
Virtual Dementia-Friendly Communities (Verily Connect) Stepped-Wedge Cluster-Randomised Controlled Trial: Improving Dementia Caregiver Wellbeing in Rural Australia

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
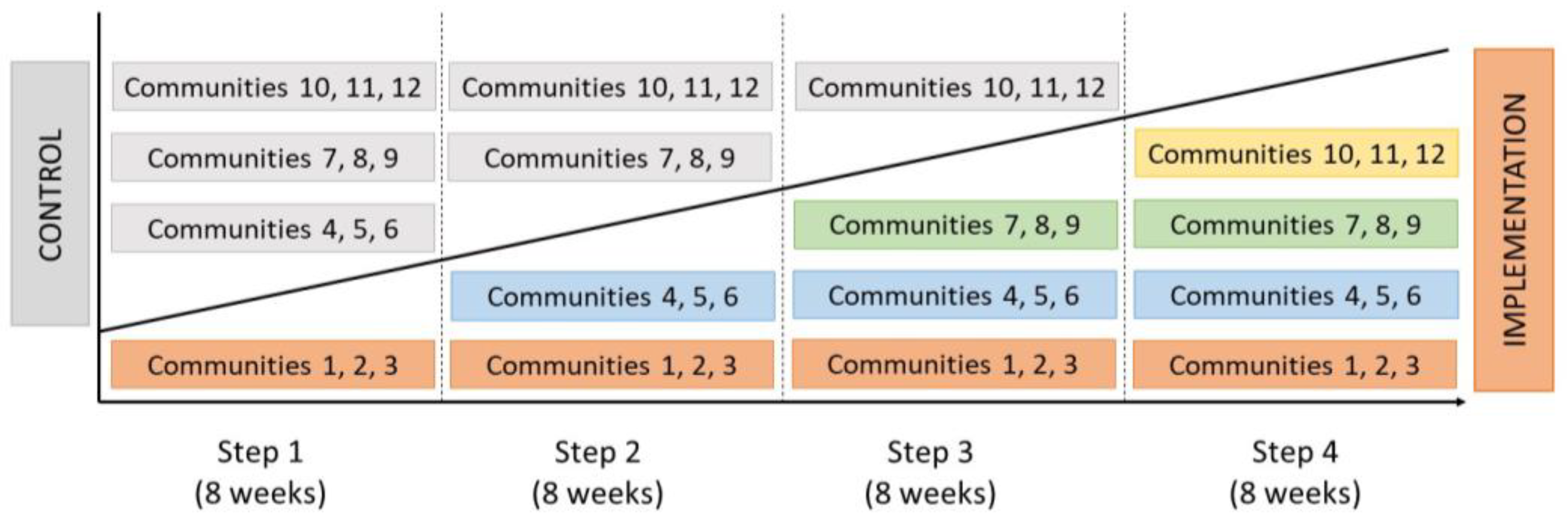
2.1. Study Design
- -
- An integrated website and mobile app (Verily Connect app).
- -
- Volunteer support and a Technology Learning Centre (Verily Connect Hub) that was physically located in each rural community.
- -
- Caregiver peer support groups that met via web-based videoconference.
2.2. Ethics Approval
2.3. Trial Registration

2.4. Study Setting and Sample
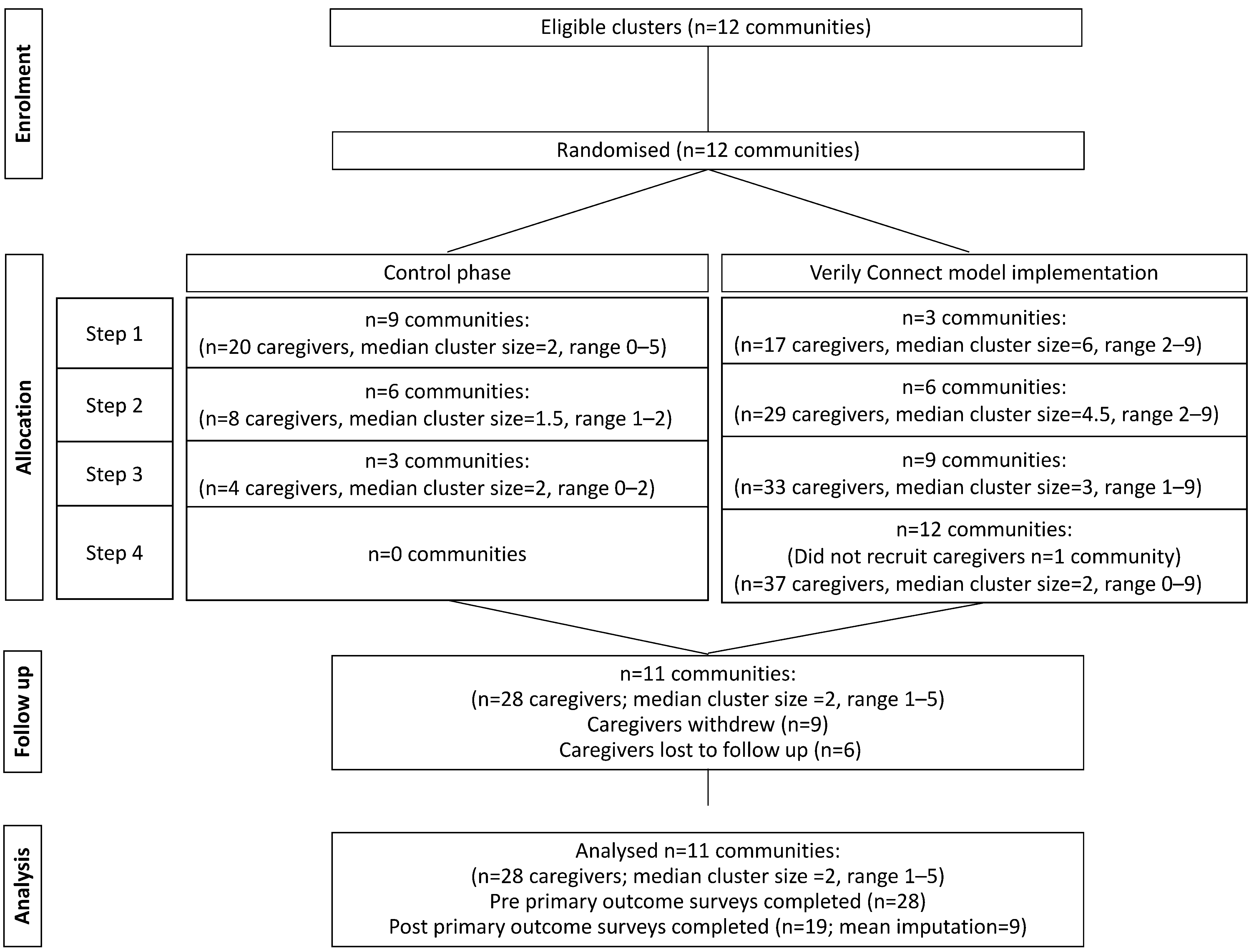
2.5. Recruitment
2.6. Data Collection and Analysis
3. Results
3.1. Caregiver Perceived Social Support and Demand
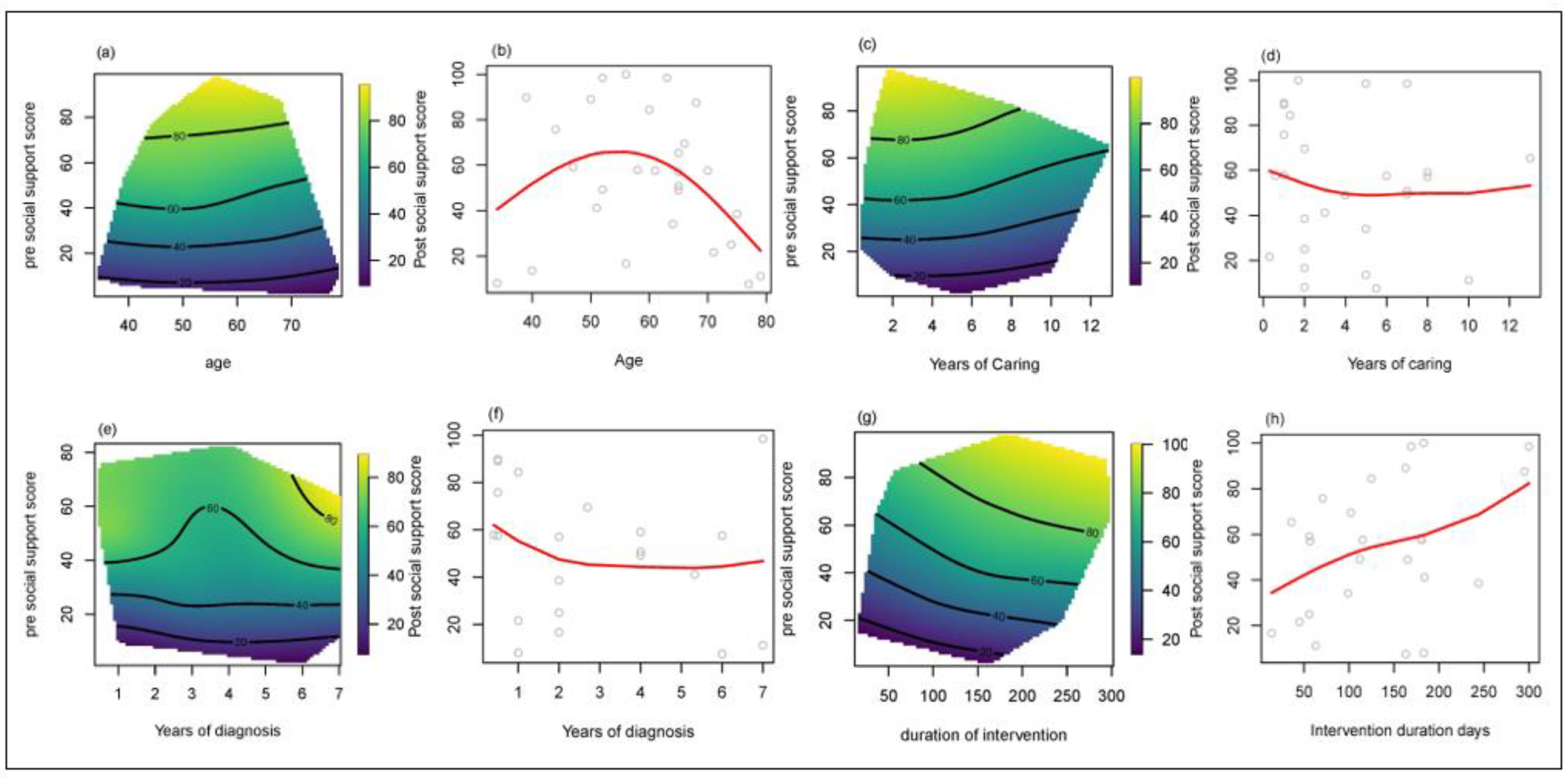
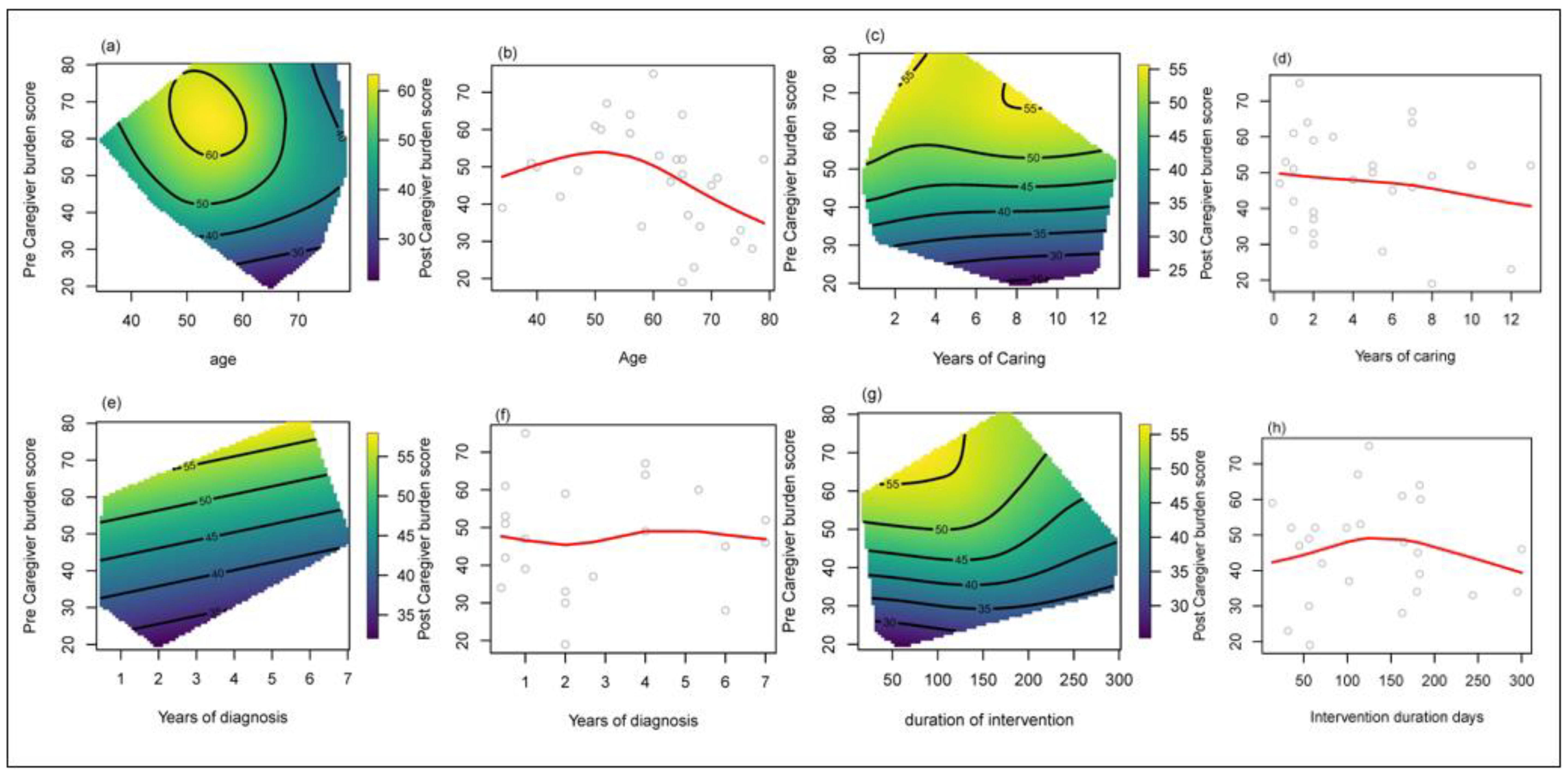
3.2. Effect of Age, Years in Caring Role, and Duration of Intervention Exposure Time (Days) on Social Support and Caregiver Demand
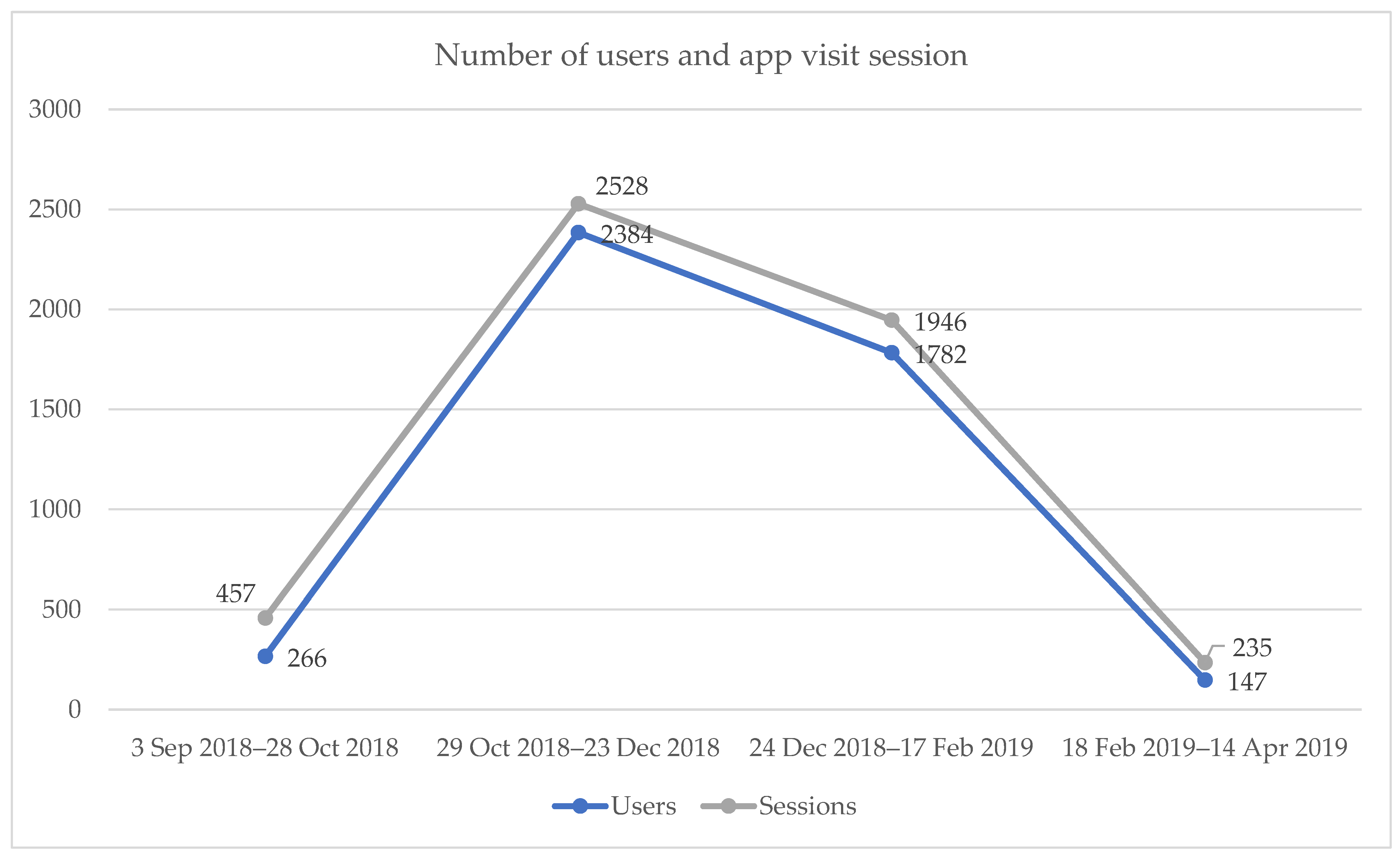
3.3. Engagement with Verily Connect Website/App
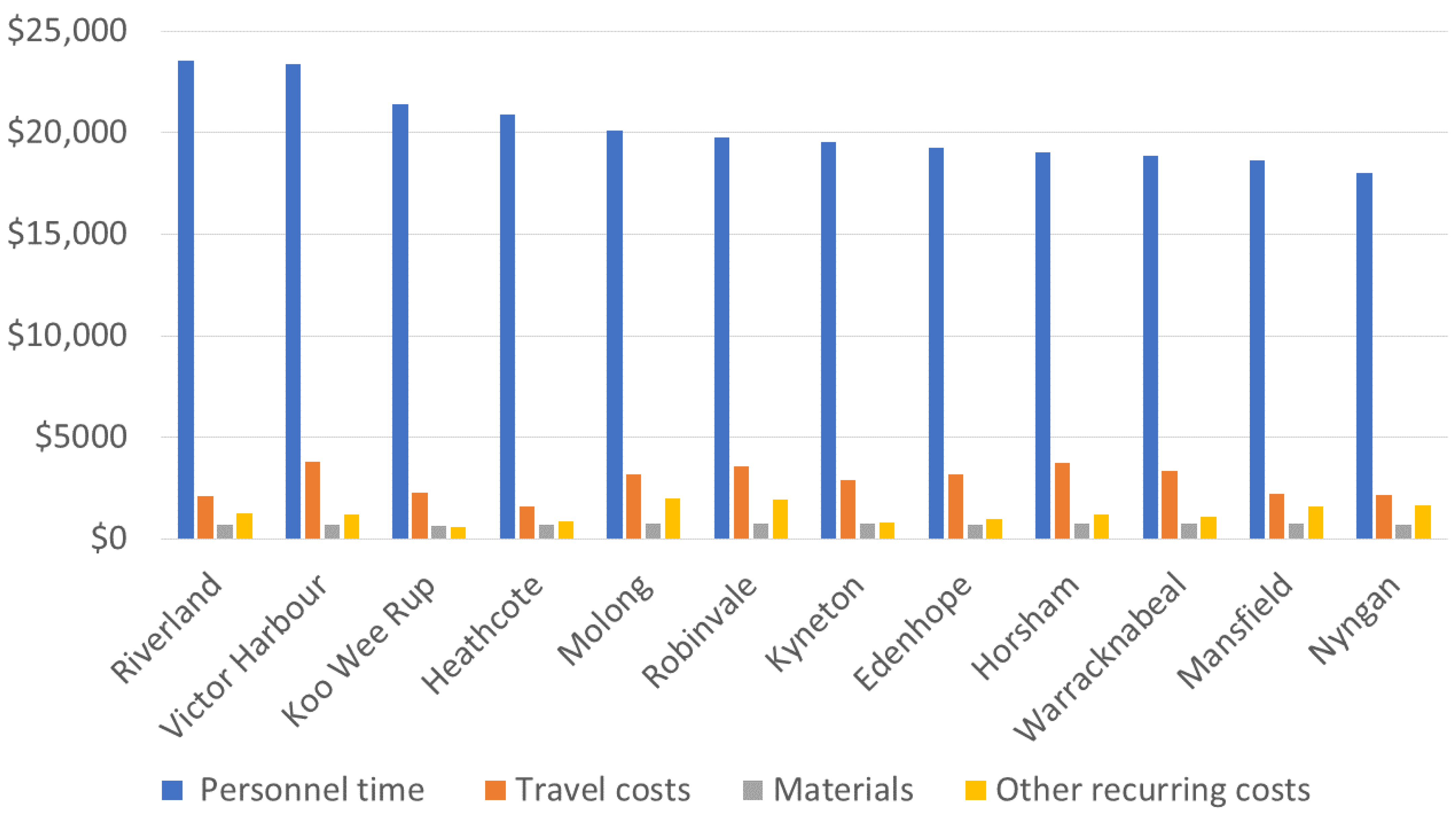
3.4. Cost Estimates and Analysis
4. Discussion
4.1. Primary Results
4.2. Study Strengths and Limitations
4.3. Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MOS-SSS | Medical Outcomes Study-Social Support Survey |
| ZBI | Zarit Burden Interview |
References
- Goodman, R.A.; Lochner, K.A.; Thambisetty, M.; Wingo, T.S.; Posner, S.F.; Ling, S.M. Prevalence of dementia subtypes in United States Medicare fee-for-service beneficiaries, 2011–2013. Alzheimer’s Dement. 2017, 13, 28–37. [Google Scholar] [CrossRef]
- Schulz, R.; Martire, L.M. Family Caregiving of Persons with Dementia: Prevalence, Health Effects, and Support Strategies. Am. J. Geriatr. Psychiatry 2004, 12, 240–249. [Google Scholar] [CrossRef]
- Papastavrou, E.; Andreou, P.; Middleton, N.; Tsangari, H.; Papacostas, S. Dementia Caregiver Burden Association with Community Participation Aspect of Social Capital. J. Adv. Nurs. 2015, 71, 2898–2910. [Google Scholar] [CrossRef]
- Elvish, R.; Cawley, R.; Keady, J. The experiences of therapy from the perspectives of carers of people with dementia: An exploratory study. Couns. Psychother. Res. 2014, 14, 56–63. [Google Scholar] [CrossRef]
- Schofield, H.; Murphy, B.; Herrman, H.E.; Bloch, S.; Singh, B.S. Carers of people aged over 50 with physical impairment, memory loss and dementia: A comparative study. Ageing Soc. 1998, 18, 355–369. [Google Scholar] [CrossRef]
- Morgan, D.; Kosteniuk, J.; O’Connell, M.E.; Kirk, A.; Stewart, N.J.; Seitz, D.; Bayly, M.; Froehlich Chow, A.; Elliot, V.; Daku, J.; et al. Barriers and facilitators to development and implementation of a rural primary health care intervention for dementia: A process evaluation. BMC Health Serv. Res. 2019, 19, 709. [Google Scholar] [CrossRef]
- Lane, C.A.; Hardy, J.; Schott, J.M. Alzheimer’s disease. Eur. J. Neurol. 2018, 25, 59–70. [Google Scholar] [CrossRef]
- Umstattd Meyer, M.R.; Janke, M.C.; Beaujean, A.A. Predictors of older adults’ personal and community mobility: Using a comprehensive theoretical mobility framework. Gerontologist 2014, 54, 398–408. [Google Scholar] [CrossRef] [PubMed]
- Longstreth, M.; McKibbin, C.; Steinman, B.; Slosser Worth, A.; Carrico, C. Exploring Information and Referral Needs of Individuals with Dementias and Informal Caregivers in Rural and Remote Areas. Clin. Gerontol. 2022, 45, 808–820. [Google Scholar] [CrossRef] [PubMed]
- Krutter, S.; Schaffler-Schaden, D.; Essl-Maurer, R.; Wurm, L.; Seymer, A.; Kriechmayr, C.; Mann, E.; Osterbrink, J.; Flamm, M. Comparing perspectives of family caregivers and healthcare professionals regarding caregiver burden in dementia care: Results of a mixed methods study in a rural setting. Age Ageing 2020, 49, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Górska, S.; Forsyth, K.; Irvine, L.; Maciver, D.; Prior, S.; Whitehead, J.; Flockhart, J.; Fairnie, J.; Reid, J. Service-related needs of older people with dementia: Perspectives of service users and their unpaid carers. Int. Psychogeriatr. 2013, 25, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Phillipson, L.; Magee, C.; Jones, S.; Reis, S.; Skladzien, E. Dementia attitudes and help-seeking intentions: An investigation of responses to two scenarios of an experience of the early signs of dementia. Aging Ment. Health 2015, 19, 968–977. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, M.E.; Crossley, M.; Cammer, A.; Morgan, D.; Allingham, W.; Cheavins, B.; Dalziel, D.; Lemire, M.; Mitchell, S.; Morgan, E. Development and evaluation of a telehealth videoconferenced support group for rural spouses of individuals diagnosed with atypical early-onset dementias. Dementia 2014, 13, 382–395. [Google Scholar] [CrossRef] [PubMed]
- McKechnie, V.; Barker, C.; Stott, J. Effectiveness of computer-mediated interventions for informal carers of people with dementia-a systematic review. Int. Psychogeriatr. 2014, 26, 1619–1637. [Google Scholar] [CrossRef] [PubMed]
- Deeken, F.; Rezo, A.; Hinz, M.; Discher, R.; Rapp, M.A. Evaluation of Technology-Based Interventions for Informal Caregivers of Patients With Dementia-A Meta-Analysis of Randomized Controlled Trials. Am. J. Geriatr. Psychiatry 2019, 27, 426–445. [Google Scholar] [CrossRef] [PubMed]
- Bui, L.K.; Park, M.; Giap, T.T. eHealth interventions for the informal caregivers of people with dementia: A systematic review of systematic reviews. Geriatr. Nurs. 2022, 48, 203–213. [Google Scholar] [CrossRef]
- Wilding, C.; Davis, H.; Rasekaba, T.; Hamiduzzaman, M.; Royals, K.; Greenhill, J.; O’Connell, M.E.; Perkins, D.; Bauer, M.; Morgan, D.; et al. Volunteers’ Support of Carers of Rural People Living with Dementia to Use a Custom-Built Application. Int. J. Environ. Res. Public Health 2021, 18, 9909. [Google Scholar] [CrossRef]
- Highfield, L.; Rajan, S.S.; Valerio, M.A.; Walton, G.; Fernandez, M.E.; Bartholomew, L.K. A non-randomized controlled stepped wedge trial to evaluate the effectiveness of a multi-level mammography intervention in improving appointment adherence in underserved women. Implement. Sci. 2015, 10, 143. [Google Scholar] [CrossRef]
- Hemming, K.; Haines, T.P.; Chilton, P.J.; Girling, A.J.; Lilford, R.J. The stepped wedge cluster randomised trial: Rationale, design, analysis, and reporting. BMJ 2015, 350, h391. [Google Scholar] [CrossRef]
- Wilding, C.; Morgan, D.; Greenhill, J.; Perkins, D.; O’Connell, M.E.; Bauer, M.; Farmer, J.; Morley, C.; Blackberry, I. Web-Based Technologies to Support Carers of People Living With Dementia: Protocol for a Mixed Methods Stepped-Wedge Cluster Randomized Controlled Trial. JMIR Res. Protoc. 2022, 11, e33023. [Google Scholar] [CrossRef]
- La Trobe University. Welcome to Verily Connect. Available online: Verilyconnect.org.au (accessed on 13 February 2023).
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef] [PubMed]
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Dumville, J.C.; Torgerson, D.J.; Hewitt, C.E. Reporting attrition in randomised controlled trials. BMJ 2006, 332, 969–971. [Google Scholar] [CrossRef] [PubMed]
- McCoy, C.E. Understanding the Intention-to-treat Principle in Randomized Controlled Trials. West. J. Emerg. Med. 2017, 18, 1075–1078. [Google Scholar] [CrossRef]
- Mirzaei, A.; Carter, S.R.; Patanwala, A.E.; Schneider, C.R. Missing data in surveys: Key concepts, approaches, and applications. Res. Soc. Adm. Pharm. 2022, 18, 2308–2316. [Google Scholar] [CrossRef]
- Singer, J.D.; Willett, J.B. Modeling Discontinuous and Nonlinear Change. In Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence; Singer, J.D., Willett, J.B., Eds.; Oxford University Press: New York, NY, USA, 2003; pp. 189–242. [Google Scholar] [CrossRef]
- Desquilbet, L.; Mariotti, F. Dose-response analyses using restricted cubic spline functions in public health research. Stat. Med. 2010, 29, 1037–1057. [Google Scholar] [CrossRef]
- Blackberry, I.; Wilding, C.; Morgan, D.; Winbolt, M.; Greenhill, J.; Perkins, D.; O’Connell, M.; Bauer, M.; Morley, C.; Farmer, J. Virtual Dementia Friendly Rural Communities (Verily) Project Final Report. 2021. Available online: https://www.latrobe.edu.au/__data/assets/pdf_file/0006/1173498/Verily-Connect-Final-Report.pdf (accessed on 18 July 2023).
- Park, S.; Freeman, J.; Middleton, C. Intersections between connectivity and digital inclusion in rural communities. Commun. Res. Pract. 2019, 5, 139–155. [Google Scholar] [CrossRef]
- Bong, W.K.; Bergland, A.; Chen, W. Technology Acceptance and Quality of Life among Older People Using a TUI Application. Int. J. Environ. Res. Public Health 2019, 16, 4706. [Google Scholar] [CrossRef]
- Meyerowitz-Katz, G.; Ravi, S.; Arnolda, L.; Feng, X.; Maberly, G.; Astell-Burt, T. Rates of attrition and dropout in app-based interventions for chronic disease: Systematic review and meta-analysis. J. Med. Internet Res. 2020, 22, e20283. [Google Scholar] [CrossRef]
- Hopwood, J.; Walker, N.; McDonagh, L.; Rait, G.; Walters, K.; Iliffe, S.; Ross, J.; Davies, N. Internet-Based Interventions Aimed at Supporting Family Caregivers of People With Dementia: Systematic Review. J. Med. Internet Res. 2018, 20, e216. [Google Scholar] [CrossRef]
- Span, M.; Smits, C.; Jukema, J.; Groen-van de Ven, L.; Janssen, R.; Vernooij-Dassen, M.; Eefsting, J.; Hettinga, M. An Interactive Web Tool for Facilitating Shared Decision-Making in Dementia-Care Networks: A Field Study. Front. Aging Neurosci. 2015, 7, 128. [Google Scholar] [CrossRef] [PubMed]
- Egan, K.J.; Pinto-Bruno, Á.C.; Bighelli, I.; Berg-Weger, M.; van Straten, A.; Albanese, E.; Pot, A.M. Online Training and Support Programs Designed to Improve Mental Health and Reduce Burden Among Caregivers of People With Dementia: A Systematic Review. J. Am. Med. Dir. Assoc. 2018, 19, 200–206.e1. [Google Scholar] [CrossRef]
- Creese, A.; Parker, D. Cost Analysis in Primary Health Care. A Training Manual for Programme Managers; World Health Organisation: Geneva, Switzerland, 1994; pp. 55–72. [Google Scholar]
- Huo, Z.; Chan, J.Y.; Lin, J.; Bat, B.K.; Chan, T.K.; Tsoi, K.K.; Yip, B.H. Supporting informal caregivers of people with dementia in cost-effective ways: A systematic review and meta-analysis. Value Health 2021, 24, 1853–1862. [Google Scholar] [CrossRef] [PubMed]
- Shaw, C.A.; Williams, K.N.; Lee, R.H.; Coleman, C.K. Cost-effectiveness of a telehealth intervention for in-home dementia care support: Findings from the FamTechCare clinical trial. Res. Nurs. Health 2021, 44, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Park, T.; Brody, L.; Cruz, K.; Mukhi, P.; Reid, M.C.; Herr, K.; Pillemer, K.; Riffin, C. Recruitment of family caregivers of persons with dementia: Lessons learned from a pilot randomized controlled trial. Front. Pain Res. 2023, 4, 1125914. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Values |
|---|---|
| Age Mean (SD), years | 60 (12) |
| Female sex, n (%) | 32 (86) |
| Has a home care package, n (%) | 5 (14) |
| Highest level of education, n (%) | |
| Secondary school (Year 7–Year 11) | 13 (34) |
| Secondary school/TAFE/College | 15 (41) |
| Undergraduate tertiary education | 4 (10) |
| Postgraduate tertiary education | 5 (14) |
| Years in caring role, n (%) | |
| <2 | 13 (35) |
| 2–6 | 13 (35) |
| >6 | 11 (30) |
| Care recipient’s relationship to caregivers, n (%) | |
| Parent | 18 (48) |
| Spouse | 14 (38) |
| Sibling | 4 (10) |
| Friend | 1 (3) |
| Care recipient’s diagnosis, n (%) | |
| Dementia | 27 (72) |
| Cognitive impairment | 4 (10) |
| No formal diagnosis | 7 (18) |
| Care recipient’s years since diagnosis, n (%) | |
| <2 | 13 (34) |
| 2–4 | 5 (14) |
| >4 | 9 (24) |
| Caregiver’s location of residence, n (%) | |
| Lives with care recipient | 17 (45) |
| Same postcode as care recipient | 17 (45) |
| Lives 50–100 km from care recipient | 4 (10) |
| Survey Round 1 | Survey Round 2 | Survey Round 3 | Survey Round 4 | Survey Round 5 | |
|---|---|---|---|---|---|
| MOS-SSS | 43.2 (25.9) | 48.4 (26.4) | 54.0 (29.3) | 56.1 (29.5) | 54.1 (29.4) |
| ZBI | 51.4 (14.7) | 50.0 (15.3) | 46.9 (13.8) |
| No. of Logon Sessions (%) | No. of Visited Pages per Session | Average Session Duration, Seconds | |
|---|---|---|---|
| Desktop | 4664 (90.0) | 1.63 | 52 |
| Mobile | 357 (6.9) | 1.58 | 207 |
| Tablet | 163 (3.1) | 3.01 | 485 |
| Total | 5184 (100) | 1.67 | 67 |
| Cost Category | Average Cost | Share of Total Cost |
|---|---|---|
| Personnel time | $20,203 | 77% |
| Materials | $703 | 3% |
| Travel costs | $2846 | 11% |
| Other recurrent costs | $1282 | 5% |
| Recurrent costs | $25,035 | 92% |
| Equipment | $797 | 3% |
| Furniture | $14 | 0% |
| Vehicles | $193 | 1% |
| Buildings | $1022 | 4% |
| Capital costs | $2026 | 8% |
| Total costs | $27,061 | 100% |
| Start-up costs | $21,036 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blackberry, I.; Rasekaba, T.; Morgan, D.; Royals, K.; Greenhill, J.; Perkins, D.; O’Connell, M.; Hamiduzzaman, M.; Winbolt, M.; Robinson, A.; et al. Virtual Dementia-Friendly Communities (Verily Connect) Stepped-Wedge Cluster-Randomised Controlled Trial: Improving Dementia Caregiver Wellbeing in Rural Australia. Geriatrics 2023, 8, 85. https://doi.org/10.3390/geriatrics8050085
Blackberry I, Rasekaba T, Morgan D, Royals K, Greenhill J, Perkins D, O’Connell M, Hamiduzzaman M, Winbolt M, Robinson A, et al. Virtual Dementia-Friendly Communities (Verily Connect) Stepped-Wedge Cluster-Randomised Controlled Trial: Improving Dementia Caregiver Wellbeing in Rural Australia. Geriatrics. 2023; 8(5):85. https://doi.org/10.3390/geriatrics8050085
Chicago/Turabian StyleBlackberry, Irene, Tshepo Rasekaba, Debra Morgan, Kayla Royals, Jennene Greenhill, David Perkins, Megan O’Connell, Mohammad Hamiduzzaman, Margaret Winbolt, Ainsley Robinson, and et al. 2023. "Virtual Dementia-Friendly Communities (Verily Connect) Stepped-Wedge Cluster-Randomised Controlled Trial: Improving Dementia Caregiver Wellbeing in Rural Australia" Geriatrics 8, no. 5: 85. https://doi.org/10.3390/geriatrics8050085