
Implementation of a Multicomponent Otago-Based Virtual Fall Reduction, Education, and Exercise Program (MOVing FREEly) in Older Veterans

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Participants
2.2. Program Design and Implementation
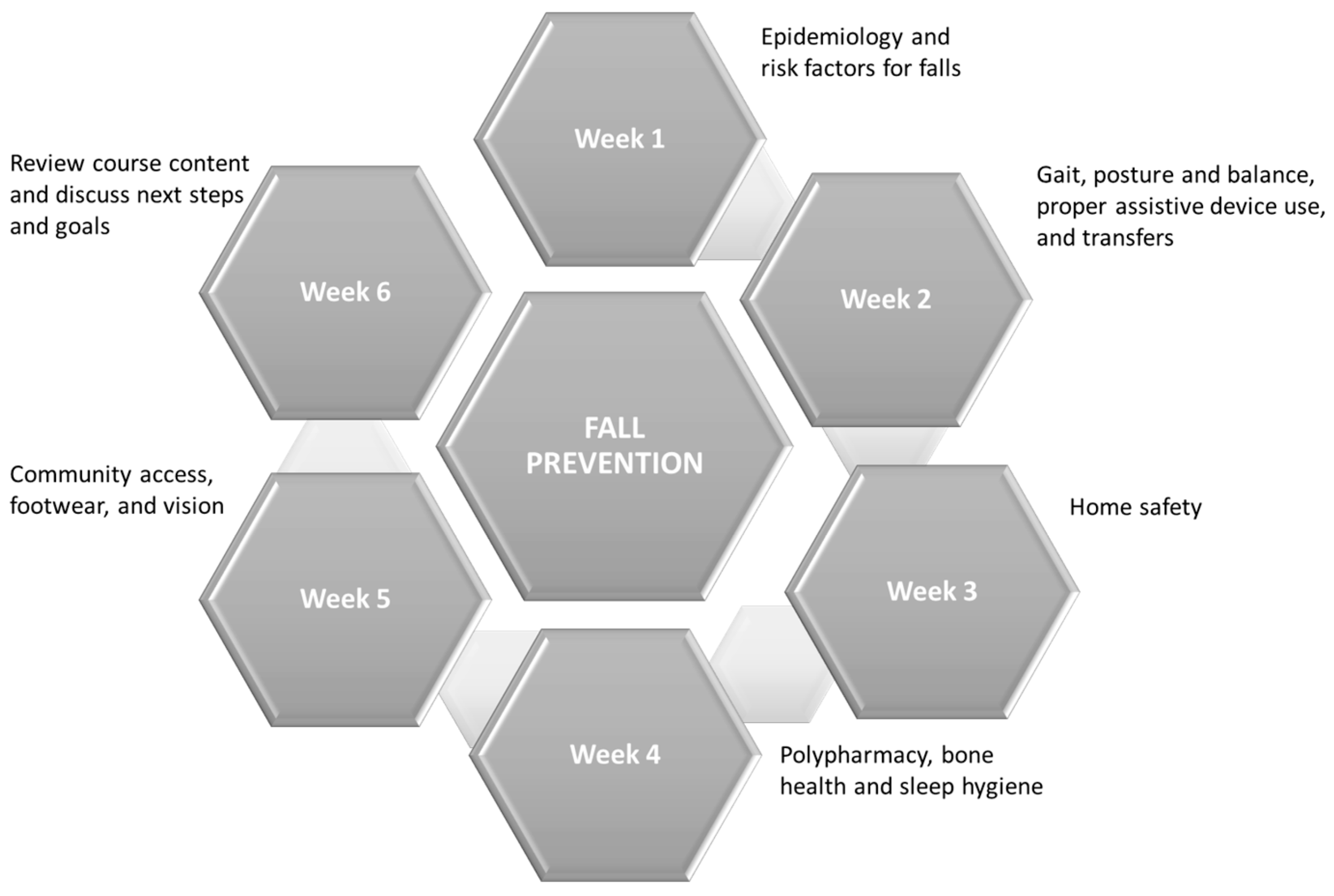
2.3. Education Program
2.4. Exercise Program
2.5. Measurements and Analysis
3. Results
3.1. Feasibility of Program
3.2. Acceptability of Program
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rubenstein, L. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef] [PubMed]
- Florence, C.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical Costs of Fatal and Nonfatal Falls in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. 2016. Web-based Injury Statistics Query and Reporting System (WISQARS): Leading Causes of Death and Injury—PDFs|Injury Center|CDC. Available online: https://www.cdc.gov/injury/wisqars/LeadingCauses.html (accessed on 28 October 2023).
- Hartholt, K.; Lee, R.; Burns, E. Mortality from falls among US adults aged 75 years or older 2000–2016. JAMA 2019, 321, 2131–2133. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M.; Campbell, A.; Gardner, M.; Devin, N. Preventing Injuries in Older People by Preventing Falls: A Meta-Analysis of Individual-Level Data. J. Am. Geriatr. Soc. 2002, 50, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, L.; Robertson, M.; Gillespie, W.; Sherrington, C.; Gates, S.; Clemson, L.; Lamb, S. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 2012, CD007146. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.; Thomas, S.; Veroniki, A.; Hamid, J.; Cogo, E.; Striffer, L. Comparisons of interventions for preventing falls in older adults: As systematic review and meta-analysis. JAMA 2017, 318, 1687–1699. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; van der Velde, N.; Martin, F.C.; Petrovic, M.; Tan, M.P.; Ryg, J.; Aguilar-Navarro, S.; Alexander, N.B.; Becker, C.; Blain, H.; et al. Task Force on Global Guidelines for Falls in Older, A. World guidelines for falls prevention and management for older adults: A global initiative. Age Ageing 2022, 51, afac205. [Google Scholar] [CrossRef]
- Mani, S.; Sharma, S.; Omar, B.; Paungmali, A.; Joseph, L. Validity and reliability of Internet-based physiotherapy assessment for musculoskeletal disorders: A systematic review. J. Telemed. Telecare 2017, 23, 379–391. [Google Scholar] [CrossRef]
- Cottrell, M.A.; Galea, O.A.; O’Leary, S.P.; Hill, A.J.; Russell, T.G. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 625–638. [Google Scholar] [CrossRef]
- Hwang, R.; Morris, N.R.; Mandrusiak, A.; Bruning, J.; Peters, R.; Korczyk, D.; Russell, T. Cost-Utility Analysis of Home-Based Telerehabilitation Compared With Centre-Based Rehabilitation in Patients With Heart Failure. Heart Lung Circ. 2019, 28, 1795–1803. [Google Scholar] [CrossRef]
- Kairy, D.; Lehoux, P.; Vincent, C.; Visintin, M. A systematic review of clinical outcomes, clinical process, healthcare utilization and costs associated with telerehabilitation. Disabil. Rehabil. 2009, 31, 427–447. [Google Scholar] [CrossRef] [PubMed]
- Bernocchi, P.; Vanoglio, F.; Baratti, D.; Morini, R.; Rocchi, S.; Luisa, A.; Scalvini, S. Home-based telesurveillance and rehabilitation after stroke: A real-life study. Top. Stroke Rehabil. 2016, 23, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Office of Connected Care: Telerehabilitation and Prosthetic Services. Available online: https://vaww.telehealth.va.gov/clinic/rehab/trehb/index.asp (accessed on 20 March 2023).
- Kintzle, S.; Rivas, W.A.; Castro, C.A. Satisfaction of the Use of Telehealth and Access to Care for Veterans During the COVID-19 Pandemic. Telemedicine and e-Health 2022, 28, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Nicosia, F.M.; Kaul, B.; Totten, A.M.; Silvestrini, M.C.; Williams, K.; Whooley, M.A.; Sarmiento, K.F. Leveraging Telehealth to improve access to care: A qualitative evaluation of Veterans’ experience with the VA TeleSleep program. BMC Health Serv. Res. 2021, 21, 77. [Google Scholar] [CrossRef] [PubMed]
- Darkins, A. The growth of telehealth services in the Veterans Health Administration between 1994 and 2014: A study in the diffusion of innovation. Telemedicine and e-Health 2014, 20, 761–768. [Google Scholar] [CrossRef]
- Alexander, N.B.; Phillips, K.; Wagner-Felkey, J.; Chan, C.L.; Hogikyan, R.; Sciaky, A.; Cigolle, C. Team VA Video Connect (VVC) to optimize mobility and physical activity in post-hospital discharge older veterans: Baseline assessment. BMC Geriatr. 2021, 21, 502. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, D.; Wilkins, S.S.; Melrose, R.J.; Hall, K.M.; Abbate, L.M.; Morey, M.C.; Castle, S.C.; Zeng, A.; Lee, C.C. Physical Function Effects of Live Video Group Exercise Interventions for Older Adults: A Systematic Review and Veteran’s Gerofit Group Case Study. Telemedicine and e-Health 2022, 29, 829–840. [Google Scholar] [CrossRef]
- Pimentel, C.B.; Gately, M.; Barczi, S.R.; Boockvar, K.S.; Bowman, E.H.; Caprio, T.V.; Colon-Emeric, C.S.; Dang, S.; Espinoza, S.E.; Garner, K.K.; et al. GRECC Connect: Geriatrics Telehealth to Empower Health Care Providers and Improve Management of Older Veterans in Rural Communities. Fed. Pract. 2019, 36, 464–470. [Google Scholar]
- Stevens, J. The STEADI tool kit: A fall prevention resource for healthcare providers. IHS Prim. Care Provid. 2013, 38, 162. [Google Scholar]
- Mahoney, J.; Clemson, L.; Schlottauer, A.; Mack, K.; Shea, T.; Gobel, V.; Cech, S. Modified Delphi Consensus to Suggest key Elements of Stepping On Falls Prevention Program. Front. Public Health 2017, 5, 21. [Google Scholar] [CrossRef]
- Clemson, L.; Cumming, R.; Kendig, H.; Swann, M.; Heard, R.; Taylor, K. The effectiveness of a community-based program for reducing the incidence of falls in the elderly: A randomized trial. J. Am. Geriatr. Soc. 2004, 52, 1487–1494. [Google Scholar] [CrossRef] [PubMed]
- Tennstedt, S.; Howland, J.; Lachman, M.; Peterson, E.; Kasten, L.; Jette, A. A randomized, controlled trial of a group intervention to reduce fear of falling and associated activity restriction in older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 1998, 53, P384–P392. [Google Scholar] [CrossRef] [PubMed]
- Haynes, M.; League, P.; Neault, G. A matter of balance: Older adults taking control of falls by building confidence. Front. Public Health 2014, 2, 274. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.; Robertson, M.; Gardner, M.; Norton, R.; Buchner, D. Falls prevention over 2 years: A randomized controlled trial in women 80 years and older. Age Ageing 1999, 28, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.; Rikli, R.; Beam, W. A 30s Chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 2013, 70, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.; Wayne, S.; Romero, L.; Baumgartner, R.; Rubenstein, L.; Garry, P. One-leg balance is an important predictor of injurious falls in older persons. J. Am. Geriatr. Soc. 1997, 46, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Shubert, T.E.; Chokshi, A.; Mendes, V.M.; Grier, S.; Buchanan, H.; Basnett, J.; Smith, M.L. Stand Tall-A Virtual Translation of the Otago Exercise Program. J. Geriatr. Phys. Ther. 2020, 43, 120–127. [Google Scholar] [CrossRef]
- Rubenstein, L.; Vivrette, R.; Harkr, J.; Stevens, J.; Kramer, B. Validating an evidence-based, self-rated fall risk questionnaire (FRQ) for older adults. J. Saf. Res. 2011, 42, 493–499. [Google Scholar] [CrossRef]
- Kempen, G.; Yardley, L.; Van Haastreg, J.; Zijlstra, G.; Beyer, N.; Hauer, K.; Todd, C. The Short FES-I: A shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing 2008, 37, 45–50. [Google Scholar] [CrossRef]
- Delbaere, K.; Close, J.C.; Mikolaizak, A.S.; Sachdev, P.S.; Brodaty, H.; Lord, S.R. The Falls Efficacy Scale International (FES-I). A comprehensive longitudinal validation study. Age Ageing 2010, 39, 210–216. [Google Scholar] [CrossRef]
- Wu, G.; Keyes, L.M. Group tele-exercise for improving balance in elders. Telemed. e-Health 2006, 12, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Kong, H.J.; Yoon, H.J. Web-Based Telepresence Exercise Program for Community-Dwelling Elderly Women With a High Risk of Falling: Randomized Controlled Trial. JMIR Mhealth Uhealth 2018, 6, e132. [Google Scholar] [CrossRef] [PubMed]
- Pew Research Center, Mobile Fact Sheet. Available online: https://www.pewresearch.org/internet/fact-sheet/mobile/ (accessed on 11 July 2023).
- Hoerster, K.; Lehavot, K.; Simpson, T.; McFall, M.; Reiber, G.; Nelson, K. Health and health behavior differences: U.S. Military, veteran, and civilian men. Am. J. Prev. Med. 2012, 43, 483–489. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sex, Male, n(%) | 24 (89.0%) |
| Age, mean (SD, range) | 75 (5.11, 64–85) |
| Race, white, n (%) | 23 (85.2%) |
| Time to Seattle VA, minutes, median (SD) | 80.2 min (±45.7) |
| Fallen within the last 12 mo, n (%) | 25 (92.6%) |
| Fall that caused an injury, n (%) | 8 (29.6%) |
| Fear of falling, n (%) | 22 (81.5%) |
| Unsteady when walking, n (%) | 23 (85.2%) |
| Use arms to stand up from a chair, n (%) | 21 (77.8%) |
| Week | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| Education | 91 | 97 | 81 | 88 | 91 | 84 |
| Exercise—overall | 77 | 87 | 87 | 83 | 80 | 86 |
| Exercise—group | 100 | 100 | 100 | 83 | 75 | 83 |
| Exercise—individual | 61 | 78 | 78 | 83 | 83 | 89 |
| Program Component | Tips | Rationale |
|---|---|---|
| Logistical considerations |
|
|
| Enrollment |
|
|
| Management and delivery of class content |
|
|
| End of Program (N = 26) | n (%) | Three Month Follow Up (N = 21) | n (%) |
|---|---|---|---|
| Fall during class | 19 (73.1%) | Fall since class ended | 7 (33.3%) |
| Reduced your fear of falling | 26 (100%) | Reduced your fear of falling | 20 (95.2%) |
| Improvement in strength, balance | 20 (76.9%) | Continued confidence in falling risk reduction | 20 (95.2%) |
| I feel more comfortable talking to HCP about medications | 23 (88.5%) | Made medication changes | 10 (47.6%) |
| Plan to continue exercising | 25 (96.1%) | Exercising at least weekly | 14 (66.7%) |
| I have made changes to my home environment to reduce risk | 19 (73.1%) | Has continued to reduce risky behaviors | 19 (90.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ritchey, K.C.; Olney, A.; Chen, S.; Martinez, E.; Paulsen, M.R.; Tunoa, J.; Powers, J.S. Implementation of a Multicomponent Otago-Based Virtual Fall Reduction, Education, and Exercise Program (MOVing FREEly) in Older Veterans. Geriatrics 2023, 8, 115. https://doi.org/10.3390/geriatrics8060115
Ritchey KC, Olney A, Chen S, Martinez E, Paulsen MR, Tunoa J, Powers JS. Implementation of a Multicomponent Otago-Based Virtual Fall Reduction, Education, and Exercise Program (MOVing FREEly) in Older Veterans. Geriatrics. 2023; 8(6):115. https://doi.org/10.3390/geriatrics8060115
Chicago/Turabian StyleRitchey, Katherine C., Amanda Olney, Sunny Chen, Erica Martinez, Michelle R. Paulsen, Jennifer Tunoa, and James S. Powers. 2023. "Implementation of a Multicomponent Otago-Based Virtual Fall Reduction, Education, and Exercise Program (MOVing FREEly) in Older Veterans" Geriatrics 8, no. 6: 115. https://doi.org/10.3390/geriatrics8060115