
Comparative Aspects of Canine Melanoma

Abstract
:1. Introduction
2. Canine Melanoma Epidemiology
3. Canine Malignant Melanoma Etiology
4. Canine Melanoma Pathological Aspects and Prognosis
- -
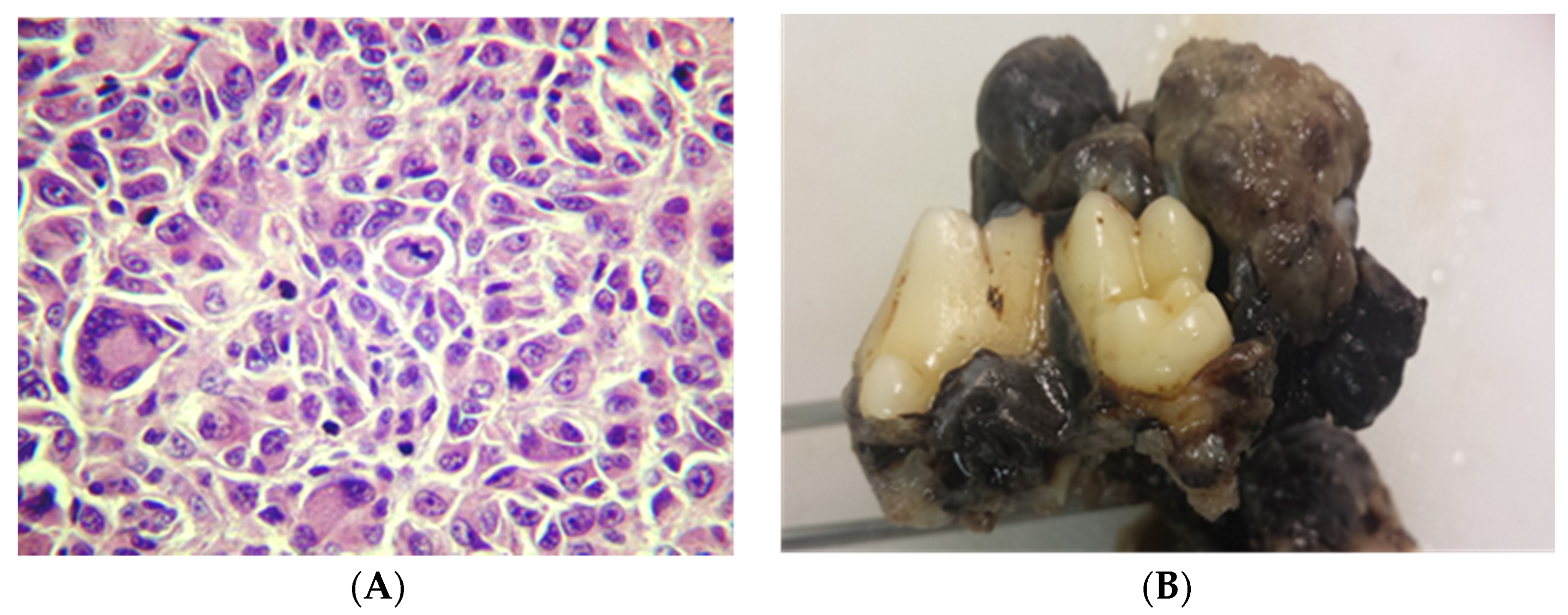
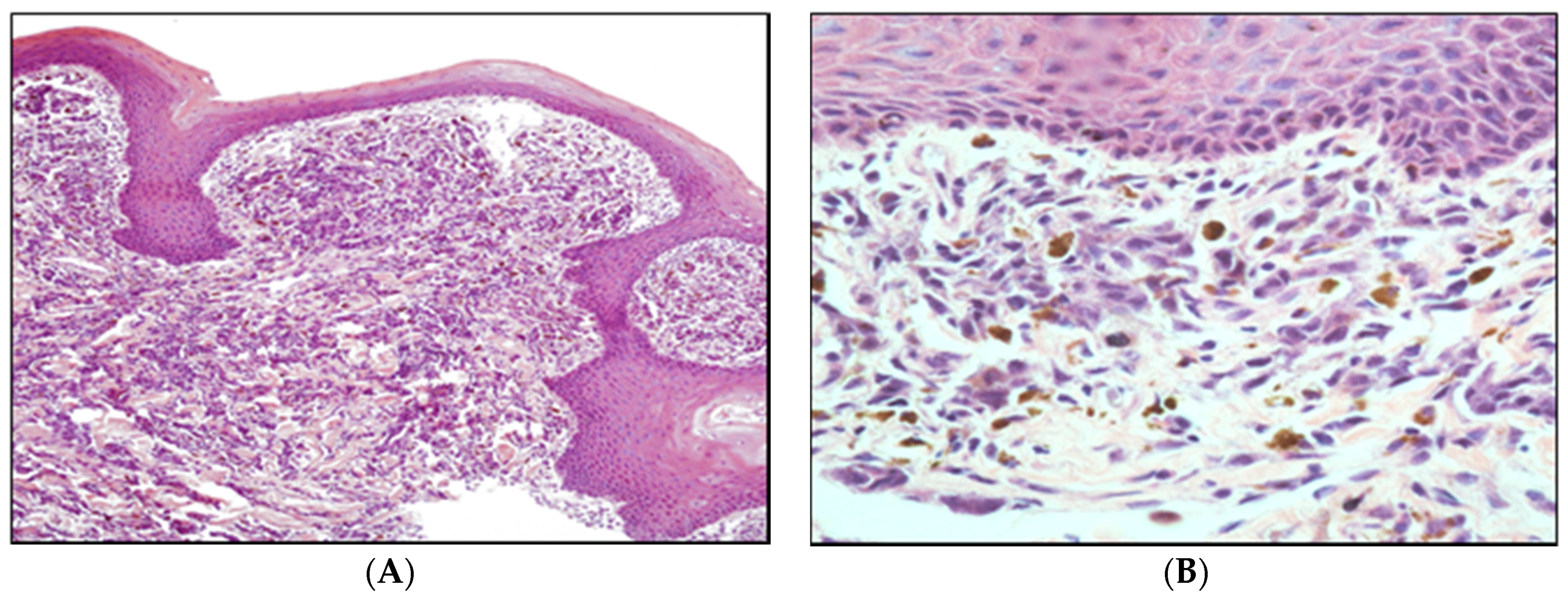
- epithelioid—round and polygonal cells (Figure 2)
- -
- spindle cell—tumor resembles fibroblasts
- -
- mixed tumors—show both cell types
5. Canine Melanoma: Molecular Aspects
- -
- CDKN2A Locus—about 70% of melanomas harbor mutations or deletions in this locus on chromosome 9p21.
- -
- Genes that are altered when normal melanocytes generate a nevus: BRAF, NRAS, and INK4a/ARF.
- -
- Genes that are mutated or deregulated when a nevus is transformed to a melanoma: BRAF, NRAS, INK4a/ARF, PTEN, c-kit, NEDD9, and MITF.
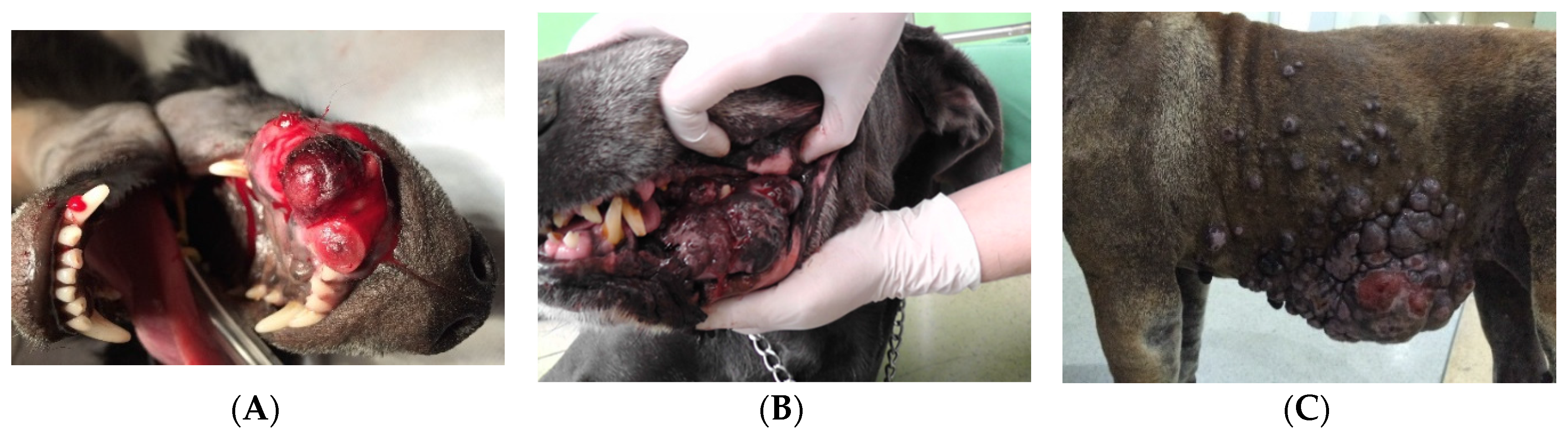
6. Canine Oral Melanomas
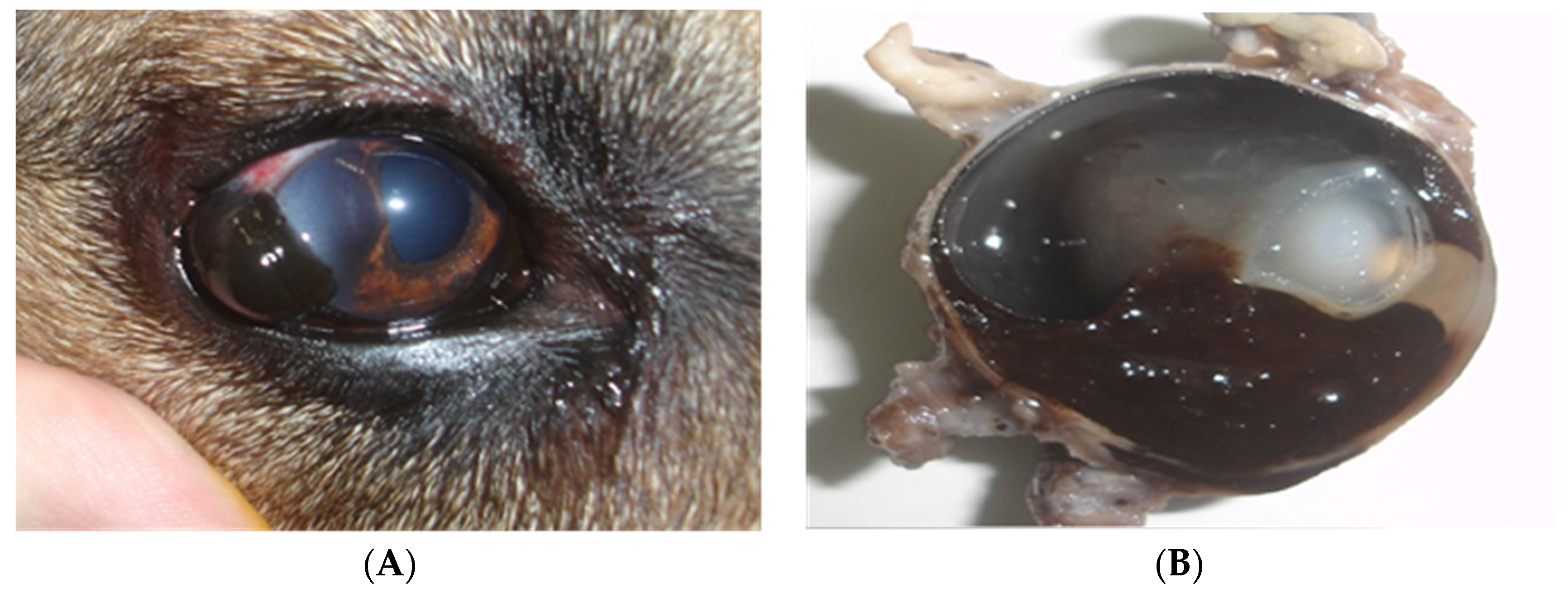
7. Canine Ocular Melanomas
8. Canine Digital Melanomas
Canine Cutaneous Melanomas
9. Treatment Modalities for Canine Melanomas
9.1. Surgery
9.2. Radiation Therapy
9.3. Chemotherapy
9.4. Immunotherapy
9.5. Outcomes after Treatment
9.6. New Perspectives for the Treatment of Canine Melanomas
10. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Sweet, M.; Kirkham, N.; Bendall, M.; Currey, L.; Bythell, J.; Heupel, M. PLoS ONE 2012. [CrossRef] [Green Version]
- Starkey, M.P.; Scase, T.J.; Mellersh, C.S.; Murphy, S. Dogs really are man’s best friend—Canine genomics has applications in veterinary and human medicine! Brief. Funct. Genomic. Proteomic. 2005, 4, 112–128. [Google Scholar] [CrossRef] [PubMed]
- Paoloni, M.; Khanna, C. Translation of new cancer treatments from pet dogs to humans. Nat. Rev. Cancer 2008, 8, 147–156. [Google Scholar]
- Nowend, K.L.; Starr-Moss, A.N.; Murphy, K.E. The function of dog models in developing gene therapy strategies for human health. Mamm. Genome 2011, 22, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Khanna, C.; Lindblad-Toh, K.; Vail, D.; London, C.; Bergman, P.; Barber, L.; Breen, M.; Kitchell, B.; McNeil, E.; Modiano, J.F.; et al. The dog as a cancer model. Nat. Biotechnol. 2006, 24, 1065–1066. [Google Scholar] [CrossRef] [PubMed]
- Fowles, J.S.; Denton, C.L.; Gustafson, D.L. Comparative analysis of MAPK and PI3K/AKT pathway activation and inhibition in human and canine melanoma. Vet. Comp. Oncol. 2015, 13, 288–304. [Google Scholar] [CrossRef] [PubMed]
- Haass, N.K.; Smalley, K.S.; Herlyn, M. The role of altered cell–cell communication in melanoma progression. J. Mol. Histol. 2004, 35, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Marcus, D.M.; Marcus, P.M.; Prabhu, R.S.; Owonikoko, T.K.; Lawson, D.H.; Switchenko, J.; Beither, J. Rising incidence of mucosal melanoma of the head and neck in the United States. J. Skin Cancer 2012, 231693. [Google Scholar]
- Gavriel, H.; McArthur, G.; Sizeland, A.; Henderson, M. Review: Mucosal melanoma of the head and neck. Melanoma Res. 2011, 21, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Meleti, M.; Leemans, C.R.; De Bree, R.; Vescovi, P.; Sesenna, E.; van der Waal, I. Head and neck mucosal melanoma: Experience with 42 patients, with emphasis on the role of postoperative radiotherapy. Head Neck 2008, 30, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Vara, J.A.; Beissenherz, M.E.; Miller, M.A.; Johnson, G.C.; Pace, L.W.; Fard, A.; Kottler, S.J. Retrospective study of 338 canine oral melanomas with clinical, histologic, and immunohistochemical review of 129 cases. Vet. Pathol. 2000, 37, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.C.; Garate, A.P.; Dagli, M.L.Z. Retrospective study of neoplasms in domestic animals: A survey between 1993 and 2002 of the service of animal pathology, department of pathology, school of veterinary medicine and animal science, University of Sao Paulo, Southeast Brazil. Braz. J. Vet. Pathol. 2012, 5, 60–69. [Google Scholar]
- Teixeira, T.F.; Silva, T.C.; Cogliati, B.; Nagamine, N.K.; Dagli, M.L.Z. Retrospective study of melanocytic neoplasms in dogs and cats. Braz. J. Vet. Pathol. 2010, 3, 100–104. [Google Scholar]
- Omholt, K.; Grafström, E.; Kanter-Lewensohn, L.; Hansson, J.; Ragnarsson-Olding, B.K. KIT pathway alterations in mucosal melanomas of the vulva and other sites. Clin. Cancer Res. 2011, 17, 3933–3942. [Google Scholar] [CrossRef] [PubMed]
- Zanoni, M.T.; Medicina, D.; Lombardi, D.; Ungari, M.; Balzarini, P.; Rossini, C.; Pellegrini, W.; Battaglia, P.; Capella, C.; Castelnuovo, P.; et al. Sinonasal mucosal melanoma: Molecular profile and therapeutic implications from a series of 32 cases. Head Neck 2013, 35, 1066–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyu, J.; Wu, Y.; Li, C.; Wang, R.; Song, H.; Ren, G.; Guo, W. Mutation scanning of BRAF, NRAS, KIT, and GNAQ/GNA11 in oral mucosal melanoma: A study of 57 cases. J. Oral Pathol. Med. 2015. [Google Scholar] [CrossRef] [PubMed]
- Curtin, J.A.; Fridlyand, J.; Kageshita, T.; Patel, H.N.; Busam, K.J.; Kutzner, H.; Cho, K.H.; Aiba, S.; Bröcker, E.B.; LeBoit, P.E.; et al. Distinct sets of genetic alterations in melanoma. N. Engl. J. Med. 2005, 353, 2135–2147. [Google Scholar] [CrossRef] [PubMed]
- Spangler, W.L.; Kass, P.H. The histologic and epidemiologic bases for prognostic consideration in canine melanocytic neoplasia. Vet. Pathol. 2006, 43, 136–149. [Google Scholar] [CrossRef] [PubMed]
- Gillard, M.; Cadieu, E.; De Brito, C.; Abadie, J.; Vergier, B.; Devauchelle, P.; Degorce, F.; Dreano, S.; Primot, A.; Dorso, L.; et al. Naturally occurring melanomas in dogs as models for non-UV pathways of human melanomas. Pigment Cell Melanoma Res. 2014, 27, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Priester, W.A. Skin tumors in domesticated animals. Data from 12 United States and Canadian Colleges of Veterinary Medicine. J. Natl. Cancer Insit. 1973, 50, 457–466. [Google Scholar]
- Goldschmidt, M.H. Pigmented lesions of the skin. Clin. Dermatol. 1994, 12, 507–514. [Google Scholar] [CrossRef]
- Marino, D.J.; Matthiesen, D.T.; Stefanacci, J.D.; Moroff, S.D. Evaluation of dogs with digit masses: 117 cases (1981–1991). J. Am. Vet. Med. Assoc. 1995, 207, 726–728. [Google Scholar] [PubMed]
- Miller, W.H.; Griffin, I.; Campbell, K.L. Muller and Kirk’s Small Animal Dermatology, 7th ed.; Elsevier Mosby: St. Louis, MO, USA, 2013; pp. 774–843. [Google Scholar]
- Teixeira, T.F.; Gentile, L.B.; Silva, T.C.; Mennecier, G.; Chaible, L.M.; Cogliati, B.; Roman, M.A.; Gioso, M.A.; Dagli, M.L.Z. Cell proliferation and expression of connexins differ in melanotic and amelanotic canine oral melanomas. Vet. Res. Commun. 2014, 38, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Tedardi, M.V.; Biondi, L.R.; Kimura, K.C.; Pedra Mendonça, P.; Grandi, F.; Latorre, A.M.; Dagli, M.L.Z. Comparative oncology in Sao Paulo, Brazil—What to learn from cancer registry. Source J. Vet. Sci. 2014, 1, 1–8. [Google Scholar]
- Tedardi, M.V.; Veneziano, D.B.; Kimura, K.C.; Pedra Mendonça, P.; Biondi, L.R.; Grandi, F.; Latorre, A.M.; Dagli, M.L.Z. Sao Paulo animal cancer registry, the first in Latin America. Vet. Comp. Oncol. 2015, 13, 154–155. [Google Scholar] [CrossRef] [PubMed]
- Haass, N.K.; Ripperger, D.; Wladykowski, E.; Dawson, P.; Gimotty, P.A.; Blome, C.; Fischer, F.; Schmage, P.; Moll, I.; Brandner, J.M. Melanoma progression exhibits a significant impact on connexin expression patterns in the epidermal tumor microenvironment. Histochem. Cell Biol. 2010, 133, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Modiano, J.F.; Ritt, M.G.; Wojcieszyn, J. The molecular basis of canine melanoma: Pathogenesis and trends in diagnosis and therapy. J. Vet. Intern. Med. 1999, 13, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.; Goldschmidt, H.; Mcmanus, P.M. A Comparative review of melanocytic neoplasms. Vet. Pathol. 2002, 39, 651–678. [Google Scholar] [CrossRef] [PubMed]
- Dzutsev, A.; Goldszmid, R.S.; Viaud, S.; Zivtogel, L.; Trinchieri, G. The role of the microbiota in inflammation, carcinogenesis, and cancer therapy. Eur. J. Immunol. 2015, 45, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Goldschmidt, M.H.; Hendrick, M.J. Tumors of the skin and soft tissues. In Tumors in Domestic Animals, 4th ed.; Meuten, D.J., Ed.; Iowa State Press: Ames, IA, USA, 2002; pp. 78–82. [Google Scholar]
- Scott, D.W.; Miller, W.H., Jr.; Griffin, C.E. Muller & Kirk’s Small Animal Dermatology, 6th ed.; Elsevier Saunders: Philadelphia, PA, USA, 2001; pp. 1–70. [Google Scholar]
- Li, G.; Herlyn, M. Dynamics of intercellular communication during melanoma development. Mol. Med. Today 2000, 6, 163–169. [Google Scholar] [CrossRef]
- Chin, L. The genetics of malignant melanoma: Lessons from mouse and man. Nat. Rev. Cancer 2003, 3, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Gaggioli, C.; Sahai, E. Melanoma invasion—Current knowledge and future directions. Pigment Cell Res. 2007, 20, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Head, K.W.; Else, R.W.; Dubielzig, R.R. Tumors of the Alimentary Tract. In Tumors in Domestic Animals, 4th ed.; Meuten, D.J., Ed.; Iowa State Press: Ames, IA, USA, 2002; pp. 426–430. [Google Scholar]
- Tajima, S.; Ura-Ishiko, A.; Hayashi, A. Melanogenesis, biosynthetic phenotype of fibronectin and collagen, and migrating activity in cloned B16 mouse melanoma cells. J. Dermatol. Sci. 1996, 12, 24–30. [Google Scholar] [CrossRef]
- Simonetti, O.; Lucarini, G.; Brancorsini, D.; Nita, P.; Bernardini, M.L.; Biagini, G.; Offidani, A. Immunohistochemical expression of vascular endothelial growth factor, matrix metalloproteinase 2 and matrix metalloproteinase 9 in cutaneous melanocytic lesions. Cancer 2002, 95, 602–624. [Google Scholar] [CrossRef] [PubMed]
- Nakhleh, R.E.; Wick, M.R.; Rocamora, A.; Swanson, P.E.; Dehner, L.P. Morphologic diversity in malignant melanomas. Am. J. Clin. Pathol. 1990, 93, 731–740. [Google Scholar] [PubMed]
- Chénier, S.; Doré, M. Oral Malignant Melanoma with Osteoid Formation in a Dog. Vet. Pathol. 1999, 36, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Smedley, R.C.; Spangler, W.L.; Esplin, D.G.; Kitchell, B.E.; Bergman, P.J.; Ho, H.Y.; Bergin, I.L.; Kiupel, M. Prognostic markers for canine melanocytic neoplasms: A comparative review of the literature and goals for future investigation. Vet. Pathol. 2011, 48, 54–72. [Google Scholar] [CrossRef] [PubMed]
- Sandusky, G.E.; Carlton, W.W.; Wightman, K.A. Diagnostic immunohistochemistry of canine round cell tumors. Vet. Pathol. 1987, 24, 495–499. [Google Scholar] [PubMed]
- Silva, A.P.; Silva, R.G.; Cogliati, B.; Dias, A.S.M.; Le Bas, A.E.; Hernandez-Blazquez, F.J. Bleaching of melanin in the epidermis of South American fur seal and its application on enzyme immunohistochemistry. Pesqui. Vet. Bras. 2011, 31, 267–270. [Google Scholar] [CrossRef] [Green Version]
- Fisher, D.E.; Kwong, L.N.; Chin, L. Melanoma. In DeVita VT, Hellman and Rosenberg’s Cancer Principles & Practice of Oncology, 8th ed.; De Vita, V.T., Jr., Lawrence, T.S., Rosenberg, S.A., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; pp. 1889–1951. [Google Scholar]
- Shelly, S.; Chien, M.B.; Yip, B.; Kent, M.S.; Theon, A.P.; McCallan, J.L.; London, C.A. Exon 15 BRAF mutations are uncommon in canine oral malignant melanomas. Mamm. Genome 2004, 16, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Chu, P.Y.; Pan, S.L.; Liu, C.H.; Lee, J.; Yeh, L.S.; Liao, A.T. KIT gene exon 11 mutations in canine malignant melanoma. Vet. J. 2013, 196, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Curtin, J.A.; Busam, K.; Pinkel, D.; Bastian, B.C. Somatic activation of KIT in distinct subtypes of melanoma. J. Clin. Oncol. 2006, 24, 4340–4346. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, J.L.; Fridlyand, J.; Patel, H.; Jain, A.N.; Busam, K.; Kageshita, T.; Ono, T.; Albertson, D.G.; Pinkel, D.; Bastian, B.C. Determinants of BRAF mutations in primary melanomas. J. Natl. Cancer Inst. 2003, 95, 1878–1890. [Google Scholar] [CrossRef] [PubMed]
- Murakami, A.; Mori, T.; Sakai, H.; Murakami, M.; Yanai, T.; Hoshino, Y.; Maruo, K. Analysis of KIT expression and KIT exon 11 mutations in canine oral malignant melanomas. Vet. Comp. Oncol. 2011, 9, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Zebary, A.; Jangard, M.; Omholt, K.; Ragnarsson-Olding, B.; Hansson, J. KIT, NRAS and BRAF mutations in sinonasal melanoma. Br. J. Cancer 2013, 109, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Goel, V.K.; Lazar, A.J.; Warneke, C.L.; Redston, M.S.; Haluska, F.G. Examination of mutations in BRAF, NRAS, and PTEN in primary cutaneous melanoma. J. Investig. Dermatol. 2006, 126, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, H.; Kennedy, K.; Shapiro, S.G.; Breen, M. BRAF Mutations in Canine Cancers. PLoS ONE 2015. [Google Scholar] [CrossRef] [PubMed]
- Bergman, P.J. Canine Oral Melanoma. Clin. Tech. Small Anim. Pract. 2007, 22, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Todoroff, R.J.; Brodey, R.S. Oral and pharyngeal neoplasia in the dog: A retrospective survey of 361 cases. J. Am. Vet. Med. Assoc. 1979, 175, 567–571. [Google Scholar] [PubMed]
- Vos, J.H.; Gaag, I.V.D. Canine and feline oral-pharyngeal tumours. J. Vet. Med. 1987, 34, 420–427. [Google Scholar] [CrossRef]
- Guerra, J.L.; Dagli, M.L.; Godoy, L.F.; Birman, E.G. A retrospective study of oral neoplasms in dogs: A survey from 1941 to 1986. Rev. Fac. Med. Vet. Zootec. Univ. S. Paulo 1989, 26, 207–212. [Google Scholar]
- Stopiglia, A.J.; Felizzola, C.R.; Dagli, M.L.Z.; Xavier, J.G.; Guerra, J.L.; Birman, E. Estudo clínico e anátomo-patológico das formações neoplásicas e não neoplásicas da cavidade bucal de cães. Comun. Cient. Fac. Med. Vet. Zootec. USP 1992, 16, 33–39. [Google Scholar]
- Ghirelli, C.D.O. In Biblioteca Digital USP. Available online: http://www.teses.usp.br/teses/disponiveis/10/10137/tde-22072008-090727/pt-br.php (assecced on 15 November 2015).
- Requicha, J.F.M.F. Repositório Universidade de Trás-os-Montes e Alto Douro. Available online: https://repositorio.utad.pt/bitstream/10348/711/1/MsC_jfmfrequicha.pdf (accessed on 15 November 2015).
- Bronden, L.B.; Eriksen, T.; Kristensen, A.T. Oral malignant melanomas and other head and neck neoplasms in Danish dogs-data from the Danish Veterinary Cancer Registry. Acta Vet. Scand. 2009, 51, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Liptak, J.M.; Withrow, S.J. Cancer of gastrointestinal tract. In Small Animal Clinical Oncology, 5th ed.; Withrow, S.J., Vail, D.M., Page, R.L., Eds.; Elsevier Saunders: St. Louis, MO, USA, 2013; pp. 381–395. [Google Scholar]
- McEntee, M.C. Clinical behavior of nonodontogenic tumors. In Oral and Maxillofacial Surgery in Dogs and Cats; Verstraete, F.J.M., Lommer, M.J., Eds.; Elsevier Saunders: Pennsylvania, PA, USA, 2012; pp. 387–402. [Google Scholar]
- Dennis, M.; Ehrhart, N.; Duncan, C.; Barnes, A.; Ehrhart, E. Frequency of and risk factors associated with lingual lesions in dogs: 1196 cases (1995–2004). J. Am. Vet. Med. Assoc. 2006, 228, 1533–1537. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.E.; Packer, R.A. Association between lymph node size and metastasis in dogs with oral malignant melanoma: 100 cases (1987–2001). J. Am. Vet. Med. Assoc. 2003, 222, 1234–1236. [Google Scholar] [CrossRef] [PubMed]
- Esplin, D.G. Survival of dogs following surgical excision of histologically well-differentiated melanocytic neoplasms of the mucous membranes of the lips and oral cavity. Vet. Pathol. 2008, 45, 889–896. [Google Scholar] [CrossRef] [PubMed]
- White, R.A.S.; Jefferies, A.R.; Freedman, L.S. Clinical staging for oropharyngeal malignancies in the dog. J. Small Anim. Pract. 1985, 26, 581–594. [Google Scholar] [CrossRef]
- MacEwen, E.G.; Patnaik, A.K.; Harvey, H.J.; Hayes, A.A.; Matus, R. Canine oral melanoma: Comparison of surgery versus surgery plus Corynebacterium parvum. Cancer Investig. 1986, 4, 397–402. [Google Scholar] [CrossRef]
- Hahn, K.A.; Denicola, D.B.; Richardson, R.C.; Hahn, E.A. Canine oral malignant melanoma: Prognostic utility of an alternative staging system. J. Small Anim. Pract. 1994, 35, 251–256. [Google Scholar] [CrossRef]
- Boston, S.E.; Lu, X.; Culp, W.T.N.; Montinaro, V.; Romanelli, G.; Dudley, R.M.; Liptak, J.M.; Mestrinho, L.A.; Buracco, P. Efficacy of systemic adjuvant therapies administered to dogs after excision of oral malignant melanomas: 151 cases (2001–2012). J. Am. Vet. Med. Assoc. 2014, 245, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Owen, L.N. TNM Classification of Tumours in Domestic Animals; World Health Organization: Geneve, Switzerland, 1980. [Google Scholar]
- Tuohy, J.L.; Selmic, L.E.; Worley, D.R.; Ehrhart, N.P.; Withrow, S.J. Outcome following curative-intent surgery for oral melanoma in dogs: 70 cases (1998–2011). J. Am. Vet. Med. Assoc. 2014, 245, 1266–1273. [Google Scholar] [CrossRef] [PubMed]
- Harvey, H.J.; MacEwen, E.G.; Braun, D.; Patnaik, A.K.; Withrow, S.J.; Jongeward, S. Prognostic criteria for dogs with oral melanoma. J. Am. Vet. Med. Assoc. 1981, 178, 580–582. [Google Scholar] [PubMed]
- Mould, J.R.B.; Petersen-Jones, S.M.; Peruccio, C.; Ratto, A.; Sassani, J.W.; Harbour, J.W. Uveal melanocytic tumors. In Ocular Tumors in Animals and Humans; Peiffer, R.L., Jr., Simons, K.B., Eds.; Iowa State Press: Ames, IA, USA, 2002; pp. 225–282. [Google Scholar]
- Dubielzig, R.R.; Ketring, K.L.; Mclellan, G.J.; Albert, D.M. Veterinary Ocular Pathology: A Comparative Review; W.B. Saunders: Philadelphia, PA, USA, 2010; p. 472. [Google Scholar]
- Wilcock, B.P.; Peiffer, J.R. Morphology and behavior of primary ocular melanomas in 91 dogs. Vet. Pathol. 1986, 23, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Garner, A.; Koornneef, L.; Levene, A.; Collin, J.R. Malignant melanoma of the eyelid skin: Histopathology and behaviour. Br. J. Ophthalmol. 1985, 69, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Conceição, L.F.; Ribeiro, A.P.; Piso, D.Y.T.; Laus, J.L. Considerations about ocular neoplasia of dogs and cats. Cienc. Rural 2010, 40, 2235–2242. [Google Scholar] [CrossRef]
- Lim, L.A.; Madigan, M.C.; Conway, R.M. Conjunctival melanoma: A review of conceptual and treatment advances. Clin. Ophthalmol. 2013, 7, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, D.; Sansom, J.; Scase, T.; Adams, V.; Mellersh, C. Canine Limbal melanoma: 30 cases (1992–2004). Part 1. Signalment, clinical and histological features and pedigree analysis. Vet. Ophthalmol. 2006, 9, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Perlmann, E.; Barros, P.S.M.; Fernandez, L.; Di Cesare, S.; Bakalian, S.; Burnier, M.N., Jr. Histopathological evaluation of pigmented intraocular tumors in dogs. Investig. Ophthalmol. Vis. Sci. 2010, 5, 5159. [Google Scholar]
- Esson, D.; Fahrer, C.; Zarfoss, M.K.; Dubielzig, R.R. Suspected uveal metastasis of a nail bed melanoma in a dog. Vet. Ophthalmol. 2007, 10, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Fineman, M.S.; Eagle, R.C.; Shields, J.A.; Shields, C.L.; Potter, P. Melanocytomalytic glaucoma in eyes with necrotic iris melanocytoma. Ophthalmology 1998, 105, 492–496. [Google Scholar] [CrossRef]
- Ryan, A.M.; Diters, R.W. Clinical and pathologic features of canine ocular melanomas. J. Am. Med. Assoc. 1984, 184, 60–67. [Google Scholar]
- Giuliano, E.A.; Chappell, R.; Fischer, B.; Dubielzig, R.R. A matched observational study of canine survival with primary intraocular melanocytic neoplasia. Vet. Ophthalmol. 1999, 2, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Konrade, K.A.; Hoffman, A.; Schubert, C.S.; Dubielzig, R.R. A histologic series of secondary uveal melanomas in eleven dogs. In Proceedings of the 40th Annual Meeting of the American College of Veterinary Ophthalmologist, Chicago, IL, USA, 4–7 November 2009.
- Willis, A.M.; Wilkie, D.A. Ocular oncology. Clin. Tech. Small Anim. Pract. 2001, 16, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Cazalot, G.; Raymond-Letron, I.; Regnier, A. Choroidal melanoma presented as glaucoma in a dog: Case report and review of the literature. Rev. Med. Vet. 2008, 159, 74–78. [Google Scholar]
- Henry, C.J.; Brewer, W.G.; Whitley, E.M.; Tyler, J.W.; Ogilvie, G.K.; Norris, A.; Fox, L.E.; Morrison, W.B.; Hammer, A.; Vail, D.M.; et al. Canine digital tumors: Veterinary cooperative oncology group retrospective study of 64 dogs. J. Vet. Intern. Med. 2005, 19, 720–724. [Google Scholar] [CrossRef] [PubMed]
- Aronsohn, M.G.; Carpenter, J.L. Distal extremity melanocytic nevi an malignant melanomas in dogs. J. Am. Anim. Hosp. Assoc. 1990, 26, 605–612. [Google Scholar]
- Wobeser, B.K.; Kidney, B.A.; Powers, B.E.; Withrow, S.J.; Mayer, M.N.; Spinato, M.T.; Allen, A.L. Diagnosis and clinical outcomes associated with surgically amputated canine digit submitted to multiple veterinary diagnostic laboratories. Vet. Pathol. 2007, 44, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Manley, C.A.M.; Leibman, N.F.; Wolchok, J.D.; Riviere, I.C.M.; Bartido, S.; Craft, D.M.; Bergman, P.J. Xenogeneic Murine Tyrosinase DNA Vaccine for Malignant Melanoma of the Digit of Dogs. J. Vet. Intern. Med. 2011, 25, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Bostock, D.E. Prognosis after surgical excision of canine melanoma. Vet. Pathol. 1979, 16, 32–40. [Google Scholar] [PubMed]
- Bergman, P.J.; Kent, M.S.; Farese, J.P. Melanoma. In Small Animal Clinical Oncology, 5th ed.; Withrow, S.J., Vail, D.M., Page, R.L., Eds.; Elsevier Saunders: St. Louis, MO, USA, 2013; pp. 321–334. [Google Scholar]
- Brockley, L.K.; Cooper, M.A.; Bennett, P.F. Malignant melanoma in 63 dogs (2001–2011): The effect of carboplatin chemotherapy on survival chemotherapy on survival. N. Z. Vet. J. 2013, 61, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.M. Surgical approach for lymph node staging of oral and maxillofacial neoplasms in dogs. J. Am. Anim. Hosp. Assoc. 1995, 31, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Herring, E.S.; Smith, M.M.; Robertson, J.L. Lymph node staging of oral and maxillofacial neoplasms in 31 dogs and cats. J. Vet. Dent. 2002, 19, 122–126. [Google Scholar] [PubMed]
- Proulx, D.R.; Ruslander, D.M.; Dodge, R.K.; Hauck, M.L.; Williams, L.E.; Horn, B.; Price, G.S.; Thrall, D.E. A retrospective analysis of 140 dogs with oral melanoma treated with external beam radiation. Vet. Radiol. Ultrasound. 2003, 44, 352–359. [Google Scholar] [CrossRef]
- Théon, A.P.; Rodriguez, C.; Madewell, B.R. Analysis of prognostic factors and patterns of failure in dogs with malignant oral tumors treated with megavoltage irradiation. J. Am. Vet. Med. Assoc. 1997, 210, 778–784. [Google Scholar] [PubMed]
- Khan, N.; Mohammad, K.K.; Almasan, A.; Singh, A.D.; Macklis, R. The evolving role of radiation therapy in the management of malignant melanoma. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 645–654. [Google Scholar] [PubMed]
- Bateman, K.E.; Catton, P.A.; Pennock, P.W.; Kruth, S.A. 0-7-21 radiation therapy for the treatment of canine oral melanoma. J. Vet. Intern. Med. 1994, 8, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.; Hayes, A.M.; Blackwood, L.; Maglennon, G.; Pattinson, H.; Sparkes, A.H. Oral malignant melanoma: The effect of coarse fractionation alone or with adjuvant carboplatin therapy. Vet. Comp. Oncol. 2005, 3, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Cancedda, S.; Bley, C.R.; Aresu, L.; Dacasto, M.; Leone, V.F.; Pizzoni, S.; Gracis, M.; Marconato, L. Efficacy and side effects of radiation therapy in comparison with radiation therapy and temozolomide in the treatment of measurable canine malignant melanoma. Vet. Comp. Oncol. 2014. [Google Scholar] [CrossRef] [PubMed]
- Freeman, K.P.; Hahn, K.A.; Harris, F.D.; King, G.K. Treatment of dogs with oral melanoma by hypofractionated radiation therapy and platinum-based chemotherapy (1987–1997). J. Vet. Intern. Med. 2003, 17, 96–101. [Google Scholar] [PubMed]
- Rassnick, K.M.; Ruslender, D.M.; Cotter, S.M.; Al-Sarraf, R.; Bruyette, D.S.; Gamblin, R.M.; Meleo, K.A.; Moore, A.S. Use of carboplatin for treatment of dogs with malignant melanoma: 27 cases (1989–2000). J. Am. Vet. Med. Assoc. 2001, 218, 1444–1448. [Google Scholar] [CrossRef] [PubMed]
- Boria, P.A.; Murry, D.J.; Bennett, P.F.; Glickman, N.W.; Snyder, P.W.; Merkel, B.L.; Schlittler, D.L.; Mutsaers, A.J.; Thomas, R.M.; Knapp, D.W. Evaluation of cisplatin combined with piroxicam for the treatment of oral malignant melanoma and oral squamous cell carcinoma in dogs. J. Am. Vet. Med. Assoc. 2004, 224, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Dank, G.; Rassnick, K.M.; Sokolovsky, Y.; Garrett, L.D.; Post, G.S.; Kitchell, B.E.; Sellon, R.K.; Kleiter, M.; Northrup, N.; Segev, G. Use of adjuvant carboplatin for treatment of dogs with oral malignant melanoma following surgical excision. Vet. Comp. Oncol. 2014, 12, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Bergman, P.J.; Mcknight, J.; Novosad, A.; Charney, S.; Farrelly, J.; Craft, D.; Wulderk, M.; Jeffers, Y.; Sadelain, M.; Hohenhaus, A.E.; et al. Long-term survival of dogs with advanced malignant melanoma after DNA vaccination with xenogeneic human tyrosinase: A phase I trial. Clin. Cancer Res. 2003, 9, 1284–1290. [Google Scholar] [PubMed]
- MacEwen, E.G.; Kurzman, I.D.; Vail, D.M.; Dubielzig, R.R.; Everlith, K.; Madewell, B.R.; Rodriguez, C.O., Jr.; Phillips, B.; Zwahlen, C.H.; Obradovich, J.; et al. Adjuvant therapy for melanoma in dogs: Results of randomized clinical trials using surgery, liposome-encapsulated muramyl triptide, and granulocyte macrophage colony-stimulang factor. Clin. Cancer Res. 1999, 5, 4249–4258. [Google Scholar] [PubMed]
- Moff, S.L.; Corey, G.R.; Gottfredsson, M. Distant cutaneous granulomas after bacille Calmette-Guérin immunotherapy for malignant melanoma: Case for direct infection. Clin. Infect. Dis. 1999, 29, 1569–1570. [Google Scholar] [CrossRef] [PubMed]
- Bianco, S.R.; Sun, J.; Fosmire, S.P.; Hance, K.; Padilla, M.L.; Ritt, M.G.; Getzy, D.M.; Duke, R.C.; Withrow, S.J.; Lana, S.; et al. Enhancing anti melanoma immune responses through apoptosis. Cancer Gene Ther. 2003, 10, 726–736. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.N.; Huelsmeyr, M.K.; Mitzey, A.; Dubielzig, R.R.; Kurzman, I.D.; MacEwen, E.G.; Vail, D.M. Development of an allogenic whole-cell tumor vaccine expressing xenogenic gp100 and implementation in phase II clinical trial in canine patients with malignant melanoma. Cancer Immunol. Immunother. 2006, 55, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Hogge, G.S.; Burkholder, J.K.; Culp, J.; Albertini, M.R.; Dubielzig, R.R.; Keller, E.T.; Yang, N.S.; MacEwen, E.G. Development of human granulocyte-macrophage colony-stimulating factor- transfected tumor cell vaccines for treatment of spontaneous canine cancer. Hum. Gene Ther. 1998, 9, 1851–1861. [Google Scholar] [CrossRef] [PubMed]
- Bergman, P.J.; Wolchok, J.D. Of mice and men (and dogs): Development of a xenogeneic DNA vaccine for canine oral malignant melanoma. Cancer Ther. 2008, 6, 817–826. [Google Scholar]
- Grosenbaugh, D.A.; Leard, A.T.; Bergman, P.J.; Klein, M.K.; Meleo, K.; Susaneck, S.; Hess, P.R.; Jankowski, M.K.; Jones, P.D.; Leibman, N.; et al. Safety and efficacy of a xenogeneic DNA vaccine encoding for human tyrosinase as adjunctive treatment for oral malignant melanoma in dogs following surgical excision of the primary tumor. Am. J. Vet. Res. 2011, 72, 1631–1638. [Google Scholar] [CrossRef] [PubMed]
- Ottnod, J.M.; Smedley, R.C.; Walshaw, R.; Hauptman, J.G.; Kiupel, M.; Obradovich, J.E. A retrospective analysis of the efficacy of Oncept vaccine for the adjunct treatment of canine oral malignant melanoma. Vet. Comp. Oncol. 2013, 11, 219–229. [Google Scholar] [CrossRef]
- Rotte, A.; Bhandaru, M.; Zhou, Y.; Mcelwee, K.J. Immunotherapy of melanoma: Present options and future promises. Cancer Metastasis Rev. 2015, 34, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Gyorffy, S.; Rodriguez-Lecompte, J.C.; Woods, J.P.; Foley, R.; Kruth, S.; Liaw, P.C.; Gauldie, J. Bone marrow-derived dendritic cell vaccination of dogs with naturally occurring melanoma by using human gp100 antigen. J. Vet. Intern. Med. 2005, 19, 56–63. [Google Scholar] [PubMed]
- Tamura, K.; Yamada, M.; Isotani, M.; Arai, H.; Yagihara, H.; Ono, K.; Washizu, T.; Bonkobara, M. Induction of dendritic cell-mediated immune responses against canine malignant melanoma cells. Vet. J. 2008, 175, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Elmslie, R. VRCC Veterinary Speciality & Emergency Hospital. Available online: http://www.vetcancerspecialists.com/blog/2013/1/31/the-controversy-surrounding-the-melanoma-vaccine-for-dogs/ (accesse on 15 November 2015).
- Yokoe, I.; Azuma, K.; Hata, K.; Mukaiyama, T.; Goto, T.; Tsuka, T.; Imagawa, T.; Itoh, N.; Murahata, Y.; Osaki, T.; et al. Clinical systemic lupeol administration for canine oral malignant melanoma. Mol. Clin. Oncol. 2015, 3, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Ribas, A.; Wolchok, J.D.; Hodi, F.S.; Hamid, O.; Kefford, R.; Weber, J.S.; Joshua, A.M.; Hwu, W.J.; Gangadhar, T.C.; et al. Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: A randomised dose-comparison cohort of a phase 1 trial. Lancet 2014, 384, 1109–1117. [Google Scholar] [CrossRef]
- Schadendorf, D.; Hodi, F.S.; Robert, C.; Weber, J.S.; Margolin, K.; Hamid, O.; Patt, D.; Chen, T.T.; Berman, D.M.; Wolchok, J.D. Pooled analysis of long-term survival data from phase II and phase III trials of ipilimumab in unresectable or metastatic melanoma. J. Clin. Oncol. 2015, 33, 1889–1894. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, N.; Konnai, S.; Ikebuchi, R.; Okagawa, T.; Adachi, M.; Takagi, S.; Kagawa, Y.; Nakajima, C.; Suzuki, Y.; Murata, S.; et al. Expression of PD-L1 on canine tumor cells and enhancement of IFN-c production from tumor infiltrating cells by PD-L1 blockade. PLoS ONE 2014. [Google Scholar] [CrossRef] [PubMed]
- Igase, M.; Hwang, C.C.; Coffey, M.; Okuda, M.; Noguchi, S.; Mizuno, T. The oncolytic effects of reovirus in canine solid tumor cell lines. J. Vet. Med. Sci. 2015, 77, 541–548. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sites/Total Number of Cases | n = 1652 | n = 143 | n = 209 |
|---|---|---|---|
| Oral | 1026 | 57 | 67 |
| Cutaneous | 448 | 44 | 88 |
| Scrotum | - | 4 | - |
| Digit | 94 | 21 | - |
| Ungual | 60 | - | - |
| Ocular | 24 | 17 | - |
| Lips/Feet | - | - | 54 |
| Reference | Gillard et al., 2014 [19] | Teixeira et al., 2010 [13] | Spangler and Kass, 2006 [18] |
| Human | Dog | |
|---|---|---|
| BRAF | 4% [50], 2% [48], 6% [14] | 0% [6,19] |
| C-KIT | 12.5% [16], 4% [50] | 0% [49] |
| NRAS | 22% [15], 14% [50], 10% [14] | 6% [19] |
| PTEN | 48.1% [15] | 4% [19] |
| GNAQ | 0% [16] | 0% [19] |
| CDK4 | 0% [17] | 0% [19] |
| Clinical Staging System for Oral Tumor | |||
|---|---|---|---|
| Primary Tumor (T) | |||
| Tis | Tumor in situ | ||
| T1 | Tumor <2 cm in diameter at greatest dimension | ||
| T1a | Without evidence of bone invasion | ||
| T1b | With evidence of bone invasion | ||
| T2 | Tumor 2–4 cm in diameter at greatest dimension | ||
| T2a | Without evidence of bone invasion | ||
| T2b | With evidence of bone invasion | ||
| T3 | Tumor >4 cm in diameter at greatest dimension | ||
| T3a | Without evidence of bone invasion | ||
| T3b | With evidence of bone invasion | ||
| Regional Lymph Nodes (N) | |||
| N0 | No regional lymph node metastasis | ||
| N1 | Movable ipsilateral lymph nodes | ||
| N1a | No evidence of lymph mode metastasis | ||
| N1b | Evidence of lymph mode metastasis | ||
| N2 | Movable contralateral lymph nodes | ||
| N2a | No evidence of lymph mode metastasis | ||
| N2b | Evidence of lymph mode metastasis | ||
| N3 | Fixed lymph nodes | ||
| Metastasis (M) | |||
| M0 | No distance metastasis | ||
| M1 | Distance metastasis | ||
| Stage Group | Tumor (T) | Nodes (N) | Metastasis (M) |
| I | T1 | N0, N1a, N2a | M0 |
| II | T2 | N0, N1a, N2a | M0 |
| III | T3 | N0, N1a, N2a | M0 |
| Any T | N1b | M0 | |
| IV | Any T | N2b, N3 | M0 |
| Any T | Any N | M0 | |
| Summary of Treatment Outcome for Canine Oral Malignant Melanoma |
|---|
| Radiation Therapy (RT) |
|
| References: Theon et al., 1997 (98); Bateman et al., 1994 (100); Murphy et al., 2005 (101); Cancedda et al., 2014 (102); Proulx et al., 2003 (97); Freeman et al., 2003 (103). |
| Surgery (SX) with Wide Margins |
|
| References: Tuohy et al., 2014 (71); Boston et al., 2014 (69); Esplin et al., 2008 (65). |
| Chemotherapy (CT) for Macroscopic Disease |
|
| References: Rassnick et al., 2001 (104); Boria et al., 2004 (105). |
| Adequate Local Treatment + Systemic Therapy |
|
| References: Dank et al., 2012 (106); Tuohy et al., 2014 (71); Boston et al., 2014 (69); Cancedda et al., 2014 (102); Freeman et al., 2003 (103). |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishiya, A.T.; Massoco, C.O.; Felizzola, C.R.; Perlmann, E.; Batschinski, K.; Tedardi, M.V.; Garcia, J.S.; Mendonça, P.P.; Teixeira, T.F.; Zaidan Dagli, M.L. Comparative Aspects of Canine Melanoma. Vet. Sci. 2016, 3, 7. https://doi.org/10.3390/vetsci3010007
Nishiya AT, Massoco CO, Felizzola CR, Perlmann E, Batschinski K, Tedardi MV, Garcia JS, Mendonça PP, Teixeira TF, Zaidan Dagli ML. Comparative Aspects of Canine Melanoma. Veterinary Sciences. 2016; 3(1):7. https://doi.org/10.3390/vetsci3010007
Chicago/Turabian StyleNishiya, Adriana Tomoko, Cristina Oliveira Massoco, Claudia Ronca Felizzola, Eduardo Perlmann, Karen Batschinski, Marcello Vannucci Tedardi, Jéssica Soares Garcia, Priscila Pedra Mendonça, Tarso Felipe Teixeira, and Maria Lucia Zaidan Dagli. 2016. "Comparative Aspects of Canine Melanoma" Veterinary Sciences 3, no. 1: 7. https://doi.org/10.3390/vetsci3010007