
Feasibility of a 12-Month Follow-Up in Swiss Older Adults after Post-Acute Care in Nursing Homes—A Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting and Participants
2.3. Baseline Data
2.4. Telephone Interview
2.5. Statistical Analysis
3. Results
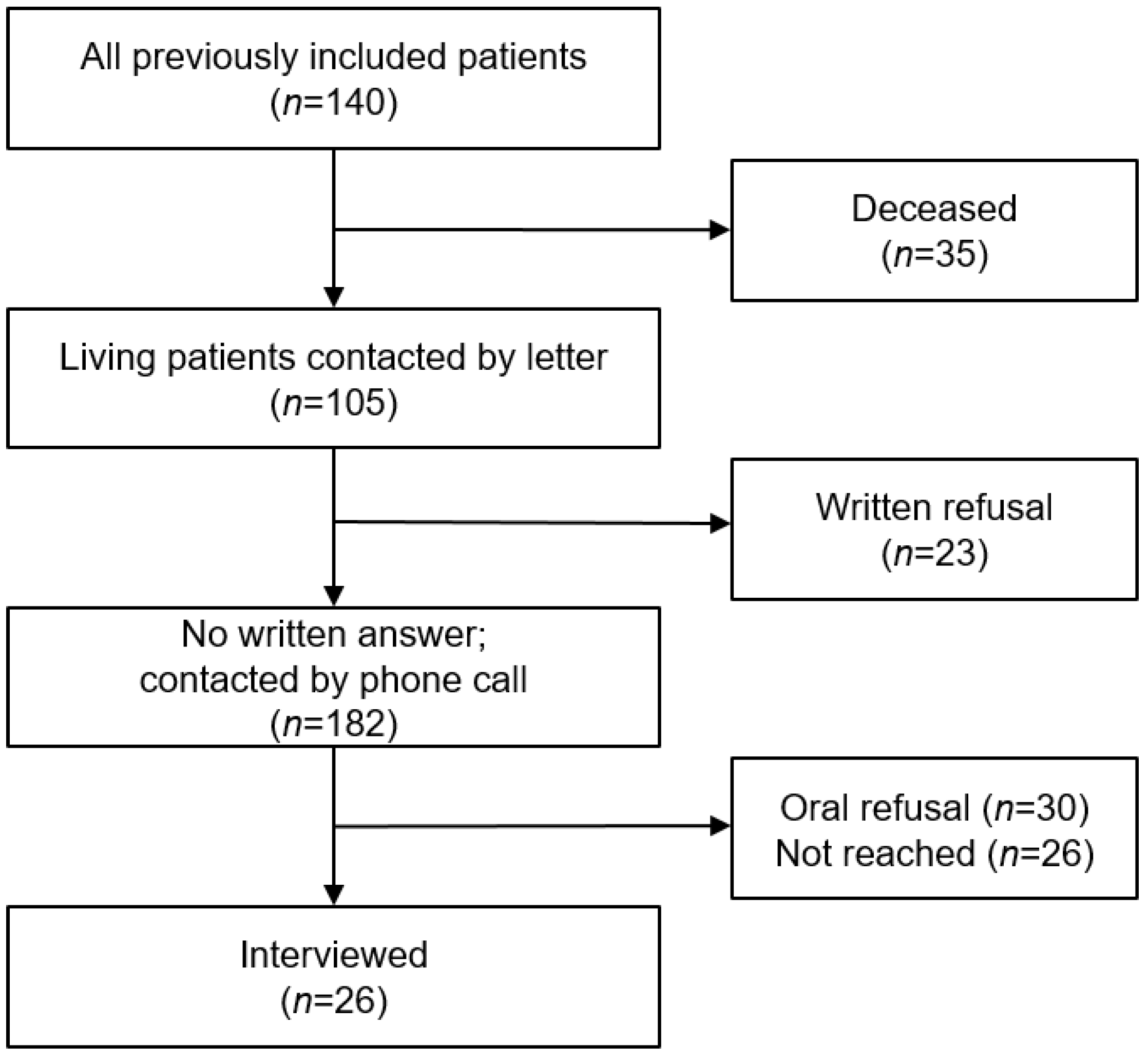
3.1. Participants
3.2. Participation Factors
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chong, E.; Ho, E.; Baldevarona-Llego, J.; Chan, M.; Wu, L.; Tay, L.; Ding, Y.Y.; Lim, W.S. Frailty in Hospitalized Older Adults: Comparing Different Frailty Measures in Predicting Short- and Long-term Patient Outcomes. J. Am. Med. Dir. Assoc. 2018, 19, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Fimognari, F.L.; Pierantozzi, A.; De Alfieri, W.; Salani, B.; Zuccaro, S.M.; Arone, A.; Palleschi, G.; Palleschi, L. The Severity of Acute Illness and Functional Trajectories in Hospitalized Older Medical Patients. J. Gerontol. Ser. A 2016, 72, 102–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, T.M.; Allore, H.; Gahbauer, E.A.; Murphy, T.E. Change in Disability After Hospitalization or Restricted Activity in Older Persons. JAMA 2010, 304, 1919–1928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, R.H.; Zorzitto, M.L. Placement problem: Diagnosis, disease or term of denigration? Can. Med. Assoc. J. 1983, 129, 331–334. [Google Scholar] [PubMed]
- Lavis, J.N.; Anderson, G.M. Appropriateness in health care delivery: Definitions, measurement and policy implications. Can. Med. Assoc. J. 1996, 154, 321–328. [Google Scholar]
- Mabire, C.; Dwyer, A.; Garnier, A.; Pellet, J. Meta-analysis of the effectiveness of nursing discharge planning interventions for older inpatients discharged home. J. Adv. Nurs. 2017, 74, 788–799. [Google Scholar] [CrossRef]
- Koné, I.; Zimmermann, B.; Wangmo, T.; Richner, S.; Weber, M.; Elger, B. Hospital discharge of patients with ongoing care needs: A cross-sectional study using data from a city hospital under SwissDRG. Swiss Med. Wkly. 2018, 148, w14575. [Google Scholar]
- Manville, M.; Klein, M.C.; Bainbridge, L. Improved outcomes for elderly patients who received care on a transitional care unit. Can. Fam. Physician 2014, 60, e263–e271. [Google Scholar]
- Thalmann, M.; Tröster, T.; Fischer, K.; Bieri-Brüning, G.; Patrick, B.; Bischoff-Ferrari, H.A.; Gagesch, M. Do older adults benefit from post-acute care following hospitalisation? A prospective cohort study at three Swiss nursing homes. Swiss Med. Wkly. 2020, 150, w20198. [Google Scholar] [CrossRef] [Green Version]
- Buurman, B.M.; Parlevliet, J.L.; Allore, H.G.; Blok, W.; van Deelen, B.A.; van Charante, E.P.M.; de Haan, R.J.; de Rooij, S.E. Comprehensive Geriatric Assessment and Transitional Care in Acutely Hospitalized Patients: The Transitional Care Bridge Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 302–309. [Google Scholar] [CrossRef] [Green Version]
- Everink, I.H.J.; Van Haastregt, J.C.M.; Evers, S.M.A.A.; Kempen, G.I.J.M.; Schols, J.M.G.A. An economic evaluation of an integrated care pathway in geriatric rehabilitation for older patients with complex health problems. PLoS ONE 2018, 13, e0191851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritt, M.; Ritt, J.I.; Sieber, C.C.; Gaßmann, K.-G. Comparing the predictive accuracy of frailty, comorbidity, and disability for mortality: A 1-year follow-up in patients hospitalized in geriatric wards. Clin. Interv. Aging 2017, 12, 293–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilotto, A.; Rengo, F.; Marchionni, N.; Sancarlo, D.; Fontana, A.; Panza, F.; Ferrucci, L.; FIRI-SIGG Study Group. Comparing the prognostic accuracy for all-cause mortality of frailty instruments: A multicentre 1-year follow-up in hospitalized older patients. PLoS ONE 2012, 7, e29090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mody, L.; Miller, D.K.; McGloin, J.M.; Freeman, M.; Marcantonio, E.R.; Magaziner, J.; Studenski, S. Recruitment and Retention of Older Adults in Aging Research. J. Am. Geriatr. Soc. 2008, 56, 2340–2348. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.; Dyson, E. Recruitment of frail older people to research: Lessons learnt through experience. J. Adv. Nurs. 2001, 36, 643–651. [Google Scholar] [CrossRef]
- Provencher, V.; Ben Mortenson, W.; Tanguay-Garneau, L.; Bélanger, K.; Dagenais, M. Challenges and strategies pertaining to recruitment and retention of frail elderly in research studies: A systematic review. Arch. Gerontol. Geriatr. 2014, 59, 18–24. [Google Scholar] [CrossRef]
- Fompeyrine, C.; Abderhalden, L.A.; Mantegazza, N.; Hofstetter, N.; Bieri-Brüning, G.; Bischoff-Ferrari, H.A.; Gagesch, M. Frailty is associated with increased mortality in older adults 12 months after discharge from post-acute care in Swiss nursing homes. J. Frailty Aging 2021, 10, 233–236. [Google Scholar]
- Bieri-Brüning, G. Akut- und Übergangspflege—Bindeglied Zwischen Spital und Zuhause. 2017: Zürcher Geriatrieforum Waid. Available online: https://docplayer.org/58854934-Zuercher-geriatrieforum-waid.html (accessed on 28 February 2023).
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Dick, J.P.; Guiloff, R.J.; Stewart, A.; Blackstock, J.; Bielawska, C.; A Paul, E.; Marsden, C.D. Mini-mental state examination in neurological patients. J. Neurol. Neurosurg. Psychiatry 1984, 47, 496–499. [Google Scholar] [CrossRef] [Green Version]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged. the Index of Adl: A Standardized Measure of Biological and Psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ortuno, R.; Walsh, C.D.; A Lawlor, B.; Kenny, R.A. A Frailty Instrument for primary care: Findings from the Survey of Health, Ageing and Retirement in Europe (SHARE). BMC Geriatr. 2010, 10, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowsher, J.; Bramlett, M.; Burnside, I.M.; Gueldner, S.H. Methodological considerations in the study of frail elderly people. J. Adv. Nurs. 1993, 18, 873–879. [Google Scholar] [CrossRef]
- Ständige Wohnbevölkerung nach Alter, Geschlecht und Staatsangehörigkeitskategorie, 2010–2021. Available online: https://www.bfs.admin.ch/asset/de/je-d-01.02.03.02 (accessed on 28 February 2023).
- Todesfälle nach Alter und Geschlecht, 1970–2021. Available online: https://www.bfs.admin.ch/bfs/de/home/statistiken/bevoelkerung/geburten-todesfaelle/todesfaelle.assetdetail.22786986.html (accessed on 28 February 2023).
- Hakkarainen, T.W.; Arbabi, S.; Willis, M.M.; Davidson, G.H.; Flum, D.R. Outcomes of Patients Discharged to Skilled Nursing Facilities After Acute Care Hospitalizations. Ann. Surg. 2016, 263, 280–285. [Google Scholar] [CrossRef] [Green Version]
- Carter, W.B.; Elward, K.; Malmgren, J.; Martin, M.L.; Larson, E. Participation of Older Adults in Health Programs and Research: A Critical Review of the Literature. Gerontologist 1991, 31, 584–592. [Google Scholar] [CrossRef]
- Forsat, N.D.; Palmowski, A.; Palmowski, Y.; Boers, M.; Buttgereit, F. Recruitment and Retention of Older People in Clinical Research: A Systematic Literature Review. J. Am. Geriatr. Soc. 2020, 68, 2955–2963. [Google Scholar] [CrossRef]
- Hall, S.; Longhurst, S.; Higginson, I.J. Challenges to conducting research with older people living in nursing homes. BMC Geriatr. 2009, 9, 38. [Google Scholar] [CrossRef] [Green Version]
- Carstensen, L.L.; Hartel, C.R. When I’m 64; National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Felsen, C.B.; Shaw, E.K.; Ferrante, J.M.; Lacroix, L.J.; Crabtree, B.F. Strategies for In-Person Recruitment: Lessons Learned from a New Jersey Primary Care Research Network (NJPCRN) Study. J. Am. Board Fam. Med. 2010, 23, 523–533. [Google Scholar] [CrossRef] [Green Version]
- Lewicki, R.J.; Tomlinson, E.C.; Gillespie, N. Models of Interpersonal Trust Development: Theoretical Approaches, Empirical Evidence, and Future Directions. J. Manag. 2006, 32, 991–1022. [Google Scholar] [CrossRef]


{kind=link}
| Overall | Deceased | Not Reached | Interviewed | Declined | p Value a | |
|---|---|---|---|---|---|---|
| (n = 140) | (n = 35) | (n = 26) | (n = 26) | (n = 53) | ||
| Age, mean (SD) | 84.1 (8.57) | 87.3 (7.63) | 81.8 (9.34) | 85.5 (7.60) | 82.5 (8.66) | 0.13 |
| Female, n (%) | 88 (37.1%) | 19 (54.3%) | 13 (50.0%) | 20 (76.9%) | 36 (67.9%) | 0.57 |
| Living Status, n (%) | ||||||
| alone | 87 (62.1%) | 16 (45.7%) | 21 (80.8%) | 16 (61.5%) | 34 (64.2%) | 0.17 |
| family/friend | 8 (5.7%) | 3 (8.6%) | 1 (3.8%) | 3 (11.5%) | 1 (1.9%) | |
| spouse | 44 (31.4%) | 15 (42.9%) | 4 (15.4%) | 7 (26.9%) | 18 (34.0%) | |
| MMSE, mean (SD) b | 24.0 (4.46) | 23.6 (4.54) | 23.8 (4.73) | 26.0 (3.92) | 23.5 (4.40) | 0.015 |
| Frailty Status b | ||||||
| robust | 6 (4.3%) | 0 (0%) | 3 (11.5%) | 0 (0%) | 3 (5.7%) | 0.33 |
| pre-frail | 52 (37.1%) | 6 (17%) | 13 (50.0%) | 10 (38.5%) | 23 (43.4%) | |
| frail | 77 (55.0%) | 27 (77.1%) | 9 (34.6%) | 16 (61.5%) | 25 (47.2%) | |
| Barthel-Index, mean (SD) | 63.2 (20.0) | 63.2 (20.0) | 66.7 (22.7) | 61.9 (20.6) | 64.9 (18.6) | 0.52 |
| Univariate Model (n = 79) | Multivariate Model a (n = 77 b) | |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| Age | 1.05 (0.98, 1.12) | 1.06 (0.98, 1.14) |
| Men (Women as reference) | 0.64 (0.22, 1.87) | 0.66 (0.18, 2.42) |
| Living Situation Home alone (Reference) | 1.0 | 1.0 |
| Family/Friend | 6.38 (0.61, 66.17) | 9.74 (0.49, 194.56) |
| Spouse | 0.83 (0.29, 2.38) | 1.39 (0.38, 5.1) |
| MMSE (one point increase) | 1.18 (1.03, 1.37) | 1.25 (1.06, 1.48) |
| Frailty Status c (robust/pre-frail as ref.) | 1.0 | 1.0 |
| Frail | 1.67 (0.64, 4.36) | 1.17 (0.39, 3.55) |
| Barthel-Index (one point increase) | 0.99 (0.97, 1.02) | 0.99 (0.96, 1.02) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gagesch, M.; Hüni, A.; Geschwindner, H.; Abderhalden, L.A.; Lang, W.; Bieri-Brüning, G.; Bischoff-Ferrari, H.A. Feasibility of a 12-Month Follow-Up in Swiss Older Adults after Post-Acute Care in Nursing Homes—A Pilot Study. Geriatrics 2023, 8, 35. https://doi.org/10.3390/geriatrics8020035
Gagesch M, Hüni A, Geschwindner H, Abderhalden LA, Lang W, Bieri-Brüning G, Bischoff-Ferrari HA. Feasibility of a 12-Month Follow-Up in Swiss Older Adults after Post-Acute Care in Nursing Homes—A Pilot Study. Geriatrics. 2023; 8(2):35. https://doi.org/10.3390/geriatrics8020035
Chicago/Turabian StyleGagesch, Michael, Andreas Hüni, Heike Geschwindner, Lauren A. Abderhalden, Wei Lang, Gaby Bieri-Brüning, and Heike A. Bischoff-Ferrari. 2023. "Feasibility of a 12-Month Follow-Up in Swiss Older Adults after Post-Acute Care in Nursing Homes—A Pilot Study" Geriatrics 8, no. 2: 35. https://doi.org/10.3390/geriatrics8020035