
Comprehensive Geriatric Care in Older Hospitalized Patients with Depressive Symptoms
 , , and
, , and
Abstract
:1. Background
2. Methods
2.1. Patients and Study Design
2.2. Comprehensive Geriatric Care (CGC)
2.3. Data Documentation and Assessments
2.4. Geriatric Depression Scale
2.5. Assessment of Walking Ability (Timed Up and Go Test, TuG)
2.6. Assessment of Balance and Gait (Tinetti Balance and Gait Test)
2.7. Mini-Mental-State Examination (MMSE)
2.8. Assessment of Basic Activities of Daily Living (Barthel Index)
2.9. Statistical Analyses
2.10. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DS | Depressive symptoms |
| GDS | Geriatric Depression Scale |
| CGC | Comprehensive geriatric care |
| TuG | Timed Up and Go test |
| IQR | Interquartile range |
| MMSE | Mini-Mental-State Evaluation |
References
- Fuhrmann, R. Ubersicht über die Versorgungsstrukturen der klinischen und rehabilitativen Geriatrie und ihre Entwicklung in der Bundesrepublik Deutschland [Overview of health care services in clinical and rehabilitation geriatrics and their development in Germany]. Z. Gerontol. Geriatr. 2001, 34, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Kolb, G.; Breuninger, K.; Gronemeyer, S.; van den Heuvel, D.; Lübke, N.; Lüttje, D.; Wittrich, A.; Wolff, J. Ten years of early complex geriatric rehabilitation therapy in the DRG system. Z. Gerontol. Geriatr. 2014, 47, 6–12. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, D.; Veer, A.; Greuel, H.W. Geriatric health care structures in Germany. The cross-border cooperation in geriatric medicine as a needs-driven further development. Z. Gerontol. Geriatr. 2014, 47, 13–16. [Google Scholar] [CrossRef]
- Amaral Gomes, E.S.; Ramsey, K.A.; Rojer, A.G.M.; Reijnierse, E.M.; Maier, A.B. The Association of Objectively Measured Physical Activity and Sedentary Behavior with (Instrumental) Activities of Daily Living in Community-Dwelling Older Adults: A Systematic Review. Clin. Interv. Aging 2021, 16, 1877–1915. [Google Scholar] [CrossRef] [PubMed]
- Rojer, A.G.M.; Ramsey, K.A.; Amaral Gomes, E.S.; D'Andrea, L.; Chen, C.; Szoeke, C.; Meskers, C.G.M.; Reijnierse, E.M.; Maier, A.B. Objectively assessed physical activity and sedentary behavior and global cognitive function in older adults: A systematic review. Mech. Ageing Dev. 2021, 198, 111524. [Google Scholar] [CrossRef]
- Walli-Attaei, M.; Rosengren, A.; Rangarajan, S.; Breet, Y.; Abdul-Razak, S.; Sharief, W.A.; Alhabib, K.F.; Avezum, A.; Chifamba, J.; Diaz, R.; et al. Metabolic, behavioural, and psychosocial risk factors and cardiovascular disease in women compared with men in 21 high-income, middle-income, and low-income countries: An analysis of the PURE study. Lancet 2022, 400, 811–821. [Google Scholar] [CrossRef]
- de Munter, L.; van de Ree, C.L.P.; van der Jagt, O.P.; Gosens, T.; Maas, H.A.A.M.; de Jongh, M.A.C. Trajectories and prognostic factors for recovery after hip fracture: A longitudinal cohort study. Int. Orthop. 2022. [Google Scholar] [CrossRef]
- Mylona, E.; Kourou, K.; Manikis, G.; Kondylakis, H.; Marias, K.; Karademas, E.; Poikonen-Saksela, P.; Mazzocco, K.; Marzorati, C.; Pat-Horenczyk, R.; et al. Trajectories and Predictors of Depression After Breast Cancer Diagnosis: A 1-year longitudinal study. In Proceedings of the 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, UK, 11–15 July 2022. [Google Scholar]
- Tsuji, T. Rehabilitation for elderly patients with cancer. Jpn. J. Clin. Oncol. 2022, 139. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, D.; Perkins, A.J.; Fuchita, M.; Gao, S.; Holler, E.; Meagher, A.D.; Mohanty, S.; French, D.D.; Lasiter, S.; Khan, B.; et al. Pre-Existing anxiety and depression in injured older adults: An under-recognized comorbidity with major health implications. Ann. Surg. Open 2022, 4, e217. [Google Scholar] [CrossRef]
- Strik, J.J.; Lousberg, R.; Cheriex, E.C.; Honig, A. One year cumulative incidence of depression following myocardial infarction and impact on cardiac outcome. J. Psychosom. Res. 2004, 56, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Spiers, G.F.; Kunonga, T.P.; Stow, D.; Hall, A.; Kingston, A.; Williams, O.; Beyer, F.; Bower, P.; Craig, D.; Todd, C.; et al. Factors associated with unmet need for support to maintain independence in later life: A systematic review of quantitative and qualitative evidence. Age Ageing 2022, 51, 228. [Google Scholar] [CrossRef] [PubMed]
- Sagen-Vik, U.; Finset, A.; Moum, T.; Vik, T.G.; Dammen, T. The longitudinal course of anxiety, depression and apathy through two years after stroke. J. Psychosom. Res. 2022, 162, 111016. [Google Scholar] [CrossRef]
- Su, S.F.; Lin, S.N. Effects of comprehensive geriatric care on depressive symptoms, emergency department visits, re-hospitalization and discharge to the same residence in older persons receiving hip-fracture surgery: A meta-analysis. Int. J. Nurs. Pract. 2022, e13099. [Google Scholar] [CrossRef]
- Kalbouneh, H.M.; Toubasi, A.A.; Albustanji, F.H.; Obaid, Y.Y.; Al-Harasis, L.M. Safety and Efficacy of SSRIs in Improving Poststroke Recovery: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2022, 11, e025868. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.S.; Kimata, R.; Almeida, O.P.; Hankey, G.J. Risk of Fractures in Stroke Patients Treated With a Selective Serotonin Reuptake Inhibitor: A Systematic Review and Meta-Analysis. Stroke 2021, 52, 2802–2808. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, P.A. Management of depression after myocardial infarction. Curr. Cardiol. Rep. 2015, 10, 80. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, R.L.; Yesavage, J.A. Geriatric Depression Scale (GDS). Clin. Gerontol. 1986, 5, 165–173. [Google Scholar]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef]
- Folstein, M.F.; Robins, L.N.; Helzer, J.E. The mini-mental state examination. Arch. Gen. Psychiatry 1983, 40, 812. [Google Scholar] [CrossRef]
- Lübke, N.; Meinck, M.; Von Renteln-Kruse, W. The Barthel Index in geriatrics. A context analysis of the Hamburg Classification Manual. Z. Gerontol. Geriatr. 2004, 37, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Riadi, I.; Kervin, L.; Dhillon, S.; Teo, K.; Churchill, R.; Card, K.G.; Sixsmith, A.; Moreno, S.; Fortuna, K.L.; Torous, J.; et al. Digital interventions for depression and anxiety in older adults: A systematic review of randomised controlled trials. Lancet Healthy Longev. 2022, 3, e558–e571. [Google Scholar] [CrossRef]
- Chang-Quan, H.; Xue-Mei, Z.; Bi-Rong, D.; Zhen-Chan, L.; Ji-Rong, Y.; Qing-Xiu, L. Health status and risk for depression among the elderly: A meta-analysis of published literature. Age Ageing 2010, 39, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Committee on the Mental Health Workforce for Geriatric Populations; Board on Health Care Services; Institute of Medicine. The Mental Health and Substance Use Workforce for Older Adults: In Whose Hands? Eden, J., Maslow, K., Le, M., Blazer, D., Eds.; National Academies Press: Washington, DC, USA, 2012.
- Byers, A.L.; Yaffe, K.; Covinsky, K.E.; Friedman, M.B.; Bruce, M.L. High occurrence of mood and anxiety disorders among older adults: The National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2010, 67, 489–496. [Google Scholar] [CrossRef] [Green Version]
- Conradie, A.; Atherton, J.; Chowdhury, E.; Duong, M.; Schwarz, N.; Worthley, S.; Eccleston, D. Health-Related Quality of Life (HRQoL) and the Effect on Outcome in Patients Presenting with Coronary Artery Disease and Treated with Percutaneous Coronary Intervention (PCI): Differences Noted by Sex and Age. J. Clin. Med. 2022, 11, 5231. [Google Scholar] [CrossRef]
- Amin, M.A.; Ahmed, M.; Nahin, S.; Kakoly, N.S. Assessment of Depression and Anxiety Among Admitted People With Heart Disease Conditions: A Cross-Sectional Hospital-Based Study in a Bangladeshi Population During the COVID-19. Front. Psychiatry 2022, 13, 895224. [Google Scholar] [CrossRef]
- Freedland, K.E.; Rich, M.W.; Skala, J.A.; Carney, R.M.; Dávila-Román, V.G.; Jaffe, A.S. Prevalence of depression in hospitalized patients with congestive heart failure. Psychosom. Med. 2003, 65, 119–128. [Google Scholar] [CrossRef]
- Xiang, X.; Wu, S.; Zuverink, A.; Tomasino, K.N.; An, R.; Himle, J.A. Internet-delivered cognitive behavioral therapies for late-life depressive symptoms: A systematic review and meta-analysis. Aging Ment. Health 2020, 24, 1196–1206. [Google Scholar] [CrossRef]
- Cremers, G.; Taylor, E.; Hodge, L.; Quigley, A. Effectiveness and Acceptability of Low-intensity Psychological Interventions on the Well-being of Older Adults: A Systematic Review. Clin. Gerontol. 2022, 45, 214–234. [Google Scholar] [CrossRef]
- Hollis, C.; Morriss, R.; Martin, J.; Amani, S.; Cotton, R.; Denis, M.; Lewis, S. Technological innovations in mental healthcare: Harnessing the digital revolution. Br. J. Psychiatry 2015, 206, 263–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sixsmith, A. AgeTech: Technology-based solutions for aging societies. In Health of Older Adults: The Canadian Experience; Rootman, I., Edwards, P., Levasseur, M., Grunberg, F., Eds.; Canadian Scholars’ Press: Toronto, ON, Canada, 2021; p. 135. [Google Scholar]
- Seo, E.J.; Son, Y.J. The Prevalence of Cognitive Frailty and Its Association with Sleep duration and Depression Among Older Adults with Heart Failure. Clin. Gerontol. 2022, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.C.; Chen, C.M.; Huang, C.J.; Mau, L.W. Depressive symptoms, chronic medical conditions and functional status: A comparison of urban and rural elders in Taiwan. Int. J. Geriatr. Psychiatry 2005, 20, 635–644. [Google Scholar] [CrossRef]
- Marcus, S.M.; Young, E.A.; Kerber, K.B.; Kornstein, S.; Farabaugh, A.H.; Mitchell, J.; Wisniewski, S.R.; Balasubramani, G.K.; Trivedi, M.H.; Rush, A.J. Gender differences in depression: Findings from the STAR*D study. J. Affect. Disord. 2005, 87, 141–150. [Google Scholar] [CrossRef]
- Pieretti, S.; Di Giannuario, A.; Di Giovannandrea, R.; Marzoli, F.; Piccaro, G.; Minosi, P.; Aloisi, A.M. Gender differences in pain and its relief. Ann. Dell'Ist. Super. Sanita 2016, 52, 184–189. [Google Scholar] [CrossRef]
- Hanania, N.A.; Müllerova, H.; Locantore, N.W.; Vestbo, J.; Watkins, M.L.; Wouters, E.F.; Rennard, S.I.; Sharafkhaneh, A. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study investigators. Determinants of depression in the ECLIPSE chronic obstructive pulmonary disease cohort. Am. J. Respir. Crit. Care Med. 2011, 183, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Chen, H.; Liu, P.; Zou, Z.; Shang, S. Determinants of depressive symptom trajectories in self-reported chronic obstructive pulmonary disease patients. BMC Pulm. Med. 2022, 22, 274. [Google Scholar] [CrossRef]
- Ak, A.K.; Çelebisoy, N.; Özdemir, H.N.; Gökçay, F. Vestibular migraine and persistent postural perceptual dizziness: Handicap, emotional comorbidities, quality of life and personality traits. Clin. Neurol. Neurosurg. 2022, 221, 107409. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
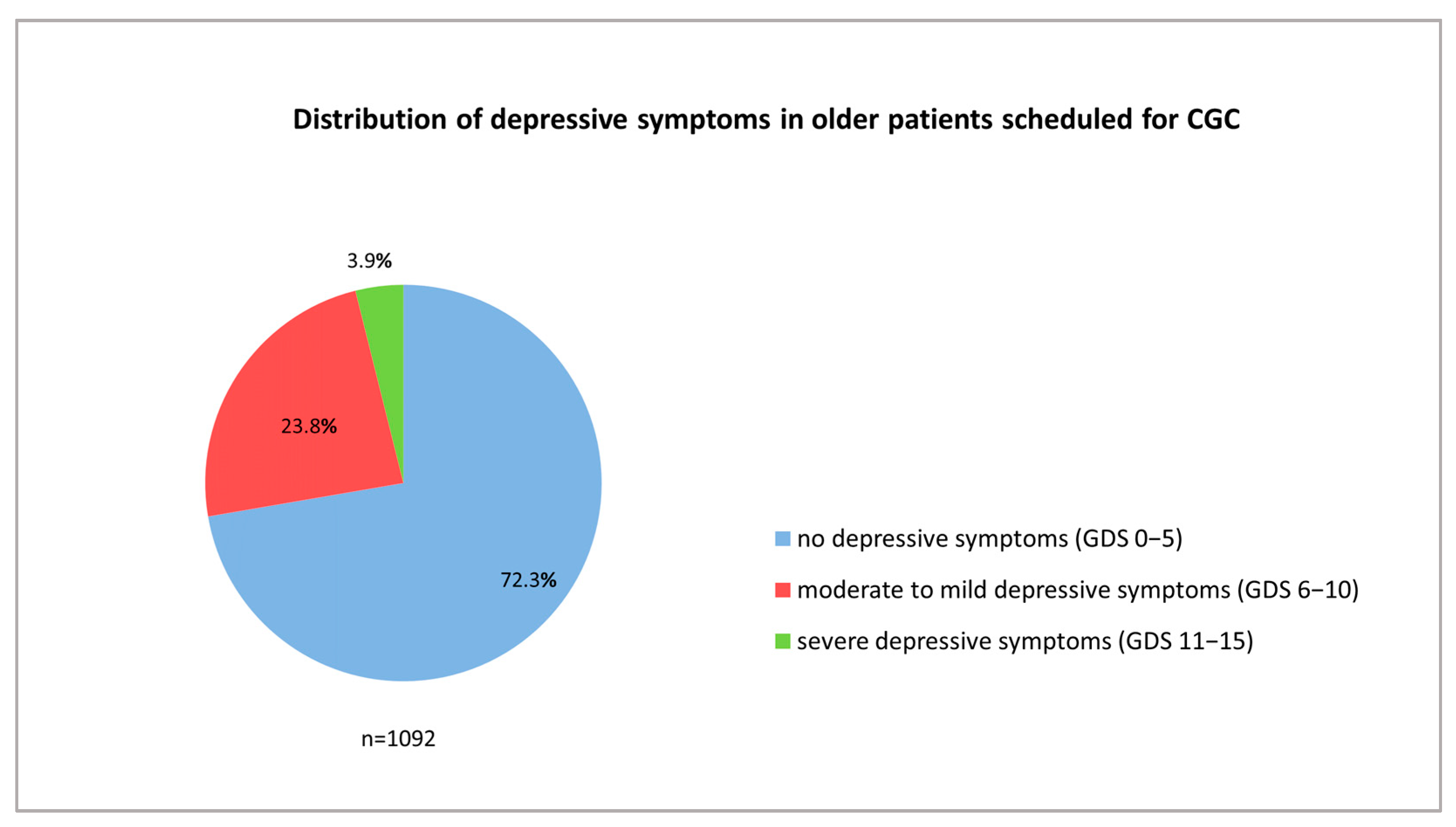
| Severe Depressive Symptoms | Mild Depressive Symptoms | No Depressive Symptoms | |
|---|---|---|---|
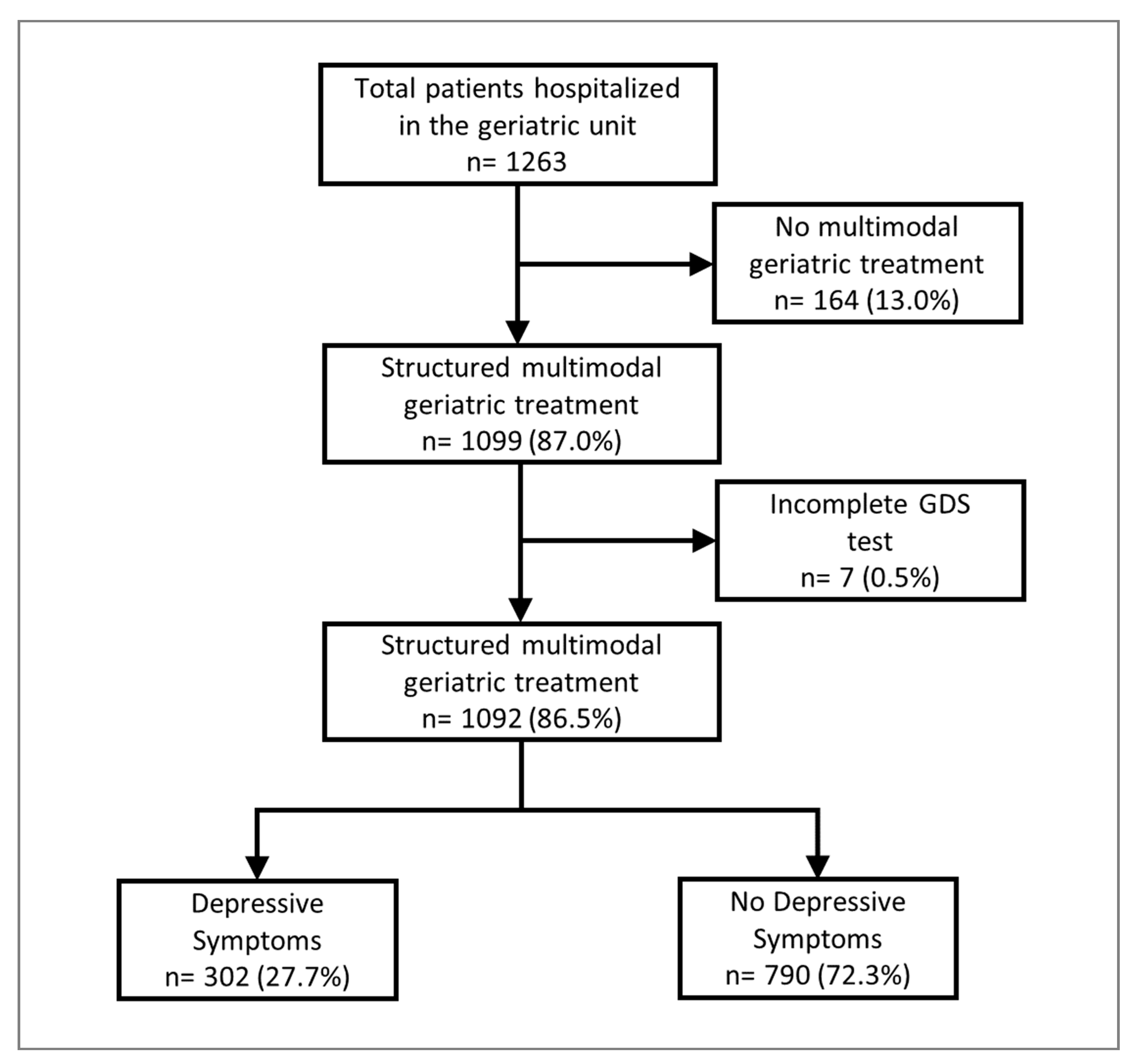
| Patients (n = 1092) | n = 42 (3.9%) | n = 260 (23.8%) | n = 790 (72.3%) |
| Prior to CGC | After CGC | p * | |
|---|---|---|---|
| Patients with depressive symptoms | |||
| Timed Up and Go (median, IQR, years) | 4 (3–5) | 3 (3–4) | <0.001 |
| Barthel Index (median, IQR, years) | 45 (30–55) | 55 (45–75) | <0.001 |
| Tinetti score (median, IQR, years) | 10 (4.75–14.25) | 14 (8–19) | <0.001 |
| Patients without depressive symptoms | |||
| Timed up and go (median, IQR, years) | 4 (3–5) | 3 (2–4) | <0.001 |
| Barthel Index (median, IQR, years) | 45 (30–60) | 55 (30–80) | <0.001 |
| Tinetti score (median, IQR, years) | 12 (6–17) | 15 (2–20) | <0.001 |
| Total Group (n = 1092) | Depressive Symptoms (n = 302) | No Depressive Symptoms (n = 790) | p * | p ** | |
|---|---|---|---|---|---|
| Age (median, IQR, years) | 83.1 (79.1–87.7) | 82.8 (79.0–87.3) | 83.3 (79.0–88.0) | 0.408 | |
| Age ≥ 80 years | 753 (69.0%) | 212 (70.2%) | 541 (68.5%) | 0.608 | |
| Sex | |||||
| Female | 700 (64.1%) | 210 (69.5%) | 490 (62.0%) | 0.024 | 0.046 |
| Male | 392 (35.9%) | 92 (30.5%) | 300 (38.0%) | ||
| Co-morbidities | |||||
| Hypertension | 849 (77.7%) | 246 (81.5%) | 603(76.3%) | 0.074 | |
| Diabetes mellitus | 335 (30.7%) | 99 (32.8%) | 236 (29.9%) | 0.379 | |
| Heart insufficiency | 258 (23.6%) | 79 (26.2%) | 179 (22.7%) | 0.233 | |
| Renal insufficiency | 381 (34.9%) | 118 (39.1%) | 263 (33.3%) | 0.076 | |
| Coronary heart disease | 279 (25.5%) | 78 (25.8%) | 201 (25.4%) | 0.938 | |
| Peripheral artery disease | 59 (5.4%) | 21 (7.0%) | 38 (4.8%) | 0.178 | |
| Atrial fibrillation | 387 (35.4%) | 116 (38.4%) | 271 (34.3%) | 0.204 | |
| Chronic obstructive pulmonary disease | 108 (9.9%) | 45 (14.9%) | 63 (8.0%) | 0.001 | <0.001 |
| Dementia | 225 (20.6%) | 48 (15.9%) | 177 (22.4%) | 0.019 | 0.062 |
| Parkinson’s disease | 62 (5.7%) | 16 (5.3%) | 46 (5.8%) | 0.884 | |
| Previous stroke | 89 (8.2%) | 27 (8.9%) | 62 (7.8%) | 0.539 | |
| Current fracture | 299 (27.4) | 83 (27.5%) | 216 (27.3%) | >0.999 | |
| Osteoporosis | 127 (11.6%) | 39 (12.9%) | 88 (11.1%) | 0.401 | |
| Vitamin B deficiency | 484 (44.3%) | 131 (43.4%) | 353 (44.7%) | 0.734 | |
| Short term adverse events while hospitalized | |||||
| Diffuse pain | 292 (26.7%) | 85 (28.1%) | 207 (26.2%) | 0.541 | |
| Delirium | 57 (5.2%) | 11 (3.6%) | 46 (5.8%) | 0.172 | |
| Pneumonia | 64 (5.9%) | 23 (7.6%) | 41 (5.2%) | 0.149 | |
| Urinary tract infection | 158 (14.5%) | 42 (13.9%) | 116 (14.7%) | 0.774 | |
| Dizziness | 79 (7.2%) | 30 (9.9%) | 49 (6.2%) | 0.037 | 0.184 |
| Deep vein thrombosis | 5 (0.5%) | 1 (0.3%) | 4 (0.5%) | 0.999 | |
| Pulmonary embolism | 4 (0.4%) | 0 (0.0%) | 4 (0.5%) | 0.580 | |
| Electrolyte imbalance | 405 (37.1%) | 120 (39.7%) | 285 (36.1%) | 0.264 | |
| Hypokalemia | 350 (32.1%) | 108 (35.8%) | 242 (30.6%) | 0.111 | |
| Hyponatremia | 100 (9.2%) | 27 (8.9%) | 73 (9.2%) | 0.999 | |
| Functional assessment on admission | |||||
| Timed Up and Go (median, IQR; mean, SD) (n = 1063) | 4 (3–5); 3.9 ± 1.1 | 4 (3–5); 4.1 ± 1.0 | 4 (3–5); 3.8 ± 1.1 | 0.001 | |
| Barthel Index (median, IQR) (n = 1029) | 45 (30–60) | 45 (30–55) | 45 (30–60) | 0.392 | |
| Tinetti Geriatric Assessment (median, IQR) (n = 994) | 12 (5–17) | 10 (4.75–14.25) | 12 (6–17) | 0.001 | |
| MMSE (median, IQR) (n = 812) | 26 (21–28) | 26 (21–27) | 26 (21–28) | 0.290 | |
| Discharge type | |||||
| In-home care | 1035 (94.8%) | 282 (93.4%) | 753 (95.3%) | 0.223 | |
| Referral to other department | 15 (1.4%) | 5 (1.7.0%) | 10 (1.3%) | 0.537 | |
| Length of hospital stay for patients with CGC (median, IQR, days) (n = 1029) | 17 (16–19) | 17 (16–19.25) | 17 (16–19) | 0. 147 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niemöller, U.; Arnold, A.; Stein, T.; Juenemann, M.; Farzat, M.; Erkapic, D.; Rosenbauer, J.; Kostev, K.; Meyer, M.; Tanislav, C. Comprehensive Geriatric Care in Older Hospitalized Patients with Depressive Symptoms. Geriatrics 2023, 8, 37. https://doi.org/10.3390/geriatrics8020037
Niemöller U, Arnold A, Stein T, Juenemann M, Farzat M, Erkapic D, Rosenbauer J, Kostev K, Meyer M, Tanislav C. Comprehensive Geriatric Care in Older Hospitalized Patients with Depressive Symptoms. Geriatrics. 2023; 8(2):37. https://doi.org/10.3390/geriatrics8020037
Chicago/Turabian StyleNiemöller, Ulrich, Andreas Arnold, Thomas Stein, Martin Juenemann, Mahmoud Farzat, Damir Erkapic, Josef Rosenbauer, Karel Kostev, Marco Meyer, and Christian Tanislav. 2023. "Comprehensive Geriatric Care in Older Hospitalized Patients with Depressive Symptoms" Geriatrics 8, no. 2: 37. https://doi.org/10.3390/geriatrics8020037