
Adhesion of Resin to Lithium Disilicate with Different Surface Treatments before and after Salivary Contamination—An In-Vitro Study

 , , ,
, , ,  ,
,  ,
,  and
and
Abstract
:1. Introduction
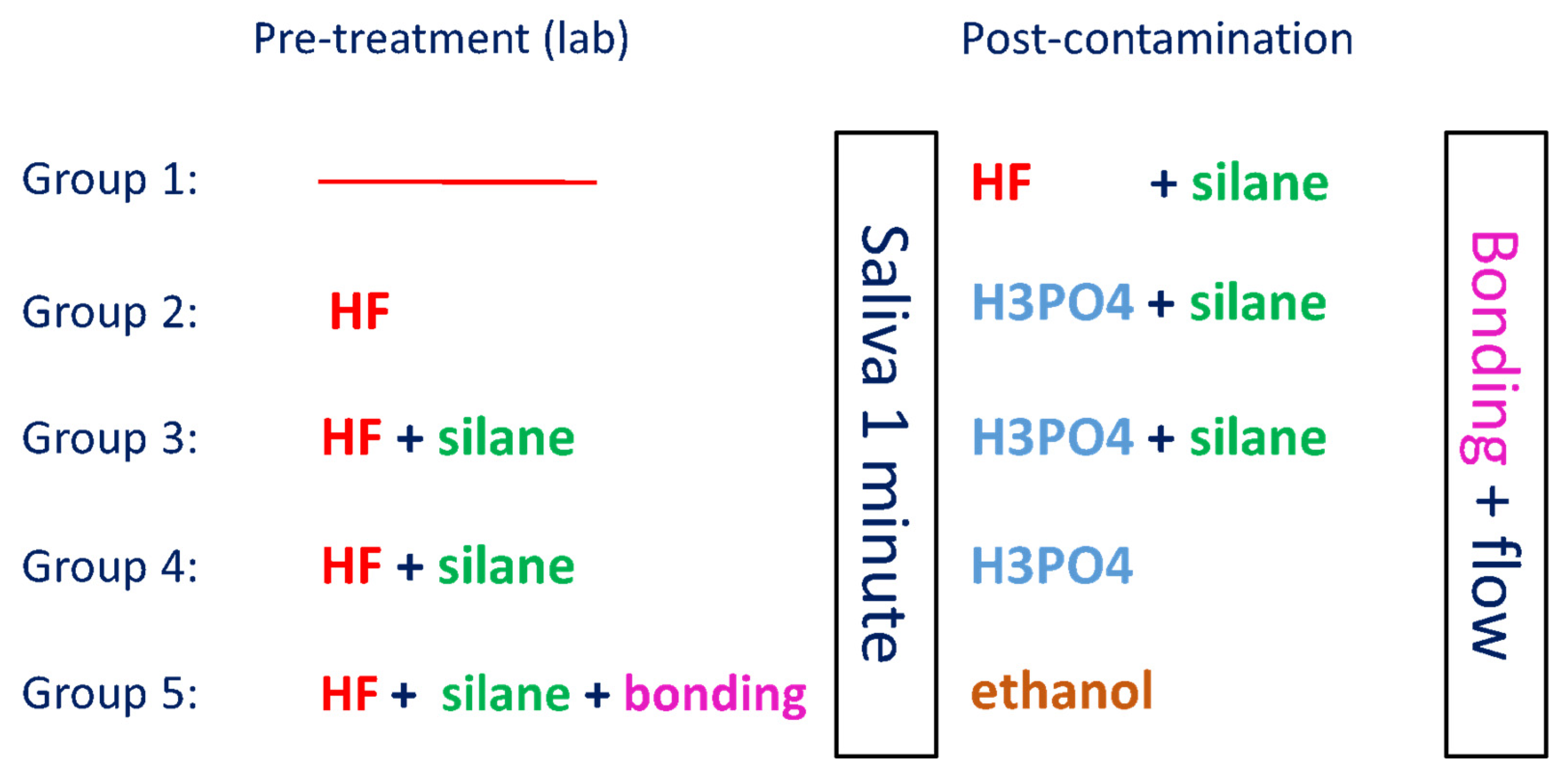
2. Materials and Methods
2.1. Specimen Preparation
2.2. Bonding of the Specimens
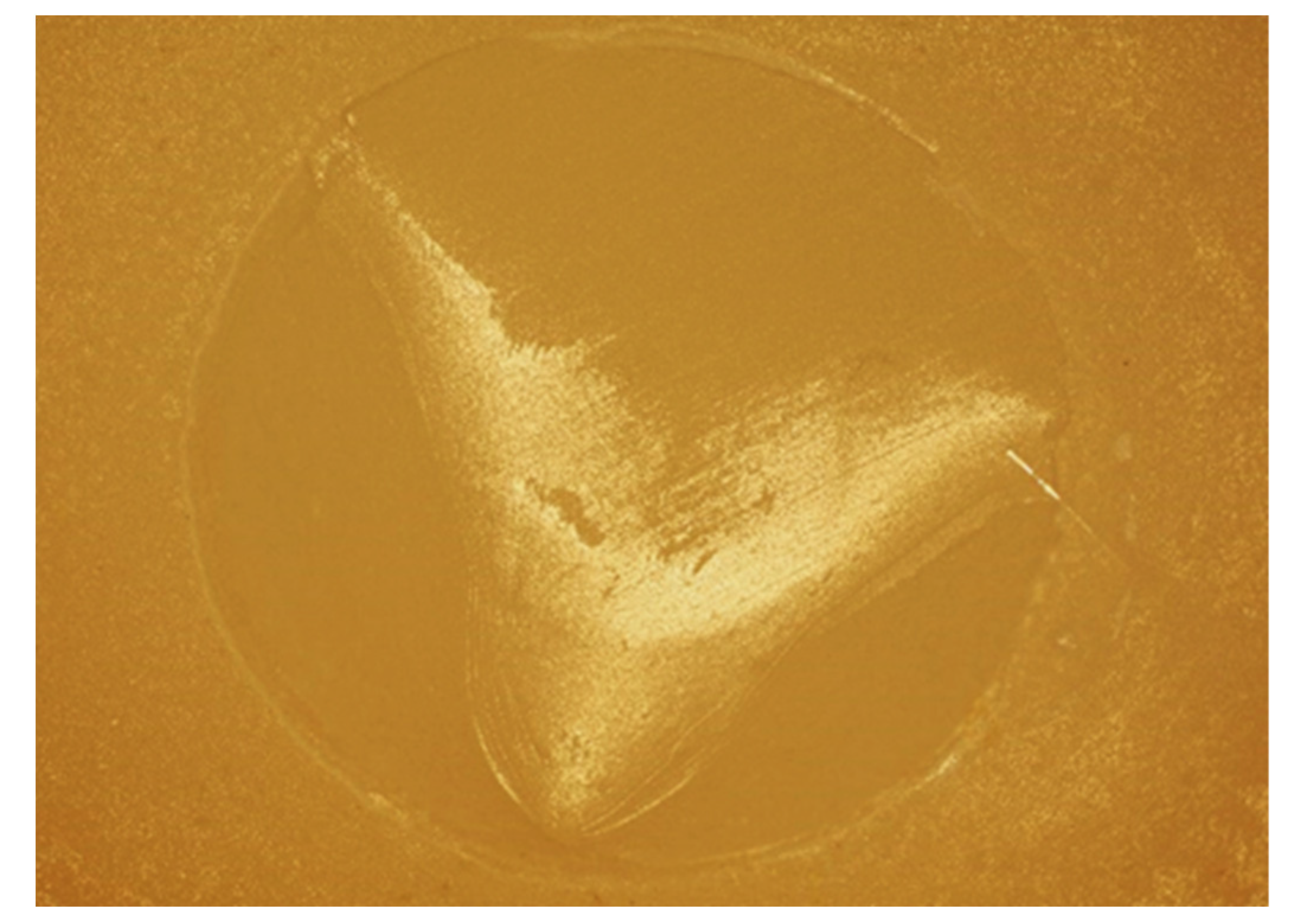
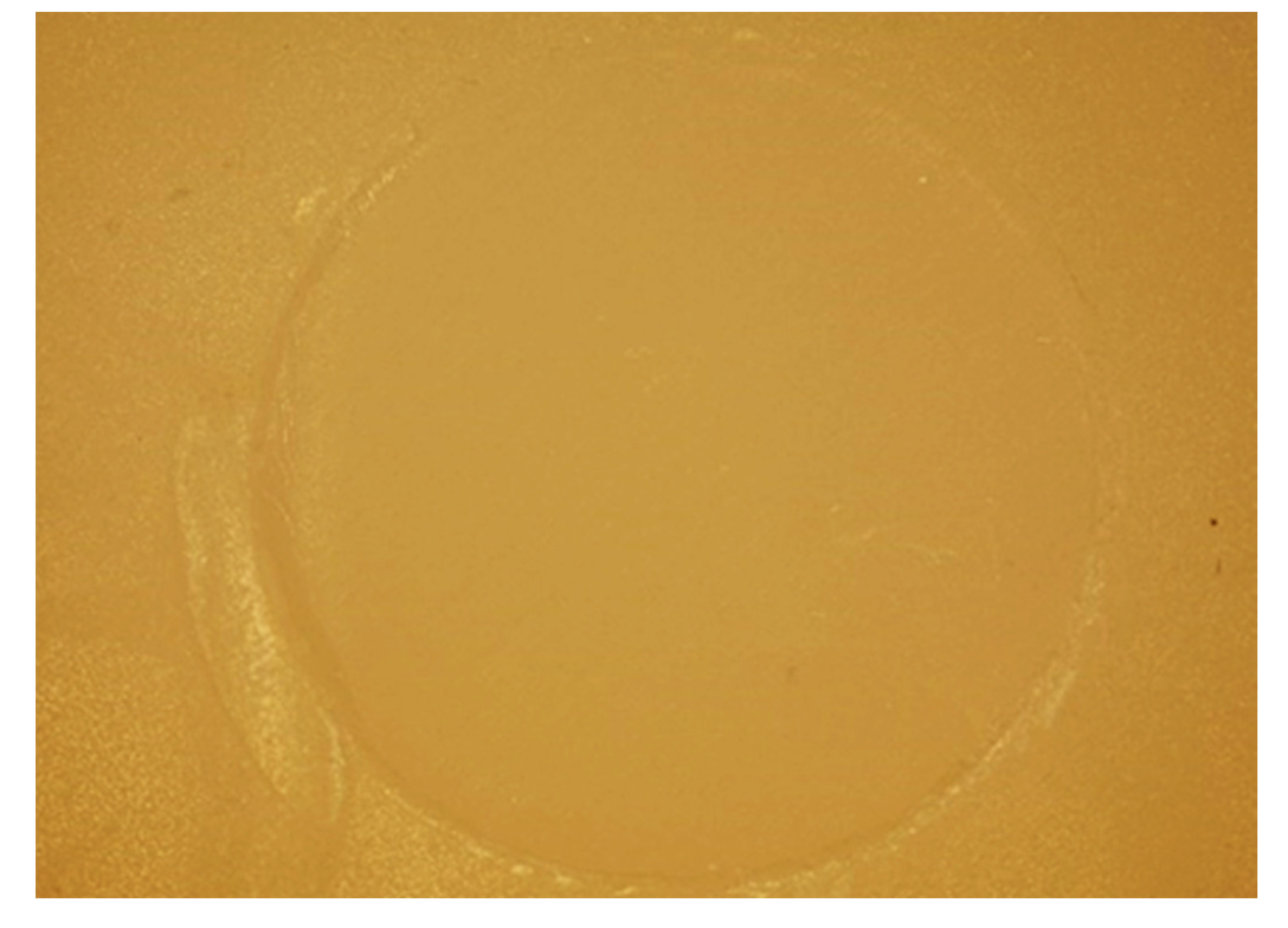
2.3. Bond Strength Test and Failure Analysis
2.4. Statistical Analysis
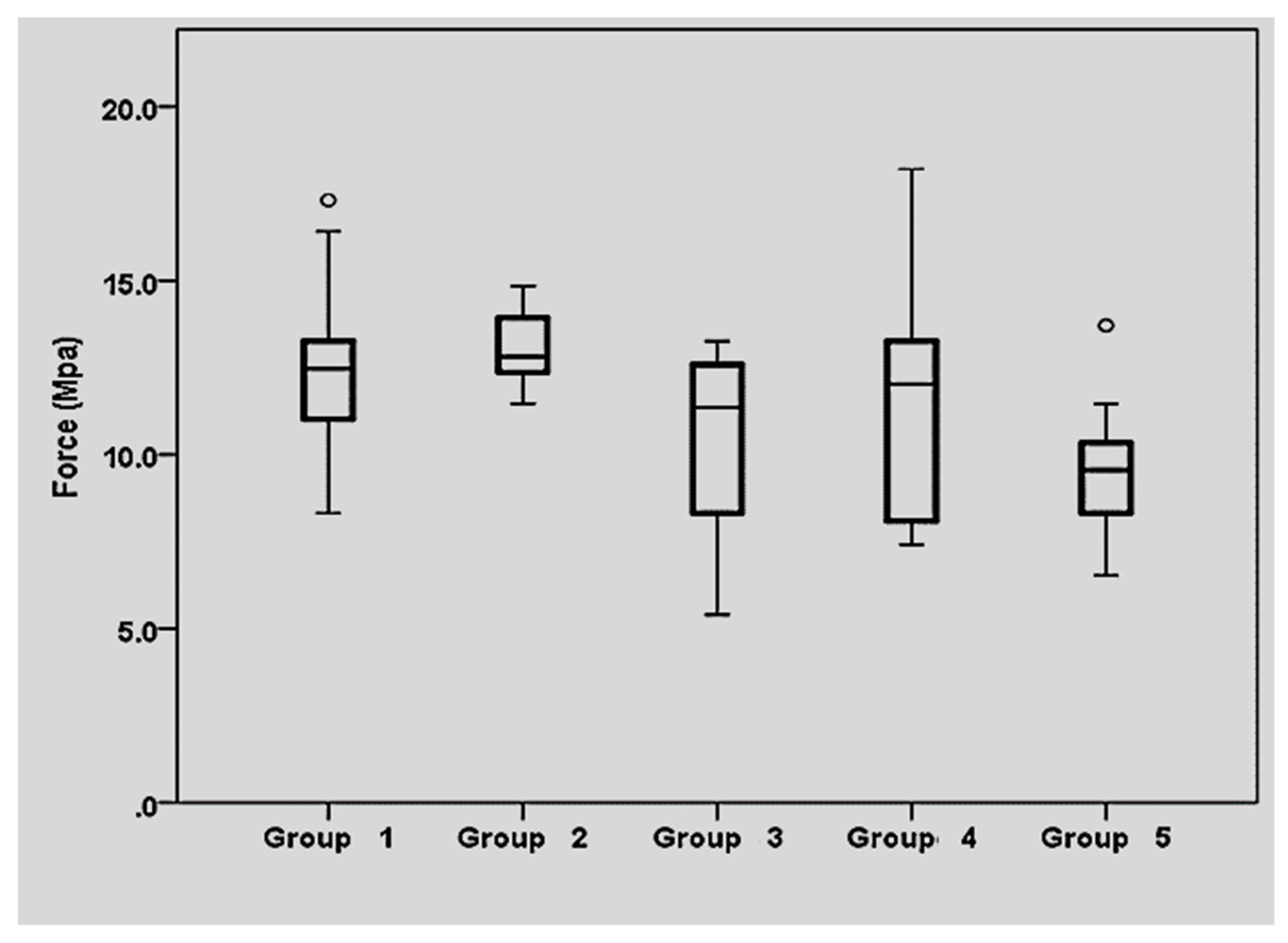
3. Results
3.1. Shear Bond Strength Results
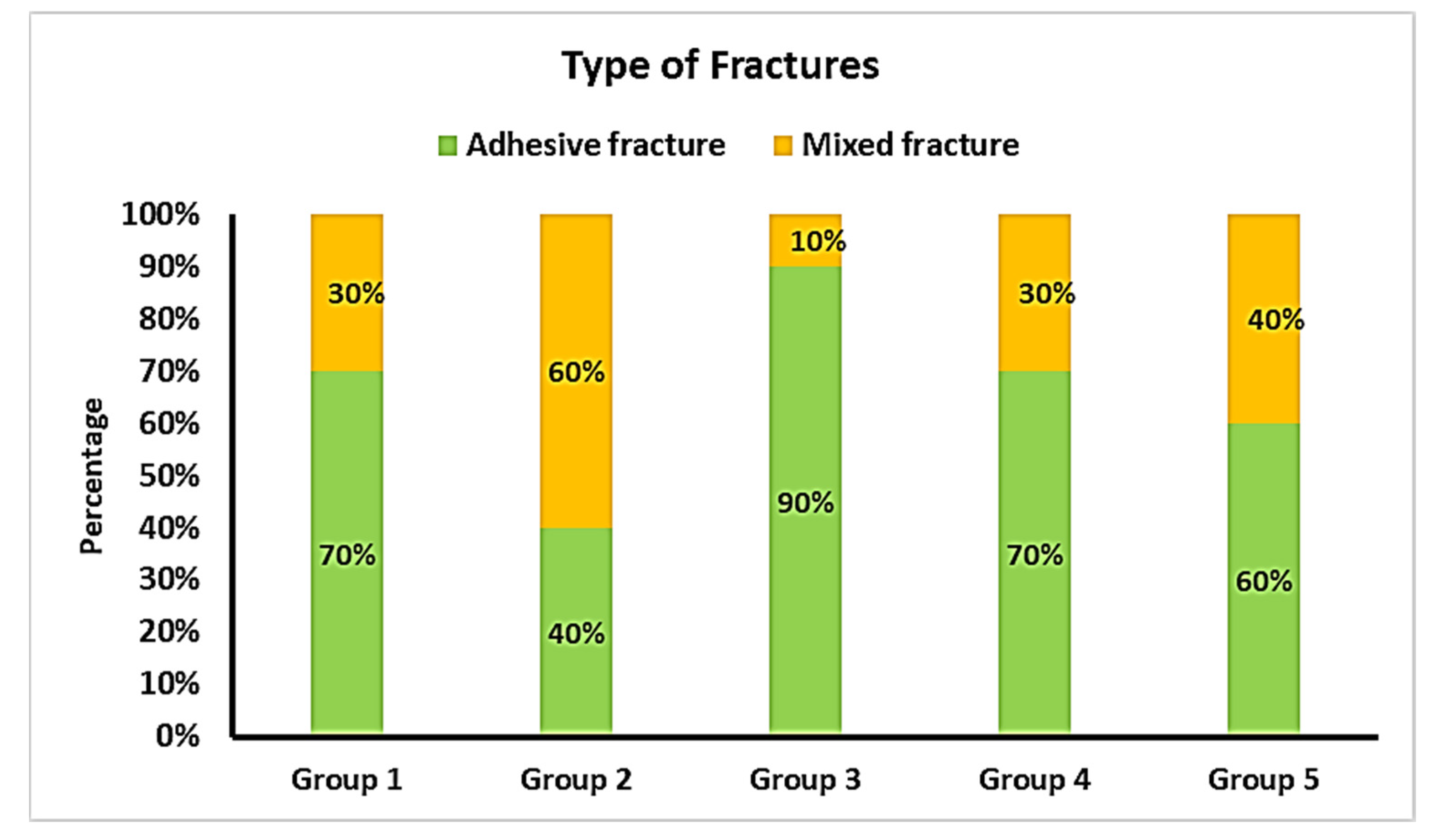
3.2. Comparison of the Types of Fracture
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Nasr, E.; Makhlouf, A.C.; Zebouni, E.; Makzoumé, J. All-ceramic Computer-aided Design and Computer-aided Manufacturing Restorations: Evolution of Structures and Criteria for Clinical Application. J. Contemp. Dent. Pract. 2019, 20, 516–523. [Google Scholar] [PubMed]
- Tian, T.; Tsoi, J.K.-H.; Matinlinna, J.P.; Burrow, M.F. Aspects of bonding between resin luting cements and glass ceramic materials. Dent. Mater. 2014, 30, 147–162. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Makarov, N.A.; Thoma, D.S.; Zwahlen, M.; Pjetursson, B.E. All-ceramic or metal-ceramic tooth-supported fixed dental prostheses (FDPs)? A systematic review of the survival and complication rates. Part I: Single crowns (SCs). Dent. Mater. 2015, 31, 603–623. [Google Scholar] [CrossRef] [Green Version]
- Puppin-Rontani, J.; Sundfeld, D.; Costa, A.R.; Correr, A.B.; Puppin-Rontani, R.M.; Borges, G.A.; Sinhoreti, M.; Correr-Sobrinho, L. Effect of Hydrofluoric Acid Concentration and Etching Time on Bond Strength to Lithium Disilicate Glass Ceramic. Oper. Dent. 2017, 42, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Borges, A.L.S.; Posritong, S.; Özcan, M.; Campos, F.; Melo, R.; Bottino, M.C. Can Cleansing Regimens Effectively Eliminate Saliva Contamination from Lithium Disilicate Ceramic Surface? Eur. J. Prosthodont. Restor. Dent. 2017, 25, 9–14. [Google Scholar]
- Koc-Dundar, B.; Özcan, M. Effect of clinical and laboratory contamination media on the adhesion of luting cement to direct and indirect resin composite materials. J. Adhes. Sci. Technol. 2017, 31, 1251–1263. [Google Scholar] [CrossRef] [Green Version]
- Nikolaus, F.; Wolkewitz, M.; Hahn, P. Bond strength of composite resin to glass ceramic after saliva contamination. Clin. Oral Investig. 2013, 17, 751–755. [Google Scholar] [CrossRef]
- Aladağ, A.; Elter, B.; Çömlekoğlu, E.; Kanat, B.; Sonugelen, M.; Kesercioğlu, A.; Özcan, M. Effect of different cleaning regimens on the adhesion of resin to saliva-contaminated ceramics. J. Prosthodont. 2015, 24, 136–145. [Google Scholar] [CrossRef] [Green Version]
- Lapinska, B.; Rogowski, J.; Nowak, J.; Nissan, J.; Sokolowski, J.; Lukomska-Szymanska, M. Effect of Surface Cleaning Regimen on Glass Ceramic Bond Strength. Molecules 2019, 24, 389. [Google Scholar] [CrossRef] [Green Version]
- Lopes, G.; Ballarin, A. Hydrofluoric Acid—Simple Things You May Do Not Know about Something You Are So Habituated to Use. Odovtos Int. J. Dent. Sci. 2015, 1, 15–23. [Google Scholar]
- Ozcan, M.; Allahbeickaraghi, A.; Dündar, M. Possible hazardous effects of hydrofluoric acid and recommendations for treatment approach: A review. Clin. Oral Investig. 2012, 16, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Bajraktarova-Valjakova, E.; Korunoska-Stevkovska, V.; Georgieva, S.; Ivanovski, K.; Bajraktarova-Misevska, C.; Mijoska, A.; Grozdanov, A. Hydrofluoric Acid: Burns and Systemic Toxicity, Protective Measures, Immediate and Hospital Medical Treatment. Maced. J. Med. Sci. 2018, 6, 2257–2269. [Google Scholar] [CrossRef] [Green Version]
- Schwerin, D.L.; Hatcher, J.D. Hydrofluoric Acid Burns. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Yoshida, K. Influence of cleaning methods on the bond strength of resin cement to saliva-contaminated lithium disilicate ceramic. Clin. Oral Investig. 2020, 24, 2091–2097. [Google Scholar] [CrossRef] [PubMed]
- Klosa, K.; Wolfart, S.; Lehmann, F.; Wenz, H.-J.; Kern, M. The effect of storage conditions, contamination modes and cleaning procedures on the resin bond strength to lithium disilicate ceramic. J. Adhes. Dent. 2009, 11, 127–135. [Google Scholar] [PubMed]
- Alfaro, M.J.; Meyers, E.J.; Ashcraft-Olmscheid, D.; Vandewalle, K.S. Effect of a new salivary-contaminant removal method on bond strength. Gen. Dent. 2016, 64, 51–54. [Google Scholar] [PubMed]
- Marfenko, S.; Özcan, M.; Attin, T.; Tauböck, T.T. Treatment of surface contamination of lithium disilicate ceramic before adhesive luting. Am. J. Dent. 2020, 33, 33–38. [Google Scholar] [PubMed]
- Zarone, F.; Di Mauro, M.I.; Ausiello, P.; Ruggiero, G.; Sorrentino, R. Current status on lithium disilicate and zirconia: A narrative review. BMC Oral Health 2019, 19, 134. [Google Scholar] [CrossRef] [Green Version]
- Aziz, A.; El-Mowafy, O.; Paredes, S. Clinical outcomes of lithium disilicate glass-ceramic crowns fabricated with CAD/CAM technology: A systematic review. Dent. Med. Probl. 2020, 57, 197–206. [Google Scholar] [CrossRef]
- Maroulakos, G.; Thompson, G.A.; Kontogiorgos, E.D. Effect of cement type on the clinical performance and complications of zirconia and lithium disilicate tooth-supported crowns: A systematic review. Report of the Committee on Research in Fixed Prosthodontics of the American Academy of Fixed Prosthodontics. J. Prosthet. Dent. 2019, 121, 754–765. [Google Scholar] [CrossRef]
- Hardan, L.; Bourgi, R.; Kharouf, N.; Mancino, D.; Zarow, M.; Jakubowicz, N.; Haikel, Y.; Cuevas-Suárez, C.-E. Reinforced Universal Adhesive by Ribose Crosslinker: A Novel Strategy in Adhesive Dentistry. Polymers 2021, 13, 704. [Google Scholar]
- Kharouf, N.; Eid, A.; Hardan, L.; Bourgi, R.; Arntz, Y.; Jmal, H.; Foschi, F.; Sauro, S.; Ball, V.; Haikel, Y.; et al. Antibacterial and bonding properties of universal adhesive dental polymers doped with pyrogallol. Polymers 2021, 13, 1538. [Google Scholar] [CrossRef] [PubMed]
- Irmak, Ö.; Yaman, B.C.; Orhan, E.O.; Kılıçarslan, M.A.; Mante, F.K.; Ozer, F. Influence of cleaning methods on bond strength to saliva contaminated zirconia. J. Esthet. Restor. Dent. 2018, 30, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Veríssimo, A.H.; Moura, D.M.D.; Tribst, J.P.M.; Araújo, A.M.M.d.; Leite, F.P.P.; Souza, R.d.A.E. Effect of hydrofluoric acid concentration and etching time on resin-bond strength to different glass ceramics. Braz. Oral Res. 2019, 33, e041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumer, L.; Schmidli, F.; Weiger, R.; Fischer, J. A systematic approach to standardize artificial aging of resin composite cements. Dent. Mater. 2015, 31, 855–863. [Google Scholar] [CrossRef]
- ISO/TS 11405:2015; Dentistry-Testing of Adhesion to Tooth Structure. International Organizazion for Standardization: Geneva, Switzerland, 2015.
- Bömicke, W.; Rammelsberg, P.; Krisam, J.; Rues, S. The Effects of Surface Conditioning and Aging on the Bond Strength Between Composite Cement and Zirconia-reinforced Lithium-Silicate Glass-Ceramics. J. Adhes. Dent. 2019, 21, 567–576. [Google Scholar]
- Alnassar, T.; Vohra, F.; Abualsaud, H.; Al-Thobity, A.M.; Flinton, R. Efficacy of novel cleansing agent for the decontamination of lithium disilicate ceramics: A shear bond strength study. J. Adhes. Sci. Technol. 2017, 31, 202–210. [Google Scholar] [CrossRef]
- Lyann, S.K.; Takagaki, T.; Nikaido, T.; Wada, T.; Uo, M.; Ikeda, M.; Sadr, A.; Tagami, J. Efficacy of Various Surface Treatments on the Bonding Performance of Saliva-contaminated Lithium-Disilicate Ceramics. J. Adhes. Dent. 2019, 21, 51–58. [Google Scholar]
- Aboush, Y.E. Removing saliva contamination from porcelain veneers before bonding. J. Prosthet. Dent. 1998, 80, 649–653. [Google Scholar] [CrossRef]
- Zhang, S.; Kocjan, A.; Lehmann, F.; Kosmac, T.; Kern, M. Influence of contamination on resin bond strength to nano-structured alumina-coated zirconia ceramic. Eur. J. Oral Sci. 2010, 118, 396–403. [Google Scholar] [CrossRef]
- Della Bona, A.; Anusavice, K.J.; Mecholsky, J.J. Failure analysis of resin composite bonded to ceramic. Dent. Mater. 2003, 19, 693–699. [Google Scholar] [CrossRef]
- Sano, H.; Shono, T.; Sonoda, H.; Takatsu, T.; Ciucchi, B.; Carvalho, R.; Pashley, D.H. Relationship between surface area for adhesion and tensile bond strength--evaluation of a micro-tensile bond test. Dent. Mater. 1994, 10, 236–240. [Google Scholar] [CrossRef]
- Sano, H.; Chowdhury, A.F.M.A.; Saikaew, P.; Matsumoto, M.; Hoshika, S.; Yamauti, M. The microtensile bond strength test: Its historical background and application to bond testing. Jpn. Dent. Sci. Rev. 2020, 56, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Sirisha, K.; Rambabu, T.; Shankar, Y.R.; Ravikumar, P. Validity of bond strength tests: A critical review: Part I. J. Conserv. Dent. 2014, 17, 305–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sirisha, K.; Rambabu, T.; Ravishankar, Y.; Ravikumar, P. Validity of bond strength tests: A critical review-Part II. J. Conserv. Dent. 2014, 17, 420–426. [Google Scholar] [CrossRef] [Green Version]
- Inoue, S.; Vargas, M.A.; Abe, Y.; Yoshida, Y.; Lambrechts, P.; Vanherle, G.; Sano, H.; Van Meerbeek, B. Microtensile bond strength of eleven contemporary adhesives to dentin. J. Adhes. Dent. 2001, 3, 237–245. [Google Scholar] [PubMed]
- Braga, R.R.; Meira, J.B.C.; Boaro, L.C.C.; Xavier, T.A. Adhesion to tooth structure: A critical review of ‘macro’ test methods. Dent. Mater. 2010, 26, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Della Bona, A.; van Noort, R. Shear vs. tensile bond strength of resin composite bonded to ceramic. J. Dent. Res. 1995, 74, 1591–1596. [Google Scholar] [CrossRef]
- Klosa, K.; Warnecke, H.; Kern, M. Effectiveness of protecting a zirconia bonding surface against contaminations using a newly developed protective lacquer. Dent. Mater. 2014, 30, 785–792. [Google Scholar] [CrossRef]
- Wegner, S.M.; Gerdes, W.; Kern, M. Effect of different artificial aging conditions on ceramic-composite bond strength. Int. J. Prosthodont. 2002, 15, 267–272. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Brand | Lot | Composition | Manufacturer |
|---|---|---|---|---|
| Glass-based ceramic | IPS e.max CAD LT A1 shade | Y30837 | SiO2,LiO2, K2O, P2O5, ZrO2, ZnO, other oxides, coloring oxides | IvoclarVivadent, Schaan, Liechtenstein |
| Ceramic etchant | Porcelain Etch | BGTV7 | 9% buffered hydrofluoric acid | Ultradent, Schaan, Liechtenstein |
| Ceramic primer | Porcelain Primer | 1900001117 | Pre-hydrolyzed silane primer with alcohol and acetone | Bisco, Schaumburg, IL, USA |
| Etching gel | DentoEtch | DE-4.12 | 37% phosphoric acid | Itena, Avenue Foch, Paris, France |
| Bonding agent | Adper Single Bond 2 | NA61948 | Bis-GMA, HEMA, dimethacrylates, ethanol, water, photoinitiators, methacrylate functional copolymer of polyacrylic and polyitaconic acids, and silica nanofiller | 3M ESPE, St. Paul, MN, USA |
| Flowable composite | Filtek Z350 XT, Flowable Restorative, A1 shade | NA37278 | Bis-GMA, TEGDMA, procrylatresins; ytterbium trifluoride, silica, zirconia/silica cluster fillers | 3M ESPE, St. Paul, MN, USA |
| N | Mean | Standard Deviation | 95% Confidence Interval | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|
| Lowerbound | Upperbound | ||||||
| Group 1 | 10 | 12.59 a | 2.71 | 10.65 | 14.53 | 8.32 | 17.31 |
| Group 2 | 10 | 13.11 a | 1.03 | 12.37 | 13.84 | 11.47 | 14.84 |
| Group 3 | 10 | 10.41 b | 2.75 | 8.44 | 12.38 | 5.40 | 13.26 |
| Group 4 | 10 | 11.74 a,b | 3.49 | 9.24 | 14.23 | 7.42 | 18.21 |
| Group 5 | 10 | 9.65 b | 1.99 | 8.22 | 11.07 | 6.52 | 13.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harouny, R.; Hardan, L.; Harouny, E.; Kassis, C.; Bourgi, R.; Lukomska-Szymanska, M.; Kharouf, N.; Ball, V.; Khairallah, C. Adhesion of Resin to Lithium Disilicate with Different Surface Treatments before and after Salivary Contamination—An In-Vitro Study. Bioengineering 2022, 9, 286. https://doi.org/10.3390/bioengineering9070286
Harouny R, Hardan L, Harouny E, Kassis C, Bourgi R, Lukomska-Szymanska M, Kharouf N, Ball V, Khairallah C. Adhesion of Resin to Lithium Disilicate with Different Surface Treatments before and after Salivary Contamination—An In-Vitro Study. Bioengineering. 2022; 9(7):286. https://doi.org/10.3390/bioengineering9070286
Chicago/Turabian StyleHarouny, Ryan, Louis Hardan, Elie Harouny, Cynthia Kassis, Rim Bourgi, Monika Lukomska-Szymanska, Naji Kharouf, Vincent Ball, and Carlos Khairallah. 2022. "Adhesion of Resin to Lithium Disilicate with Different Surface Treatments before and after Salivary Contamination—An In-Vitro Study" Bioengineering 9, no. 7: 286. https://doi.org/10.3390/bioengineering9070286