Effects of Music Therapy on Patients with Dementia—A Systematic Review


Abstract
:1. Introduction
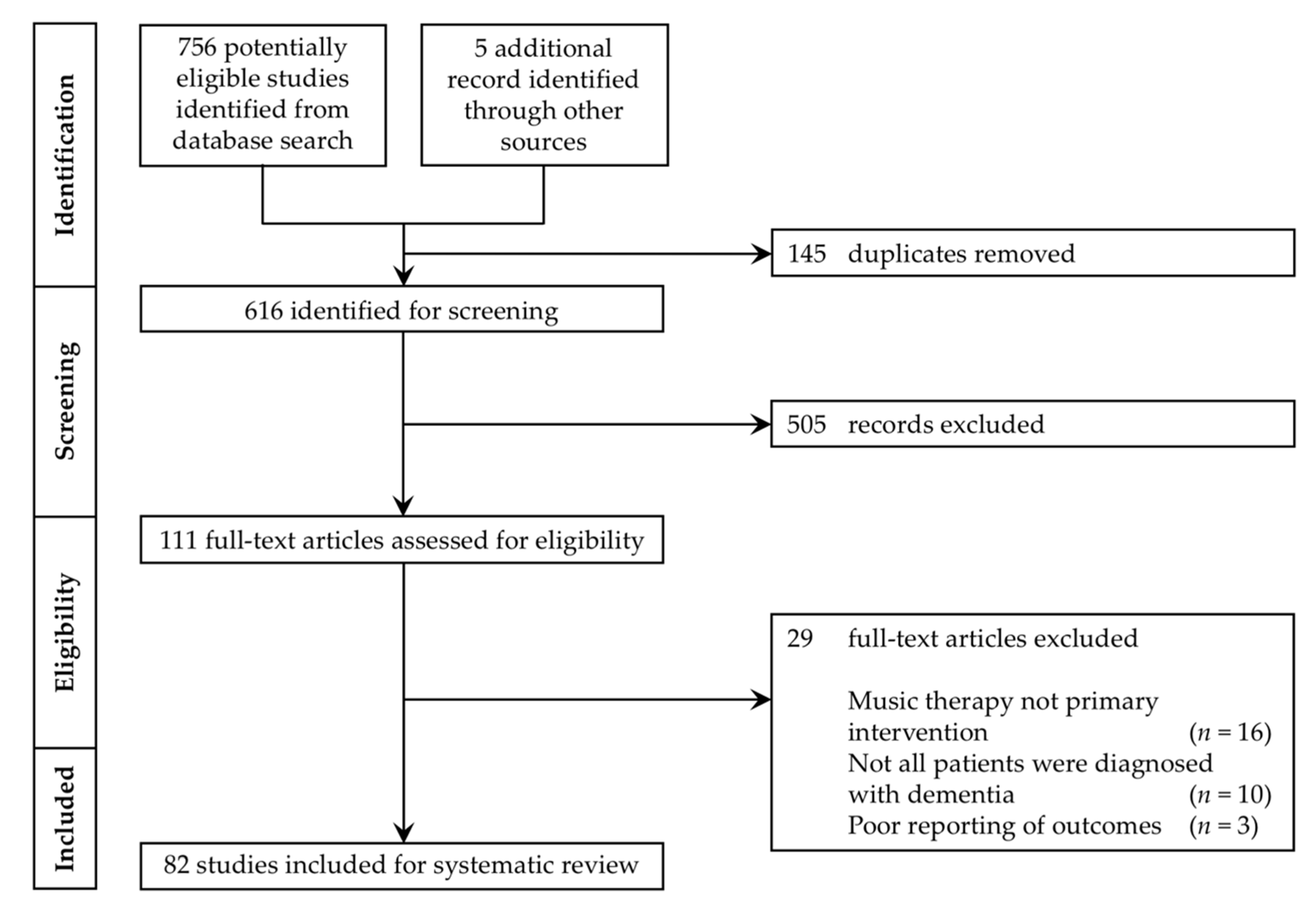
2. Materials and Methods
3. Results
3.1. Cognition
3.1.1. Overall Cognition
3.1.2. Memory
3.1.3. Language
3.2. Behavioral and Psychological Symptoms of Dementia (BPSDs)
3.2.1. Overall BPSD
3.2.2. Anxiety and Depression
3.2.3. Agitation
3.3. Apathy
3.4. Daily Functioning
3.5. Physiological Outcomes
3.6. Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Department of Economic and Social Affairs; United Nations. World Population Prospects 2019: Highlights. 2019. Available online: https://population.un.org/wpp/Publications/Files/WPP2019_10KeyFindings.pdf (accessed on 24 July 2020).
- Fiest, K.M.; Jetté, N.; Roberts, J.I.; Maxwell, C.J.; Smith, E.E.; Black, S.E.; Hogan, D.B. The Prevalence and Incidence of Dementia: A Systematic Review and Meta-analysis. Can. J. Neurol. Sci. 2016, 43, S3–S50. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Society. Risk Factors for Dementia (Factsheet 450LP). 2016. Available online: https://www.alzheimers.org.uk/sites/default/files/pdf/factsheet_risk_factors_for_dementia.pdf (accessed on 24 July 2020).
- Kalaria, R.N.; Maestre, G.E.; Arizaga, R.; Friedland, R.P.; Galasko, D.; Hall, K.; Antuono, P. Alzheimer’s disease and vascular dementia in developing countries: Prevalence, management, and risk factors. Lancet Neurol. 2008, 7, 812–826. [Google Scholar] [CrossRef] [Green Version]
- Blanco-Silvente, L.; Castells, X.; Saez, M.; Barceló, M.A.; Garre-Olmo, J.; Vilalta-Franch, J.; Capellà, D. Discontinuation, Efficacy, and Safety of Cholinesterase Inhibitors for Alzheimer’s Disease: A Meta-Analysis and Meta-Regression of 43 Randomized Clinical Trials Enrolling 16 106 Patients. Int. J. Neuropsychopharmacol. 2014, 20, 519–528. [Google Scholar] [CrossRef]
- Raglio, A.; Filippi, S.; Bellandi, D.; Stramba-Badiale, M. Global music approach to persons with dementia: Evidence and practice. Clin. Interv. Aging 2014, 9, 1669. [Google Scholar] [CrossRef] [Green Version]
- Davis, W.B.; Gfeller, K.E.; Thaut, M. An Introduction to Music Therapy: Theory and Practice; American Music Therapy Association: Silver Spring, MD, USA, 2008. [Google Scholar]
- Definition and Quotes about Music Therapy. Available online: https://www.musictherapy.org/about/quotes/ (accessed on 10 August 2020).
- Bruscia, K.E. Defining Music Therapy; Gilsum, N.H., Ed.; Barcelona: New Braunfels, TX, USA, 1998. [Google Scholar]
- Li, C.; Liu, C.; Yang, Y.; Chou, M.; Chen, C.; Lai, C. Adjunct effect of music therapy on cognition in Alzheimer’s disease in Taiwan: A pilot study. Neuropsychiatr. Dis. Treat. 2015, 11, 291. [Google Scholar] [CrossRef] [Green Version]
- Hong, I.S.; Choi, M.J. Songwriting oriented activities improve the cognitive functions of the aged with dementia. Arts Psychother. 2011, 38, 221–228. [Google Scholar] [CrossRef]
- Raglio, A.; Bellelli, G.; Traficante, D.; Gianotti, M.; Ubezio, M.C.; Villani, D.; Trabucchi, M. Efficacy of Music Therapy in the Treatment of Behavioral and Psychiatric Symptoms of Dementia. Alzheimer Dis. Assoc. Disord. 2008, 22, 158–162. [Google Scholar] [CrossRef] [Green Version]
- Lyu, J.; Zhang, J.; Mu, H.; Li, W.; Champ, M.; Xiong, Q.; Li, M. The Effects of Music Therapy on Cognition, Psychiatric Symptoms, and Activities of Daily Living in Patients with Alzheimer’s Disease. J. Alzheimers Dis. 2018, 64, 1347–1358. [Google Scholar] [CrossRef] [Green Version]
- Chu, H.; Yang, C.; Lin, Y.; Ou, K.; Lee, T.; O’Brien, A.P.; Chou, K. The Impact of Group Music Therapy on Depression and Cognition in Elderly Persons with Dementia. Biol. Res. Nurs. 2013, 16, 209–217. [Google Scholar] [CrossRef]
- Särkämö, T.; Tervaniemi, M.; Laitinen, S.; Numminen, A.; Kurki, M.; Johnson, J.K.; Rantanen, P. Cognitive, Emotional, and Social Benefits of Regular Musical Activities in Early Dementia: Randomized Controlled Study. Gerontologist 2013, 54, 634–650. [Google Scholar] [CrossRef] [Green Version]
- Ceccato, E.; Vigato, G.; Bonetto, C.; Bevilacqua, A.; Pizziolo, P.; Crociani, S.; Barchi, E. STAM Protocol in Dementia. Am. J. Alzheimers Dis. Other Dement. 2012, 27, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Lord, T.R.; Garner, J.E. Effects of Music on Alzheimer Patients. Percept. Mot. Skills 1993, 76, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Kanamori, M.; Watanabe, M.; Nagasawa, S.; Kojima, E.; Ooshiro, H.; Nakahara, D. Behavioral and endocrinological evaluation of music therapy for elderly patients with dementia. Nurs. Health Sci. 2004, 6, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Li, Z.; Xie, J.; Wang, T.; Yu, C.; An, N. Music therapy improves cognitive function and behavior in patients with moderate Alzheimer’s disease. Int. J. Clin. Exp. Med. 2018, 11, 4808–4814. [Google Scholar]
- Choi, A.; Lee, M.S.; Cheong, K.; Lee, J. Effects of Group Music Intervention on Behavioral and Psychological Symptoms in Patients with Dementia: A Pilot-Controlled Trial. Int. J. Neurosci. 2009, 119, 471–481. [Google Scholar] [CrossRef]
- Svansdottir, H.B.; Snaedal, J. Music therapy in moderate and severe dementia of Alzheimer’s type: A case–control study. Int. Psychogeriatr. 2006, 18, 613–621. [Google Scholar] [CrossRef] [Green Version]
- Pongan, E.; Tillmann, B.; Leveque, Y.; Trombert, B.; Getenet, J.C.; Auguste, N.; Rouch, I. Can Musical or Painting Interventions Improve Chronic Pain, Mood, Quality of Life, and Cognition in Patients with Mild Alzheimer’s Disease? Evidence from a Randomized Controlled Trial. J. Alzheimers Dis. 2017, 60, 663–677. [Google Scholar] [CrossRef]
- Nair, B.K.; Heim, C.; Krishnan, C.; D’este, C.; Marley, J.; Attia, J. The effect of Baroque music on behavioural disturbances in patients with dementia. Australas. J. Ageing 2011, 30, 11–15. [Google Scholar] [CrossRef]
- Raglio, A.; Bellelli, G.; Traficante, D.; Gianotti, M.; Ubezio, M.; Gentile, S.; Trabucchi, M. Efficacy of music therapy treatment based on cycles of sessions: A randomised controlled trial. Aging Ment. Health 2010, 14, 900–904. [Google Scholar] [CrossRef]
- Tang, Q.; Zhou, Y.; Yang, S.; Thomas, W.K.; Smith, G.D.; Yang, Z.; Chung, J.W. Effect of music intervention on apathy in nursing home residents with dementia. Geriatr. Nurs. 2018, 39, 471–476. [Google Scholar] [CrossRef]
- Lin, Y.; Chu, H.; Yang, C.; Chen, C.; Chen, S.; Chang, H.; Chou, K. Effectiveness of group music intervention against agitated behavior in elderly persons with dementia. Int. J. Geriatr. Psychiatry 2010, 26, 670–678. [Google Scholar] [CrossRef] [PubMed]
- De la Rubia Ortí, J.E.; García-Pardo, M.P.; Iranzo, C.C.; Madrigal, J.J.; Castillo, S.S.; Rochina, M.J.; Gascó, V.J. Does Music Therapy Improve Anxiety and Depression in Alzheimer’s Patients? J. Altern. Complement. Med. 2018, 24, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Okada, K.; Kurita, A.; Takase, B.; Otsuka, T.; Kodani, E.; Kusama, Y.; Atarashi, H.; Mizuno, K. Effects of Music Therapy on Autonomic Nervous System Activity, Incidence of Heart Failure Events, and Plasma Cytokine and Catecholamine Levels in Elderly Patients with Cerebrovascular Disease and Dementia. Int. Heart J. 2009, 50, 95–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez, A.; Maseda, A.; Marante-Moar, M.P.; Labra, C.D.; Lorenzo-López, L.; Millán-Calenti, J.C. Comparing the Effects of Multisensory Stimulation and Individualized Music Sessions on Elderly People with Severe Dementia: A Randomized Controlled Trial. J. Alzheimers Dis. 2016, 52, 303–315. [Google Scholar] [CrossRef]
- Shiltz, D.L.; Lineweaver, T.T.; Brimmer, T.; Cairns, A.C.; Halcomb, D.S.; Juett, J.; Plewes, J. “Music First” An Alternative or Adjunct to Psychotropic Medications for the Behavioral and Psychological Symptoms of Dementia. GeroPsych 2018, 31, 17–30. [Google Scholar] [CrossRef]
- Narme, P.; Clément, S.; Ehrlé, N.; Schiaratura, L.; Vachez, S.; Courtaigne, B.; Samson, S. Efficacy of Musical Interventions in Dementia: Evidence from a Randomized Controlled Trial. J. Alzheimers Dis. 2013, 38, 359–369. [Google Scholar] [CrossRef]
- Ho, R.T.; Fong, T.C.; Sing, C.; Lee, P.H.; Leung, A.B.; Chung, K.S.; Kwok, J.K. Managing behavioral and psychological symptoms in Chinese elderly with dementia via group-based music intervention: A cluster randomized controlled trial. Dementia 2018, 18, 2785–2798. [Google Scholar] [CrossRef]
- Sakamoto, M.; Ando, H.; Tsutou, A. Comparing the effects of different individualized music interventions for elderly individuals with severe dementia. Int. Psychogeriatr. 2013, 25, 775–784. [Google Scholar] [CrossRef]
- Kwak, J.; Anderson, K.; Valuch, K.O. Findings from a Prospective Randomized Controlled Trial of an Individualized Music Listening Program for Persons With Dementia. J. Appl. Gerontol. 2018, 39, 567–575. [Google Scholar] [CrossRef]
- Raglio, A.; Bellandi, D.; Baiardi, P.; Gianotti, M.; Ubezio, M.C.; Zanacchi, E.; Stramba-Badiale, M. Effect of Active Music Therapy and Individualized Listening to Music on Dementia: A Multicenter Randomized Controlled Trial. J. Am. Geriatr. Soc. 2015, 63, 1534–1539. [Google Scholar] [CrossRef]
- Guétin, S.; Portet, F.; Picot, M.; Pommié, C.; Messaoudi, M.; Djabelkir, L.; Touchon, J. Effect of Music Therapy on Anxiety and Depression in Patients with Alzheimer’s Type Dementia: Randomised, Controlled Study. Dement. Geriatr. Cogn. Disord. 2009, 28, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Maseda, A.; Cibeira, N.; Lorenzo-López, L.; González-Abraldes, I.; Buján, A.; Labra, C.D.; Millán-Calenti, J.C. Multisensory Stimulation and Individualized Music Sessions on Older Adults with Severe Dementia: Effects on Mood, Behavior, and Biomedical Parameters. J. Alzheimers Dis. 2018, 63, 1415–1425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ragneskog, H.; Bråne, G.; Karlsson, I.; Kihlgren, M. Influence of Dinner Music on Food Intake and Symptoms Common in Dementia. Scand. J. Caring Sci. 1996, 10, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Chang, A.M.; Lee, W. A preferred music listening intervention to reduce anxiety in older adults with dementia in nursing homes. J. Clin. Nurs. 2010, 19, 1056–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarkson, K.A.; Cassidy, K.; Eskes, G.A. Singing Soothes: Music Concerts for the Management of Agitation in Older Adults with Dementia. Can. J. Geriatr. 2007, 10, 80–87. [Google Scholar]
- Sung, H.; Lee, W.; Li, T.; Watson, R. A group music intervention using percussion instruments with familiar music to reduce anxiety and agitation of institutionalized older adults with dementia. Int. J. Geriatr. Psychiatry 2011, 27, 621–627. [Google Scholar] [CrossRef]
- Cooke, M.L.; Moyle, W.; Shum, D.H.; Harrison, S.D.; Murfield, J.E. A randomized controlled trial exploring the effect of music on agitated behaviours and anxiety in older people with dementia. Aging Ment. Health 2010, 14, 905–916. [Google Scholar] [CrossRef]
- Cooke, M.; Moyle, W.; Shum, D.; Harrison, S.; Murfield, J. A Randomized Controlled Trial Exploring the Effect of Music on Quality of Life and Depression in Older People with Dementia. J. Health Psychol. 2010, 15, 765–776. [Google Scholar] [CrossRef] [Green Version]
- Chang, F.; Huang, H.; Lin, K.; Lin, L. The effect of a music programme during lunchtime on the problem behaviour of the older residents with dementia at an institution in Taiwan. J. Clin. Nurs. 2010, 19, 939–948. [Google Scholar] [CrossRef]
- Garland, K.; Beer, E.; Eppingstall, B.; O’connor, D.W. A Comparison of Two Treatments of Agitated Behavior in Nursing Home Residents with Dementia: Simulated Family Presence and Preferred Music. Am. J. Geriatr. Psychiatry 2007, 15, 514–521. [Google Scholar] [CrossRef]
- Ragneskog, H.; Asplund, K.; Kihlgren, M.; Norberg, A. Individualized music played for agitated patients with dementia: Analysis of video-recorded sessions. Int. J. Nurs. Pract. 2001, 7, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Jennings, B.; Vance, D. The Short-Term Effects of Music Therapy on Different Types of Agitation in Adults with Alzheimer’s. Act. Adapt. Aging 2002, 26, 27–33. [Google Scholar] [CrossRef]
- Ridder, H.M.; Stige, B.; Qvale, L.G.; Gold, C. Individual music therapy for agitation in dementia: An exploratory randomized controlled trial. Aging Ment. Health 2013, 17, 667–678. [Google Scholar] [CrossRef] [Green Version]
- Ledger, A.J.; Baker, F.A. An investigation of long-term effects of group music therapy on agitation levels of people with Alzheimer’s Disease. Aging Ment. Health 2007, 11, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Vink, A.C.; Zuidersma, M.; Boersma, F.; Jonge, P.D.; Zuidema, S.U.; Slaets, J.P. The effect of music therapy compared with general recreational activities in reducing agitation in people with dementia: A randomised controlled trial. Int. J. Geriatr. Psychiatry 2012, 28, 1031–1038. [Google Scholar] [CrossRef]
- Holmes, C.; Knights, A.; Dean, C.; Hodkinson, S.; Hopkins, V. Keep music live: Music and the alleviation of apathy in dementia subjects. Int. Psychogeriatr. 2006, 18, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Matsushita, H. Long-Term Effects of Music Therapy on Elderly with Moderate/Severe Dementia. J. Music Ther. 2006, 43, 317–333. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Cai, J.; An, L.; Hui, F.; Ren, T.; Ma, H.; Zhao, Q. Does music therapy enhance behavioral and cognitive function in elderly dementia patients? A systematic review and meta-analysis. Ageing Res. Rev. 2017, 35, 1–11. [Google Scholar] [CrossRef]
- Gómez-Romero, M.; Jiménez-Palomares, M.; Rodríguez-Mansilla, J.; Flores-Nieto, A.; Garrido-Ardila, E.M.; González López-Arza, M.V. Benefits of music therapy on behaviour disorders in subjects diagnosed with dementia: A systematic review. Neurologia 2017, 32, 253–263. [Google Scholar] [CrossRef]
- Peretz, I.; Gagnon, L.; Hébert, S.; Macoir, J. Singing in the Brain: Insights from Cognitive Neuropsychology. Music Percept. 2004, 21, 373–390. [Google Scholar] [CrossRef] [Green Version]
- Steinke, W.R.; Cuddy, L.L.; Jakobson, L.S. Dissociations among functional subsystems governing melody recognition after right-hemisphere damage. Cogn. Neuropsychol. 2001, 18, 411–437. [Google Scholar] [CrossRef] [PubMed]
- Bradt, J.; Dileo, C.; Magill, L.; Teague, A. Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst. Rev. 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Kühlmann, A.Y.R.; De Rooij, A.; Kroese, L.F.; Van Dijk, M.; Hunink, M.G.M.; Jeekel, J. Meta-analysis evaluating music interventions for anxiety and pain in surgery. Br. J. Surg. 2018, 105, 773–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.C.; Wang, H.H.; Lu, C.Y.; Chen, T.B.; Lin, Y.H.; Lee, I. The effect of music therapy on reducing depression in people with dementia: A systematic review and meta-analysis. Geriatr. Nurs. 2019, 40, 510–516. [Google Scholar] [CrossRef]
- Tsoi, K.K.F.; Chan, J.Y.C.; Ng, Y.M.; Lee, M.M.Y.; Kwok, T.C.Y.; Wong, S.Y.S. Receptive Music Therapy Is More Effective than Interactive Music Therapy to Relieve Behavioral and Psychological Symptoms of Dementia: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2018, 19, 568–576. [Google Scholar] [CrossRef]
- Sihvonen, A.J.; Särkämö, T.; Leo, V.; Tervaniemi, M.; Altenmüller, E.; Soinila, S. Music-based interventions in neurological rehabilitation. Lancet Neurol. 2017, 16, 648–660. [Google Scholar] [CrossRef] [Green Version]
- American Music Therapy Association. Scope of Music Therapy Practice. Available online: https://www.musictherapy.org/about/scope_of_music_therapy_practice/ (accessed on 22 August 2020).
- Moreira, S.V.; Justi, F.R.R.; Moreira, M. Can musical intervention improve memory in Alzheimer’s patients? Evidence from a systematic review. Dement. Neuropsychol. 2018, 12, 133–142. [Google Scholar] [CrossRef]
- Pedersen, S.K.A.; Lugo, R.G.; Andreassen, M.; Sütterlin, S. Effects of Music on Agitation in Dementia: A Meta-Analysis. Front. Psychol. 2017, 8, 742. [Google Scholar] [CrossRef]
- Schumann, C.; Alexopoulos, P.; Perneczky, R. Determinants of self- and carer-rated quality of life and caregiver burden in Alzheimer disease. Int. J. Geriatr. Psychiatry 2019, 34, 1378–1385. [Google Scholar] [CrossRef]
- Birks, J.S.; Grimley Evans, J. Rivastigmine for Alzheimer’s disease. Cochrane Database Syst. Rev. 2015, 4. [Google Scholar] [CrossRef]
- Birks, J.S.; Harvey, R.J. Donepezil for dementia due to Alzheimer’s disease. Cochrane Database Syst. Rev. 2018, 6. [Google Scholar] [CrossRef]


{kind=link}
| Modalities [9] | Description |
|---|---|
| Song writing | Usually under the guidance of a music therapist in a group session; patients write lyrics for a melody. |
| Directed music listening | Music is played to patients in individualized sessions, sometimes according to their preference. |
| Music and relaxation exercises | Patients stretch and breathe to the rhythm of music. |
| Lyric discussion | A group-based session where patients discuss the lyrics of a song with each other, often in the presence of a music therapist. |
| Singing/Toning | Patients sing to accompany a given melody with lyrics. |
| Moving to music | Patients move or dance to songs. |
| Recording and video creation | Patients participate in producing a music recording or video. |
| Adapted instrument lessons | Patients learn to play musical instruments with the difficulty adapted to their personal condition. |
| Inclusion Criteria of Study: | Exclusion Criteria of Study: |
|---|---|
| Types of study: Randomized controlled trials (RCTs), cohort studies, case-control studies, case reports and case series, systematic reviews and meta analyses | Studies with music therapy combined with another intervention (e.g., cognitive enhancement therapies) |
| English full-text articles only | Studies with patients with unclear/possible clinical diagnosis of dementia, or patients with mild cognitive impairment |
| Study intervention: music therapy | Interventions of rhythmic auditory stimulation |
| Study population: patients clinically diagnosed with dementia |
| Modality of Music Therapy | Singing | Music Listening | Playing Musical Instruments | Song-Writing | Lyric Reading | Combined (2 or More Modalities) | |
|---|---|---|---|---|---|---|---|
| Outcomes | |||||||
| Cognition | |||||||
| Improved overall cognition | Y: Two studies [15,19] N: One study [13] | Y: One study [15] Mixed: One study [10] * N: Two studies [29,30] | N: One study [12] | Y: One study [11] | N: One study [13] | Y: One study [14] N: Three studies [18,25,31] | |
| Improved memory | Y: One study [15] N: One study [13] | – | – | Y: One study [11] | N: One study [13] | Y: Two studies [16,17] | |
| Improved language or verbal fluency | Y: One study [13] | – | – | Y: One study [11] | Y: One study [13] | Y: One study [18] | |
| Behavioral and Psychological Symptoms of Dementia (BPSD) | |||||||
| Reduced overall BPSD (lower NPI score) | Y: Two studies [13,25] | Y: Two studies [32,33] N: Three studies [10,34,35] | Y: One study [12] N: One study [35] | – | Y: One study [13] | Y: Two studies [20,21] | |
| Reduced anxiety or depression | Mixed: One study [22] ** | Y: Five studies [29,36,37,38,39] N: Two studies [30,40] | N: One study [24] | – | – | Y: Six studies [14,17,20,27,31,41] N: One study [42,43] **** | |
| Reduced agitation | – | Y: Six studies [29,30,40,44,45,46] N: Two studies [23,34] | Y: One study [24] | – | – | Y: Five studies [18,26,31,47,48] N: Four studies [41,42,49,50] | |
| Apathy | |||||||
| Reduced apathy | – | Mixed: One study [51] *** | Y: One study [24] | – | – | Y: One study [25] | |
| Daily Functioning | |||||||
| Improved daily functioning (improved Barthel Index) | N: One study [13] | – | N: One study [12] | – | N: One study [13] | Y: One study [16] | |
| Physiological outcomes | |||||||
| Reduced congested heart failure events | – | – | – | – | – | Y: One study [28] | |
| Reduced pain | Y: One study [22] | – | – | – | – | – | |
| Increased appetite | – | Y: One study [38] | – | – | – | – | |
| Lowered blood pressure | – | – | – | – | – | Y: One study [52] | |
| Decreased IL-6 and catecholamines | – | – | – | – | – | Y: One study [28] | |
| Reduction in salivary cortisol | – | – | – | – | – | Y: One study [27] N: Two studies [14,52] | |
| Quality of life | |||||||
| Improved quality of life | Y: One study [22] | Y: One study [15] N: One study [33] | – | – | – | Y: Two studies [20,33] N: Two studies [43,48] | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lam, H.L.; Li, W.T.V.; Laher, I.; Wong, R.Y. Effects of Music Therapy on Patients with Dementia—A Systematic Review. Geriatrics 2020, 5, 62. https://doi.org/10.3390/geriatrics5040062
Lam HL, Li WTV, Laher I, Wong RY. Effects of Music Therapy on Patients with Dementia—A Systematic Review. Geriatrics. 2020; 5(4):62. https://doi.org/10.3390/geriatrics5040062
Chicago/Turabian StyleLam, Hei Long, Wai Tak Victor Li, Ismail Laher, and Roger Y. Wong. 2020. "Effects of Music Therapy on Patients with Dementia—A Systematic Review" Geriatrics 5, no. 4: 62. https://doi.org/10.3390/geriatrics5040062