
Predictors of Nursing Home Entry within 36 Months after Hospitalization via the Emergency Department among Persons Aged 75 Years or Older

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
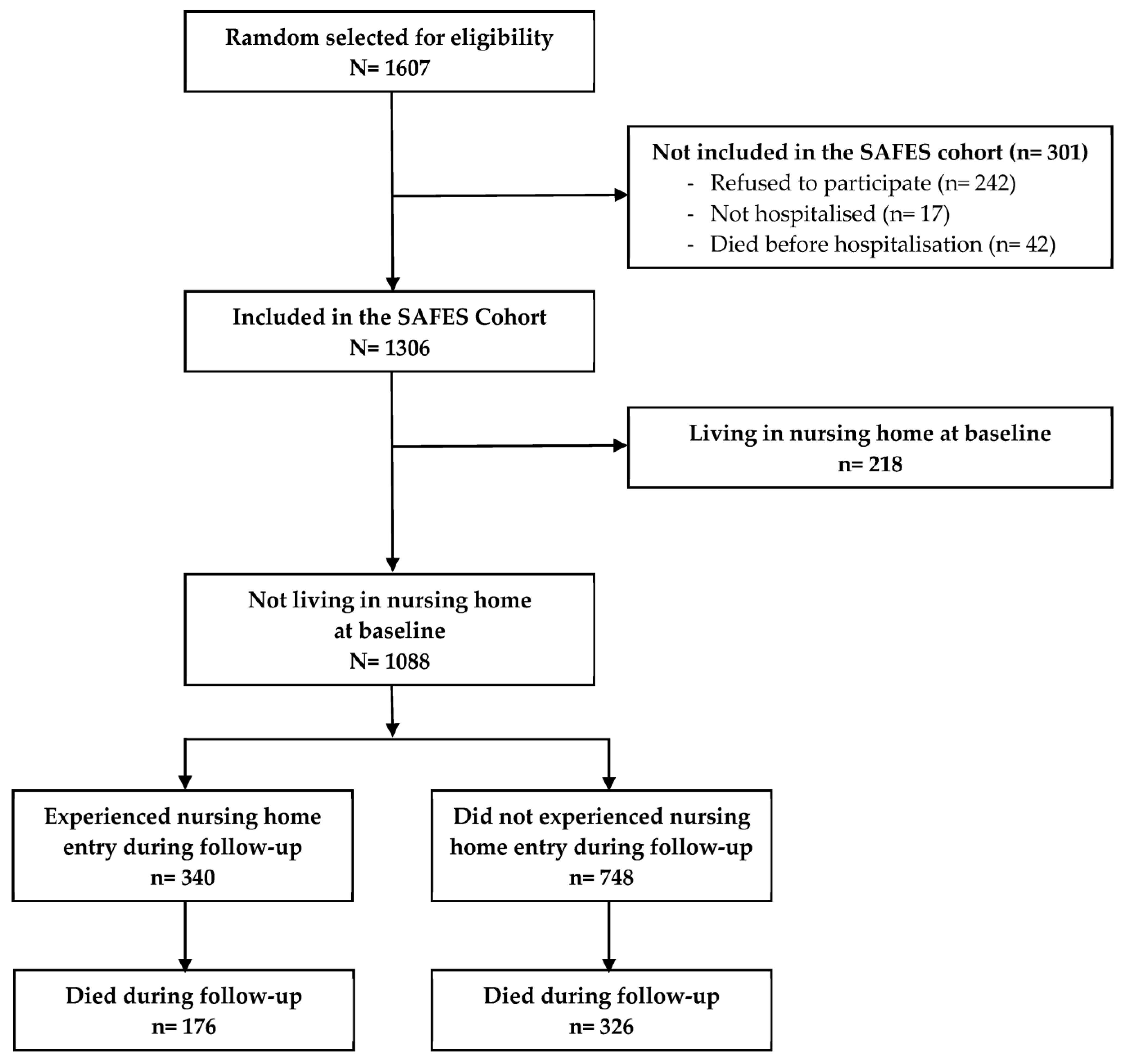
2.2. Study Population
2.3. Variables Studied
2.4. Ethical Considerations
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carrère, A.; Dubost, C. État de Santé et Dépendance des Seniors; Portrait Social: Paris, France, 2018; Volume 2018, pp. 71–78. [Google Scholar]
- Duan-Porter, W.; Ullman, K.; Rosebush, C.; McKenzie, L.; Ensrud, K.E.; Ratner, E.; Greer, N.; Shippee, T.; Gaugler, J.E.; Wilt, T.J. Interventions to Prevent or Delay Long-Term Nursing Home Placement for Adults with Impairments—A Systematic Review of Reviews. J. Gen. Intern. Med. 2020, 35, 2118–2129. [Google Scholar] [CrossRef] [PubMed]
- Marek, K.D.; Stetzer, F.; Adams, S.J.; Popejoy, L.L.; Rantz, M. Aging in place versus nursing home care: Comparison of costs to Medicare and Medicaid. Res. Gerontol. Nurs. 2012, 5, 123–129. [Google Scholar] [CrossRef]
- Campbell-Enns, H.J.; Campbell, M.; Rieger, K.L.; Thompson, G.N.; Doupe, M.B. No Other Safe Care Option: Nursing Home Admission as a Last Resort Strategy. Gerontologist 2020, 60, 1504–1514. [Google Scholar] [CrossRef] [PubMed]
- Hajek, A.; Brettschneider, C.; Lange, C.; Posselt, T.; Wiese, B.; Steinmann, S.; Weyerer, S.; Werle, J.; Pentzek, M.; Fuchs, A.; et al. Longitudinal Predictors of Institutionalization in Old Age. PLoS ONE 2015, 10, e0144203. [Google Scholar] [CrossRef] [PubMed]
- Viljanen, A.; Salminen, M.; Irjala, K.; Heikkila, E.; Isoaho, R.; Kivela, S.L.; Korhonen, P.; Vahlberg, T.; Viitanen, M.; Wuorela, M.; et al. Chronic conditions and multimorbidity associated with institutionalization among Finnish community-dwelling older people: An 18-year population-based follow-up study. Eur. Geriatr. Med. 2021, 12, 1275–1284. [Google Scholar] [CrossRef]
- Takeuchi, M.; Showa, S.; Kitazawa, K.; Mori, M. Living alone is associated with an increased risk of institutionalization in older men: A follow-up study in Hamanaka Town of Hokkaido, Japan. Geriatr. Gerontol. Int. 2018, 18, 867–872. [Google Scholar] [CrossRef]
- Uriz-Otano, F.; Pla-Vidal, J.; Tiberio-Lopez, G.; Malafarina, V. Factors associated to institutionalization and mortality over three years, in elderly people with a hip fracture—An observational study. Maturitas 2016, 89, 9–15. [Google Scholar] [CrossRef]
- Salminen, M.; Laine, J.; Vahlberg, T.; Viikari, P.; Wuorela, M.; Viitanen, M.; Viikari, L. Factors associated with institutionalization among home-dwelling patients of Urgent Geriatric Outpatient Clinic: A 3-year follow-up study. Eur. Geriatr. Med. 2020, 11, 745–751. [Google Scholar] [CrossRef]
- Ramsey, K.A.; Rojer, A.G.M.; van Garderen, E.; Struik, Y.; Kay, J.E.; Lim, W.K.; Meskers, C.G.M.; Reijnierse, E.M.; Maier, A.B. The Association of Changes in Physical Performance during Geriatric Inpatient Rehabilitation with Short-Term Hospital Readmission, Institutionalization, and Mortality: RESORT. J. Am. Med. Dir. Assoc. 2022, 23, 1883.e1–1883.e8. [Google Scholar] [CrossRef]
- Jung, H.W.; Jang, I.Y.; Lee, C.K.; Yu, S.S.; Hwang, J.K.; Jeon, C.; Lee, Y.S.; Lee, E. Usual gait speed is associated with frailty status, institutionalization, and mortality in community-dwelling rural older adults: A longitudinal analysis of the Aging Study of Pyeongchang Rural Area. Clin. Interv. Aging 2018, 13, 1079–1089. [Google Scholar] [CrossRef] [Green Version]
- Drame, M.; Novella, J.L.; Lang, P.O.; Somme, D.; Jovenin, N.; Laniece, I.; Couturier, P.; Heitz, D.; Gauvain, J.B.; Voisin, T.; et al. Derivation and validation of a mortality-risk index from a cohort of frail elderly patients hospitalised in medical wards via emergencies: The SAFES study. Eur. J. Epidemiol. 2008, 23, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Akpom, C.A. A measure of primary sociobiological functions. Int. J. Health Serv. 1976, 6, 493–508. [Google Scholar] [CrossRef] [PubMed]
- Gilleard, C.J.; Willmott, M.; Vaddadi, K.S. Self-report measures of mood and morale in elderly depressives. Br. J. Psychiatry 1981, 138, 230–235. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatry Association. DSM-IV, Diagnosis and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatry Association: Washington, DC, USA, 1994. [Google Scholar]
- Rubenstein, L.Z.; Harker, J.O.; Salva, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathias, S.; Nayak, U.S.; Isaacs, B. Balance in elderly patients: The “get-up and go” test. Arch. Phys. Med. Rehabil. 1986, 67, 387–389. [Google Scholar] [PubMed]
- Vellas, B.J.; Wayne, S.J.; Romero, L.; Baumgartner, R.N.; Rubenstein, L.Z.; Garry, P.J. One-leg balance is an important predictor of injurious falls in older persons. J. Am. Geriatr. Soc. 1997, 45, 735–738. [Google Scholar] [CrossRef]
- Sundararajan, V.; Henderson, T.; Perry, C.; Muggivan, A.; Quan, H.; Ghali, W.A. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 2004, 57, 1288–1294. [Google Scholar] [CrossRef]
- Norton, D.; McLaren, R.; Exton-Smith, A.N. An Investigation of Nursing Problems in Hospitals; Churchill Livingstone: New York, NY, USA, 1975. [Google Scholar]
- Fine, J.; Gray, R. A proportional hazards model for the subdistribution of a competing risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Kay, R. Goodness of fit methods for the proportional hazards regression model: A review. Rev. Epidemiol. Sante Publique 1984, 32, 185–198. [Google Scholar]
- Kim, Y.P.; Choe, Y.R.; Park, J.H.; Kim, S.; Won, C.W.; Hwang, H.S. Frailty index associated with all-cause mortality, long-term institutionalization, and hip fracture. Eur. Geriatr. Med. 2019, 10, 403–411. [Google Scholar] [CrossRef]
- Bunt, S.; Steverink, N.; Olthof, J.; van der Schans, C.P.; Hobbelen, J.S.M. Social frailty in older adults: A scoping review. Eur. J. Ageing 2017, 14, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Quach, L.T.; Primack, J.; Bozzay, M.; Madrigal, C.; Erqou, S.; Rudolph, J.L. The Intersection of Physical and Social Frailty in Older Adults. Rhode Isl. Med. J. 2021, 104, 16–19. [Google Scholar]
- Makizako, H.; Shimada, H.; Tsutsumimoto, K.; Lee, S.; Doi, T.; Nakakubo, S.; Hotta, R.; Suzuki, T. Social Frailty in Community-Dwelling Older Adults as a Risk Factor for Disability. J. Am. Med. Dir. Assoc. 2015, 16, 1003.e7–1003.e11. [Google Scholar] [CrossRef] [PubMed]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Makino, K.; Lee, S. Social Frailty Leads to the Development of Physical Frailty among Physically Non-Frail Adults: A Four-Year Follow-Up Longitudinal Cohort Study. Int. J. Environ. Res. Public Health 2018, 15, 490. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.H.; Okada, K.; Matsushita, E.; Uno, C.; Satake, S.; Martins, B.A.; Kuzuya, M. The association of social frailty with intrinsic capacity in community-dwelling older adults: A prospective cohort study. BMC Geriatr. 2021, 21, 515. [Google Scholar] [CrossRef]
- Burholt, V.; Windle, G.; Ferring, D.; Balducci, C.; Fagerstrom, C.; Thissen, F.; Weber, G.; Wenger, G.C. Reliability and validity of the Older Americans Resources and Services (OARS) social resources scale in six European countries. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2007, 62, S371–S379. [Google Scholar] [CrossRef] [Green Version]
- Miralles, R.; Sabartes, O.; Ferrer, M.; Esperanza, A.; Llorach, I.; Garcia-Palleiro, P.; Cervera, A.M. Development and validation of an instrument to predict probability of home discharge from a geriatric convalescence unit in Spain. J. Am. Geriatr. Soc. 2003, 51, 252–257. [Google Scholar] [CrossRef]
- Zheng, P.P.; Guo, Z.L.; Du, X.J.; Yang, H.M.; Wang, Z.J. Prevalence of Disability among the Chinese Older Population: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 1656. [Google Scholar] [CrossRef]
- Berlau, D.J.; Corrada, M.M.; Kawas, C. The prevalence of disability in the oldest-old is high and continues to increase with age: Findings from The 90+ Study. Int. J. Geriatr. Psychiatry 2009, 24, 1217–1225. [Google Scholar] [CrossRef] [Green Version]
- Guay, M.; Dubois, M.F.; Corrada, M.; Lapointe-Garant, M.P.; Kawas, C. Exponential increases in the prevalence of disability in the oldest old: A Canadian national survey. Gerontology 2014, 60, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Ganapathy, A.; Nieves, J.W. Nutrition and Sarcopenia—What Do We Know? Nutrients 2020, 12, 1755. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Dawson, A.; Shaw, S.C.; Harvey, N.C.; Kanis, J.A.; Binkley, N.; Reginster, J.Y.; Chapurlat, R.; Chan, D.C.; Bruyere, O.; et al. Nutrition and physical activity in the prevention and treatment of sarcopenia: Systematic review. Osteoporos. Int. 2017, 28, 1817–1833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marengoni, A.; Tazzeo, C.; Calderon-Larranaga, A.; Roso-Llorach, A.; Onder, G.; Zucchelli, A.; Rizzuto, D.; Vetrano, D.L. Multimorbidity Patterns and 6-Year Risk of Institutionalization in Older Persons: The Role of Social Formal and Informal Care. J. Am. Med. Dir. Assoc. 2021, 22, 2184–2189.e1. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | N | % |
|---|---|---|
| Age (years) | ||
| <85 | 592 | 54.4 |
| ≥85 | 496 | 45.6 |
| Sex | ||
| Female | 667 | 61.3 |
| Male | 421 | 38.7 |
| Level of education | ||
| Primary school (or less) | 719 | 70.0 |
| Secondary school | 216 | 21.0 |
| University | 92 | 9.0 |
| Living alone | ||
| No | 542 | 50.8 |
| Yes | 526 | 49.2 |
| Main caregiver | ||
| No | 356 | 32.7 |
| Yes | 732 | 67.3 |
| Formal help | ||
| No | 314 | 30.2 |
| Yes | 726 | 69.8 |
| Informal help | ||
| No | 121 | 11.6 |
| Yes | 919 | 88.4 |
| Dependence for the ADLs | ||
| No | 180 | 17.2 |
| Yes | 869 | 82.8 |
| Walking difficulties | ||
| No | 225 | 20.7 |
| Yes | 862 | 79.3 |
| Balance difficulties | ||
| No | 525 | 48.9 |
| Yes | 548 | 51.1 |
| Dementia syndrome | ||
| No | 629 | 58.4 |
| Yes | 449 | 41.6 |
| Delirium | ||
| No | 857 | 79.5 |
| Yes | 221 | 20.5 |
| Depression or risk thereof | ||
| No | 641 | 58.9 |
| Yes | 447 | 41.1 |
| Serum albumin (g/L) | ||
| ≥35 | 445 | 41.8 |
| <35 | 633 | 58.2 |
| Total MNA Score | ||
| ≥24 | 449 | 41.3 |
| <24 | 639 | 58.7 |
| Risk of pressure ulcers | ||
| No | 711 | 65.5 |
| Yes | 374 | 34.5 |
| Visual impairment | ||
| No | 534 | 51.4 |
| Yes | 505 | 48.6 |
| Hearing impairment | ||
| No | 613 | 56.6 |
| Yes | 470 | 43.4 |
| Recent hospital admission | ||
| No | 781 | 73.1 |
| Yes | 288 | 26.9 |
| Day of hospital admission | ||
| Weekday | 835 | 76.8 |
| Weekend | 253 | 23.2 |
| Bivariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| Characteristics | OR | IC 95% | p | OR | IC 95% | p |
| Age (years): ≥85 | 2.16 | 1.73–2.68 | <0.0001 | |||
| Male sex | 0.74 | 0.59–0.94 | 0.01 | |||
| Level of education | ||||||
| Primary school (or less) | 1 | |||||
| Secondary school | 0.96 | 0.73–1.27 | 0.79 | |||
| University | 0.74 | 0.48–1.14 | 0.17 | |||
| Living alone: yes | 1.80 | 1.44–2.25 | <0.0001 | 2.00 | 1.59–2.54 | <0.0001 |
| Main caregiver: yes | 1.13 | 0.90–1.43 | 0.28 | |||
| Formal help: yes | 1.48 | 1.15–1.91 | 0.003 | |||
| Informal help: yes | 0.80 | 0.58–1.11 | 0.17 | |||
| Dependence for the ADLs: yes | 2.17 | 1.55–3.05 | <0.0001 | 1.81 | 1.24–2.64 | 0.002 |
| Walking difficulties: yes | 1.40 | 1.05–1.88 | 0.02 | |||
| Balance difficulties: yes | 1.60 | 1.29–2.00 | <0.0001 | 1.37 | 1.09–1.73 | 0.007 |
| Dementia syndrome: yes | 2.03 | 1.64–2.52 | <0.0001 | 1.80 | 1.42–2.29 | <0.0001 |
| Delirium: yes | 1.03 | 0.77–1.37 | 0.86 | |||
| Depression or risk thereof: yes | 1.29 | 1.04–1.60 | 0.02 | |||
| Serum albumin level: <35 g/L | 0.94 | 0.76–1.16 | 0.55 | |||
| Total MNA score: <24 | 1.11 | 0.89–1.38 | 0.36 | |||
| Risk of pressure ulcers: yes | 1.78 | 1.43–2.22 | <0.0001 | 1.42 | 1.10–1.82 | 0.006 |
| Visual impairment: yes | 1.19 | 0.96–1.48 | 0.12 | |||
| Hearing impairment: yes | 1.15 | 0.93–1.43 | 0.20 | |||
| Recent hospital admission: yes | 1.01 | 0.79–1.29 | 0.94 | |||
| Day of hospital admission: weekend | 1.24 | 0.97–1.58 | 0.08 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dramé, M.; Volberg, A.; Kanagaratnam, L.; Coutureau, C.; Godaert, L. Predictors of Nursing Home Entry within 36 Months after Hospitalization via the Emergency Department among Persons Aged 75 Years or Older. Geriatrics 2023, 8, 67. https://doi.org/10.3390/geriatrics8030067
Dramé M, Volberg A, Kanagaratnam L, Coutureau C, Godaert L. Predictors of Nursing Home Entry within 36 Months after Hospitalization via the Emergency Department among Persons Aged 75 Years or Older. Geriatrics. 2023; 8(3):67. https://doi.org/10.3390/geriatrics8030067
Chicago/Turabian StyleDramé, Moustapha, Alison Volberg, Lukshe Kanagaratnam, Claire Coutureau, and Lidvine Godaert. 2023. "Predictors of Nursing Home Entry within 36 Months after Hospitalization via the Emergency Department among Persons Aged 75 Years or Older" Geriatrics 8, no. 3: 67. https://doi.org/10.3390/geriatrics8030067