
Exploring Telehealth Readiness in a Resource Limited Setting: Digital and Health Literacy among Older People in Rural India (DAHLIA)

Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Setting
2.2. Participant Recruitment and Inclusion
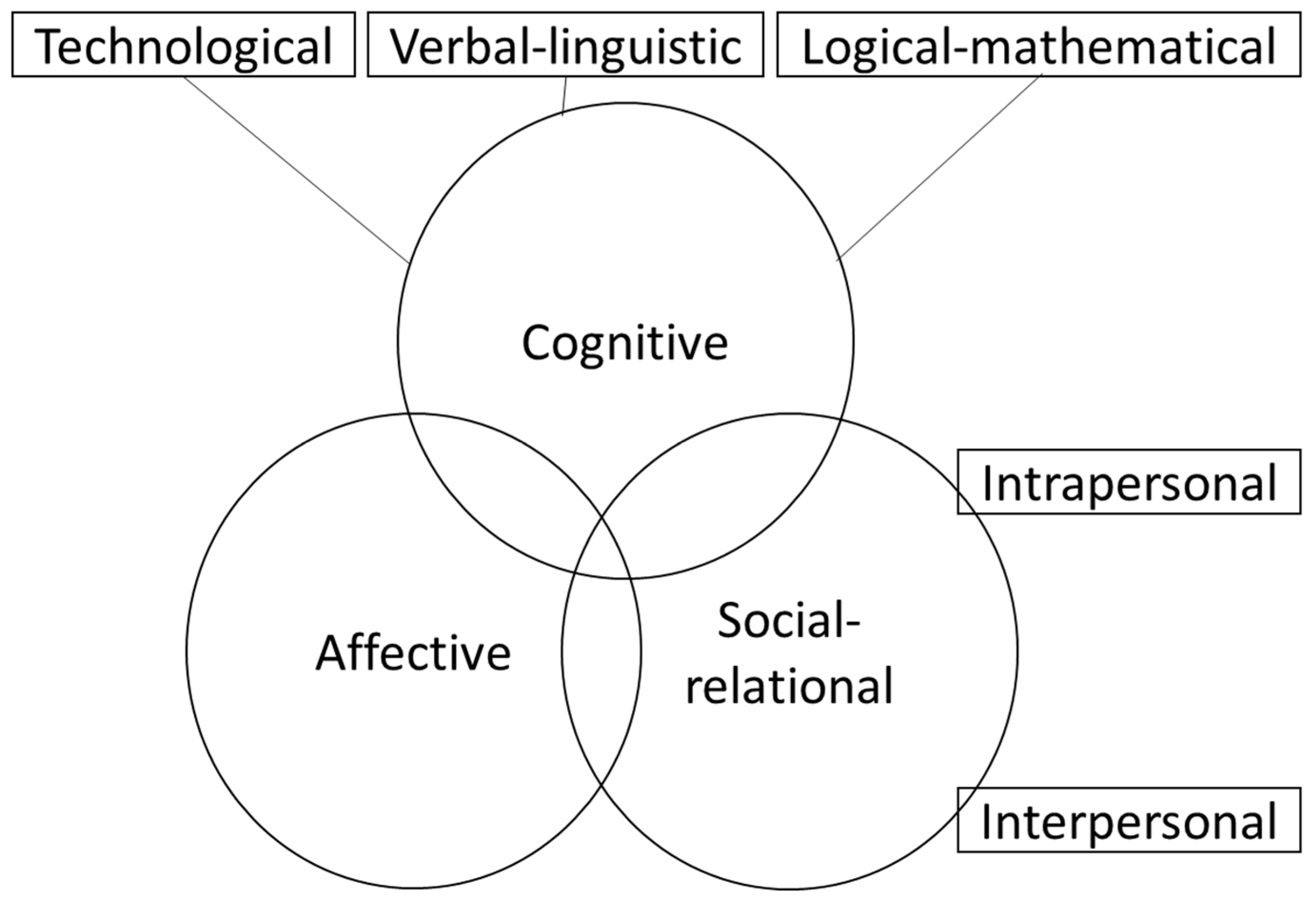
2.3. Digital Literacy Model
2.4. Quantitative Data Collection
2.5. Qualitative Data Collection
2.6. Data Analyses
3. Results
3.1. Quantitative Analysis
3.2. Qualitative Analysis
3.2.1. Health Behaviours and Access to Healthcare
The Building of Health Beliefs and Pathways to Health
“We eat healthy food like Ragi balls. We follow an active lifestyle. We go about looking after our livestock and toiling in the fields every day”… Patient 4, FG1.
“Our children tell us about eating habits and other lifestyle modifications. Sometimes we learn some things from the television”... Patient 1, FG3.
“When we fall sick, we go to doctor and they advise us to eat healthy food and do regular exercise”… Patient 22, CF4.
“We get to know about them from our friends and neighbours”… Patient 5, FG2.
“There is one government run hospital for every 10 villages which has a doctor and a nurse. They refer us to the tertiary care centres in cities for any major health issues”… Patient 14, FG2.
To get my FBS done I have to be on fasting 8 h and have to travel for four hours to reach hospital. The wait at the hospital OPD [out-patient department] increases the fasting duration to up to 10–12 h straight. In such cases, getting an appointment before coming to the hospital will be helpful”... Patient 3, FG2.
3.2.2. Digital Literacy
Cognitive “Limited Exposure, Experiences and Efficacy with Technology”
“Our children have mobile phones. I know how to talk using a phone, but I don’t know to make a call or use the keypad for messages”... Patient 4, FG3.
“We use internet to get health information instead of traveling for second opinion”… Patient 15, CF4.
“My son will browse the internet for information regarding health issues and explain it to me”… Patient 2, FG1.
3.3. Social Relational Domain “It Takes a Village to Raise an Elder”
“At home our families help us in taking care of our health. But they are busy today; hence we neighbours came together to the hospital”… Patient 6 & 5, FG3.
“Our friends and neighbours tell us about the health complications. They tell us about their experience regarding their surgeries, their admissions and what the doctor advised to prevent the complications”… Patient 25, CF4.
“My granddaughter is educated and sending messages will be helpful for me since I can’t read messages”… Patient 5, SG3.
“Sending a reminder message to my son’s phone regarding my appointment will be very helpful”… Patient 3, SG.
“I cannot ask someone to read it out to me all the time. They might get irritated or annoyed after a couple of times. So we prefer calling [the hospital] sometimes”… Patient 7, SG4.
3.4. Affective Domain—Lack of Confidence with Using Technology
“If you can’t get it, you can’t use it”
“We don’t know how to read”... Patients 28 & 30, CF4.
“I know how to read and text but I can’t read because I can’t see. If my vision was good then I could read and text but now I can’t”… Patient 7, FG4.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. World Report on Ageing and Health; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- Chatterji, S.; Kowal, P.; Mathers, C.; Naidoo, N.; Verdes, E.; Smith, J.P.; Suzman, R. The Health of Aging Populations in China and India. Health Aff. 2008, 27, 1052–1063. [Google Scholar] [CrossRef] [PubMed]
- Robbins, T.D.; Keung, S.N.L.C.; Arvanitis, T.N. E-health for active ageing; A systematic review. Maturitas 2018, 114, 34–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.T.; Hamid, F.; Pati, S.; Atun, R.; Millett, C. Impact of Noncommunicable Disease Multimorbidity on Healthcare Utilisation and Out-Of-Pocket Expenditures in Middle-Income Countries: Cross Sectional Analysis. PLoS ONE 2015, 10, e0127199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peek, S.T.M.; Wouters, E.J.M.; van Hoof, J.; Luijkx, K.G.; Boeije, H.R.; Vrijhoef, H.J.M. Factors influencing acceptance of technology for aging in place: A systematic review. Int. J. Med. Inform. 2014, 83, 235–248. [Google Scholar] [CrossRef] [Green Version]
- Bloom, D.E.; Luca, D.L. Chapter 1—The Global Demography of Aging: Facts, Explanations, Future. In Handbook of the Economics of Population Aging; Piggott, J., Woodland, A., Eds.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 3–56. [Google Scholar]
- Mini, G.; Thankappan, K.R. Pattern, correlates and implications of non-communicable disease multimorbidity among older adults in selected Indian states: A cross-sectional study. BMJ Open 2017, 7, e013529. [Google Scholar] [CrossRef]
- Kankeu, H.T.; Saksena, P.; Xu, K.; Evans, D.B. The financial burden from non-communicable diseases in low- and middle-income countries: A literature review. Health Res. Policy Syst. 2013, 11, 31. [Google Scholar] [CrossRef]
- Grimes, C.E.; Bowman, K.G.; Dodgion, C.M.; Lavy, C.B.D. Systematic Review of Barriers to Surgical Care in Low-Income and Middle-Income Countries. World J. Surg. 2011, 35, 941–950. [Google Scholar] [CrossRef]
- United Nations Population Fund. Caring for Our Elders: Early Responses. India Ageing Report—2017; United Nations Population Fund (UNFPA): New Dehli, India, 2017. [Google Scholar]
- Portz, J.D.; Miller, A.; Foster, B.; Laudeman, L. Persuasive features in health information technology interventions for older adults with chronic diseases: A systematic review. Health Technol. 2016, 6, 89–99. [Google Scholar] [CrossRef]
- Bujnowska-Fedak, M.M.; Grata-Borkowska, U. Use of Telemedicine-Based Care for the Aging and Elderly: Promises and Pitfalls. Smart Homecare Technol. TeleHealth 2015, 3, 91. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Alcalá, C.I.; Pliego-Pastrana, P.; Rosales-Lagarde, A.; Lopez-Noguerola, J.S.; Molina-Trinidad, E.M. Information and Communication Technologies in the Care of the Elderly: Systematic Review of Applications Aimed at Patients with Dementia and Caregivers. JMIR Rehabil. Assist. Technol. 2016, 3, e6. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Stroulia, E.; Nikolaidis, I.; Miguel-Cruz, A.; Rincón, A.M.R. Smart homes and home health monitoring technologies for older adults: A systematic review. Int. J. Med. Inform. 2016, 91, 44–59. [Google Scholar] [CrossRef]
- Gell, N.M.; Rosenberg, D.E.; Demiris, G.; Lacroix, A.Z.; Patel, K.V. Patterns of Technology Use Among Older Adults with and Without Disabilities. Gerontologist 2013, 55, 412–421. [Google Scholar] [CrossRef]
- Marschollek, M.; Mix, S.; Wolf, K.-H.; Effertz, B.; Haux, R.; Steinhagen-Thiessen, E. Ict-Based Health Information Services for Elderly People: Past Experiences, Current Trends, and Future Strategies. Med. Inform. Internet Med. 2007, 32, 251–261. [Google Scholar] [CrossRef]
- Cimperman, M.; Brenčič, M.M.; Trkman, P.; Stanonik, M.D.L. Older Adults’ Perceptions of Home Telehealth Services. Telemed. eHealth 2013, 19, 786–790. [Google Scholar] [CrossRef]
- Desai, G.; Singh, S.; Chatterjee, P.; Dey, A. Mobile Health Initiatives in Geriatrics: The Needs, Attitudes and Expectations of Older Indians. Innov. Aging 2017, 1, 1190–1191. [Google Scholar] [CrossRef] [Green Version]
- Tennant, B.; Stellefson, M.; Dodd, V.; Chaney, B.; Chaney, D.; Paige, S.; Alber, J. eHealth Literacy and Web 2.0 Health Information Seeking Behaviors Among Baby Boomers and Older Adults. J. Med. Internet Res. 2015, 17, e70. [Google Scholar] [CrossRef]
- Norman, C.D.; Skinner, H.A. eHealth Literacy: Essential Skills for Consumer Health in a Networked World. J. Med. Internet Res. 2006, 8, e9. [Google Scholar] [CrossRef]
- Chesser, A.K.; Woods, N.K.; Smothers, K.; Rogers, N. Health Literacy and Older Adults: A Systematic Review. Gerontol. Geriatr. Med. 2016, 2. [Google Scholar] [CrossRef] [Green Version]
- Martin, A. Digeulit–a European Framework for Digital Literacy: A Progress Report. J. Eliteracy 2005, 2, 130–136. [Google Scholar]
- Heart, T.; Kalderon, E. Older Adults: Are They Ready to Adopt Health-Related Ict? Int. J. Med. Inform. 2011, 82, e209–e231. [Google Scholar] [CrossRef]
- Olson, K.E.; O’Brien, M.A.; Rogers, W.A.; Charness, N. Diffusion of Technology: Frequency of use for Younger and Older Adults. Ageing Int. 2011, 36, 123–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, H.S.; Shillair, R.; Cotton, S.R. Social Support and “Playing Around”: An Examination of How Older Adults Acquire Digital Literacy with Tablet Computers. J. Appl. Gerontol. 2015, 36, 29–55. [Google Scholar] [CrossRef] [PubMed]
- Cartelli, A. Theory and Practice in Digital Competence Assessment. Int. J. Digit. Lit. Digit. Competence 2010, 1, 561–574. [Google Scholar] [CrossRef]
- Antonio, A.; Tuffley, D. Bridging the Age-Based Digital Divide. Int. J. Digit. Lit. Digit. Competence 2015, 6, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.; Coughlin, J.F. Perspective: Older Adults’ Adoption of Technology: An Integrated Approach to Identifying Determinants and Barriers. J. Prod. Innov. Manag. 2015, 32, 747–759. [Google Scholar] [CrossRef]
- Klimova, B.; Poulova, P. Older People and Technology Acceptance. In Proceedings of the Human Aspects of IT for the Aged Population, Acceptance, Communication and Participation, Las Vegas, NV, USA, 15–20 July 2018. [Google Scholar]
- Ahmed, H.; Haq, I.; Rahman, A.; Tonner, E.; Abbass, R.; Sharif, F.; Asinger, S.; Sbai, M. Older people and technology: Time to smarten up our act. Future Healthc. J. 2021, 8, e166–e169. [Google Scholar] [CrossRef]
- Friemel, T. The digital divide has grown old: Determinants of a digital divide among seniors. New Media Soc. 2014, 18, 313–331. [Google Scholar] [CrossRef]
- Thielke, S.; Harniss, M.; Thompson, H.; Patel, S.; Demiris, G.; Johnson, K. Maslow’s Hierarchy of Human Needs and the Adoption of Health-Related Technologies for Older Adults. Ageing Int. 2011, 37, 470–488. [Google Scholar] [CrossRef]
- Price-Haywood, E.G.; Harden-Barrios, J.; Ulep, R.; Luo, Q. Ehealth Literacy: Patient Engagement in Identifying Strategies to Encour-age Use of Patient Portals among Older Adults. Popul. Health Manag. 2017, 20, 486–494. [Google Scholar] [CrossRef]
- Norman, C.D.; Skinner, H.A. Eheals: The Ehealth Literacy Scale. J. Med. Internet Res. 2006, 8, e27. [Google Scholar] [CrossRef] [Green Version]
- Chew, L.D.; Griffin, J.M.; Partin, M.R.; Noorbaloochi, S.; Grill, J.P.; Snyder, A.; Bradley, K.A.; Nugent, S.M.; Baines, A.D.; VanRyn, M. Validation of Screening Questions for Limited Health Literacy in a Large VA Outpatient Population. J. Gen. Intern. Med. 2008, 23, 561–566. [Google Scholar] [CrossRef] [Green Version]
- Chew, L.D.; Bradley, K.A.; Boyko, E.J. Brief questions to identify patients with inadequate health literacy. Health 2004, 11, 12. [Google Scholar]
- Nahar, P.; Kannuri, N.K.; Mikkilineni, S.; Murthy, G.; Phillimore, P. mHealth and the management of chronic conditions in rural areas: A note of caution from southern India. Anthr. Med. 2017, 24, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Neter, E.; Brainin, E. eHealth Literacy: Extending the Digital Divide to the Realm of Health Information. J. Med. Internet Res. 2012, 14, e19. [Google Scholar] [CrossRef]
- Schreurs, K.; Quan-Haase, A.; Martin, K. Problematizing the Digital Literacy Paradox in the Context of Older Adults’ ICT Use: Aging, Media Discourse, and Self-Determination. Can. J. Commun. 2017, 42, 359–377. [Google Scholar] [CrossRef] [Green Version]
- Jennett, P.A.; Affleck Hall, L.; Hailey, D.; Ohinmaa, A.; Anderson, C.; Thomas, R.; Young, B.; Lorenzetti, D.; Scott, R.E. The Socio-Economic Impact of Telehealth: A Systematic Review. J. Telemed. Telecare 2003, 9, 311–320. [Google Scholar] [CrossRef]
- Wade, V.A.; Karnon, J.; Elshaug, A.G.; Hiller, J.E. A systematic review of economic analyses of telehealth services using real time video communication. BMC Health Serv. Res. 2010, 10, 233. [Google Scholar] [CrossRef] [Green Version]
- Speyer, R.; Denman, D.; Wilkes-Gillan, S.; Chen, Y.; Bogaardt, H.; Kim, J.; Heckathorn, D.; Cordier, R. Effects of telehealth by allied health professionals and nurses in rural and remote areas: A systematic review and meta-analysis. J. Rehabil. Med. 2018, 50, 225–235. [Google Scholar] [CrossRef] [Green Version]
- McLendon, S.F. Interactive Video Telehealth Models to Improve Access to Diabetes Specialty Care and Education in the Rural Setting: A Systematic Review. Diabetes Spectr. 2017, 30, 124–136. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| n | % | |
|---|---|---|
| Age (median (IQR), years | 71 (68–78) | |
| Gender | ||
| Male | 94 | 62.7 |
| Female | 56 | 37.3 |
| Highest level of education | ||
| None | 49 | 32.7 |
| Primary | 52 | 34.7 |
| Secondary | 29 | 19.3 |
| Post-secondary | 20 | 19.3 |
| Participant self-reported presenting health conditions | ||
| Diabetes mellitus | 45 | 30.0 |
| Hypertension | 27 | 18.0 |
| Fatigue | 13 | 8.7 |
| Eye/sight related condition | 22 | 14.7 |
| Myalgia/ joint pain/muscle pain | 15 | 10.0 |
| Pain, other parts of body | 15 | 10.0 |
| Loss of appetite | 4 | 2.7 |
| Hearing loss | 6 | 4.0 |
| Asthma | 6 | 4.0 |
| Other respiratory conditions | 9 | 6.0 |
| General age-related conditions | 3 | 2.0 |
| Cardiovascular related condition | 5 | 3.3 |
| Dermatological condition | 8 | 5.3 |
| Gastrointestinal condition | 7 | 4.7 |
| Fever | 3 | 2.0 |
| Other conditions | 27 | 18.0 |
| JSS Hospital as usual hospital visited | ||
| Yes | 119 | 79.3 |
| No | 29 | 19.3 |
| Number visits to JSS Hospital in past 12 months | ||
| 0–1 visit | 57 | 38.0 |
| 2–3 visits | 27 | 18.0 |
| 4–5 visits | 46 | 30.7 |
| >5 visits | 20 | 13.3 |
| Travel time to JSS hospital (minutes) (median (IQR)) | 45.0 (70.0) | |
| Another hospital closer to residence | ||
| Yes | 135 | 90.0 |
| No | 15 | 10.0 |
| Self-rated health [Median (IQR)] | 5.0 (5.0) | |
| Sex | Education | ||||||
|---|---|---|---|---|---|---|---|
| Total | Males | Females | p | ≤Primary | ≤Secondary | p | |
| n (%) | n (%) | n | n | n | |||
| Availability/access to technology | |||||||
| Home telephone | |||||||
| No | 141 (94.0) | 87 (96.2) | 54 (96.4) | 0.49 | 96 (95.0) | 45 (91.8) | 0.48 |
| Yes | 9 (6.0) | 7 (7.4) | 2 (3.6) | 5 (5.0) | 4 (8.2) | ||
| Mobile Phone | |||||||
| No mobile phone | 63 (42.0) | 32 (34.4) | 31 (55.4) | 0.01 | 55 (55.0) | 8 (16.3) | <0.001 |
| Mobile phone (standard calls and texts) | 73 (48.7) | 49 (52.7) | 24 (42.9) | 45 (45.0) | 28 (57.1) | ||
| Smartphone with internet access | 13 (8.7) | 12 (12.9) | 1 (1.8) | 0 | 13 (26.5) | ||
| Tablet | |||||||
| No | 145 (96.7) | 89 (94.7) | 56 (100.0) | 0.16 | 100 (99.0) | 45 (91.9) | 0.04 |
| Yes | 5 (3.3) | 5 (5.3) | 0 | 1 (1.0) | 4 (8.2) | ||
| Problems with mobile phone coverage | |||||||
| No problems | 94 (62.7) | 60 (63.8) | 34 (60.7) | 0.72 | 53 (55.2) | 41 (83.7) | <0.001 |
| Sometimes have problems | 21 (14.0) | 14 (14.9) | 7 (12.5) | 15 (14.9) | 6 (12.2) | ||
| Consistently have problems | 35 | 20 (21.3) | 15 (26.8) | 33 (32.7) | 2 (4.1) | ||
| Internet access at home | |||||||
| No | 136 (90.7) | 82 (87.2) | 54 (96.4) | 0.13 | 100 (99.0) | 36 (73.5) | <0.001 |
| Yes | 14 (9.3) | 12 (12.8) | 2 (3.6) | 1 (1.0) | 13 (26.5) | ||
| Used a computer | |||||||
| No | 146 (93.3) | 91 (96.8) | 55 (98.2) | 1.00 | 101 (100.0) | 45 (91.8) | 0.004 |
| Yes (home computer) | 4 (2.7) | 3 (3.2) | 1 (1.8) | 0 | 4 (8.2) | ||
| Sent e-mail or text message | |||||||
| Never | 133 (88.7) | 79 (84.0) | 54 (96.4) | 0.11 | 99 (98.0) | 34 (69.4) | <0.001 |
| Rarely | 6 (4.0) | 5 (5.3) | 1 (1.8) | 2 (2.0) | 4 (8.2) | ||
| Some days | 7 (4.7) | 7 (7.4) | 0 | 0 | 7 (14.3) | ||
| Most days | 4 (2.7) | 3 (3.2) | 1 (1.8) | 0 | 4 (8.2) | ||
| Used social media | |||||||
| No | 137 (91.3) | 82 (87.2) | 55 (98.2) | 0.03 | 101 (100.0) | 36 (73.5) | <0.001 |
| Yes | 12 (12.8) | 1 (1.8) | 0 | 13 (26.5) | |||
| 13 (8.7) | |||||||
| 8 (5.3) | |||||||
| 3 (2.0) | |||||||
| Used internet for videoconferencing or communication | |||||||
| No | 148 (98.7) | 2 (2.1) | 0 | 0.53 | 0 | 2 (4.1) | 0.11 |
| Yes | 2 (1.3) | 92 (97.9) | 56 (100.0) | 101 (100.0) | 47 (95.9) | ||
| Used internet to shop for groceries/ personal items | |||||||
| No | 146 (97.3) | 4 (4.3) | 0 | 0.30 | 0 | 4 (8.2) | 0.01 |
| Yes | 4 (2.7) | 90 (95.7) | 56 (100.0) | 101 (100.0) | 45 (91.8) | ||
| Pay bills/banking | |||||||
| No | 146 (97.3) | 90 (95.7) | 56 (100.0) | 0.30 | 101 (100.0) | 45 (91.8) | 0.01 |
| Yes | 4 (2.7) | 4 (4.3) | 0 | 0 | 4 (8.2) | ||
| Contact/find health care provider | |||||||
| No | 134 (89.3) | 79 (84.0) | 55 (98.2) | 0.006 | 101 (100.0) | 33 (67.3) | <0.001 |
| Yes | 16 (10.7) | 15 (16.0) | 1 (1.8) | 0 | 16 (32.7) | ||
| Get information about health conditions | |||||||
| No | 144 (96.0) | 88 (93.6) | 56 (100.0) | 0.08 | 101 (100.0) | 43 (87.8) | 0.001 |
| Yes | 6 (4.0) | 6 (6.4) | 0 | 0 | 6 (12.2) | ||
| Order/refill prescriptions | |||||||
| No | 147 (98.0) | 91 (97.8) | 56 (100.0) | 0.52 | 101 (100.0) | 2 (4.2) | 0.10 |
| Yes | 2 (1.3) | 2 (2.2) | 0 | 0 | 46 (95.8) | ||
| Sex | Education Level | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | Male | Female | ≤Primary | ≤Secondary | |||||||
| n | % | n | % | p | n | % | n | % | p | |||
| Digital literacy | 0.006 | <0.001 | ||||||||||
| Has NOT used internet for online shopping/banking or health-related purposes. | 134 | 89.3 | 79 | 84.0 | 55 | 98.2 | 101 | 100.0 | 33 | 67.3 | ||
| Has used internet for online shopping/banking AND/OR health-related purposes. | 16 | 10.7 | 15 | 16.0 | 1 | 1.8 | 0 | 0.0 | 16 | 32.7 | ||
| Health literacy | ||||||||||||
| Reading | 0.62 | 0.04 | ||||||||||
| Adequate | 5 | 3.3 | 3 | 3.2 | 2 | 3.6 | 1 | 1.0 | 4 | 8.2 | ||
| Inadequate | 145 | 96.7 | 91 | 96.8 | 54 | 96.4 | 100 | 99.0 | 45 | 91.8 | ||
| Learning | 0.001 | <0.001 | ||||||||||
| Adequate | 35 | 23.3 | 30 | 31.9 | 5 | 8.9 | 5 | 5.9 | 29 | 59.2 | ||
| Inadequate | 115 | 76.7 | 64 | 68.1 | 51 | 91.1 | 95 | 94.1 | 20 | 40.8 | ||
| Forms | 0.002 | <0.001 | ||||||||||
| Adequate | 41 | 27.3 | 34 | 36.2 | 7 | 12.5 | 11 | 10.9 | 30 | 61.2 | ||
| Inadequate | 109 | 72.7 | 60 | 63.8 | 49 | 87.5 | 90 | 89.1 | 19 | 38.8 | ||
| Framework Domain | Theme |
|---|---|
| Cognitive | Limited exposure, experiences and efficacy with technology—thereby limiting usage of available technologies |
| Social relations | “It takes a village to raise an elder”—multiple people within an older adult’s village are important contributors to the development of health beliefs, behaviours and maintenance of health |
| Affective | Lack of confidence with using technology—resulting in limited capability to receive and interpret the information |
| Other | Health behaviours and access to healthcare—the building of health beliefs and pathways to health comprised of a multifactorial layer of family, friends, neighbours and doctors |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rasekaba, T.M.; Pereira, P.; Rani. G, V.; Johnson, R.; McKechnie, R.; Blackberry, I. Exploring Telehealth Readiness in a Resource Limited Setting: Digital and Health Literacy among Older People in Rural India (DAHLIA). Geriatrics 2022, 7, 28. https://doi.org/10.3390/geriatrics7020028
Rasekaba TM, Pereira P, Rani. G V, Johnson R, McKechnie R, Blackberry I. Exploring Telehealth Readiness in a Resource Limited Setting: Digital and Health Literacy among Older People in Rural India (DAHLIA). Geriatrics. 2022; 7(2):28. https://doi.org/10.3390/geriatrics7020028
Chicago/Turabian StyleRasekaba, Tshepo Mokuedi, Pratibha Pereira, Vinaya Rani. G, Riya Johnson, Rebecca McKechnie, and Irene Blackberry. 2022. "Exploring Telehealth Readiness in a Resource Limited Setting: Digital and Health Literacy among Older People in Rural India (DAHLIA)" Geriatrics 7, no. 2: 28. https://doi.org/10.3390/geriatrics7020028