. Gen. Intern. Med. 2012, 27, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Zed, P.J. Incidence, severity and preventability of medication-related visits to the emergency department: A prospective study. Can. Med. Assoc. J. (CMAJ) 2008, 178, 1563–1569. [Google Scholar] [CrossRef]
- Mekonnen, A.B.; Redley, B.; de Courten, B.; Manias, E. Potentially inappropriate prescribing and its associations with health-related and system-related outcomes in hospitalised older adults: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 2021, 87, 4150–4172. [Google Scholar] [CrossRef] [PubMed]
- Eshetie, T.C.; Roberts, G.; Nguyen, T.A.; Gillam, M.H.; Maher, D.; Kalisch Ellett, L.M. Potentially inappropriate medication use and related hospital admissions in aged care residents: The impact of dementia. Br. J. Clin. Pharmacol. 2020, 86, 2414–2423. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, D.; Cherubini, A.; Guiteras, A.R.; Denkinger, M.; Beuscart, J.-B.; Onder, G.; Gudmundsson, A.; Cruz-Jentoft, A.J.; Knol, W.; Bahat, G.; et al. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 3. Eur. Geriatr. Med. 2023, 14, 625–632. [Google Scholar] [CrossRef]
- Anderson, K.; Stowasser, D.; Freeman, C.; Scott, I. Prescriber barriers and enablers to minimising potentially inappropriate medications in adults: A systematic review and thematic synthesis. BMJ Open 2014, 4, e006544. [Google Scholar] [CrossRef]
- Fahrni, M.L.; Azmy, M.T.; Usir, E.; Aziz, N.A.; Hassan, Y. Inappropriate prescribing defined by STOPP and START criteria and its association with adverse drug events among hospitalized older patients: A multicentre, prospective study. PLoS ONE 2019, 14, e0219898. [Google Scholar] [CrossRef]
- Potter, E.L.; Lew, T.E.; Sooriyakumaran, M.; Edwards, A.M.; Tong, E.; Aung, A.K. Evaluation of pharmacist-led physician-supported inpatient deprescribing model in older patients admitted to an acute general medical unit. Australas. J. Ageing 2019, 38, 206–210. [Google Scholar] [CrossRef]
- Crook, M.; Ajdukovic, M.; Angley, C.; Soulsby, N.; Doecke, C.; Stupans, I.; Angley, M. Eliciting comprehensive medication histories in the emergency department: The role of the pharmacist. Pharm. Pract. 2007, 5, 78–84. [Google Scholar] [CrossRef]
- Marshall, J.; Hayes, B.D.; Koehl, J.; Hillmann, W.; Bravard, M.A.; Jacob, S.; Gil, R.; Mitchell, E.; Ferrante, F.; Giulietti, J.; et al. Effects of a pharmacy-driven medication history program on patient outcomes. Am. J. Health Syst. Pharm. 2022, 79, 1652–1662. [Google Scholar] [CrossRef]
- Jovevski, J.J.; Smith, C.R.; Roberts, J.L.; Dev, S.; Iloabuchi, T.C.; Gruber, E.A.; Williams, M.J.; Slaven, J.E.; Mitchell, A.M. Implementation of a compulsory clinical pharmacist-led medication deprescribing intervention in high-risk seniors in the emergency department. Acad. Emerg. Med. 2023, 30, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Kuntz, J.L.; Kouch, L.; Christian, D.; Hu, W.; Peterson, P.L. Patient Education and Pharmacist Consultation Influence on Nonbenzodiazepine Sedative Medication Deprescribing Success for Older Adults. Perm. J. 2019, 23, 18–161. [Google Scholar] [CrossRef] [PubMed]
- Bayliss, E.A.; Shetterly, S.M.; Drace, M.L.; Norton, J.D.; Maiyani, M.; Gleason, K.S.; Sawyer, J.K.; Weffald, L.A.; Green, A.R.; Reeve, E.; et al. Deprescribing Education vs Usual Care for Patients With Cognitive Impairment and Primary Care Clinicians: The OPTIMIZE Pragmatic Cluster Randomized Trial. JAMA Intern. Med. 2022, 182, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.; Tayes, C.; Toda, K.; Hayes, B.; Lee, S.; Liu, S.; Selman, K.; Thatphet, P.; Skains, R. 132 Geriatric Emergency Department Guidelines 2.0: A Systematic Review of Emergency Department-Based Geriatric Medication Programs to Reduce Potentially Inappropriate Medications and Adverse Events. Ann. Emerg. Med. 2023, 82, S57. [Google Scholar] [CrossRef]
- Jay, S.; Whittaker, P.; Mcintosh, J.; Hadden, N. Can consultant geriatrician led comprehensive geriatric assessment in the emergency department reduce hospital admission rates? A systematic review. Age Ageing 2016, 46, 366–372. [Google Scholar] [CrossRef]
- Wheeler, A.J.; Scahill, S.; Hopcroft, D.; Stapleton, H. Reducing medication errors at transitions of care is everyone’s business. Aust. Prescr. 2018, 41, 73. [Google Scholar] [CrossRef]
- Bloomfield, H.E.; Greer, N.; Linsky, A.M.; Bolduc, J.; Naidl, T.; Vardeny, O.; MacDonald, R.; McKenzie, L.; Wilt, T.J. Deprescribing for community-dwelling older adults: A systematic review and meta-analysis. J. Gen. Intern. Med. 2020, 35, 3323–3332. [Google Scholar] [CrossRef]
- 6.2 Medication Management Reviews, 75 Years and Over; Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2021. Available online: https://www.safetyandquality.gov.au/sites/default/files/2021-04/fourth_atlas_2021_-_6.2_medications_management_reviews_75_years_and_over_0.pdf (accessed on 24 December 2023).
- Hospital-Initiated Medication Reviews; Transitions of Care and Primary Care Leadership Committee, The Society of Hospital Pharmacists of Australia: Collingwood, Australia, 2020.
- Powell, C.; Tomlinson, J.; Quinn, C.; Fylan, B. Interventions for self-management of medicines for community-dwelling people with dementia and mild cognitive impairment and their family carers: A systematic review. Age Ageing 2022, 51, afac089. [Google Scholar] [CrossRef]
- Elliott, R.A.; Goeman, D.; Beanland, C.; Koch, S. Ability of older people with dementia or cognitive impairment to manage medicine regimens: A narrative review. Curr. Clin. Pharmacol. 2015, 10, 213–221. [Google Scholar] [CrossRef]

| Presence of Polypharmacy | Absence of Polypharmacy | p-Value | |
|---|---|---|---|
| N = 161 (80.5%) | N = 39 (19.5) | ||
| Age, mean (SD), years | 82.0 (8.4) | 76.2 (9.1) | <0.001 |
| Sex, n (%) | 0.19 | ||
| Male | 60 (37.3%) | 19 (48.7%) | |
| Female | 101 (62.7%) | 20 (51.3%) | |
| Mode of presentation, n (%) | 0.89 | ||
| Ambulance | 119 (73.9%) | 30 (76.9%) | |
| Community transport | 9 (5.6%) | 1 (2.6%) | |
| Other | 33 (20.5%) | 8 (20.5%) | |
| ATS, n (%) | 0.62 | ||
| 1 | 1 (0.6%) | 0 (0%) | |
| 2 | 16 (9.9%) | 6 (15.4%) | |
| 3 | 90 (55.9%) | 24 (61.6%) | |
| 4 | 52 (32.3%) | 9 (23.0%) | |
| 5 | 2 (1.2%) | 0 (0%) | |
| Accommodation before presentation, n (%) | 0.99 | ||
| Home | 139 (86.3%) | 34 (87.2%) | |
| Other | 22 (13.7%) | 5 (12.8%) | |
| Co-morbidities, n (%) | |||
| Hypertension | 126 (78.3%) | 16 (44.4%) | |
| Dyslipidaemia | 89 (55.3%) | 6 (16.7%) | |
| Arthritis | 53 (32.9%) | 3 (8.3%) | |
| Diabetes | 52 (32.3%) | 6 (16.7%) | |
| Atrial fibrillation/arrhythmia | 50 (31.1%) | 4 (11.1%) | |
| Depression/anxiety | 49 (30.4%) | 6 (16.7%) | |
| Osteoporosis | 47 (29.2%) | 4 (11.1%) | |
| Ischaemic heart disease | 46 (28.6%) | 2 (5.6%) | |
| Asthma/COPD | 43 (26.7%) | 2 (5.6%) | |
| Cancer | 33 (20.5%) | 4 (11.1%) | |
| Allergy present, n (%) | 0.48 | ||
| Yes | 72 (44.7%) | 15 (38.5%) | |
| No | 89 (55.3%) | 24 (61.5%) | |
| Number of allergies *, median (IQR) | 1 (1–3) | 2 (1–3) | 0.85 |
| Total number of regular home medications, median (IQR) | 9 (6–12) | 3 (2–4) | <0.001 |
| Total number of PRN medications, median (IQR) | 1 (0–2) | 0 (0–1) | 0.002 |
| Category of STOPP/START | STOPP Proportion of Patients 81 (40.5%) | START Proportion of Patients 177 (88.5%) |
|---|---|---|
| A | 33 (40.7%) | 37 (20.9%) |
| B | 4 (4.9%) | 7 (3.9%) |
| C | 6 (7.4%) | 10 (5.6%) |
| D | 27 (33.3%) | 0 |
| E | 2 (2.5%) | 35 (19.8%) |
| F | 2 (2.5%) | 1 (0.6%) |
| G | 1 (1.2%) | 0 |
| H | 1 (1.2%) | 0 |
| I | 1 (1.2%) | 87 (49.1%) |
| L | 4 (4.9%) | - |
| Total | 81 (100%) | 177 (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, H.T.M.; Roman, C.; Yip, G.; Dooley, M.; Salahudeen, M.S.; Mitra, B. Influence of Potentially Inappropriate Medication Use on Older Australians’ Admission to Emergency Department Short Stay. Geriatrics 2024, 9, 6. https://doi.org/10.3390/geriatrics9010006
Tran HTM, Roman C, Yip G, Dooley M, Salahudeen MS, Mitra B. Influence of Potentially Inappropriate Medication Use on Older Australians’ Admission to Emergency Department Short Stay. Geriatrics. 2024; 9(1):6. https://doi.org/10.3390/geriatrics9010006
Chicago/Turabian StyleTran, Hoa T. M., Cristina Roman, Gary Yip, Michael Dooley, Mohammed S. Salahudeen, and Biswadev Mitra. 2024. "Influence of Potentially Inappropriate Medication Use on Older Australians’ Admission to Emergency Department Short Stay" Geriatrics 9, no. 1: 6. https://doi.org/10.3390/geriatrics9010006