
Aromatherapy Massage vs. Foot Reflexology on the Severity of Restless Legs Syndrome in Female Patients Undergoing Hemodialysis

 and
and 
Abstract
:
1. Introduction
2. Materials and Methods
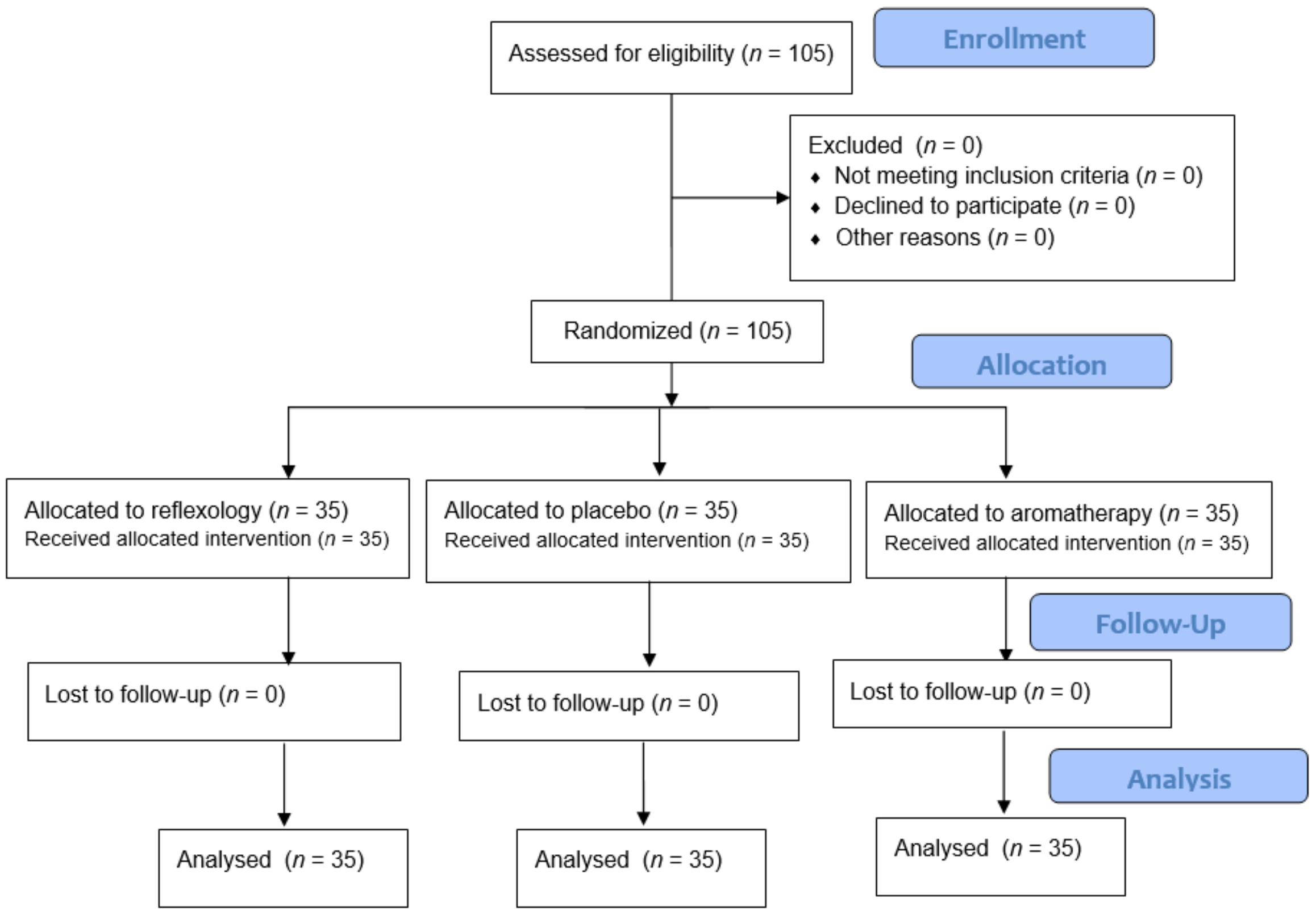
2.1. Design
2.2. Setting and Sampling
2.3. Blinding
2.4. Eligibility Criteria
2.5. Measures
2.6. Interventions
2.6.1. Reflexology
2.6.2. Aromatherapy Massage
2.6.3. Placebo
2.7. Ethical Considerations
2.8. Data Analysis
3. Results
3.1. Demographic Characteristics
3.2. Effects of the Interventions on RLS Severity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lin, X.-W.; Zhang, J.-F.; Qiu, M.-Y.; Ni, L.-Y.; Yu, H.-L.; Kuo, S.-H.; Ondo, W.G.; Yu, Q.; Wu, Y.-C. Restless legs syndrome in end stage renal disease patients undergoing hemodialysis. BMC Neurol. 2019, 19, 1–7. [Google Scholar] [CrossRef]
- Sateia, M.J. International Classification of Sleep Disorders-Third Edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Guo, S.; Huang, J.; Jiang, H.; Han, C.; Li, J.; Xu, X.; Zhang, G.; Lin, Z.; Xiong, N.; Wang, T. Restless Legs Syndrome: From Pathophysiology to Clinical Diagnosis and Management. Front. Aging Neurosci. 2017, 9, 171. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-M.; Kwon, H.-M.; Lim, C.S.; Kim, Y.S.; Lee, S.-J.; Nam, H. Restless Legs Syndrome in Patients on Hemodialysis: Symptom Severity and Risk Factors. J. Clin. Neurol. 2008, 4, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Jafari, M.; Rafie, S.; Azizi, M.; Bahadoram, M.; Jafari, S. Restless legs syndrome in hemodialysis patients. Saudi J. Kidney Dis. Transplant. 2016, 27, 326–330. [Google Scholar] [CrossRef]
- Lee, J. A Review of Restless Legs Syndrome in Patients on Hemodialysis. Kidney 2008, 18, 9–13. [Google Scholar] [CrossRef]
- Selcuk, N.; Kutlu, R.; Sayin, S.; Kal, O. Restless legs syndrome and quality of life in chronic hemodialysis patients. Niger. J. Clin. Pract. 2018, 21, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Yıldız, A. Assessment of cardiac autonomic functions by heart rate variability in patients with restless legs syndrome. Turk Kardiyol. Dern. Ars. 2018, 46, 191–196. [Google Scholar] [CrossRef]
- Lakasing, E. Exercise beneficial for restless legs syndrome. Practitioner 2008, 252, 43–45. [Google Scholar]
- Lettieri, C.J.; Eliasson, A.H. Pneumatic Compression Devices Are an Effective Therapy for Restless Legs Syndrome: A prospective, randomized, double-blinded, sham-controlled trial. Chest 2009, 135, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, U.H.; Myrer, J.W.; Johnson, A.W.; Hilton, S.C. Restless legs syndrome and near-infrared light: An alternative treatment option. Physiother. Theory Pract. 2010, 27, 345–351. [Google Scholar] [CrossRef]
- Mitchell, U.H. Nondrug-related aspect of treating Ekbom disease, formerly known as restless legs syndrome. Neuropsychiatr. Dis. Treat. 2011, 7, 251–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Draper, D.O.; Tessier, D.G. Sports Massage: An Overview. Athl. Ther. Today 2005, 10, 67–69. [Google Scholar] [CrossRef]
- Bahrami, T.; Rejeh, N.; Heravi-Karimooi, M.; Vaismoradi, M.; Tadrisi, S.; Sieloff, C.L. Aromatherapy massage versus reflexology on female elderly with acute coronary syndrome. Nurs. Crit. Care 2017, 23, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Embong, N.H.; Soh, Y.C.; Ming, L.C.; Wong, T.W. Revisiting reflexology: Concept, evidence, current practice, and practitioner training. J. Tradit. Complement. Med. 2015, 5, 197–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.; Chen, K.; Kuo, S.; Chen, I. Can foot reflexology be a complementary therapy for sleep disturbances? Evidence appraisal through a meta-analysis of randomized controlled trials. J. Adv. Nurs. 2021, 77, 1683–1697. [Google Scholar] [CrossRef] [PubMed]
- Özdemir, G.; Ovayolu, N.; Ovayolu, Ö. The effect of reflexology applied on hemodialysis patients with fatigue, pain and cramps. Int. J. Nurs. Pract. 2013, 19, 265–273. [Google Scholar] [CrossRef]
- Ali, B.; Al-Wabel, N.A.; Shams, S.; Ahamad, A.; Khan, S.A.; Anwar, F. Essential oils used in aromatherapy: A systemic review. Asian Pac. J. Trop. Biomed. 2015, 5, 601–611. [Google Scholar] [CrossRef] [Green Version]
- Metin, Z.G.; Donmez, A.A.; Izgu, N.; Ozdemir, L.; Arslan, I.E. Aromatherapy Massage for Neuropathic Pain and Quality of Life in Diabetic Patients. J. Nurs. Sch. 2017, 49, 379–388. [Google Scholar] [CrossRef]
- Gedney, J.J.; Glover, T.L.; Fillingim, R. Sensory and Affective Pain Discrimination after Inhalation of Essential Oils. Psychosom. Med. 2004, 66, 599–606. [Google Scholar] [CrossRef] [Green Version]
- Firoozeei, T.S.; Feizi, A.; Rezaeizadeh, H.; Zargaran, A.; Roohafza, H.R.; Karimi, M. The antidepressant effects of lavender (Lavandula angustifolia Mill.): A systematic review and meta-analysis of randomized controlled clinical trials. Complement. Ther. Med. 2021, 59, 102679. [Google Scholar] [CrossRef]
- Hashemi, S.H.; Hajbagheri, A.; Aghajani, M. The Effect of Massage with Lavender Oil on Restless Leg Syndrome in Hemodialysis Patients: A Randomized Controlled Trial. Nurs. Midwifery Stud. 2015, 4, e29617. [Google Scholar] [CrossRef] [Green Version]
- Özdemir, S.T.; Akyol, A. Effect of inhaler and topical lavender oil on pain management of arteriovenous fistula cannulation. J. Vasc. Access 2021. [Google Scholar] [CrossRef]
- Kang, H.-J.; Nam, E.S.; Lee, Y.; Kim, M. How Strong is the Evidence for the Anxiolytic Efficacy of Lavender? Systematic Review and Meta-analysis of Randomized Controlled Trials. Asian Nurs. Res. 2019, 13, 295–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karadag, E.; Bağlama, S.S. The Effect of Aromatherapy on Fatigue and Anxiety in Patients Undergoing Hemodialysis Treatment: A randomized controlled study. Holist. Nurs. Pract. 2019, 33, 222–229. [Google Scholar] [CrossRef]
- Muz, G.; Taşcı, S. Effect of aromatherapy via inhalation on the sleep quality and fatigue level in people undergoing hemodialysis. Appl. Nurs. Res. 2017, 37, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Ajorpaz, N.M.; Rahemi, Z.; Aghajani, M.; Hashemi, S.H. Effects of glycerin oil and lavender oil massages on hemodialysis patients’ restless legs syndrome. J. Bodyw. Mov. Ther. 2020, 24, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Habibzade, H.; Khalkhali, H.; Ghaneii, R. Study of the relationship between restless legs syndrome and sleep disturbance among patients in critical care units. Iran J. Crit. Care Nurs. 2011, 4, 153–158. [Google Scholar]
- Babashahi, M.; Kahangi, L.; Babashahi, F.; Fayazi, S. Comparing the Effect Of Massage Aromatherapy and Massage on Anxiety Level Of the Patients in the Preoperative Period: A clinical trial. Evid. Based Care 2012, 2, 19–28. [Google Scholar]
- International RLS Study Group (IRLSSG). Diagnostic Criteria. Available online: http://irlssg.org/diagnostic-criteria (accessed on 26 January 2020).
- Atkinson, M.; Allen, R.; DuChane, J.; Murray, C.; Kushida, C.; Roth, T. Validation of the Restless Legs Syndrome Quality of Life Instrument (RLS-QLI): Findings of a Consortium of National Experts and the RLS Foundation. Qual. Life Res. 2004, 13, 679–693. [Google Scholar] [CrossRef]
- Karatas, N.; Dalgic, A.I. Effects of reflexology on child health: A systematic review. Complement. Ther. Med. 2020, 50, 102364. [Google Scholar] [CrossRef]
- Buckle, J. Clinical Aromatherapy-E-Book: Essential Oils in Healthcare, 3rd ed.; Elsevier: St. Louis, MO, USA, 2015. [Google Scholar]
- Nasiri, M.; Abbasi, M.; Khosroabadi, Z.Y.; Saghafi, H.; Hamzeei, F.; Amiri, M.H.; Yusefi, H. Short-term effects of massage with olive oil on the severity of uremic restless legs syndrome: A double-blind placebo-controlled trial. Complement. Ther. Med. 2019, 44, 261–268. [Google Scholar] [CrossRef]
- Bouya, S.; Ahmadidarrehsima, S.; Badakhsh, M.; Balouchi, A.; Koochakzai, M. Effect of aromatherapy interventions on hemodialysis complications: A systematic review. Complement. Ther. Clin. Pract. 2018, 32, 130–138. [Google Scholar] [CrossRef]
- Hassanzadeh, M.; Kiani, F.; Bouya, S.; Zarei, M. Comparing the effects of relaxation technique and inhalation aromatherapy on fatigue in patients undergoing hemodialysis. Complement. Ther. Clin. Pract. 2018, 31, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Şentürk, A.; Kartın, P.T. The Effect of Lavender Oil Application via Inhalation Pathway on Hemodialysis Patients’ Anxiety Level and Sleep Quality. Holist. Nurs. Pract. 2018, 32, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Shahgholian, N.; Jazi, S.K.; Karimian, J.; Valiani, M. The effects of two methods of reflexology and stretching exercises on the severity of restless leg syndrome among hemodialysis patients. Iran. J. Nurs. Midwifery Res. 2016, 21, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Unal, K.S.; Akpinar, R.B. The effect of foot reflexology and back massage on hemodialysis patients’ fatigue and sleep quality. Complement. Ther. Clin. Pract. 2016, 24, 139–144. [Google Scholar] [CrossRef]
- Ahmadidarrehsima, S.; Mohammadpourhodki, R.; Ebrahimi, H.; Keramati, M.; Dianatinasab, M. Effect of foot reflexology and slow stroke back massage on the severity of fatigue in patients undergoing hemodialysis: A semi-experimental study. J. Complement. Integr. Med. 2018, 15. [Google Scholar] [CrossRef]
- Kliegel, E. Holistic Reflexology: Essential Oils and Crystal Massage in Reflex Zone Therapy, 1st ed.; Healing Arts Press, Simon and Schuster: Rochester, NY, USA, 2018. [Google Scholar]


{kind=link}
{kind=link}
| Characteristic | Aromatherapy Massage | Reflexology | Placebo | p-Value |
|---|---|---|---|---|
| Age (year) | 48.17 ± 1.65 | 52.77 ± 1.58 | 50.45 ± 1.13 | 0.09 |
| Education level | 0.001 | |||
| Illiterate | 3 (2.9%) | 9 (8.6%) | 8 (7.6%) | |
| Elementary | 24 (22.9%) | 29 (27.6%) | 13 (12.4%) | |
| Diploma | 3 (2.9%) | 2 (1.9%) | 14 (33.3%) | |
| Marital status | 1 | |||
| Married | 30 (28.6%) | 30 (28.6%) | 30 (28.6%) | |
| Single and widow | 5 (4.8%) | 5 (4.8%) | 5 (4.8%) | |
| Occupation | 0.6 | |||
| Housewife | 34 (32.5%) | 35 (33.3%) | 34 (32.5%) | |
| Employed | 1 (0.9%) | 0 (0%) | 1 (0.9%) | |
| Family history of restless legs syndrome | 0.12 | |||
| Yes | 8 (7.6%) | 3 (2.9%) | 3 (2.9%) | |
| No | 27 (25.7%) | 32 (30.5%) | 32 (30.5%) | |
| Duration of hemodialysis | 5.07 ± 0.53 | 5.41 ± 0.48 | 5.31 ± 0.43 | 0.49 |
| Smoking | 0.81 | |||
| Yes | 2 (1.9%) | 2 (1.9%) | 1 (0.9%) | |
| No | 33 (31.4%) | 33 (31.4%) | 34 (32.4%) |
| Time | Group | Mean ± SD | ||
|---|---|---|---|---|
| Before the intervention | Reflexology | 19.77 ± 3.049 | ||
| Aromatherapy massage | 21.71 ± 4.515 | |||
| Placebo | 20.43 ± 4.565 | |||
| After 4 weeks of the intervention | Foot Reflexology | 18.60 ± 5.192 | ||
| Aromatherapy | 17.06 ± 5.179 | |||
| Placebo | 20.54 ± 3.071 | |||
| After 8 weeks of the intervention | Foot Reflexology | 16.80 ± 5.357 | ||
| Aromatherapy | 13.20 ± 4.880 | |||
| Placebo | 19.51 ± 2.904 | |||
| Tests of Fixed Effects | Estimates of Fixed Effects | |||
| Source | DF | F | Sig | |
| Time | 2102 | 36.89 | 0.001 | a vs. c SE = 0.87, t = 1.04, p = 0.30 b vs. c SE = 0.60, t = 1.69, p = 0.09 |
| Group | 2102 | 5.70 | 0.004 | Reflexology vs. Placebo SE = 1.07, t = −2.51, p = 0.01 Aromatherapy vs. Placebo SE = 1.07, t = −5.86, p = 0.001 |
| Time*Group | 4102 | 10.06 | 0.001 | Reflexology *,a vs. Placebo *,a SE = 1.24, t = 1.65, p = 0.10 Aromatherapy *,a vs. Placebo *,a SE = 1.24, t = 6.12, p = 0.001 Foot Reflexology *,b vs. Placebo *,a SE = 0.85, t = 0.90, p = 0.37 Aromatherapy *,b vs. Placebo *,a SE = 0.85, t = 3.30, p = 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghasemi, M.; Rejeh, N.; Bahrami, T.; Heravi-Karimooi, M.; Tadrisi, S.D.; Vaismoradi, M. Aromatherapy Massage vs. Foot Reflexology on the Severity of Restless Legs Syndrome in Female Patients Undergoing Hemodialysis. Geriatrics 2021, 6, 99. https://doi.org/10.3390/geriatrics6040099
Ghasemi M, Rejeh N, Bahrami T, Heravi-Karimooi M, Tadrisi SD, Vaismoradi M. Aromatherapy Massage vs. Foot Reflexology on the Severity of Restless Legs Syndrome in Female Patients Undergoing Hemodialysis. Geriatrics. 2021; 6(4):99. https://doi.org/10.3390/geriatrics6040099
Chicago/Turabian StyleGhasemi, Mahbobeh, Nahid Rejeh, Tahereh Bahrami, Majideh Heravi-Karimooi, Seyed Davood Tadrisi, and Mojtaba Vaismoradi. 2021. "Aromatherapy Massage vs. Foot Reflexology on the Severity of Restless Legs Syndrome in Female Patients Undergoing Hemodialysis" Geriatrics 6, no. 4: 99. https://doi.org/10.3390/geriatrics6040099