

Guiding Post-Hospital Recovery by ‘What Matters:’ Implementation of Patient Priorities Identification in a VA Community Living Center
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
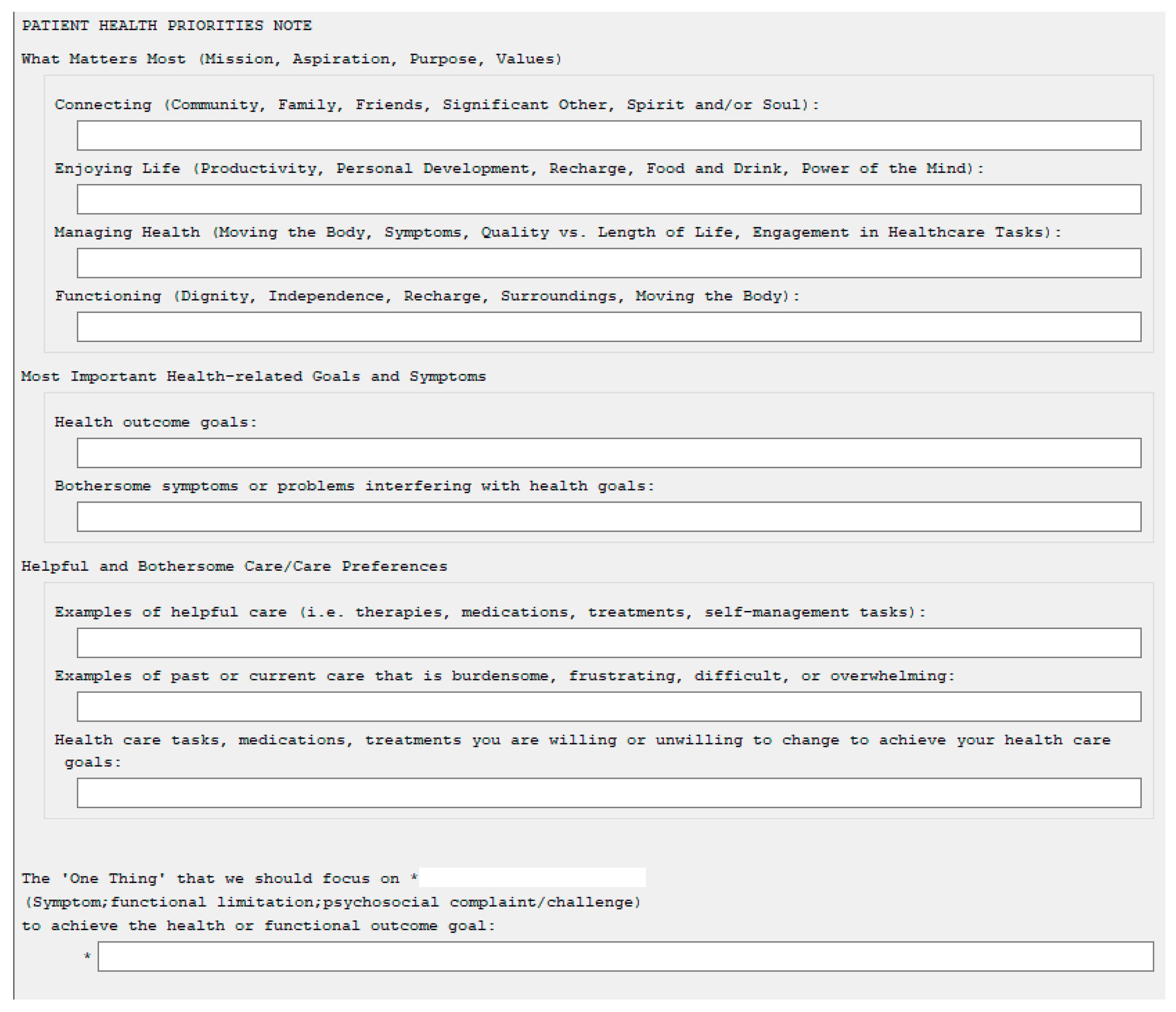
2.2. Health Priorities Identification (HPI)
2.3. Health Priorities Identification (HPI) Implementation Strategy
2.3.1. Implementation Team
2.3.2. HPI Facilitator Training
2.4. Implementation Measurement and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stange, K.C. In This Issue: Challenges of Managing Multimorbidity. Ann. Fam. Med. 2012, 10, 2–3. [Google Scholar] [CrossRef] [Green Version]
- Tinetti, M.E. The gap between clinical trials and the real world: Extrapolating treatment effects from younger to older adults. JAMA Intern. Med. 2014, 174, 397–398. [Google Scholar] [CrossRef]
- Naik, A.D.; Martin, L.A.; Moye, J.; Karel, M.J. Health Values and Treatment Goals of Older, Multimorbid Adults Facing Life-Threatening Illness. J. Am. Geriatr. Soc. 2016, 64, 625–631. [Google Scholar] [CrossRef] [Green Version]
- Institute for Healthcare Improvement: What is an Age-Friendly System. Available online: http://www.ihi.org/Engage/Initiatives/Age-Friendly-Health-Systems/Pages/default.aspx (accessed on 24 March 2022).
- Tinetti, M.E.; Costello, D.M.; Naik, A.D.; Davenport, C.; Hernandez-Bigos, K.; Van Liew, J.R.; Esterson, J.; Kiwak, E.; Dindo, L. Outcome Goals and Health Care Preferences of Older Adults with Multiple Chronic Conditions. JAMA Netw. Open 2021, 4, e211271. [Google Scholar] [CrossRef]
- Naik, A.; Tinetti, M.; Dindo, L. Available online: https://patientprioritiescare.org/wp-content/uploads/2022/02/ppc-health-priorities-1024x576.jpg (accessed on 8 April 2022).
- Tinetti, M.; Dindo, L.; Smith, C.D.; Blaum, C.; Costello, D.; Ouellet, G.; Rosen, J.; Hernandez-Bigos, K.; Geda, M.; Naik, A. Challenges and strategies in patients’ health priorities-aligned decision-making for older adults with multiple chronic conditions. PLoS ONE 2019, 14, e0218249. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Naik, A.D.; Dindo, L.; Costello, D.M.; Esterson, J.; Geda, M.; Rosen, J.; Hernandez-Bigos, K.; Smith, C.D.; Ouellet, G.M.; et al. Association of Patient Priorities-Aligned Decision-Making with Patient Outcomes and Ambulatory Health Care Burden Among Older Adults With Multiple Chronic Conditions: A Nonrandomized Clinical Trial. JAMA Intern. Med. 2019, 179, 1688–1697. [Google Scholar] [CrossRef]
- Van den Brink, A.M.; Gerritsen, D.L.; Voshaar, R.C.; Koopmans, R.T. Residents with mental-physical multimorbidity living in long-term care facilities: Prevalence and characteristics. A systematic review. Int. Psychogeriatr. 2013, 25, 531–548. [Google Scholar] [CrossRef]
- Hojlo, C. The VA’s Transformation of Nursing Home Care: From Nursing Homes to Community Living Centers. Generations 2010, 34, 43–48. [Google Scholar]
- Thomas, K.S.; Cote, D.; Makineni, R.; Intrator, O.; Kinosian, B.; Phibbs, C.S.; Allen, S.M. Change in VA Community Living Centers 2004–2011: Shifting Long-Term Care to the Community. J. Aging Soc. Policy 2018, 30, 93–108. [Google Scholar] [CrossRef]
- Ouellet, G.M.; Kiwak, E.; Costello, D.M.; Green, A.R.; Geda, M.; Naik, A.D.; Tinetti, M.E. Clinician Perspectives on Incorporating Patients’ Values-Based Health Priorities in Decision-Making. J. Am. Geriatr. Soc. 2021, 69, 267–269. [Google Scholar] [CrossRef]
- Jd, J.F.; Dindo, L.; Catic, A.; Johnson, A.; Amspoker, A.B.; Gravier, A.; Dawson, D.B.; Tinetti, M.E.; Naik, A.D. Feasibility of Clinicians Aligning Health Care with Patient Priorities in Geriatrics Ambulatory Care. J. Am. Geriatr. Soc. 2020, 68, 2112–2116. [Google Scholar] [CrossRef]
- Naik, A.D.; Dindo, L.N.; Liew, J.R.; Hundt, N.E.; Vo, L.; Hernandez-Bigos, K.; Esterson, J.; Geda, M.; Rosen, J.; Blaum, C.S.; et al. Development of a Clinically Feasible Process for Identifying Individual Health Priorities. J. Am. Geriatr. Soc. 2018, 66, 1872–1879. [Google Scholar] [CrossRef] [Green Version]
- Warren, C.; McGraw, A.P.; Van Boven, L. Values and preferences: Defining preference construction. WIREs Cogn. Sci. 2011, 2, 193–205. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Esterson, J.; Ferris, R.; Posner, P.; Blaum, C.S. Patient Priority–Directed Decision Making and Care for Older Adults with Multiple Chronic Conditions. Clin. Geriatr. Med. 2016, 32, 261–275. [Google Scholar] [CrossRef]
- Solberg, L.I. Improving Medical Practice: A Conceptual Framework. Ann. Fam. Med. 2007, 5, 251–256. [Google Scholar] [CrossRef]
- Blaum, C.S.; Rosen, J.; Naik, A.D.; Smith, C.D.; Dindo, L.; Vo, L.; Ba, K.H.; Esterson, J.; Geda, M.; Ferris, R.; et al. Feasibility of Implementing Patient Priorities Care for Older Adults with Multiple Chronic Conditions. J. Am. Geriatr. Soc. 2018, 66, 2009–2016. [Google Scholar] [CrossRef] [Green Version]
- Neal, J.W.; Neal, Z.P.; VanDyke, E.; Kornbluh, M. Expediting the Analysis of Qualitative Data in Evaluation:A Procedure for the Rapid Identification of Themes From Audio Recordings (RITA). Am. J. Eval. 2015, 36, 118–132. [Google Scholar] [CrossRef] [Green Version]
- Lagrotteria, A.; Swinton, M.; Simon, J.; King, S.; Boryski, G.; Ma, I.W.Y.; Dunne, F.; Singh, J.; Bernacki, R.E.; You, J.J. Clinicians’ Perspectives After Implementation of the Serious Illness Care Program: A Qualitative Study. JAMA Netw. Open 2021, 4, e2121517. [Google Scholar] [CrossRef]
- Lage, D.E.; Caudry, D.J.; Ackerly, D.C.; Keating, N.L.; Grabowski, D.C. The Care Continuum for Hospitalized Medicare Beneficiaries Near Death. Ann. Intern. Med. 2018, 168, 748. [Google Scholar] [CrossRef]
- Davenport, C.; Ouellet, J.; Tinetti, M.E. Use of the Patient-Identified Top Health Priority in Care Decision-making for Older Adults With Multiple Chronic Conditions. JAMA Netw. Open 2021, 4, e2131496. [Google Scholar] [CrossRef]
- The Agency for Healthcare Research and Quality: The Share Approach. Available online: https://www.ahrq.gov/health-literacy/curriculum-tools/shareddecisionmaking/index.html (accessed on 8 June 2022).
- The Agency for Healthcare Quality. The SHARE Approach-Essential Steps of Shared Decision Making: Quick Reference Guide. Available online: https://www.ahrq.gov/health-literacy/professional-training/shared-decision/tool/resource-2.html (accessed on 8 June 2020).
- Van Haitsma, K.; Abbott, K.M.; Arbogast, A.; Bangerter, L.R.; Heid, A.R.; Behrens, L.L.; Madrigal, C. A Preference-Based Model of Care: An Integrative Theoretical Model of the Role of Preferences in Person-Centered Care. Gerontologist 2020, 60, 376–384. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Cycle 1 | Cycle 2 |
|---|---|
| Plan: | Plan: |
|
|
| Do: | Do: |
|
|
| Study: | Study: |
|
|
| Act/Lessons learned: | Act/Lessons learned: |
|
|
| Theme | Quote |
|---|---|
| Appropriateness for CLC | “PPC is good fit for CLC. When working with Veterans who are very depressed with psychiatric issues, it’s a way to remind them of what they talked about and what their goals are. She has noticed one veteran in particular—goal hasn’t changed, but every day is different. His goal is he wants to go home, but he has to get stronger and eat. It makes it easier having that conversation.” “Definitely thinks it’s a good fit. Thinks figuring out what matters most to patients can help with the connection between the provider and the veteran. It gives them something to come back to when talking about with Veterans about their care, especially with rehab.” |
| Helped or hindered ability to care for Veterans | “Learning what matters most helps connection between veteran and provider, and learning those important things about veterans helps build rapport. The veteran is more likely to remember who she is; it definitely helps with veteran engagement in their rehab.” “[PPC] It’s a great model. Sees what patients want for their healthcare gets overlooked. It can also help guide a general approach so are not inundating people with specialists and medications that aren’t necessary. “I’m excited about this kind of approach to help people take charge of their own healthcare.” “PPC has been helpful. Partly just because it helps us to identify things that are really important to them so we can help tailor our approach. I don’t think it’s hindered our ability to provide clinical care.” ““if anything it helps move the care forward and that’s why it’s so important.” Taking a wholistic approach to the patient—they are more than their amputation or the sprained limb. You have to take into consideration what’s important. Definitely a value added to their care.” “[PPC] has definitely helped. When you have these interdisciplinary teams working together, it helps make sure needs are met. Helps to make care more cohesive and flowing rather than staggered.” |
| Impact of HPI on workflow | “Took a little time to get acclimated and integrate PPC into normal routine. Estimated took about 30–45 min extra, but less now. The creation of a template with the [PPC] questions cut down a lot of time. Before I was typing in every question. Now can just put in the answers the veteran gives.” “I didn’t think it had impacted [my] work flow.” “For most part it aligns with what were already trying to do but it gives more of a framework. We focus a lot on geriatric care…. It gives us a good framework to have these conversations and help direct care.” “Didn’t think impacts flow—“it’s just the way I talk to them.” Doesn’t feel that different from what [I was] doing before, just worded a little bit different.” “Would think [it] wouldn’t take as long once [one] gets more used to the conversations because right now it is new. I will stumble less.” |
| Staff/System Barriers | “Trying to delegate the [HPI conversation] responsibility to one or two individuals identified the need for more HPI facilitators. It was important to workflow to acknowledge the time it takes to have those conversations and the time it takes to document those conversations.” “A lot of PPC is changing the way providers see things. Of course, as providers they have an idea of what is best for the veteran, but they have to remember to take in what’s important to the veteran as well. They can work together. It’s a shift in how they speak to the residents.” “Sometimes there was a time [barrier] if short staffed or more patients than normal, would probably leave the additional part out and make a note to come back. But this would be very rare.” “There are few barriers to implementing PPC. It’s just a different way to have a conversation. The end goal is getting the veteran to their better state of health whatever that looks like. Instead of telling them what to do because that’s what providers want.” |
| Patient Barriers | “PPC conversations can be challenging when veterans are very depressed. Getting through the conversation in one session is hard. Have to go back and try to reengage. Veterans weren’t able to sit with her and have the entire conversation.” “Patients have no problems answering the questions, unless they have dementia.” “Some patients have been challenging. One patient severely depressed and has cognitive issues, and it’s really hard for him to think about what would be his priorities outside of ‘I want to rest and lie in bed.’ Having those conversations can be extremely time consuming and difficult.” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ritchey, K.C.; Solberg, L.M.; Citty, S.W.; Kiefer, L.; Martinez, E.; Gray, C.; Naik, A.D. Guiding Post-Hospital Recovery by ‘What Matters:’ Implementation of Patient Priorities Identification in a VA Community Living Center. Geriatrics 2023, 8, 74. https://doi.org/10.3390/geriatrics8040074
Ritchey KC, Solberg LM, Citty SW, Kiefer L, Martinez E, Gray C, Naik AD. Guiding Post-Hospital Recovery by ‘What Matters:’ Implementation of Patient Priorities Identification in a VA Community Living Center. Geriatrics. 2023; 8(4):74. https://doi.org/10.3390/geriatrics8040074
Chicago/Turabian StyleRitchey, Katherine C., Laurence M. Solberg, Sandra Wolfe Citty, Lea Kiefer, Erica Martinez, Caroline Gray, and Aanand D. Naik. 2023. "Guiding Post-Hospital Recovery by ‘What Matters:’ Implementation of Patient Priorities Identification in a VA Community Living Center" Geriatrics 8, no. 4: 74. https://doi.org/10.3390/geriatrics8040074