

Functional Training and Dual-Task Training Improve the Executive Function of Older Women
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
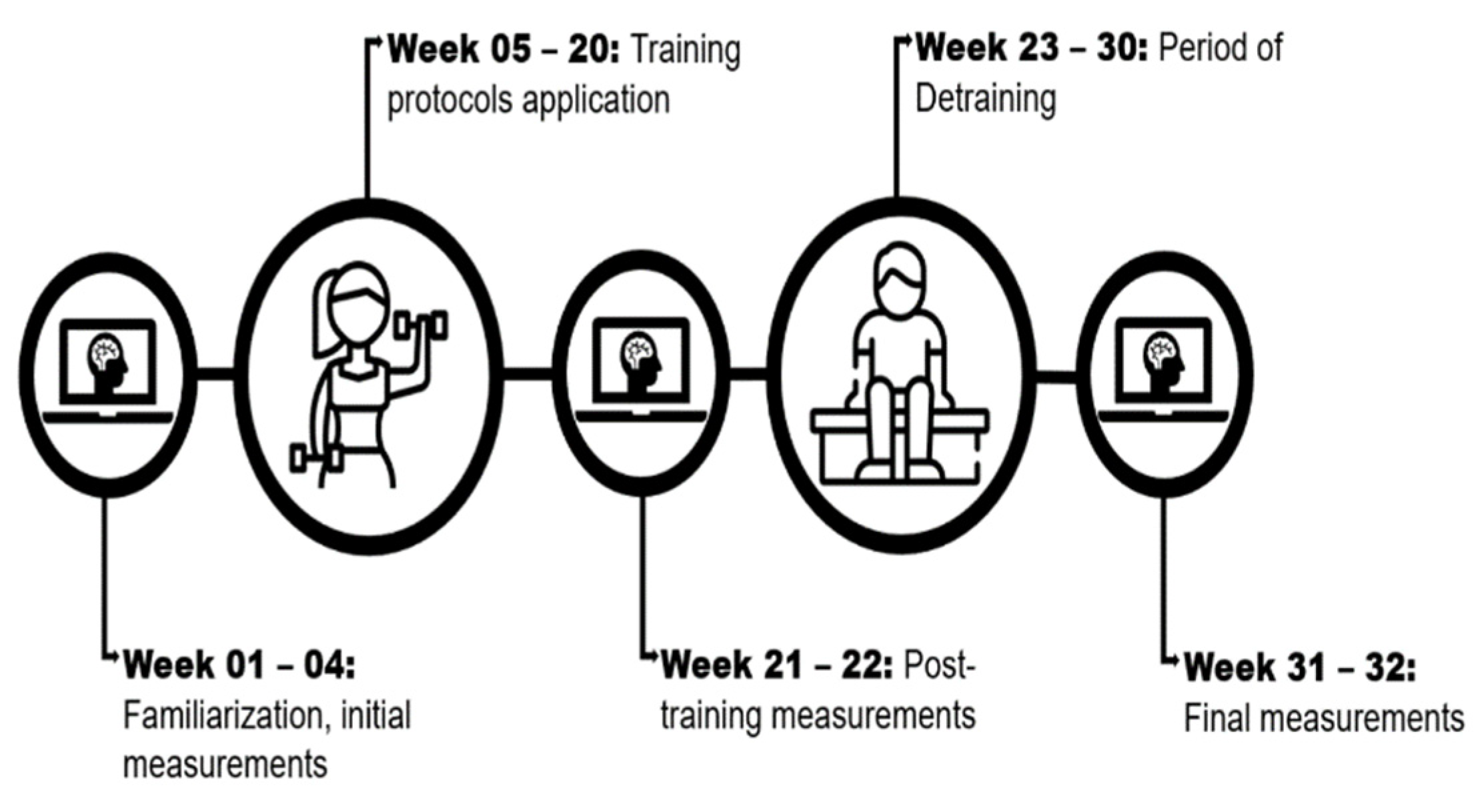
2.1. Study Design
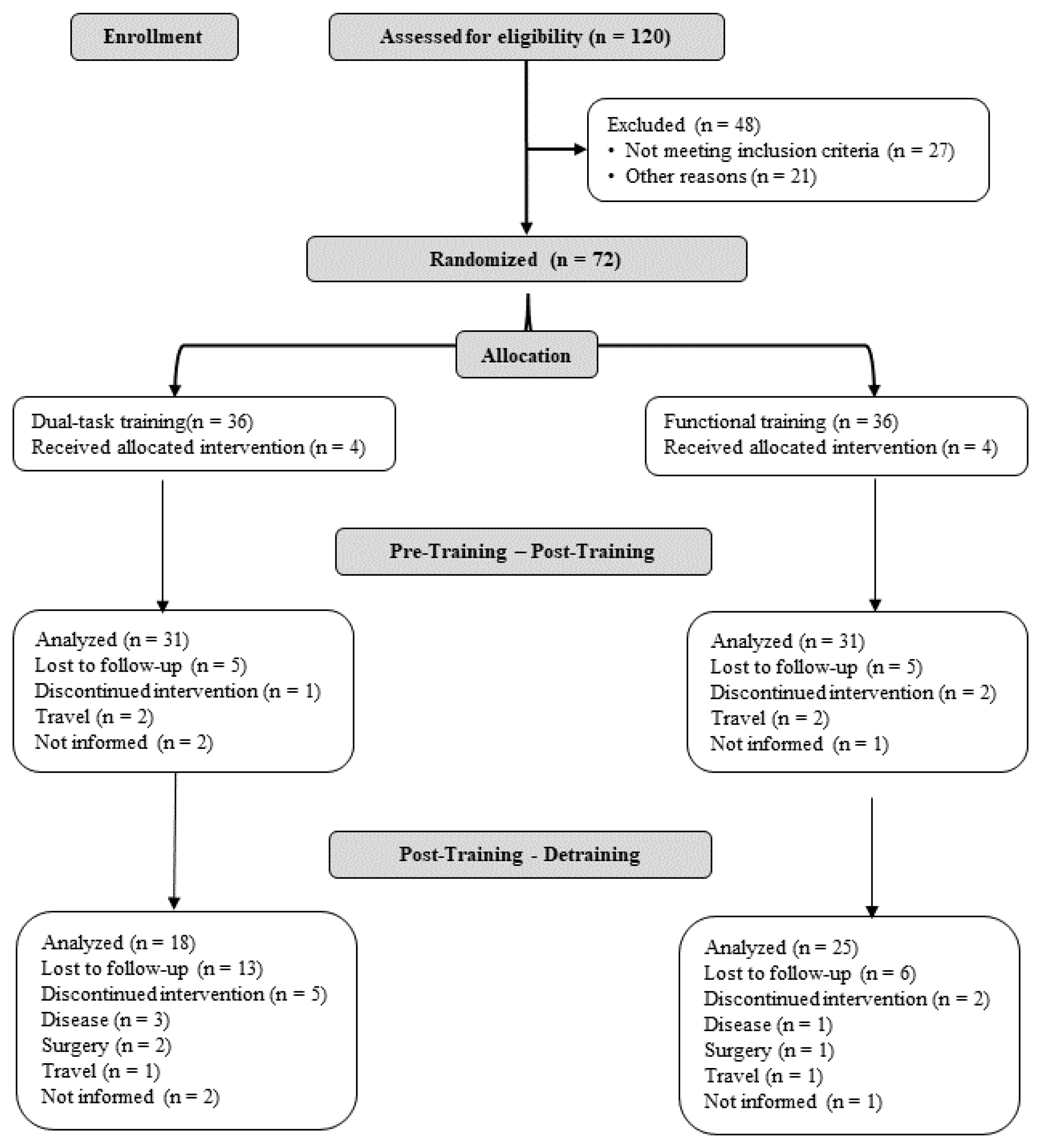
2.2. Participants
2.3. Intervention Procedures
2.4. Procedures
2.4.1. Anthropometric Characteristics
2.4.2. Executive Function
Inhibitory Control
Memory Working
Cognitive Flexibility
2.4.3. Sample Size
2.4.4. Statistical Analysis
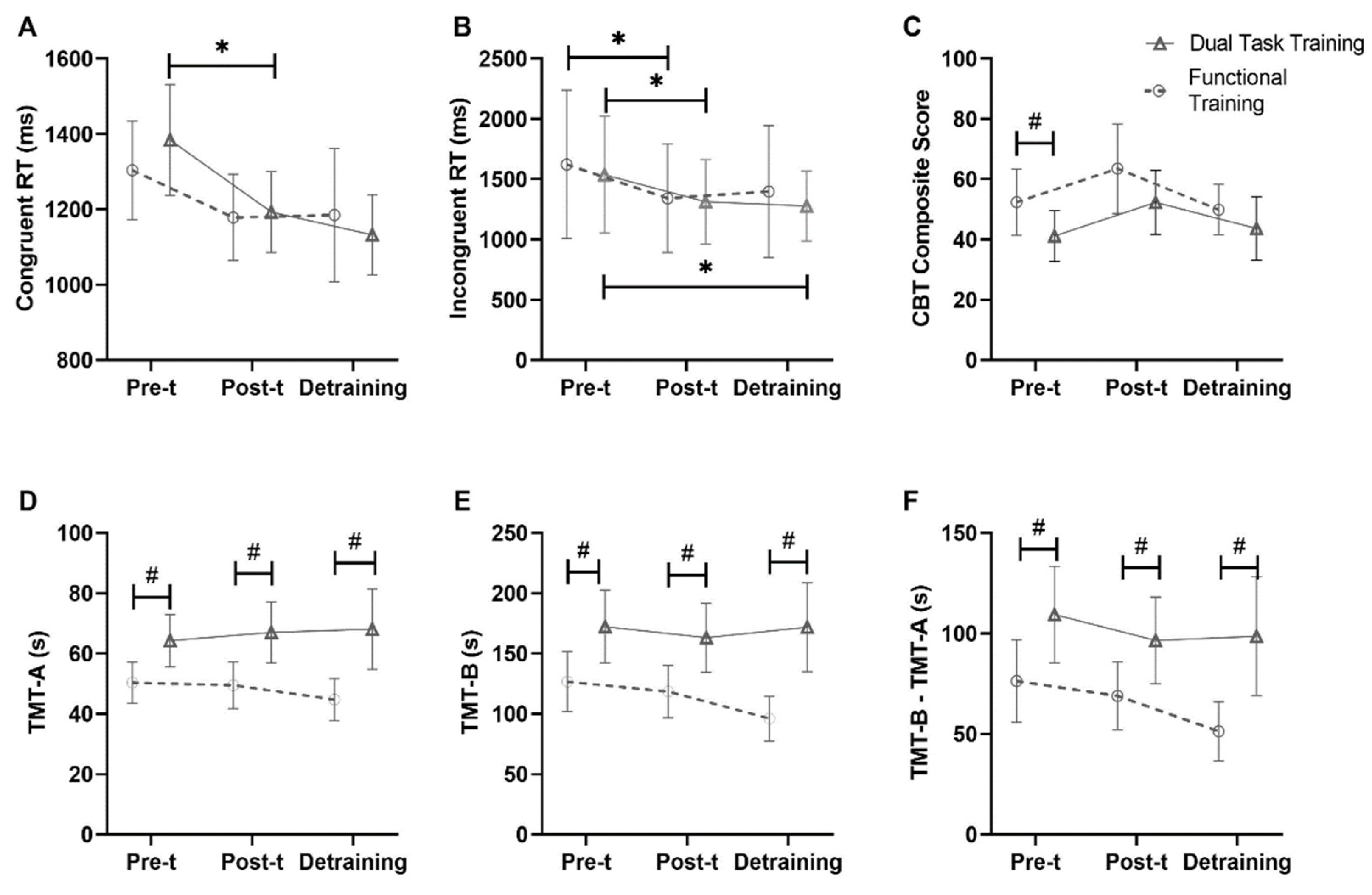
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed]
- Kang, W.; Wang, J.; Malvaso, A. Inhibitory Control in Aging: The Compensation-Related Utilization of Neural Circuits Hypothesis. Front. Aging Neurosci. 2022, 13, 771885. [Google Scholar] [CrossRef] [PubMed]
- Rabi, R.; Chow, R.; Paracha, S.; Hasher, L.; Gardner, S.; Anderson, N.D.; Alain, C. The Effects of Aging and Time of Dayon Inhibitory Control: An Event-Related Potential Study. Front. Aging Neurosci. 2022, 14, 821043. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A. Working Memory: Theories, Models, and Controversies. Annu. Rev. Psychol. 2012, 63, 1–29. [Google Scholar] [CrossRef]
- Sattari, N.; Whitehurst, L.N.; Ahmadi, M.; Mednick, S.C. Does Working Memory Improvement Benefit from Sleep in Older Adults? Neurobiol. Sleep Circadian Rhythm. 2019, 6, 53–61. [Google Scholar] [CrossRef]
- Borella, E.; Carretti, B.; Riboldi, F.; De Beni, R. Working Memory Training in Older Adults: Evidence of Transfer and Maintenance Effects. Psychol. Aging 2010, 25, 767–778. [Google Scholar] [CrossRef]
- Pieruccini-Faria, F.; Lord, S.R.; Toson, B.; Kemmler, W.; Schoene, D. Mental Flexibility Influences the Association Between Poor Balance and Falls in Older People—A Secondary Analysis. Front. Aging Neurosci. 2019, 11, 133. [Google Scholar] [CrossRef]
- Mahmoudpour, A.; Ferdousi Kejani, K.; Karami, M.; Toosi, M.; Ahmadboukani, S. Cognitive Flexibility and Emotional Self-regulation of the Elderly with Empty Nest Syndrome: Benefits of Acceptance and Commitment Therapy. Health Sci. Rep. 2023, 6, e1397. [Google Scholar] [CrossRef]
- Gabriel, K.P.; Mason, J.M.; Sternfeld, B. Recent Evidence Exploring the Associations between Physical Activity and Menopausal Symptoms in Midlife Women: Perceived Risks and Possible Health Benefits. Women’s Midlife Health 2015, 1, 1. [Google Scholar] [CrossRef]
- Barha, C.K.; Davis, J.C.; Falck, R.S.; Nagamatsu, L.S.; Liu-Ambrose, T. Sex Differences in Exercise Efficacy to Improve Cognition: A Systematic Review and Meta-Analysis of Randomized Controlled Trials in Older Humans. Front. Neuroendocrinol. 2017, 46, 71–85. [Google Scholar] [CrossRef]
- Ferguson, H.J.; Brunsdon, V.E.A.; Bradford, E.E.F. The Developmental Trajectories of Executive Function from Adolescence to Old Age. Sci. Rep. 2021, 11, 1382. [Google Scholar] [CrossRef] [PubMed]
- Genazzani, A.R.; Pluchino, N.; Luisi, S.; Luisi, M. Estrogen, Cognition and Female Ageing. Hum. Reprod. Update 2007, 13, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T. Consequences of Age-Related Cognitive Declines. Annu. Rev. Psychol. 2012, 63, 201–226. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.M.; Copeland, C.T.; Lowe, D.A.; Heyanka, D.J.; Linck, J.F. Contribution of Executive Functioning to Instrumental Activities of Daily Living in Older Adults. Appl. Neuropsychol. Adult 2020, 27, 326–333. [Google Scholar] [CrossRef]
- Davis, J.C.; Marra, C.A.; Najafzadeh, M.; Liu-Ambrose, T. The Independent Contribution of Executive Functions to Health Related Quality of Life in Older Women. BMC Geriatr. 2010, 10, 16. [Google Scholar] [CrossRef]
- Leckie, R.L.; Oberlin, L.E.; Voss, M.W.; Prakash, R.S.; Szabo-Reed, A.; Chaddock-Heyman, L.; Phillips, S.M.; Gothe, N.P.; Mailey, E.; Vieira-Potter, V.J.; et al. BDNF Mediates Improvements in Executive Function Following a 1-Year Exercise Intervention. Front. Hum. Neurosci. 2014, 8. [Google Scholar] [CrossRef]
- Chen, F.-T.; Etnier, J.L.; Chan, K.-H.; Chiu, P.-K.; Hung, T.-M.; Chang, Y.-K. Executive Functioning as a Predictor of Weight Loss and Physical Activity Outcomes. Sports Med. 2020, 50, 1451–1467. [Google Scholar] [CrossRef]
- Ghai, S.; Ghai, I.; Effenberg, A.O. Effects of Dual Tasks and Dual-Task Training on Postural Stability: A Systematic Review and Meta-Analysis. CIA 2017, 12, 557–577. [Google Scholar] [CrossRef]
- Marusic, U.; Verghese, J.; Mahoney, J.R. Cognitive-Based Interventions to Improve Mobility: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2018, 19, 484–491.e3. [Google Scholar] [CrossRef]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Navarro, I.; Cordellat, A.; Roldán, A.; Sanchis, G.; Blasco-lafarga, C.; Martinez-Navarro, I.; Cordellat, A.; Roldán, A.; Sanchis, G.; Blasco-lafarga, C. 120 Min / Week of Neuromotor Multicomponent Training Are Enough to Improve Executive Function and Functional Fitness in Older Women. Exp. Gerontol. 2021, 145, 111199. [Google Scholar] [CrossRef] [PubMed]
- Bouaziz, W.; Lang, P.O.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Vogel, T. Health Benefits of Multicomponent Training Programmes in Seniors: A Systematic Review. Int. J. Clin. Pract. 2016, 70, 520–536. [Google Scholar] [CrossRef] [PubMed]
- La Scala Teixeira, C.V.; Evangelista, A.L.; Pereira, P.E.d.A.; Da Silva-Grigoletto, M.E.; Bocalini, D.S.; Behm, D.G. Complexity: A Novel Load Progression Strategy in Strength Training. Front. Physiol. 2019, 10, 839. [Google Scholar] [CrossRef]
- Aragão-Santos, J.C.; de Resende-Neto, A.G.; Da Silva-Grigoletto, M.E. Different Types of Functional Training on the Functionality and Quality of Life in Postmenopausal Women: A Randomized and Controlled Trial. J. Sports Med. Phys. Fitness 2020, 60, 1283–1290. [Google Scholar] [CrossRef]
- Resende-Neto, A.G.; da Silva Resende, M.; Oliveira-Andrade, B.C.; da Silva Chaves, L.M.; Brandão, L.H.A.; Nogueira, A.C.; Mota, M.M.; DeSantana, J.M.; Da Silva-Grigoletto, M.E. Functional Training in Comparison to Traditional Training on Physical Fitness and Quality of Movement in Older Women. Sport Sci. Health 2021, 17, 213–222. [Google Scholar] [CrossRef]
- Al-Yahya, E.; Dawes, H.; Smith, L.; Dennis, A.; Howells, K.; Cockburn, J. Cognitive Motor Interference While Walking: A Systematic Review and Meta-Analysis. Neurosci. Biobehav. Rev. 2011, 35, 715–728. [Google Scholar] [CrossRef]
- Park, J.-H. Is Dual-Task Training Clinically Beneficial to Improve Balance and Executive Function in Community-Dwelling Older Adults with a History of Falls? Int. J. Environ. Res. Public Health 2022, 19, 10198. [Google Scholar] [CrossRef]
- Gavelin, H.M.; Dong, C.; Minkov, R.; Bahar-Fuchs, A.; Ellis, K.A.; Lautenschlager, N.T.; Mellow, M.L.; Wade, A.T.; Smith, A.E.; Finke, C.; et al. Combined Physical and Cognitive Training for Older Adults with and without Cognitive Impairment: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Ageing Res. Rev. 2020, 66, 101232. [Google Scholar] [CrossRef]
- Wu, Y.; Zang, M.; Wang, B.; Guo, W. Does the Combination of Exercise and Cognitive Training Improve Working Memory in Older Adults? A Systematic Review and Meta-Analysis. PeerJ 2023, 11, e15108. [Google Scholar] [CrossRef]
- Blasco-Lafarga, C.; Cordellat, A.; Forte, A.; Roldán, A.; Monteagudo, P. Short and Long-Term Trainability in Older Adults: Training and Detraining Following Two Years of Multicomponent Cognitive—Physical Exercise Training. Int. J. Environ. Res. Public Health 2020, 17, 5984. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. Int. J. Surg. 2011, 9, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Cesar, K.G.; Yassuda, M.S.; Porto, F.H.G.; Brucki, S.M.D.; Nitrini, R. MoCA Test: Normative and Diagnostic Accuracy Data for Seniors with Heterogeneous Educational Levels in Brazil. Arq. Neuro-Psiquiatr. 2019, 77, 775–781. [Google Scholar] [CrossRef]
- Scarpina, F.; Tagini, S. The Stroop Color and Word Test. Front. Psychol. 2017, 8, 557. [Google Scholar] [CrossRef] [PubMed]
- Stroop, J.R. Studies of Interference in Serial Verbal Reactions. J. Exp. Psychol. Gen. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Bailey, K.V.; Ferro-Luzzi, A. Use of Body Mass Index of Adults in Assessing Individual and Community Nutritional Status. Bull. World Health Organ. 1995, 73, 673–680. [Google Scholar]
- Vandierendonck, A.; Kemps, E.; Fastame, M.C.; Szmalec, A. Working Memory Components of the Corsi Blocks Task. Br. J. Psychol. 2004, 95, 57–79. [Google Scholar] [CrossRef]
- De Paula, J.J.; Malloy-Diniz, L.F.; Romano-Silva, M.A. Reliability of Working Memory Assessment in Neurocognitive Disorders: A Study of the Digit Span and Corsi Block-Tapping Tasks. Rev. Bras. De Psiquiatr. 2016, 38, 262–263. [Google Scholar] [CrossRef]
- Pantoja-Cardoso, A.; Aragão-Santos, J.C.; Pereira, M.R.M.; Santos, P.d.J.; Dos-Santos, A.C.; Faro, H.; Heredia-Elvar, J.R.; Fortes, L.d.S.; Silva-Grigoletto, M.E.D. Reproducibility of Inhibitory Control Measures, Working Memory and Cognitive Flexibility of Older Women. Rev. Bras. Fisiol. Exerc. 2023, 22, e225470. [Google Scholar] [CrossRef]
- Kessels, R.P.C.; van Zandvoort, M.J.E.; Postma, A.; Kappelle, L.J.; de Haan, E.H.F. The Corsi Block-Tapping Task: Standardization and Normative Data. Appl. Neuropsychol. 2000, 7, 252–258. [Google Scholar] [CrossRef]
- Reitan, R.M. The Relation of the Trail Making Test to Organic Brain Damage. J. Consult. Psychol. 1955, 19, 393–394. [Google Scholar] [CrossRef] [PubMed]
- Voos, M.C.; Custódio, E.B.; Malaquias, J. Relationship of Executive Function and Educational Status with Functional Balance in Older Adults. J. Geriatr. Phys. Ther. 2011, 34, 11–18. [Google Scholar] [PubMed]
- Erdfelder, E.; Faul, F.; Buchner, A. GPOWER: A General Power Analysis Program. Behav. Res. Methods Instrum. Comput. 1996, 28, 1–11. [Google Scholar] [CrossRef]
- Coetsee, C.; Terblanche, E. The Effect of Three Different Exercise Training Modalities on Cognitive and Physical Function in a Healthy Older Population. Eur. Rev. Aging Phys. Act. 2017, 14, 13. [Google Scholar] [CrossRef]
- The Jamovi Project. Jamovi Version 2.3.21 (Computer Software). 2022. Available online: https://www.jamovi.org (accessed on 30 June 2023).
- Cohen, J. Stafisfical Power Analysis for the Behavioural Sciences, 2nd ed.; Hillside, N.J., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Lakens, D. Calculating and Reporting Effect Sizes to Facilitate Cumulative Science: A Practical Primer for t-Tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef]
- Belleville, S.; Mellah, S.; de Boysson, C.; Demonet, J.-F.; Bier, B. The Pattern and Loci of Training-Induced Brain Changes in Healthy Older Adults Are Predicted by the Nature of the Intervention. PLoS ONE 2014, 9, e102710. [Google Scholar] [CrossRef]
- Pesce, C. Shifting the Focus from Quantitative to Qualitative Exercise Characteristics in Exercise and Cognition Research. J. Sport Exerc. Psychol. 2012, 34, 766–786. [Google Scholar] [CrossRef]
- Chainay, H.; Joubert, C.; Massol, S. Behavioural and ERP Effects of Cognitive and Combined Cognitive and Physical Training on Working Wemory and Executive Function in Healthy Older Adults. ACP 2021, 17, 58–69. [Google Scholar] [CrossRef]
- Jardim, N.Y.V.; Bento-Torres, N.V.O.; Costa, V.O.; Carvalho, J.P.R.; Pontes, H.T.S.; Tomás, A.M.; Sosthenes, M.C.K.; Erickson, K.I.; Bento-Torres, J.; Diniz, C.W.P. Dual-Task Exercise to Improve Cognition and Functional Capacity of Healthy Older Adults. Front. Aging Neurosci. 2021, 13, 589299. [Google Scholar] [CrossRef]
- Guo, W.; Wang, B.; Lu, Y.; Zhu, Q.; Shi, Z.; Ren, J. The Relationship between Different Exercise Modes and Visuospatial Working Memory in Older Adults: A Cross-Sectional Study. PeerJ 2016, 4, e2254. [Google Scholar] [CrossRef]
- Brown, A.K.; Liu-Ambrose, T.; Tate, R.; Lord, S.R. The Effect of Group-Based Exercise on Cognitive Performance and Mood in Seniors Residing in Intermediate Care and Self-Care Retirement Facilities: A Randomised Controlled Trial. Br. J. Sports Med. 2009, 43, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Mekari, S.; Neyedli, H.F.; Fraser, S.; O’Brien, M.W.; Martins, R.; Evans, K.; Earle, M.; Aucoin, R.; Chiekwe, J.; Hollohan, Q.; et al. High-Intensity Interval Training Improves Cognitive Flexibility in Older Adults. Brain Sci. 2020, 10, 796. [Google Scholar] [CrossRef] [PubMed]
- Forte, R.; Boreham, C.A.; Leite, C.; De Vito, G.; Brennan, L.; Gibney, E.R.; Pesce, C. Enhancing Cognitive Functioning in the Elderly: Multicomponent vs Resistance Training. CIA 2013, 8, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Aragão-Santos, J.C.; De Resende-Neto, A.G.; Nogueira, A.C.; Feitosa-Neta, M.d.L.; Brandão, L.H.; Chaves, L.M.; Da Silva-Grigoletto, M.E. The Effects of Functional and Traditional Strength Training on Different Strength Parameters of Elderly Women: A Randomized and Controlled Trial. J. Sports Med. Phys. Fit. 2019, 59, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Resende-Neto, A.G.d.R.; Santos, M.S.; Silva, R.J.S.; de Santana, J.M.; da Silva-Grigoletto, M.E. Effects of Different Neuromuscular Training Protocols on the Functional Capacity of Elderly Women. Rev. Bras. De Med. Do Esporte 2018, 24, 140–144. [Google Scholar] [CrossRef]
- Brustio, P.R.; Rabaglietti, E.; Formica, S.; Liubicich, M.E. Dual-Task Training in Older Adults: The Effect of Additional Motor Tasks on Mobility Performance. Arch. Gerontol. Geriatr. 2018, 75, 119–124. [Google Scholar] [CrossRef]
- Weinstein, A.M.; Voss, M.W.; Prakash, R.S.; Chaddock, L.; Szabo, A.; White, S.M.; Wojcicki, T.R.; Mailey, E.; McAuley, E.; Kramer, A.F.; et al. The Association between Aerobic Fitness and Executive Function Is Mediated by Prefrontal Cortex Volume. Brain Behav. Immun. 2012, 26, 811–819. [Google Scholar] [CrossRef] [PubMed]
- Predovan, D.; Berryman, N.; Lussier, M.; Comte, F.; Vu, T.T.M.; Villalpando, J.M.; Bherer, L. Assessment of the Relationship Between Executive Function and Cardiorespiratory Fitness in Healthy Older Adults. Front. Psychol. 2021, 12, 742184. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 1st Part | 2nd Part | 3rd Part | 4th Part | 5th Part | |
|---|---|---|---|---|---|
| FT | Frontal run skipping in a walking pattern | Latter agility | Deadlift | Relay | Single stretching + breathing |
| Battle rope | Goblet squat | ||||
| High-knee skips | Med ball throw | Farmer’s walk | |||
| Climbing on and off the step | Rowing | ||||
| Agility between cones | Pushing | ||||
| DTT | Standing Stretch Patterns + Mobility and Stability + Evocation | Bipodal balance with feet together, one glued to the other + Balancing a ball, throwing from one hand to the other in front | Stationary march + Progression of steps from 2 to 2 and from 3 to 3 according to the command | Pass the ball to the side (calling for colors) in an isometric squat position, counting the number of turns | Single stretching + breathing |
| Unipodal balance with assisting stick, in pairs, evoking the name of a class without repeating what has already been said | Lateral displacement with side shift | ||||
| Straight line walking with feet on edge of center strip balancing baton |
| DTT (n = 31) | FT (n = 31) | Total (n = 62) | |||||
|---|---|---|---|---|---|---|---|
| Variables | Mean ± SD | CI 95% | Mean ± SD | CI 95% | Mean ± SD | CI 95% | p-Value |
| Age (years) | 67 ± 5 | 65–69 | 66 ± 5 | 64–68 | 66 ± 5 | 65–68 | 0.405 |
| Body Mass (kg) | 66.3 ± 11.2 | 62.1–70.4 | 65.4 ± 8.9 | 62.1–68.7 | 65.8 ± 10.1 | 63.3–68.4 | 0.745 |
| Height (m) | 1.53 ± 0.05 | 1.51–1.55 | 1.55 ± 0.05 | 1.53–1.57 | 1.54 ± 0.05 | 1.53–1.54 | 0.112 |
| BMI (kg/m2) | 28.3 ± 4.3 | 26.7–29.9 | 27.1 ± 3.5 | 25.8–28.4 | 27.7 ± 3.9 | 26.7–28.7 | 0.25 |
| MoCA (score) | 21.0 ± 4.3 | 19.4–22.6 | 22.3 ± 3.7 | 20.9–23.7 | 21.6 ± 4.1 | 20.6–22.7 | 0.208 |
| Education (relative and absolute frequency) | |||||||
| Incomplete Elementary | 22.6 (14) | 14.5 (9) | 37.1 (23) | 0.694 | |||
| Complete Elementary | 3.2 (2) | 3.2 (2) | 6.5 (4) | ||||
| Incomplete High School | 1.6 (1) | 1.6 (1) | 3.2 (2) | ||||
| Complete High School | 19.4 (12) | 22.6 (14) | 41.9 (26) | ||||
| Incomplete Undergraduete degree | 1.6 (1) | 1.6 (1) | 3.2 (2) | ||||
| Complete Undergraduete degree | 1.6 (1) | 6.4 (4) | 8.5 (5) | ||||
| Medical History (relative and absolute frequency) | |||||||
| Hypertension | 59.5 (22) | 40.5 (15) | 59.7 (37) | 0.07 | |||
| Depression | 80.0 (4) | 20.0 (1) | 8.1 (5) | 0.162 | |||
| Diabetes | 60.0 (9) | 40.0 (6) | 24.2 (15) | 0.374 | |||
| Body pain | 51.2 (22) | 48.8 (21) | 70.5 (43) | 0.632 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pantoja-Cardoso, A.; Aragão-Santos, J.C.; Santos, P.d.J.; Dos-Santos, A.C.; Silva, S.R.; Lima, N.B.C.; Vasconcelos, A.B.S.; Fortes, L.d.S.; Da Silva-Grigoletto, M.E. Functional Training and Dual-Task Training Improve the Executive Function of Older Women. Geriatrics 2023, 8, 83. https://doi.org/10.3390/geriatrics8050083
Pantoja-Cardoso A, Aragão-Santos JC, Santos PdJ, Dos-Santos AC, Silva SR, Lima NBC, Vasconcelos ABS, Fortes LdS, Da Silva-Grigoletto ME. Functional Training and Dual-Task Training Improve the Executive Function of Older Women. Geriatrics. 2023; 8(5):83. https://doi.org/10.3390/geriatrics8050083
Chicago/Turabian StylePantoja-Cardoso, Alan, Jose Carlos Aragão-Santos, Poliana de Jesus Santos, Ana Carolina Dos-Santos, Salviano Resende Silva, Newton Benites Carvalho Lima, Alan Bruno Silva Vasconcelos, Leonardo de Sousa Fortes, and Marzo Edir Da Silva-Grigoletto. 2023. "Functional Training and Dual-Task Training Improve the Executive Function of Older Women" Geriatrics 8, no. 5: 83. https://doi.org/10.3390/geriatrics8050083