
Artificial Intelligence Models in the Diagnosis of Adult-Onset Dementia Disorders: A Review

 ,
,  , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Document Search
2.2. Inclusion and Exclusion Criteria
2.3. Quality Assessment
3. Results
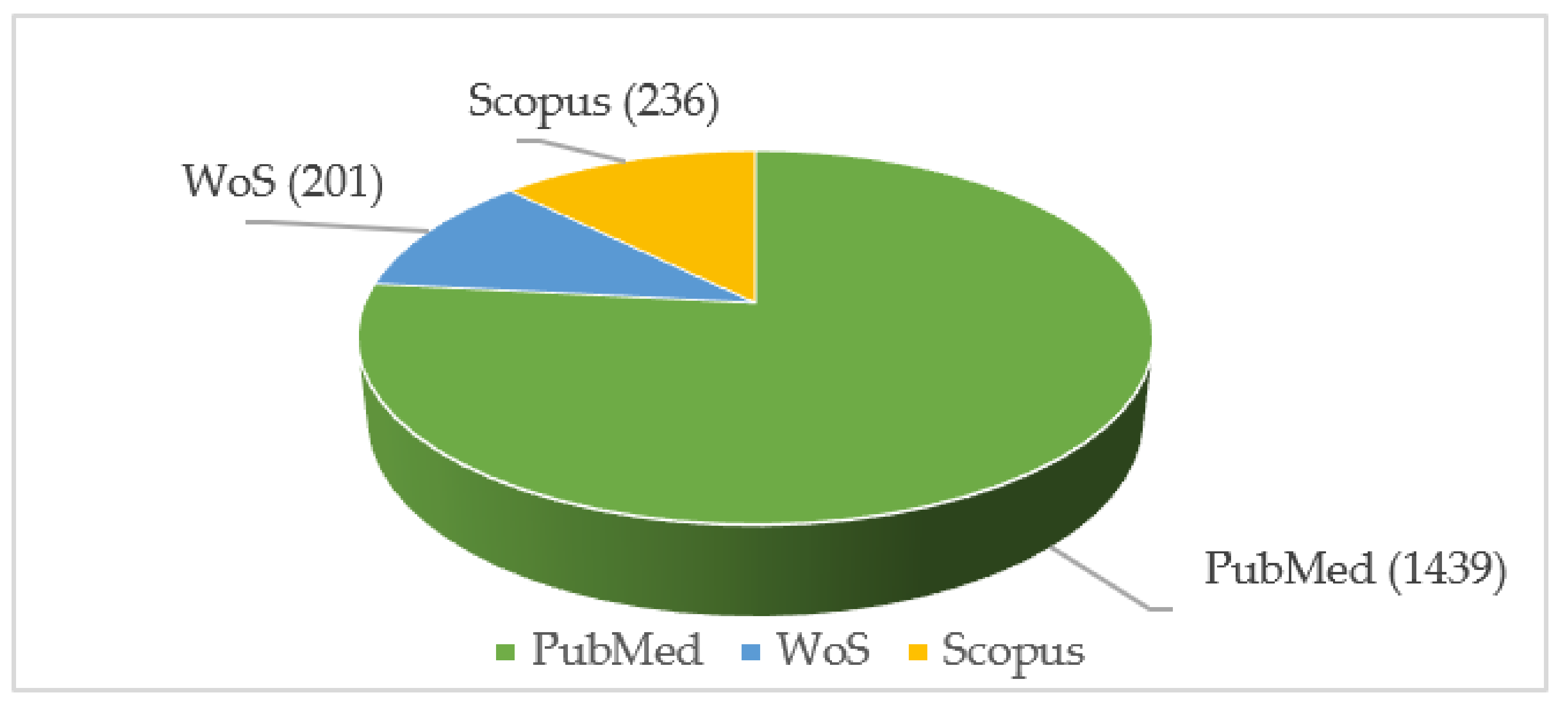
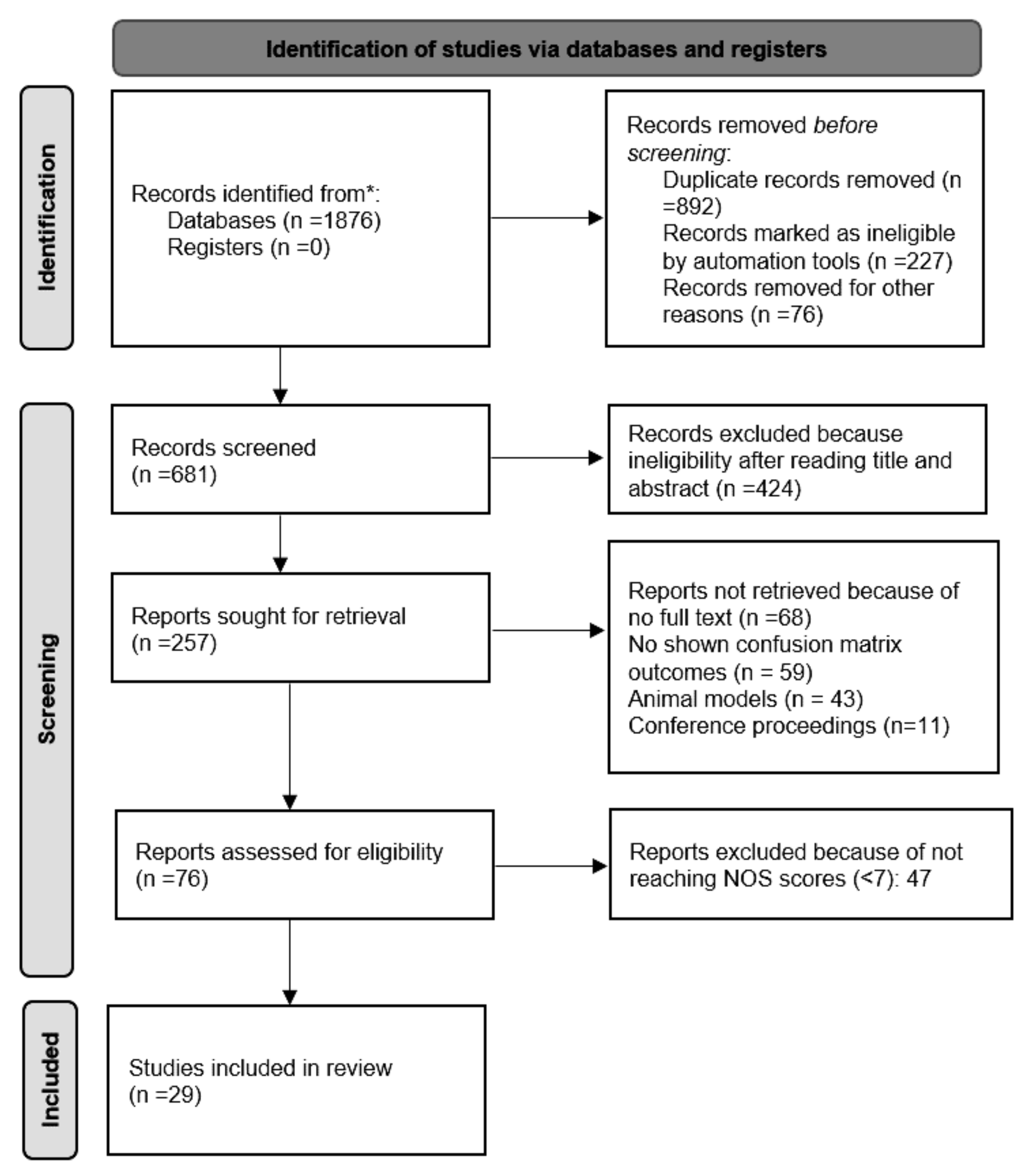
3.1. Search Outcomes
3.2. Study Characteristics
4. Discussion
4.1. AI for Diagnostic Purposes
- A.
- MCI detection
- B.
- AD diagnosis
- C.
- Frontotemporal (FTD) and Lewy bodies (LBD) dementia
- D.
- PD diagnosis
4.2. Model Assessment
4.3. Research Implications
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Harrison, R.A.; Kesler, S.R.; Johnson, J.M.; Penas-Prado, M.; Sullaway, C.M.; Wefel, J.S. Neurocognitive dysfunction in adult cerebellar medulloblastoma. Psycho-Oncology 2019, 28, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.J.; Zhao, Z.; Shen, H.R.; Bing, Q.; Li, N.; Guo, X.; Hu, J. Adolescent/adult-onset homocysteine remethylation disorders characterized by gait disturbance with/without psychiatric symptoms and cognitive decline: A series of seven cases. Neurol. Sci. 2021, 42, 1987–1993. [Google Scholar] [CrossRef]
- Dubois, B.; Villain, N.; Frisoni, G.B.; Rabinovici, G.D.; Sabbagh, M.; Cappa, S.; Bejanin, A.; Bombois, S.; Epelbaum, S.; Teichmann, M.; et al. Clinical diagnosis of Alzheimer’s disease: Recommendations of the International Working Group. Lancet. Neurol. 2021, 20, 484–496. [Google Scholar] [CrossRef]
- Spiegel, D.; Lewis-Ferńandez, R.; Lanius, R.; Vermetten, E.; Simeon, D.; Friedman, M. Dissociative disorders in DSM-5. Annu. Rev. Clin. Psychol. 2013, 9, 299–326. [Google Scholar] [CrossRef] [PubMed]
- Gnerre, P.; La Regina, M.; Bozzano, C.; Pomero, F.; Re, R.; Meschi, M.; Montemurro, D.; Marchetti, A.; Di Lillo, M.; Tirotta, D. Delirium: The invisible syndrome. Ital. J. Med. 2016, 10, 119–127. [Google Scholar] [CrossRef]
- Bhat, R.; Rockwood, K. Delirium as a disorder of consciousness. J. Neurol. Neurosurg. Psychiatry 2007, 78, 1167. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.E.; Bondi, M.W. Mild Cognitive Impairment and Dementia: Definitions, Diagnosis, and Treatment; Oxford University Press: Oxford, UK, 2013; Volume 403. [Google Scholar]
- Vahia, V.N. Diagnostic and statistical manual of mental disorders 5: A quick glance. Indian J. Psychiatry. 2013, 55, 220–223. [Google Scholar] [CrossRef]
- Dening, T.; Sandilyan, M.B. Dementia: Definitions and types. Nurs. Stand. 2015, 29, 37–42. [Google Scholar] [CrossRef]
- Aarsland, D. Epidemiology and Pathophysiology of Dementia-Related Psychosis. J. Clin. Psychiatry 2020, 81, 27625. [Google Scholar] [CrossRef]
- Ferencz, B.; Gerritsen, L. Genetics and Underlying Pathology of Dementia. Neuropsychol. Rev. 2015, 25, 113–124. [Google Scholar] [CrossRef]
- Ingelsson, M.; Fukumoto, H.; Newell, K.L.; Growdon, J.H.; Hedley-Whyte, E.T.; Frosch, M.P.; Albert, M.S.; Hyman, B.T.; Irizarry, M.C. Early Abeta accumulation and progressive synaptic loss, gliosis, and tangle formation in AD brain. Neurology 2004, 62, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Pozo, A.; Mielke, M.L.; Gómez-Isla, T.; Betensky, R.A.; Growdon, J.H.; Frosch, M.P.; Hyman, B.T. Reactive glia not only associates with plaques but also parallels tangles in Alzheimer’s disease. Am. J. Pathol. 2011, 179, 1373–1384. [Google Scholar] [CrossRef]
- Serrano-Pozo, A.; Frosch, M.P.; Masliah, E.; Hyman, B.T. Neuropathological Alterations in Alzheimer Disease. Cold Spring Harb. Perspect. Med. 2011, 1, a006189. [Google Scholar] [CrossRef]
- Wisniewski, H.M.; Silverman, W. Diagnostic criteria for the neuropathological assessment of Alzheimer’s disease: Current status and major issues. Neurobiol. Aging 1997, 18, S43–S50. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef]
- Maki, Y.; Yamaguchi, H. Early detection of dementia in the community under a community-based integrated care system. Geriatr. Gerontol. Int. 2014, 14, 2–10. [Google Scholar] [CrossRef]
- Arevalo-Rodriguez, I.; Smailagic, N.; Roqué-Figuls, M.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Bonfill Cosp, X.; Cullum, S. Mini-Mental State Examination (MMSE) for the early detection of dementia in people with mild cognitive impairment (MCI). Cochrane Database Syst. Rev. 2021, 7, CD010783. [Google Scholar] [CrossRef]
- Battineni, G.; Hossain, M.A.; Chintalapudi, N.; Traini, E.; Dhulipalla, V.R.; Ramasamy, M.; Amenta, F. Improved Alzheimer’s Disease Detection by MRI Using Multimodal Machine Learning Algorithms. Diagnostics 2021, 11, 2103. [Google Scholar] [CrossRef]
- Carotenuto, A.; Traini, E.; Fasanaro, A.M.; Battineni, G.; Amenta, F. Tele-Neuropsychological Assessment of Alzheimer’s Disease. J. Pers. Med. 2021, 11, 688. [Google Scholar] [CrossRef] [PubMed]
- Woźniacka, A.; Patrzyk, S.; Mikołajczyk, M. Artificial intelligence in medicine and dermatology. Postep. Dermatol. Alergol. 2021, 38, 948–952. [Google Scholar] [CrossRef]
- James, C.; Ranson, J.M.; Everson, R.; Llewellyn, D.J. Performance of Machine Learning Algorithms for Predicting Progression to Dementia in Memory Clinic Patients. JAMA Netw. Open 2021, 4, e2136553. [Google Scholar] [CrossRef] [PubMed]
- Herraiz, Á.H.; Martínez-Rodrigo, A.; Bertomeu-González, V.; Quesada, A.; Rieta, J.J.; Alcaraz, R. A Deep Learning Approach for Featureless Robust Quality Assessment of Intermittent Atrial Fibrillation Recordings from Portable and Wearable Devices. Entropy 2020, 22, 733. [Google Scholar] [CrossRef] [PubMed]
- Gaubert, S.; Houot, M.; Raimondo, F.; Ansart, M.; Corsi, M.C.; Naccache, L.; Sitt, J.D.; Habert, M.O.; Dubois, B.; De Vico Fallani, F.; et al. A machine learning approach to screen for preclinical Alzheimer’s disease. Neurobiol. Aging 2021, 105, 205–216. [Google Scholar] [CrossRef]
- Tsang, G.; Xie, X.; Zhou, S.M. Harnessing the Power of Machine Learning in Dementia Informatics Research: Issues, Opportunities, and Challenges. IEEE Rev. Biomed. Eng. 2020, 13, 113–129. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Oh, I.; Schindler, S.; Lai, A.M.; Payne, P.R.O.; Gupta, A. Machine learning for modeling the progression of Alzheimer disease dementia using clinical data: A systematic literature review. JAMIA Open 2021, 4, ooab052. [Google Scholar] [CrossRef]
- Agarwal, D.; Marques, G.; De la Torre-Díez, I.; Franco Martin, M.A.; García Zapiraín, B.; Martín Rodríguez, F. Transfer Learning for Alzheimer’s Disease through Neuroimaging Biomarkers: A Systematic Review. Sensors 2021, 21, 7259. [Google Scholar] [CrossRef]
- Merkin, A.; Krishnamurthi, R.; Medvedev, O.N. Machine learning, artificial intelligence and the prediction of dementia. Curr. Opin. Psychiatry 2022, 35, 123–129. [Google Scholar] [CrossRef]
- Landolfi, A.; Ricciardi, C.; Donisi, L.; Cesarelli, G.; Troisi, J.; Vitale, C.; Barone, P.; Amboni, M. Machine Learning Approaches in Parkinson’s Disease. Curr. Med. Chem. 2021, 28, 6548–6568. [Google Scholar] [CrossRef]
- Savage, N. How AI and neuroscience drive each other forwards. Nature 2019, 571, S15–S17. [Google Scholar] [CrossRef]
- Fan, J.; Fang, L.; Wu, J.; Guo, Y.; Dai, Q. From brain science to artificial intelligence. Engineering 2020, 6, 248–252. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Goenka, N.; Tiwari, S. AlzVNet: A volumetric convolutional neural network for multiclass classification of Alzheimer’s disease through multiple neuroimaging computational approaches. Biomed. Signal Process. Control 2022, 74, 103500. [Google Scholar] [CrossRef]
- Helaly, H.A.; Badawy, M.; Haikal, A.Y. Deep Learning Approach for Early Detection of Alzheimer’s Disease. Cognit. Comput. 2021, 1, 1–17. [Google Scholar] [CrossRef]
- Pan, D.; Zeng, A.; Jia, L.; Huang, Y.; Frizzell, T.; Song, X. Early Detection of Alzheimer’s Disease Using Magnetic Resonance Imaging: A Novel Approach Combining Convolutional Neural Networks and Ensemble Learning. Front. Neurosci. 2020, 14, 259. [Google Scholar] [CrossRef]
- Hazarika, R.A.; Kandar, D.; Maji, A.K. An experimental analysis of different Deep Learning based Models for Alzheimer’s Disease classification using Brain Magnetic Resonance Images. J. King Saud Univ.-Comput. Inf. Sci. 2021. In Press. [Google Scholar] [CrossRef]
- Mathotaarachchi, S.; Pascoal, T.A.; Shin, M.; Benedet, A.L.; Kang, M.S.; Beaudry, T.; Fonov, V.S.; Gauthier, S.; Rosa-Neto, P. Identifying incipient dementia individuals using machine learning and amyloid imaging. Neurobiol. Aging 2017, 59, 80–90. [Google Scholar] [CrossRef]
- Naganandhini, S.; Shanmugavadivu, P. Effective Diagnosis of Alzheimer’s Disease using Modified Decision Tree Classifier. Procedia Comput. Sci. 2019, 165, 548–555. [Google Scholar] [CrossRef]
- Boutet, A.; Madhavan, R.; Elias, G.J.B.; Joel, S.E.; Gramer, R.; Ranjan, M.; Paramanandam, V.; Xu, D.; Germann, J.; Loh, A.; et al. Predicting optimal deep brain stimulation parameters for Parkinson’s disease using functional MRI and machine learning. Nat. Commun. 2021, 12, 3043. [Google Scholar] [CrossRef]
- Fei, Z.; Yang, E.; Yu, L.; Li, X.; Zhou, H.; Zhou, W. A Novel deep neural network-based emotion analysis system for automatic detection of mild cognitive impairment in the elderly. Neurocomputing 2022, 468, 306–316. [Google Scholar] [CrossRef]
- Kang, M.J.; Kim, S.Y.; Na, D.L.; Kim, B.C.; Yang, D.W.; Kim, E.J.; Na, H.R.; Han, H.J.; Lee, J.H.; Kim, J.H.; et al. Prediction of cognitive impairment via deep learning trained with multi-center neuropsychological test data. BMC Med. Inform. Decis. Mak. 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Xue, C.; Karjadi, C.; Paschalidis, I.C.; Au, R.; Kolachalama, V.B. Detection of dementia on voice recordings using deep learning: A Framingham Heart Study. Alzheimer’s Res. Ther. 2021, 13, 1–15. [Google Scholar] [CrossRef] [PubMed]
- El-Sappagh, S.; Alonso, J.M.; Islam, S.M.R.; Sultan, A.M.; Kwak, K.S. A multilayer multimodal detection and prediction model based on explainable artificial intelligence for Alzheimer’s disease. Sci. Rep. 2021, 11, 2660. [Google Scholar] [CrossRef] [PubMed]
- Battineni, G.; Chintalapudi, N.; Amenta, F.; Traini, E. A Comprehensive Machine-Learning Model Applied to Magnetic Resonance Imaging (MRI) to Predict Alzheimer’s Disease (AD) in Older Subjects. J. Clin. Med. 2020, 9, 2146. [Google Scholar] [CrossRef]
- Venugopalan, J.; Tong, L.; Hassanzadeh, H.R.; Wang, M.D. Multimodal deep learning models for early detection of Alzheimer’s disease stage. Sci. Rep. 2021, 11, 3254. [Google Scholar] [CrossRef]
- Herzog, N.J.; Magoulas, G.D. Brain asymmetry detection and machine learning classification for diagnosis of early dementia. Sensors 2021, 21, 778. [Google Scholar] [CrossRef]
- Bron, E.E.; Steketee, R.M.E.; Houston, G.C.; Oliver, R.A.; Achterberg, H.C.; Loog, M.; Van Swieten, J.C.; Hammers, A.; Niessen, W.J.; Smits, M.; et al. Diagnostic classification of arterial spin labeling and structural MRI in presenile early stage dementia. Hum. Brain Mapp. 2014, 35, 4916–4931. [Google Scholar] [CrossRef]
- Pekkala, T.; Hall, A.; Lötjönen, J.; Mattila, J.; Soininen, H.; Ngandu, T.; Laatikainen, T.; Kivipelto, M.; Solomon, A. Development of a late-life dementia prediction index with supervised machine learning in the population-based CAIDE study. J. Alzheimer’s Dis. 2017, 55, 1055–1067. [Google Scholar] [CrossRef]
- Byeon, H. Application of machine learning technique to distinguish parkinson’s disease dementia and alzheimer’s dementia: Predictive power of parkinson’s disease-related non-motor symptoms and neuropsychological profile. J. Pers. Med. 2020, 10, 31. [Google Scholar] [CrossRef]
- Miltiadous, A.; Tzimourta, K.D.; Giannakeas, N.; Tsipouras, M.G.; Afrantou, T.; Ioannidis, P.; Tzallas, A.T. Alzheimer’s disease and frontotemporal dementia: A robust classification method of eeg signals and a comparison of validation methods. Diagnostics 2021, 11, 1437. [Google Scholar] [CrossRef] [PubMed]
- Danso, S.O.; Zeng, Z.; Muniz-Terrera, G.; Ritchie, C.W. Developing an Explainable Machine Learning-Based Personalised Dementia Risk Prediction Model: A Transfer Learning Approach With Ensemble Learning Algorithms. Front. Big Data 2021, 4, 21. [Google Scholar] [CrossRef] [PubMed]
- Juutinen, M.; Wang, C.; Zhu, J.; Haladjian, J.; Ruokolainen, J.; Puustinen, J.; Vehkaoja, A. Parkinson’s disease detection from 20-step walking tests using inertial sensors of a smartphone: Machine learning approach based on an observational case-control study. PLoS ONE 2020, 15, e0236258. [Google Scholar] [CrossRef] [PubMed]
- Sabry, F.; Eltaras, T.; Labda, W.; Alzoubi, K.; Malluhi, Q. Machine Learning for Healthcare Wearable Devices: The Big Picture. J. Healthc. Eng. 2022, 2022, 4653923. [Google Scholar] [CrossRef]
- Ghoraani, B.; Boettcher, L.N.; Hssayeni, M.D.; Rosenfeld, A.; Tolea, M.I.; Galvin, J.E. Detection of Mild Cognitive Impairment and Alzheimer’s Disease using Dual-task Gait Assessments and Machine Learning Behnaz. Physiol. Behav. 2021, 176, 100–106. [Google Scholar] [CrossRef]
- Shimoda, A.; Li, Y.; Hayashi, H.; Kondo, N. Dementia risks identified by vocal features via telephone conversations: A novel machine learning prediction model. PLoS ONE 2021, 16, e0253988. [Google Scholar] [CrossRef]
- Boettcher, L.N.; Hssayeni, M.; Rosenfeld, A.; Tolea, M.I.; Galvin, J.E.; Ghoraani, B. Dual-Task Gait Assessment and Machine Learning for Early- detection of Cognitive Decline. Physiol. Behav. 2020, 176, 139–148. [Google Scholar] [CrossRef]
- Alzheimer’s Association. 2016 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2016, 12, 459–509. [Google Scholar] [CrossRef]
- WHO. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Signaevsky, M.; Marami, B.; Prastawa, M.; Tabish, N.; Iida, M.A.; Zhang, X.F.; Sawyer, M.; Duran, I.; Koenigsberg, D.G.; Bryce, C.H.; et al. Antemortem detection of Parkinson’s disease pathology in peripheral biopsies using artificial intelligence. Acta Neuropathol. Commun. 2022, 10, 21. [Google Scholar] [CrossRef]
- Lee, G.; Nho, K.; Kang, B.; Sohn, K.A.; Kim, D.; Weiner, M.W.; Aisen, P.; Petersen, R.; Jack, C.R.; Jagust, W.; et al. Predicting Alzheimer’s disease progression using multi-modal deep learning approach. Sci. Rep. 2019, 9, 1952. [Google Scholar] [CrossRef]
- Almubark, I.; Chang, L.C.; Shattuck, K.F.; Nguyen, T.; Turner, R.S.; Jiang, X. A 5-min Cognitive Task With Deep Learning Accurately Detects Early Alzheimer’s Disease. Front. Aging Neurosci. 2020, 12, 450. [Google Scholar] [CrossRef] [PubMed]
- Fulton, L.V.; Dolezel, D.; Harrop, J.; Yan, Y.; Fulton, C.P. Classification of alzheimer’s disease with and without imagery using gradient boosted machines and resnet-50. Brain Sci. 2019, 9, 212. [Google Scholar] [CrossRef] [PubMed]
- Odusami, M.; Maskeliūnas, R.; Damaševičius, R. An Intelligent System for Early Recognition of Alzheimer’s Disease Using Neuroimaging. Sensors 2022, 22, 740. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Hampel, H.; Feldman, H.H.; Scheltens, P.; Aisen, P.; Andrieu, S.; Bakardjian, H.; Benali, H.; Bertram, L.; Blennow, K.; et al. Preclinical Alzheimer’s disease: Definition, natural history, and diagnostic criteria. Alzheimer’s Dement. 2016, 12, 292–323. [Google Scholar] [CrossRef]
- Scheltens, P.; Blennow, K.; Breteler, M.M.B.; De Strooper, B.; Frisoni, G.B.; Salloway, S.; Van der Flier, W.M. Alzheimer’s disease. Lancet 2016, 388, 505–517. [Google Scholar] [CrossRef]
- Drury-Ruddlesden, J.; Health, I. Rehabilitation in Advanced Dementia through Computer-Assisted Exergaming with Able-X: A Collective Case Study. Ph.D. Thesis, Victoria University of Wellington, Wellington, New Zealand, 2017. [Google Scholar] [CrossRef]
- Hu, J.; Qing, Z.; Liu, R.; Zhang, X.; Lv, P.; Wang, M.; Wang, Y.; He, K.; Gao, Y.; Zhang, B. Deep Learning-Based Classification and Voxel-Based Visualization of Frontotemporal Dementia and Alzheimer’s Disease. Front. Neurosci. 2021, 14, 1468. [Google Scholar] [CrossRef]
- García-Gutierrez, F.; Díaz-Álvarez, J.; Matias-Guiu, J.A.; Pytel, V.; Matías-Guiu, J.; Cabrera-Martín, M.N.; Ayala, J.L. GA-MADRID: Design and validation of a machine learning tool for the diagnosis of Alzheimer’s disease and frontotemporal dementia using genetic algorithms. Med. Biol. Eng. Comput. 2022, 1, 1–20. [Google Scholar] [CrossRef]
- Bougea, A.; Efthymiopoulou, E.; Spanou, I.; Zikos, P. A Novel Machine Learning Algorithm Predicts Dementia With Lewy Bodies Versus Parkinson’s Disease Dementia Based on Clinical and Neuropsychological Scores. J. Geriatr. Psychiatry Neurol. 2022, 35, 317–320. [Google Scholar] [CrossRef]
- Galvin, J.E.; Chrisphonte, S.; Cohen, I.; Greenfield, K.K.; Kleiman, M.J.; Moore, C.; Riccio, M.L.; Rosenfeld, A.; Shkolnik, N.; Walker, M.; et al. Characterization of dementia with Lewy bodies (DLB) and mild cognitive impairment using the Lewy body dementia module (LBD-MOD). Alzheimer’s Dement. 2021, 17, 1675–1686. [Google Scholar] [CrossRef]
- Ni, Y.C.; Tseng, F.P.; Pai, M.C.; Hsiao, I.T.; Lin, K.J.; Lin, Z.K.; Lin, C.Y.; Chiu, P.Y.; Hung, G.U.; Chang, C.C.; et al. The Feasibility of Differentiating Lewy Body Dementia and Alzheimer’s Disease by Deep Learning Using ECD SPECT Images. Diagnostics 2021, 11, 2091. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Database | Query |
|---|---|
| PubMed | English AND (“Artificial Intelligence” [Title/Abstract/MeSH] OR “Machine Learning”[Title/Abstract/MeSH]) OR “Deep learning” AND (“diagnosis”[Title/Abstract] OR “detection”[Title/Abstract] OR “identification”[Title/Abstract] OR “recognition”[Title/Abstract]) OR “interpretation”[Title/Abstract]) AND (“dementia”[All Fields] AND “MRI”[All Fields]) AND “PET” [All Fields]) AND “image data”[All Fields]) NOT “classification” [Title/Abstract/MeSH] NOT “ranking”[Title/Abstract/MeSH] NOT “grouping”[Title/Abstract/MeSH] NOT Review[ptyp] NOT books and Documents [ptyp] NOT conference [ptyp] |
| WoS | (“AI” AND “Artificial Intelligence” AND “Machine Learning” AND “Deep Learning”) AND (“Diagnosis” OR “Identification” OR “recognition”) AND (“dementia” OR “Alzheimer’s disease” OR “MRI” OR “PET” OR “medical imaging” OR “neuro”) NOT “segmentation” NOT “functional” NOT “connectivity”) AND LANGUAGE: (English) AND DOCUMENT TYPES: (Review OR Proceedings Paper) |
| Scopus | TITLE-ABS-KEY (“Artificial Intelligence” AND “Machine Learning” AND “Deep Learning”) AND (“Diagnosis” OR “Identification” OR “recognition” OR “interpretation) AND (“neurological diseases” OR “neurogenerative disorders” OR “dementia” OR “MRI” OR “PET”) AND LIMIT-TO (LANGUAGE, “English”) AND (LIMIT-TO (EXACT KEYWORD, “dementia”) |
| N | Country | Study Cohort | Dementia Category | AI Model | AI Modality | Validation Methods | Accuracy | Sensitivity | Specificity | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Canada | Prospective | AD | RUSRF | PET, MRI | Independent test set | 84% | 70.8% | 86.5% | [39] |
| 2 | UK, China | Retrospective | MCI, Dementia | MobileNet, SVM | Facial expressions | 5-fold cross-validation | 73.3% | N/A | N/A | [42] |
| 3 | India | Retrospective | AD | DNN, Inception-V1, V2, V3, Residual Networks, DenseNet | MRI | Independent test set | 90.22% | N/A | N/A | [38] |
| 4 | India | Retrospective | AD | CNN | MRI | Independent test set | 98.3% | 97% | N/A | [35] |
| 5 | India | Retrospective | AD | DTC-HPT | MRI | Independent test set | 99% | 99.10% | N/A | [40] |
| 6 | Egypt | Retrospective | AD | CNN | MRI | 10-fold cross-validation | 97% | 95% | N/A | [36] |
| 7 | USA | Retrospective | AD | ResNet-50, GBM | MRI | 10-fold cross-validation | 99% | N/A | N/A | [64] |
| 8 | USA | Retrospective | AD | MLP | Cognitive data | Independent test set | 92.98% | 93.75% | 92.68% | [63] |
| 9 | Canada | Retrospective | AD | CNN | MRI | 5-fold cross-validation | 84% | N/A | N/A | [37] |
| 10 | South Korea | Retrospective | MCI, Dementia | ANN | NPT data | 10-fold cross-validation | 96.66% | 96% | 96.8% | [43] |
| 11 | USA | Prospective | Dementia | LSTM, CNN | Voice Data | 5-fold cross-validation | 74% | 66.3% | 84.7% | [44] |
| 12 | USA | Prospective | PD | CNN | WSI | Cross-validation | 99% | 99% | 99% | [61] |
| 13 | USA | Prospective | AD | RNN | MRI | 5-fold cross-validation | 81% | 84% | 80%% | [62] |
| 14 | Lithuania | Retrospective | AD | ResNet18, DenseNet201 | MRI | Cross-validation | 98.86% | 98.89% | N/A | [65] |
| 15 | Canada | Prospective | PD | ML model | MRI | Independent test set/ 5-fold cross-validation | 88% | N/A | N/A | [41] |
| 16 | Spain | Retrospective | AD | RF | MRI | Cross-validation | 94.4% | N/A | N/A | [45] |
| 17 | Greece | Retrospective | AD and Frontotemporal Dementia | DT, RF, ANN, SVM, Naïve Bayes, and KNN | EEG | 10-fold and leave-one-patient-out cross-validation | 80% (DT)–99.1% (RF) | 94% (NB)–98.6% (RF) | 58% (NB)–99% (RF) | [52] |
| 18 | Italy | Retrospective | AD | Gradient boosting, SVM, LR, RF, AdaBoosting, NB | MRI | Cross-validation | 95.96% (NB)–97.58% (GB) | 95%–96% | N/A | [46] |
| 19 | UK | Retrospective | Dementia | RF and XGBoost | Clinical data | 5-fold cross-validation | 85% (RF)–87% (XGB) | 73% (RF)–76% (XGB) | 99% (RF) and (XGB) | [53] |
| 20 | USA | Retrospective | PD | Classification tree, Gaussian Kernel, LDA, Ensemble, KNN, LR, Naive Bayes, SVM, RF | Clinical data | Leave-one-subject-out cross-validation | 74.1% (SVM)–84.5% (KNN) | 70.6% (SVM)–88.5% (KNN) | 79.2% (SVM)–84.6% (LR) | [54] |
| 21 | USA | Retrospective | AD | KNN, SVM, DT, RF, DL | MRI, SNP, clinical data | Internal cross-validation and an external test set | 68% (KNN)–89%(DL) | N/A | N/A | [47] |
| 22 | Italy | Retrospective | PD | SVM, KNN, LDA, LR | Clinical data | 10-fold cross-validation | 90.1% (LDA)–91.8% (SVM) | 68.4% (SVM)–87.5% (SVM optimized cost) | N/A | [55] |
| 23 | UK | Retrospective | Dementia | NB, LD, SVM, and KNN | MRI | 10-fold cross-validation | 77% (NB)–93% (C-SVM) | 72.5% (CNN)–99% (KNN) | 67% (KNN)–95% (SVM) | [48] |
| 24 | Netherlands | Retrospective | Dementia | Linear SVM | MRI, PET | LOO cross-validation and four-fold cross-validation | 89% (voxel)–90% (Region) | 83% (Region)–85% (voxel) | 79% (voxel)–90% (Region) | [49] |
| 25 | Finland | Prospective | Dementia | SVM | MRI/CT, clinical data | 5-fold cross-validation | 95% | 93% | 99% | [50] |
| 26 | Japan | Retrospective | Dementia | XGBoost, RF, LR | Clinical data | - | 86.3% (XGBoost)–89.3% (LR) | 85.7% (XGBoost)–96.4% (LR) | 80.0% (RF)–89.3% (LR) | [57] |
| 27 | USA | Retrospective | MCI and AD | SVM | Clinical data | 5-fold cross-validation | 91% | N/A | N/A | [56] |
| 28 | USA | Prospective | MCI | SVM | Clinical data | 5-fold cross-validation | 77.17% | 81.97% | 67.74% | [58] |
| 29 | Korea | Retrospective | AD and PD | RF | MRI | 5-fold cross-validation | 73.3% | 78.0% | 70.0% | [51] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Battineni, G.; Chintalapudi, N.; Hossain, M.A.; Losco, G.; Ruocco, C.; Sagaro, G.G.; Traini, E.; Nittari, G.; Amenta, F. Artificial Intelligence Models in the Diagnosis of Adult-Onset Dementia Disorders: A Review. Bioengineering 2022, 9, 370. https://doi.org/10.3390/bioengineering9080370
Battineni G, Chintalapudi N, Hossain MA, Losco G, Ruocco C, Sagaro GG, Traini E, Nittari G, Amenta F. Artificial Intelligence Models in the Diagnosis of Adult-Onset Dementia Disorders: A Review. Bioengineering. 2022; 9(8):370. https://doi.org/10.3390/bioengineering9080370
Chicago/Turabian StyleBattineni, Gopi, Nalini Chintalapudi, Mohammad Amran Hossain, Giuseppe Losco, Ciro Ruocco, Getu Gamo Sagaro, Enea Traini, Giulio Nittari, and Francesco Amenta. 2022. "Artificial Intelligence Models in the Diagnosis of Adult-Onset Dementia Disorders: A Review" Bioengineering 9, no. 8: 370. https://doi.org/10.3390/bioengineering9080370