
An Exploratory Study of Nutrition Knowledge and Challenges Faced by Informal Carers of Community-Dwelling People with Dementia: Online Survey and Thematic Analysis


Abstract
:1. Introduction
- What is the nutrition knowledge of informal carers of people with dementia?
- What are common nutrition-related issues faced by informal carers of people with dementia?
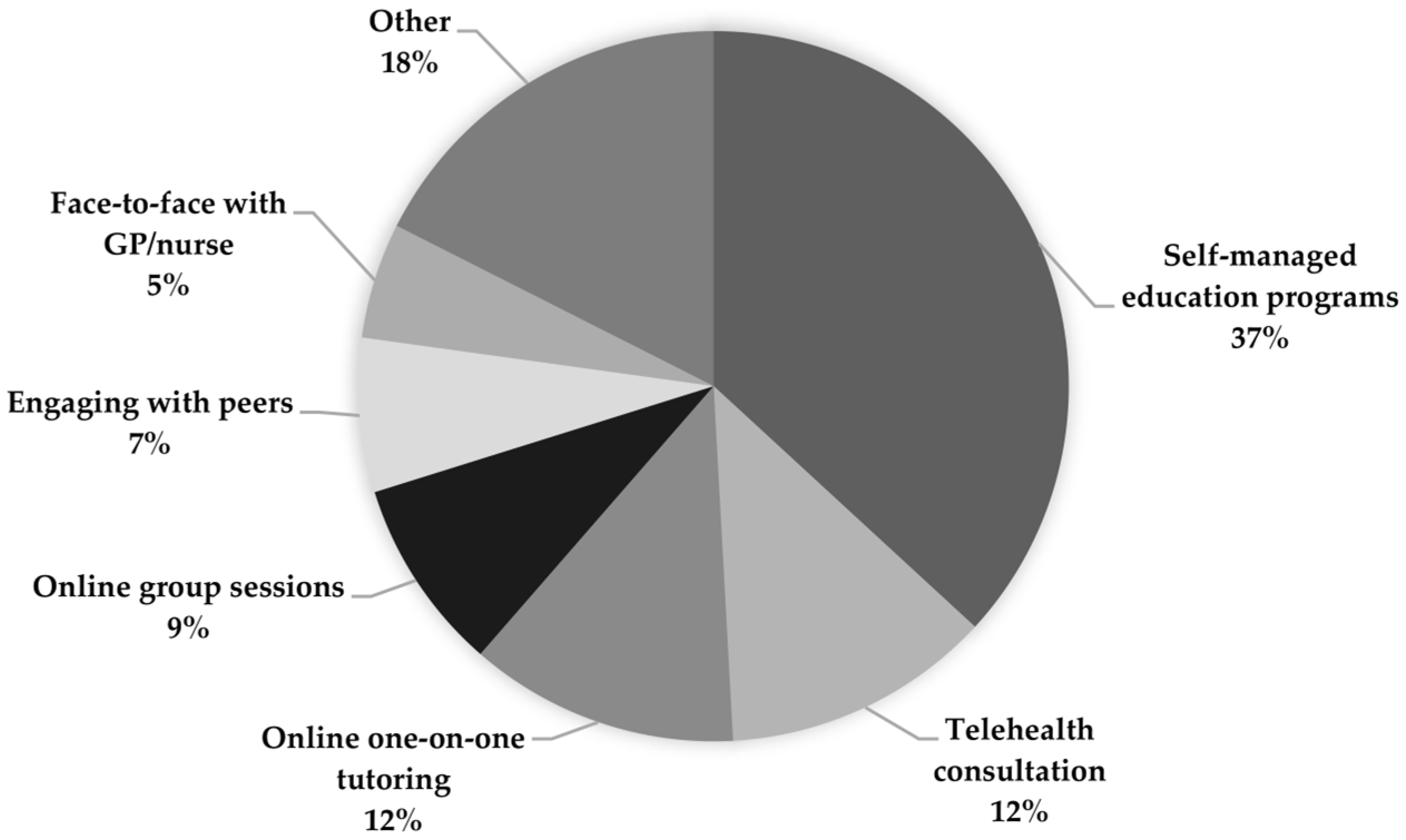
- What are the preferred modes of delivery of nutrition education for informal carers of people with dementia?
2. Materials and Methods
2.1. Study Design
2.2. Participant Selection
2.3. Data Collection
2.3.1. Quantitative Data
- (1)
- Sociodemographic information.
- (2)
- Nutrition knowledge was assessed using the revised General Nutrition Knowledge Questionnaire for Australia (AUS-R-NKQ). The AUS-R-NKQ was redesigned and validated in 2020 after advances in understanding the diet–disease relationship and changes in nutrition recommendations [25]. The General Nutrition Knowledge Questionnaire (GNKQ) is validated internationally and in Australia [26,27,28]. The thirty-eight-item questionnaire consists of four categories:
- Dietary recommendations: Eleven questions focussed on the Australian Dietary Guidelines.
- Nutrients in foods: Nine questions relating to the different food groups (meats, vegetables, fruits, grains, and dairy products) and the nutrients they contain (carbohydrates, proteins, fats, fibre, minerals, and vitamins).
- Food choices: Nine questions assessing knowledge of healthy food choices.
- Diet–disease relationships: Nine questions about the interaction between diet and nutrition, and common health problems and diseases.
- (3)
- Nutritional care and provision and nutrition-related issues in people with dementia.
- (4)
- Preferred delivery modes of nutrition education programmes for informal carers.
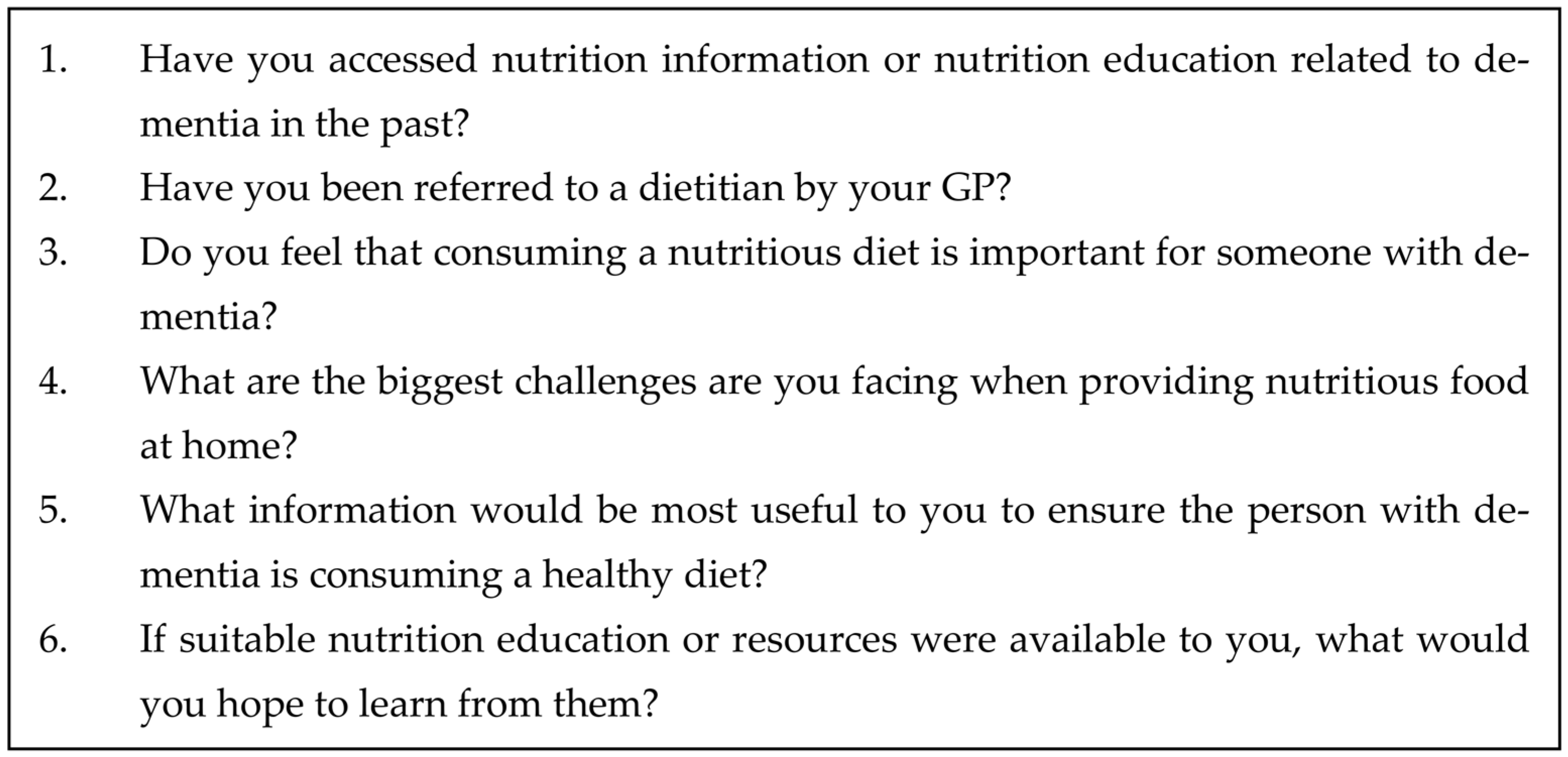
2.3.2. Qualitative Data
2.4. Data Analysis
3. Results
3.1. Interviewed Participants
3.2. Thematic Analysis
3.2.1. Theme 1: Providing a Healthy Diet Is Challenging for Carers
“I think his communication and ability to say what he wants and what he needs, might diminish, which means that you, you really have to kind of be looking after the food side of things and encouraging and, you know, presenting good options, rather than just waiting for them to choose something.”(P10)
Sub-Theme 1: Physiological Changes Make it Difficult to Provide a Healthy Diet
“You, you’ve got no weight gain and loss of appetite and pressure on your gut and all that sort of stuff. So, all of those things compound to make the fact that eating probably isn’t much fun.”(P1)
“He’s not tasting anything and getting the salt pot and just chucking it on the plate. So, I don’t cook with salt, or barely because I know he’s not going to taste it and chuck the salt on top of it.”(P2)
Sub-Theme 2: Memory Loss Contributes to Lower Energy Intake
“Sometimes, he forgets to eat when he is on his own. Sometimes I cook things he likes, something that when he was young, in his younger years, like homemade pie. He likes that because that reminds him of his young days of his childhood.”(P6)
“Or she doesn’t drink enough water we have to push her to drink water. She’s forgotten a little bit. Sometimes she forgets how to swallow.”(P5)
Sub-Theme 3: Financial Barriers to Healthy Nutrition
“I mean, there have been, you know, difficulties as you know, last few years with, you know, floods and COVID and that kind of thing, trying to access fruit and veg that, you know, isn’t too expensive.”(P9)
Sub-Theme 4: The Provision of a Healthy Diet Accentuates Carer Burden
“I think it’s the carers that need to be supported so they can continue doing what they’re doing. It’s tiring. People should be giving me information and helping me with what I need. I’m helping my dad; I’m helping my family—rather than me having to look out for everything. Plus trying to work full time. It’s hard.”(P5)
“Realistically, there are so many battles to be had with this condition and there’s so many things I have to think about every day. Just basic things, and it’s just one more thing to have to think about [nutrition]. […] If somebody would tell me that there was a HelloFresh [meal delivery service] for dementia, like a special diet that I could pay for, I would pay any money for that.”(P8)
“Making things up at times gets a little bit difficult, putting the time in. We had over 50 medical appointments last year. I was too tired last night to get any dinner last night, so we bought a hamburger and we had that with, I’d cooked corn on the cob.”(P9)
“I make all of her evening meals and I make things I know that she likes, and I bulk make them and I freeze them in very small serves. So, it’s hard for me when I make the food, I know it’s good food and I’ve put protein in it and stuff, but she won’t eat it.”(P7)
3.2.2. Theme 2: The Importance of a Healthy Diet
“It is important, yes because I think the brain will function better if the person eats healthy food. Like more broccoli, cauliflower, more spinach, green vegetables, lots of water. Yeah, and more nuts. So, I think the brain will function better if it’s healthy food rather than just pizza or pasta or canned food, for example.”(P6)
Sub-Theme 1: Adapting to the Person and Being Creative Are Essential
“You know, I think enjoyment is really one of the one of the few things that that we can get out of life, and this was making, maybe be as big a message as enjoying food. And you know, it’s important to keep that going, and to make sure that while technically, you know, a healthy diet is being provided. It also needs to be really tasty, and to make people want to eat rather than you know, getting through mechanically like you need fuel.”(P10)
Sub-Theme 2: Carers Aim to Provide a Healthy Dietary Pattern
“I’ve been very, very keen to follow up research on topics such as intermittent fasting, you know, low carb, low salt diets, etc. [They’ve] come from a variety of sources, many of them online, but usually from reliable sources, fully qualified people who have done research and are open about what works and what doesn’t. The Mediterranean diet seems to be the winner at the moment, and I think that would go for the general population, but also for people who have dementia. [..] I think you need to eat well [and] cut out as many processed foods as possible.”(P10)
Sub-Theme 3: Involving the Person with Dementia and Social Eating Can Improve Nutrition
“Well, we couldn’t use the table at the same time. And so, I found that [if] [person with dementia] was sitting watching TV, […], we had to stop that quickly, because that isolates him. Yeah, so we sit, and we talk, and he always says ‘oh, this is a great meal’. I mean he doesn’t always know where his meals come from. But presented nicely, you know, he’s happy and eats it all.”(P11)
“I think the social contact helps him a lot. He likes when someone is with him to eat together. Yeah, and it helps him a lot when we cook when I pass things. So, I allow him, I allow him sometimes to cook or let’s cook together! Yeah, that helps a lot, when the social connection and interaction, when we cook together.”(P6)
“There’s one meal he makes which is pasta, because we keep [chickens], we can make, we make fresh pasta with our own eggs. But with some assistance, he can still do that. So, he gets a huge sense of achievement from doing that.”(P4)
Sub-Theme 4: The Association between Diet, Lack of Exercise, and Sedentary Behaviour
“[T]hey don’t do much exercise, you know, if you don’t move, you’re not going to develop an appetite.”(P1)
“His physical condition [heart issues] doesn’t let him to be active. So, I think that’s why he’s lost weight”(P11)
“He’s more sedentary these days, so he’s not as active. So, there’s a tendency to overeat.”(P4)
3.2.3. Theme 3: Carers Seek Accessible and Clear Information on Nutrition
“I have done the University of Tasmania UD-MOOC online for dementia. So, I understand that one of the risk factors can be diet. I’m aware of a healthy diet being beneficial to anybody during their life.”(P7)
“I’m right behind her that I guarantee you this will be me and in 20 or 30 years. I know that I need to be thinking about my own brain health.”(P7)
“If you search on the internet for information about healthy eating, there is a plethora of information, often inconsistent and even contradictory. It isn’t easy for people to decide which sources of information to rely on.”(P4)
“I don’t think enough information is given to people from the doctors. […] I think that even if the doctors had a handout. That’s easy for a doctor to hand out and give to the person and say: Do you understand this? If you’ve got any problems…?”(P11)
“A factsheet or something, that would help. These are the foods to eat, these are the foods to avoid, these really help, these don’t help.”(P5)
“I’d hope to learn what science has, not just one study, you know, really solid peer base review research as to what’s coming out as the best way or is there [a] definite solid link with some foods perhaps to avoid and other foods to gravitate towards to have more.”(P7)
“I’d like to learn, I guess, information that reinforces what you know, and is up to date, I mean, things that [are] changing, information and ideas, and guidelines change over time.”(P1)
3.2.4. Theme 4: Inadequate Support from Healthcare Professionals
“GP never talked about nutrition. Never. So, I also don’t think it’s her area of interest or expertise.”(P3)
“If I can be really honest, I don’t think they understand dementia themselves [GPs], and I don’t think they care.”(P5)
“We have changed doctors, […] we weren’t very satisfied with how much help we were getting. But we were desperate for any advice and education, and he kind of went ‘ah you know, you can go online there, you know, you can Google’ which didn’t really help us. But he’s never focused very much on diet beyond general health, or weight loss, and suggesting dieting for weight loss, but has never really provided any advice around her cognitive decline.”(P8)
“It’s all about the other services that the GPs need to know about. And we’re saying it all the time. Their knowledge isn’t enough, so what we need is like dementia-trained nurses in a practice or something like that, and they would be the ones that would feed all this information regarding nutrition.”(P11)
“I mean, I think you know, in a 15-min discussion, there’s often lots of other things going on. And I think they just probably don’t even think about it. Diabetics, yeah, and other things, probably not.”(P1)
Sub-Theme 1: GPs Do Not Offer Referral to a Dietitian
“I know that when I’ve worked, I’ve worked in aged care. So, we have used dietitians in aged care for people with problems, they should be used for everybody, not just for people with problems.”(P11)
“I think it would be a good idea! I don’t think the importance of diet relating to dementia is widely known, and I would be interested in seeing a nutritionist or a dietitian in respect [to] my partner, yes. But he hasn’t done that.”(P4)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Duong, S.; Patel, T.; Chang, F. Dementia: What pharmacists need to know. Can. Pharm. J. 2017, 150, 118–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Institute of Health. Dementia in Australia; AIHW: Canberra, Australia, 2022. [Google Scholar]
- Pathak, K.; Mattos, E. Dementia and Nutrition; Intech Open: London, UK, 2021. [Google Scholar] [CrossRef]
- Perneczky, R. Dementia treatment versus prevention. Dialogues Clin. Neurosci. 2019, 21, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Ydstebø, A.E.; Benth, J.; Bergh, S.; Selbæk, G.; Vossius, C. Informal and formal care among persons with dementia immediately before nursing home admission. BMC Geriatr. 2020, 20, 296. [Google Scholar] [CrossRef]
- Lindeza, P.; Rodrigues, M.; Costa, J.; Guerreiro, M.; Rosa, M.M. Impact of dementia on informal care: A systematic review of family caregivers’ perceptions. BMJ Support. Palliat. Care 2020. [Google Scholar] [CrossRef] [PubMed]
- Wimo, W.; Gauthier, S.; Prince, M. Global Estimates of Informal Care; Alzheimer’s Disease International: London, UK, 2018. [Google Scholar]
- Brodaty, H.; Donkin, M. Family caregivers of people with dementia. Dialogues Clin. Neurosci. 2009, 11, 217–228. [Google Scholar] [CrossRef]
- DiZazzo-Miller, R.; Samuel, P.S.; Barnas, J.M.; Welker, K.M. Addressing everyday challenges: Feasibility of a family caregiver training program for people with dementia. Am. J. Occup. Ther. 2014, 68, 212–220. [Google Scholar] [CrossRef] [Green Version]
- Fostinelli, S.; De Amicis, R.; Leone, A.; Giustizieri, V.; Binetti, G.; Bertoli, S.; Battezzati, A.; Cappa, S.F. Eating Behavior in Aging and Dementia: The Need for a Comprehensive Assessment. Front. Nutr. 2020, 7, 604488. [Google Scholar] [CrossRef]
- Holm, B.; Söderhamn, O. Factors associated with nutritional status in a group of people in an early stage of dementia. Clin. Nutr. 2003, 22, 385–389. [Google Scholar] [CrossRef]
- Ball, L.; Jansen, S.; Desbrow, B.; Morgan, K.; Moyle, W.; Hughes, R. Experiences and nutrition support strategies in dementia care: Lessons from family carers. Nutr. Diet. 2015, 72, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Tucker, K.L. Nutrient intake, nutritional status, and cognitive function with aging. Ann. N. Y. Acad. Sci. 2016, 1367, 38–49. [Google Scholar] [CrossRef] [Green Version]
- Mole, L.; Kent, B.; Abbott, R.; Hickson, M. Family carers’ experiences of nutritional care for people living with dementia at home: An interpretative phenomenological analysis. Dementia 2021, 20, 231–246. [Google Scholar] [CrossRef] [Green Version]
- Sanders, C.; Behrens, S.; Schwartz, S.; Wengreen, H.; Corcoran, C.D.; Lyketsos, C.G.; Tschanz, J.T. Nutritional Status is Associated with Faster Cognitive Decline and Worse Functional Impairment in the Progression of Dementia: The Cache County Dementia Progression Study1. J. Alzheimers Dis. 2016, 52, 33–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, S.S. Strategies for home nutritional support in dementia care and its relevance in low-middle-income countries. J. Fam. Med. Prim. Care 2020, 9, 43–48. [Google Scholar] [CrossRef]
- Soto, M.E.; Secher, M.; Gillette-Guyonnet, S.; van Kan, G.A.; Andrieu, S.; Nourhashemi, F.; Rolland, Y.; Vellas, B. Weight Loss and Rapid Cognitive Decline in Community-Dwelling Patients with Alzheimer’s Disease. J. Alzheimer’s Dis. 2012, 28, 647–654. [Google Scholar] [CrossRef]
- Kigozi, E.; Egwela, C.; Kamoga, L.; Nalugo Mbalinda, S.; Kaddumukasa, M. Nutrition Challenges of Patients with Alzheimer’s Disease and Related Dementias: A Qualitative Study from the Perspective of Caretakers in a Mental National Referral Hospital. Neuropsychiatr. Dis. Treat. 2021, 17, 2473–2480. [Google Scholar] [CrossRef] [PubMed]
- Mole, L.; Kent, B.; Abbott, R.; Wood, C.; Hickson, M. The nutritional care of people living with dementia at home: A scoping review. Health Soc. Care Community 2018, 26, e485–e496. [Google Scholar] [CrossRef] [Green Version]
- Johansson, M.F.; McKee, K.J.; Dahlberg, L.; Williams, C.L.; Summer Meranius, M.; Hanson, E.; Magnusson, L.; Ekman, B.; Marmstål Hammar, L. A comparison of spouse and non-spouse carers of people with dementia: A descriptive analysis of Swedish national survey data. BMC Geriatr. 2021, 21, 338. [Google Scholar] [CrossRef]
- Anantapong, K.; Sampson, E.L.; Davies, N. A shared decision-making model about care for people with severe dementia: A qualitative study based on nutrition and hydration decisions in acute hospitals. Int. J. Geriatr. Psychiatry 2023, 38, e5884. [Google Scholar] [CrossRef]
- Silver, H.J.; Wellman, N.S. Nutrition Education May Reduce Burden in Family Caregivers of Older Adults. J. Nutr. Educ. Behav. 2002, 34, S53–S58. [Google Scholar] [CrossRef]
- Li, Y.; Sun, D.; Zhang, X.; Li, H.; Zhao, Y.; Ma, D.; Li, Z.; Sun, J. Informal dementia caregivers’ experiences and perceptions about mealtime care: A qualitative evidence synthesis. J. Adv. Nurs. 2020, 76, 3317–3328. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J. Research Design: Qualitative, Quantitative, and Mixed-Method Approaches; Sage: London, UK, 2009. [Google Scholar]
- Thompson, C.; Vidgen, H.A.; Gallegos, D.; Hannan-Jones, M. Validation of a revised General Nutrition Knowledge Questionnaire for Australia. Public. Health Nutr. 2021, 24, 1608–1618. [Google Scholar] [CrossRef]
- Hendrie, G.A.; Coveney, J.; Cox, D. Exploring nutrition knowledge and the demographic variation in knowledge levels in an Australian community sample. Public. Health Nutr. 2008, 11, 1365–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendrie, G.A.; Cox, D.; Coveney, J. Validation of the General Nutrition Knowledge Questionnaire in an Australian Community Sample. Nutr. Diet. 2008, 65, 72–77. [Google Scholar] [CrossRef]
- Kliemann, N.; Wardle, J.; Johnson, F.; Croker, H. Reliability and validity of a revised version of the General Nutrition Knowledge Questionnaire. Eur. J. Clin. Nutr. 2016, 70, 1174–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrado-Martín, Y.; Nair, P.; Anantapong, K.; Aker, N.; Moore, K.J.; Smith, C.H.; Rait, G.; Sampson, E.L.; Manthorpe, J.; Davies, N. Family caregivers’ and professionals’ experiences of supporting people living with dementia’s nutrition and hydration needs towards the end of life. Health Soc. Care Community 2022, 30, 307–318. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual. Res. Psychol. 2021, 18, 328–352. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. Adm. Policy Ment. Health Ment. Health Serv. Res. 2015, 42, 533–544. [Google Scholar] [CrossRef] [Green Version]
- Scalvedi, M.L.; Gennaro, L.; Saba, A.; Rossi, L. Relationship Between Nutrition Knowledge and Dietary Intake: An Assessment Among a Sample of Italian Adults. Front. Nutr. 2021, 8, 714493. [Google Scholar] [CrossRef] [PubMed]
- Kullen, C.J.; Farrugia, J.-L.; Prvan, T.; O’Connor, H.T. Relationship between general nutrition knowledge and diet quality in Australian military personnel. Br. J. Nutr. 2016, 115, 1489–1497. [Google Scholar] [CrossRef] [Green Version]
- Goodman, S.; Armendariz, G.C.; Corkum, A.; Arellano, L.; Jáuregui, A.; Keeble, M.; Marshall, J.; Sacks, G.; Thrasher, J.F.; Vanderlee, L.; et al. Recall of government healthy eating campaigns by consumers in five countries. Public. Health Nutr. 2021, 24, 3986–4000. [Google Scholar] [CrossRef]
- Spendlove, J.K.; Heaney, S.E.; Gifford, J.A.; Prvan, T.; Denyer, G.S.; O’Connor, H.T. Evaluation of general nutrition knowledge in elite Australian athletes. Br. J. Nutr. 2012, 107, 1871–1880. [Google Scholar] [CrossRef] [Green Version]
- Hamzaid, N.H.; Flood, V.M.; Prvan, T.; O’Connor, H.T. General nutrition knowledge among carers at group homes for people with intellectual disability. J. Intellect. Disabil. Res. 2018, 62, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Anantapong, K.; Davies, N.; Chan, J.; McInnerney, D.; Sampson, E.L. Mapping and understanding the decision-making process for providing nutrition and hydration to people living with dementia: A systematic review. BMC Geriatr. 2020, 20, 520. [Google Scholar] [CrossRef]
- Huis In Het Veld, J.G.; Willemse, B.M.; van Asch, I.F.; Groot Zwaaftink, R.B.; Verkade, P.J.; Twisk, J.W.; Verkaik, R.; Blom, M.M.; van Meijel, B.; Francke, A.L. Online Self-Management Support for Family Caregivers Dealing With Behavior Changes in Relatives With Dementia (Part 2): Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e13001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaingankar, J.A.; Subramaniam, M.; Picco, L.; Eng, G.K.; Shafie, S.; Sambasivam, R.; Zhang, Y.J.; Sagayadevan, V.; Chong, S.A. Perceived unmet needs of informal caregivers of people with dementia in Singapore. Int. Psychogeriatr. 2013, 25, 1605–1619. [Google Scholar] [CrossRef]
- Keller, H.; Smith, D.; Kasdorf, C.; Dupuis, S.; Schindel Martin, L.; Edward, G.; Cook, C.; Genoe, M. Nutrition Education Needs and Resources for Dementia Care in the Community. Am. J. Alzheimer’s Dis. Other Dement. 2008, 23, 13–22. [Google Scholar] [CrossRef]
- Papachristou, I.; Hickeys, G.; Iliffe, S. Involving Caregivers of People With Dementia to Validate Booklets on Food-Related Activities: A Qualitative Think-Aloud Study. J. Appl. Gerontol. 2018, 37, 644–664. [Google Scholar] [CrossRef]
- Lee, J.; Nguyen, J.; O’Leary, F. Content, Quality and Accuracy of Online Nutrition Resources for the Prevention and Treatment of Dementia: A Review of Online Content. Dietetics 2022, 1, 148–163. [Google Scholar] [CrossRef]
- Keller, H.H.; Martin, L.S.; Dupuis, S.; Reimer, H.; Genoe, R. Strategies to support engagement and continuity of activity during mealtimes for families living with dementia; a qualitative study. BMC Geriatr. 2015, 15, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, R.D.; Black, L.J.; Begley, A. Nutrition Education Programs for Adults with Neurological Diseases Are Lacking: A Scoping Review. Nutrients 2022, 14, 1577. [Google Scholar] [CrossRef]
- Papachristou, I.; Hickey, G.; Iliffe, S. Dementia informal caregiver obtaining and engaging in food-related information and support services. Dementia 2017, 16, 108–118. [Google Scholar] [CrossRef]
- Gibson, C.; Goeman, D.; Hutchinson, A.; Yates, M.; Pond, D. The provision of dementia care in general practice: Practice nurse perceptions of their role. BMC Fam. Pract. 2021, 22, 110. [Google Scholar] [CrossRef]
- Martin, A.; O’Connor, S.; Jackson, C. A scoping review of gaps and priorities in dementia care in Europe. Dementia 2020, 19, 2135–2151. [Google Scholar] [CrossRef] [Green Version]
- Smith, L.; Amella, E.J.; Nemeth, L. Perceptions of Home Health Nurses Regarding Suffering, Artificial Nutrition, and Hydration in Late-Stage Dementia. Home Healthc. Now. 2016, 34, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Yang, X.; Song, Y.; Song, B.; Zhang, Y.; Liu, J.; Wang, Q.; Yu, J. Challenges of Dementia Care in China. Geriatrics 2017, 2, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, P.; Barrado-Martín, Y.; Anantapong, K.; Moore, K.; Smith, C.; Sampson, E.; Manthorpe, J.; Walters, K.; Davies, N. Experiences of Carers and People with Dementia from Ethnic Minority Groups Managing Eating and Drinking at Home in the United Kingdom. Nutrients 2022, 14, 2395. [Google Scholar] [CrossRef]
- Timlin, D.; Giannantoni, B.; McCormack, J.M.; Polito, A.; Ciarapica, D.; Azzini, E.; Giles, M.; Simpson, E.E.A. Comparison of barriers and facilitators of MIND diet uptake among adults from Northern Ireland and Italy. BMC Public. Health 2021, 21, 265. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, H.-C.; Chao, H.-C.; Wang, J.-J. Features of problematic eating behaviors among community-dwelling older adults with dementia: Family caregivers’ experience. Geriatr. Nurs. 2013, 34, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, X.; Su, J.; Li, H.; Meng, X.; Zhang, S.; Fang, S.; Wang, W.; Bao, L.; Sun, J. Optimizing mealtime care for people with dementia from the perspective of formal caregivers: A systematic review of qualitative research. Int. J. Nurs. Stud. 2021, 123, 104046. [Google Scholar] [CrossRef]
- Freitag, D. Caregiver Perception and Knowledge on Dementia-Specific Nutritional Approaches. Master’s Thesis, Minnesota State University, Mankato, MN, USA, 2021. [Google Scholar]
- Chai, B.; Gao, F.; Wu, R.; Dong, T.; Gu, C.; Lin, Q.; Zhang, Y. Vitamin D deficiency as a risk factor for dementia and Alzheimer’s disease: An updated meta-analysis. BMC Neurol. 2019, 19, 284. [Google Scholar] [CrossRef] [PubMed]
- D’Cunha, N.M.; Georgousopoulou, E.N.; Dadigamuwage, L.; Kellett, J.; Panagiotakos, D.B.; Thomas, J.; McKune, A.J.; Mellor, D.D.; Naumovski, N. Effect of long-term nutraceutical and dietary supplement use on cognition in the elderly: A 10-year systematic review of randomised controlled trials. Br. J. Nutr. 2018, 119, 280–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siervo, M.; Shannon, O.M.; Llewellyn, D.J.; Stephan, B.C.M.; Fontana, L. Mediterranean diet and cognitive function: From methodology to mechanisms of action. Free Radic. Biol. Med. 2021, 176, 105–117. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All Carers | Female Carers | Male Carers | p-Value | |
|---|---|---|---|---|
| n | 57 | 44 | 13 | |
| 63.0 ± 13.1 | 61.5 ± 12.1 | 68.2 ± 15.3 | 0.108 | |
| Education: | 0.475 | |||
| Certificate/diploma | 11 | 8 | 3 | |
| Year 10 or equivalent | 3 | 3 | 0 | |
| Year 12 or equivalent | 4 | 2 | 2 | |
| University degree | 24 | 18 | 6 | |
| Higher university degree | 15 | 13 | 2 | |
| Time spent being a carer: | 0.674 | |||
| <6 months | 2 | 2 | 0 | |
| 6 months–1 year | 5 | 3 | 2 | |
| 1 year–2 years | 6 | 5 | 1 | |
| 2 years to 5 years | 23 | 19 | 4 | |
| 5 years to 10 years | 21 | 15 | 6 | |
| Relationship: | 0.786 | |||
| Spouse | 26 | 18 | 8 | |
| Child | 16 | 13 | 3 | |
| Grandchild | 1 | 1 | 0 | |
| Other relative | 8 | 6 | 2 | |
| Neighbour/friend | 1 | 1 | 0 | |
| Personal care worker | 3 | 3 | 0 | |
| Other | 2 | 2 | 0 | |
| Retirement: | 0.022 | |||
| Yes | 28 | 18 | 10 | |
| No | 29 | 26 | 3 | |
| Area of residence: | 0.943 | |||
| Urban | 39 | 28 | 11 | |
| Regional | 18 | 16 | 2 | |
| Ethnicity: | 0.505 | |||
| Australian | 34 | 27 | 7 | |
| African | 1 | 1 | 0 | |
| British | 8 | 7 | 1 | |
| Chinese | 3 | 1 | 2 | |
| European | 6 | 5 | 1 | |
| South Asian | 2 | 1 | 1 | |
| Other | 3 | 2 | 1 |
| All Carers | Female Carers | Male Carers | p-Value | |
|---|---|---|---|---|
| n | 57 | 44 | 13 | |
| AUS-R GNKQ scores | 22.9 ± 4.57 | 23.8 ± 4.51 | 20.0 ± 3.53 | 0.007 |
| Resources accessed by carers: | 0.213 | |||
| Consulted a dietitian | 8 | 7 | 1 | |
| Consulted GP | 6 | 4 | 2 | |
| Specialist (e.g., geriatrician) | 5 | 4 | 1 | |
| Advice from friend/family | 2 | 2 | 0 | |
| Read a book about nutrition | 3 | 3 | 0 | |
| Course on nutrition | 1 | 0 | 1 | |
| Internet | 1 | 0 | 1 | |
| Multidisciplinary team | 15 | 12 | 3 | |
| Did not answer | 16 | 12 | 4 | |
| Perceived balanced diet provided by the carer: | 0.754 | |||
| Yes | 36 | 28 | 8 | |
| No | 13 | 9 | 4 | |
| Not sure | 6 | 5 | 1 | |
| Change in protein consumption: | 0.884 | |||
| Not sure | 2 | 2 | 0 | |
| Increase | 5 | 3 | 1 | |
| Decrease | 29 | 22 | 7 | |
| No change | 21 | 16 | 5 | |
| Sweet foods craving: | 0.139 | |||
| Not sure | 2 | 2 | 0 | |
| Increase | 27 | 19 | 8 | |
| Decrease | 12 | 12 | 0 | |
| No change | 16 | 11 | 5 | |
| Fruit and vegetable intake: | 0.855 | |||
| Not sure | 2 | 2 | 0 | |
| Increase | 10 | 8 | 2 | |
| Decrease | 22 | 17 | 5 | |
| No change | 23 | 17 | 6 | |
| Consumption of salty foods: | 0.755 | |||
| Not sure | 2 | 2 | 0 | |
| Increase | 7 | 6 | 1 | |
| Decrease | 10 | 8 | 2 | |
| No change | 38 | 28 | 10 | |
| Observed weight change: | 0.655 | |||
| Weight gain | 10 | 7 | 3 | |
| Weight loss | 31 | 25 | 6 | |
| No change | 12 | 8 | 4 | |
| Weight fluctuation | 1 | 1 | 0 | |
| Did not answer | 3 | 3 | 0 | |
| Nutrition-related issues: | 0.900 | |||
| No issues | 12 | 8 | 4 | |
| Dysphagia | 2 | 2 | 0 | |
| Forgetting to eat | 5 | 4 | 1 | |
| Chewing difficulties | 2 | 2 | 0 | |
| Functional difficulties | 3 | 2 | 1 | |
| Refusing offered food | 10 | 8 | 2 | |
| Combination of multiple issues | 23 | 18 | 5 |
| Code | Age | Ethnicity | Dementia Type | Relationship | Years as a Carer | Place of Residence | Occupation | AUS-R NKQ Result |
|---|---|---|---|---|---|---|---|---|
| P1 | 69 | Australian | Unsure | Family member | 5–10 | NSW | Nurse | 31 |
| P2 | 61 | European | Vascular | Live-in carer | 5–10 | QLD | Live-in carer | 24 |
| P3 | 64 | British | Lewy Body | Child | 5–10 | NSW | Psychologist | 21 |
| P4 | 69 | European | Alzheimer’s | Spouse | 2–5 | SA | Retired | 24 |
| P5 | 56 | Australian | Alzheimer’s | Child | 2–5 | NSW | Social worker | 18 |
| P6 | 51 | European | Alcohol-related | Spouse | 5–10 | NSW | Social worker | 21 |
| P7 | 68 | Australian | Vascular | Family member | 2–5 | SA | Retired | 26 |
| P8 | 53 | Australian | Alzheimer’s | Child | 1–2 | WA | Writer | 24 |
| P9 | 78 | Australian | Alzheimer’s | Spouse | 2–5 | NSW | Retired | 24 |
| P10 | 67 | Australian | Alzheimer’s | Spouse | 2–5 | NSW | Retired | 29 |
| P11 | 77 | Australian | Alzheimer’s | Spouse | 5–10 | NSW | Retired | 22 |
| Theme | Sub-Theme |
|---|---|
|
|
|
|
| |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lahiouel, A.; Kellett, J.; Isbel, S.; D’Cunha, N.M. An Exploratory Study of Nutrition Knowledge and Challenges Faced by Informal Carers of Community-Dwelling People with Dementia: Online Survey and Thematic Analysis. Geriatrics 2023, 8, 77. https://doi.org/10.3390/geriatrics8040077
Lahiouel A, Kellett J, Isbel S, D’Cunha NM. An Exploratory Study of Nutrition Knowledge and Challenges Faced by Informal Carers of Community-Dwelling People with Dementia: Online Survey and Thematic Analysis. Geriatrics. 2023; 8(4):77. https://doi.org/10.3390/geriatrics8040077
Chicago/Turabian StyleLahiouel, Abdeljalil, Jane Kellett, Stephen Isbel, and Nathan M. D’Cunha. 2023. "An Exploratory Study of Nutrition Knowledge and Challenges Faced by Informal Carers of Community-Dwelling People with Dementia: Online Survey and Thematic Analysis" Geriatrics 8, no. 4: 77. https://doi.org/10.3390/geriatrics8040077