
Sustaining or Declining Physical Activity: Reports from an Ethnically Diverse Sample of Older Adults



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Data Collection
2.2.1. Survey Data
2.2.2. Interview Data
- Have you made any change in your level of physical activity in the last several (2–3) years?
- Do you think you should be more physically active than you are? Why or why not?
- What, if anything, makes it difficult to make or sustain a change in activity level?
2.2.3. Protection of Human Subject
2.3. Data Analysis
2.3.1. Quantitative Analysis
2.3.2. Qualitative Analysis
3. Results
3.1. Sample Characteristics
3.2. Comparison by Ethnic Groups
Ethnic Group Differences in Relevant Characteristics
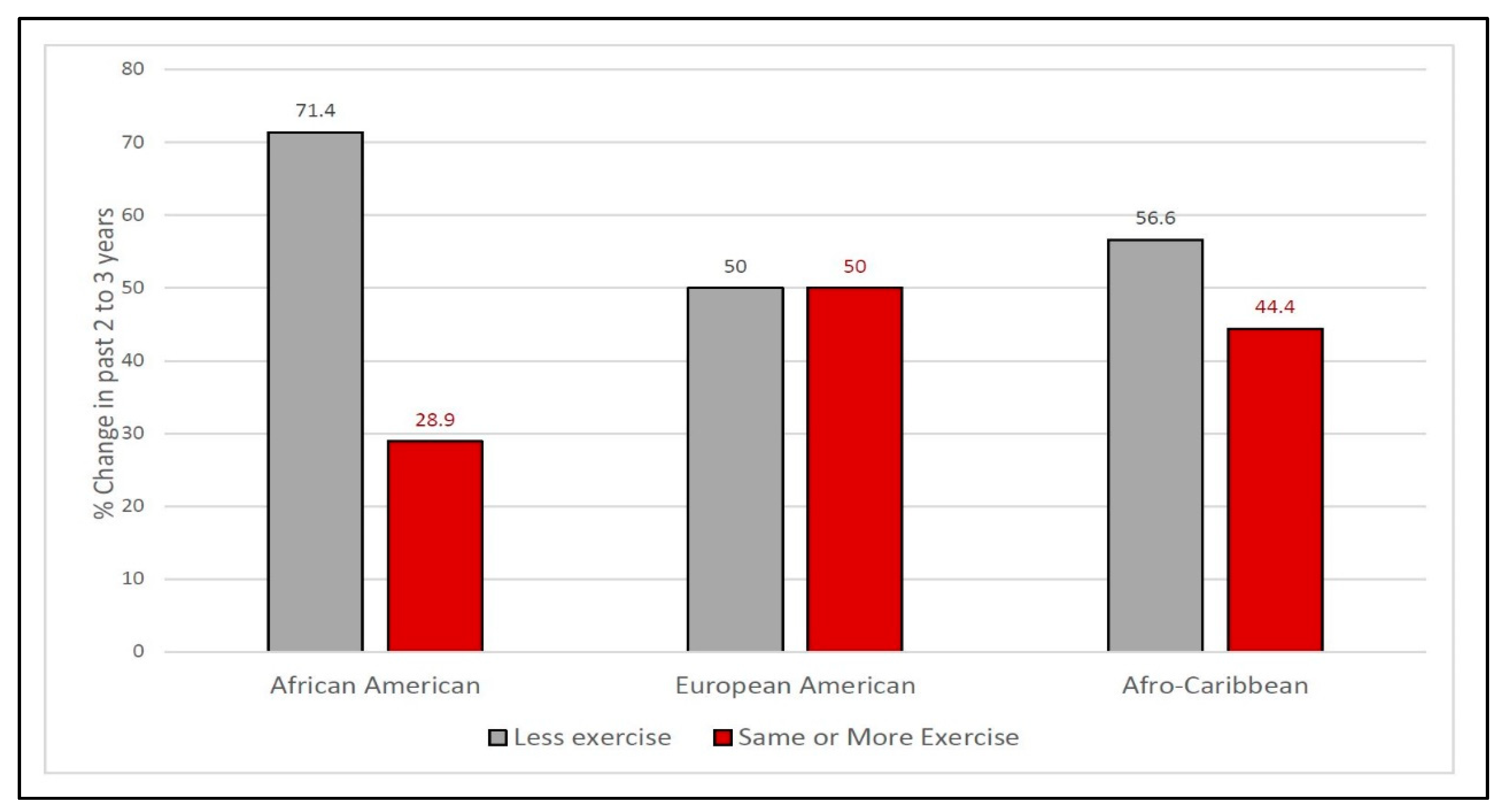
3.3. Sustaining Physical Activity
3.4. Explaining Activity Levels
- Positive on Physical Activity
- I think I am doing a good job of regular exercise. (AC)
- Stooping, bending, stretching for a few minutes a day; I do a lot of walking and we do dancing at church. (AA)
- I always feel better when I exercise. (AC)
- The body is meant to move. (You) can’t just sit. (EA)
- I know it’s important to keep moving. (AC)
- Exercise is good for you. It’s important to move your joints if you have arthritis. (EA)
- More physical activity keeps your body going, which keeps your brain going. (AA)
- 2.
- Struggling to Sustain Physical Activity.
- Sometimes my hip hurts and I don’t feel like walking. (AC)
- When I exercise, there is pain in my neck and back due to arthritis. (EA)
- I force myself to walk each day. My long-distance walking is much shorter now because I get short of breath. (AA)
- 3.
- Wishing They Could Do More.
- If I had known I would live this long, I would have taken better care of myself. I want to think about how to improve it and make it better. (AA)
- Want to be more active. Back pain and arthritis. (EA)
- I think I should get involved and exercise. I know I should exercise for my bad knees. (AA)
- My metabolism is slow; everything I eat turns to fat. I would love to be more active. (EA)
- I know it’s good for me and I should be doing it more often. (AC)
- 4.
- Physical Barriers Impeding Activity.
- Poor circulation, varicose veins, and swelling. (AC)
- The pain in my knees makes it difficult to do much walking. (AC)
- No exercise anymore because of shoulder problems. (AC)
- I don’t have the energy. I get tired so fast. (AA)
- I get short of breath. (AA)
- 5.
- Psychological Barriers Impeding Activity.
- Would go to the gym more if I wasn’t working part-time. (AC)
- Finding time after work, when I still have energy. (AA)
- Not enough time. (EA)
- I have too much to do. (AC)
- I am lazy and do what I want. (AA)
- Probably I could do more, but I just don’t. (AC)
- Lack of motivation. (AC)
- I’m not doing anything right now. (AC)
- By sleeping so many hours, I have less time to be active, have gained some weight. (EA)
- I don’t want to become more active. (AC)
- I don’t like exercising. I can’t find more places to dance. (EA)
3.5. Themes
3.6. Too Old
3.7. Influence of Friends and Family
3.8. Effect of Ethnic Group Membership
3.9. Confusion between Physical and Social Activity
4. Discussion
4.1. Summary of Results
4.2. Toward a Lifetime of Physical Activity
4.3. Facilitators and Barriers to Sustaining Activity
4.4. Tailoring Physical Activity Interventions
4.5. Limitations
4.6. Implications for Future Physical Activity and Interventions
4.7. Implications for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sampaio, A.; Marques-Aleixo, I.; Seabra, A.; Mota, J.; Marques, E.; Carvalho, J. Physical fitness in institutionalized older adults with dementia: Association with cognition, functional capacity and quality of life. Aging Clin. Exp. Res. 2020, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Physical Activity—Key Facts. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 12 May 2021).
- U.S. Department of Health & Human Services. Facts & Statistics. 2020. Available online: https://www.hhs.gov/fitness/resource-center/facts-and-statistics/index.html (accessed on 14 July 2020).
- Smith, G.L.; Banting, L.; Eime, R.; O’Sullivan, G.; Van Uffelen, J.G. The association between social support and physical activity in older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 56. [Google Scholar] [CrossRef]
- Kim, E.S.; Kubzansky, L.D.; Soo, J.; Boehm, J.K. Maintaining Healthy Behavior: A Prospective Study of Psychological Well-Being and Physical Activity. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2017, 51, 337–347. [Google Scholar] [CrossRef]
- Andrews, R.M.; Tan, E.J.; Varma, V.R.; Rebok, G.W.; Romani, W.A.; Seeman, T.E.; Gruenewald, T.L.; Tanner, E.K.; Carlson, M.C. Positive aging expectations are associated with physical activity among urban-dwelling older adults. Gerontologist 2017, 57, S178–S186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crombie, I.K.; Irvine, L.; Williams, B.; McGinnis, A.R.; Slane, P.W.; Alder, E.M.; McMurdo, M.E. Why older people do not participate in leisure time physical activity: A survey of activity levels, beliefs, and deterrents. Age Ageing 2004, 33, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Rivera-Torres, S.; Fahey, T.D.; Rivera, M.A. Adherence to Exercise Programs in Older Adults: Informative Report. Gerontol. Geriatr. Med. 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Cavazzatto, T.G.; Ronque, E.R.V.; Vieira, E.R.; Queiroga, M.R.; Junior, H.S. Social-Ecological Correlates of Regular Leisure-Time Physical Activity Practice among Adults. Int. J. Environ. Res. Public Health 2020, 17, 3619. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Clark, V.L. Plano. Designing and Conducting Mixed Methods Research; Sage Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Tappen, R.M.; Rosselli, M.; Engstrom, G. Use of the MC-FAQ and MMSE-FAQ in cognitive screening of African Americans, Hispanic Americans and European Americans. Am. J. Geriatr. Psychiatry 2012, 20, 955–962. [Google Scholar] [CrossRef]
- Pfeffer, R.I.; Kurosaki, M.T.T.; Harrah, J.C.H.; Chance, J.M.; Filos, R.S. Measurement of Functional Activities in Older Adults in the Community. J. Gerontol. 1982, 37, 323–329. [Google Scholar] [CrossRef]
- Superior Spreadsheet Solutions Offered with SAS/CALC Software. SAS Commun. 1991, 17, 2–5.
- Miles, M.B.; Huberman, A.M.; Saldaña, J. Qualitative Data Analysis: A Methods Sourcebook, 4th ed.; SAGE: Los Angeles, CA, USA, 2020. [Google Scholar]
- Tappen, R.M. Advanced Nursing Research: From Theory to Practice (2nd Ed.) 2016, 1st ed.; Jones and Bartlett Learning: Sudbury, MA, USA, 2011. [Google Scholar]
- Patton, M.Q. Qualitative Research and Evaluation Methods, 4th ed.; Sage Publishing: St Paul, MN, USA, 2014. [Google Scholar]
- Morgan, G.S.; Willmott, M.; Ben-Shlomo, Y.; Haase, A.M.; Campbell, R.M. A life fulfilled: Positively influencing physical activity in older adults—A systematic review and meta-ethnography. BMC Public Health 2019, 19, 1–13. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed. Available online: https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf (accessed on 12 May 2021).
- Vieira, E.R.; Tappen, R.; Gropper, S.S.; Severi, M.T.; Engstrom, G.; De Oliveira, M.R.; Barbosa, A.C.; Da Silva, R.A. Changes on Walking During Street Crossing Situations and on Dorsiflexion Strength of Older Caribbean Americans After an Exercise Program: A Pilot Study. J. Aging Phys. Act. 2017, 25, 525–532. [Google Scholar] [CrossRef]
- Notthoff, N.; Reisch, P.; Gerstorf, D. Individual Characteristics and Physical Activity in Older Adults: A Systematic Review. Gerontology 2017, 63, 443–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, C.; Sheeran, P. The health belief model. In Predicting Health Behavior, 2nd ed.; Conner, M., Norman, P., Eds.; Open University Press: New York, NY, USA, 2005; pp. 28–80. [Google Scholar]
- Rosenstock, I.M. Historical origins of the health belief model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Sas-Nowosielski, K.; Hadzik, A.; Gorna, J.; Grabara, M. Applying the health belief model in explaining the stages of exercise change in older adults. Pol. J. Sport Tour. 2016, 23, 221–225. [Google Scholar] [CrossRef] [Green Version]
- Conner, M.; Sparks, P. Theory of Planned Behaviour and Health Belief. In Predicting Health Behavior, 2nd ed.; Conner, M., Norman, P., Eds.; Open University Press: New York, NY, USA, 2005; pp. 170–222. [Google Scholar]
- Rhodes, R.E.; McEwan, D.; Rebar, A.L. Theories of physical activity behavior change: A history and synthesis of approaches. Psychol. Sport Exerc. 2019, 42, 100–109. [Google Scholar] [CrossRef]
- Bandura, A. Health promotion from the perspective of social cognitive theory. In Understanding and Changing Health Behavior: From Health Beliefs to Self-Regulation; Norman, P., Abraham, C., Conner, M., Eds.; Hardwood Academic Publishers: Amsterdam, The Netherlands, 2000; pp. 299–339. [Google Scholar]
- Naugle, K.M.; Ohlman, T.; Naugle, K.E.; Riley, Z.A.; Keith, N.R. Physical activity behavior predicts endogenous pain modulation in older adults. Pain 2017, 158, 383–390. [Google Scholar] [CrossRef]
- Koltyn, K.F. Using Physical Activity to Manage Pain in Older Adults. J. Aging Phys. Act. 2002, 10, 226–239. [Google Scholar] [CrossRef] [Green Version]
- Quicke, J.G.; Foster, N.E.; Thomas, M.J.; Holden, M.A. Is long-term physical activity safe for older adults with knee pain? a systematic review. Osteoarthr. Cartil. 2015, 23, 1445–1456. [Google Scholar] [CrossRef] [Green Version]
- Grossman, M.D.; Steward, A.L. You aren’t going to get better by just sitting around: Physical activity perceptions, motivators and barriers in adults 75 years of age or older. Am. J. Geriatr. Cardiol. 2003, 12, 33–37. [Google Scholar] [CrossRef]
- Kortebein, P.; Ferrando, A.; Lombeida, J.; Wolfe, R.; Evans, W.J. Effect of 10 days of bed rest on skeletal muscle in healthy older adults. JAMA 2007, 297, 1772–1774. [Google Scholar] [CrossRef]
- McAuley, E.; Elavsky, S.; Motl, R.W.; Konopack, J.F.; Hu, L.; Marquez, D.X. Physical activity, self-efficacy, and self-esteem: Longitudinal relationships in older adults. J. Gerontol. 2005, 60, 268–275. [Google Scholar] [CrossRef] [Green Version]
- Senkowski, V.; Gannon, C.; Branscum, P. Behavior Change Techniques Used in Theory of Planned Behavior Physical Activity Interventions Among Older Adults: A Systematic Review. J. Aging Phys. Act. 2019, 27, 746–754. [Google Scholar] [CrossRef]
- Schutzer, K.A. Barriers and motivations to exercise in older adults. Prev. Med. 2004, 39, 1056–1061. [Google Scholar] [CrossRef]
- Pool, M.S.; Agyemang, C.O.; Smalbrugge, M. Interventions to improve social determinants of health among elderly ethnic minority groups: A review. Eur. J. Public Health 2017, 27, 1048–1054. [Google Scholar] [CrossRef]


{kind=link}
| African American | European American | Afro-Caribbean | |||
|---|---|---|---|---|---|
| Continuous Variables | M (SD) | M (SD) | M (SD) | F | p |
| Age in years | 74.90 (7.50) | 76.95 (9.18) | 75.76 (7.31) | 0.36 | 0.69 |
| Years of education | 11.80 (3.04) | 17.78 (4.65) | 11.06 (3.23) | 19.36 | <0.01 *b |
| Years in U.S. | 74.92 (7.48) | 67.59 (17.45) | 36.25 (15.37) | 38.00 | <0.01 *c |
| Cognition (MMSE) | 26.55 (2.79) | 27.58 (4.15) | 27.68 (3.66) | 0.60 | 0.55 |
| Function (FAQ) | 2.14 (3.00) | 1.73 (3.95) | 2.64 (4.87) | 0.26 | 0.77 |
| BMI kg/m2 | 43.29 (6.56) | 35.22 (3.81) | 37.66 (6.52) | 11.00 | <0.01 *a |
| Categorical Variables | African American | European American | Afro-Caribbean | Phi Coefficient | Fisher’s Exact Test p |
| Gender | 2 (M) 19 (F) | 14 (M) 10 (F) | 4 (M) 13 (F) | 0.45 | <0.01 *b |
| Born in the U.S. | 0 (no) 21 (yes) | 4 (no) 20 (yes) | 15 (no) 2 (yes) | 0.78 | <0.01 *c |
| Receiving Medicaid | 15 (no) 6 (yes) | 22 (no) 1 (yes) | 14 (no) 3 (yes) | 0.27 | 0.09 |
| 95% CI for OR | ||||||||
|---|---|---|---|---|---|---|---|---|
| B | SE | Wald | df | p | OR | Lower | Upper | |
| Ethnicity (EA) | - | - | 3.138 | 2 | 0.208 | - | - | - |
| AA | 1.68 | 1.08 | 2.40 | 1 | 0.122 | 5.35 | 0.64 | 44.67 |
| AC | 2.50 | 1.46 | 2.92 | 1 | 0.088 | 12.19 | 0.69 | 214.57 |
| Age | −0.08 | 0.04 | 3.30 | 1 | 0.069 | 0.92 | 0.85 | 1.01 |
| BMI | 0.05 | 0.09 | 0.28 | 1 | 0.594 | 1.05 | 0.88 | 1.26 |
| Constant | 3.34 | 4.04 | 0.69 | 1 | 0.408 | 28.22 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tappen, R.; Vieira, E.R.; Gropper, S.S.; Newman, D.; Horne, C. Sustaining or Declining Physical Activity: Reports from an Ethnically Diverse Sample of Older Adults. Geriatrics 2021, 6, 57. https://doi.org/10.3390/geriatrics6020057
Tappen R, Vieira ER, Gropper SS, Newman D, Horne C. Sustaining or Declining Physical Activity: Reports from an Ethnically Diverse Sample of Older Adults. Geriatrics. 2021; 6(2):57. https://doi.org/10.3390/geriatrics6020057
Chicago/Turabian StyleTappen, Ruth, Edgar Ramos Vieira, Sareen S. Gropper, David Newman, and Cassandre Horne. 2021. "Sustaining or Declining Physical Activity: Reports from an Ethnically Diverse Sample of Older Adults" Geriatrics 6, no. 2: 57. https://doi.org/10.3390/geriatrics6020057