
Efficacy of Kinematic Parameters for Assessment of Temporomandibular Joint Function and Disfunction: A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Selection Process
2.4. Data Collection Process
2.5. Data Items
2.6. Quality and Risk of Bias Assessment
2.7. Outcome Variables
2.8. Measures of Treatment Effect
2.9. Synthesis Methods
3. Results
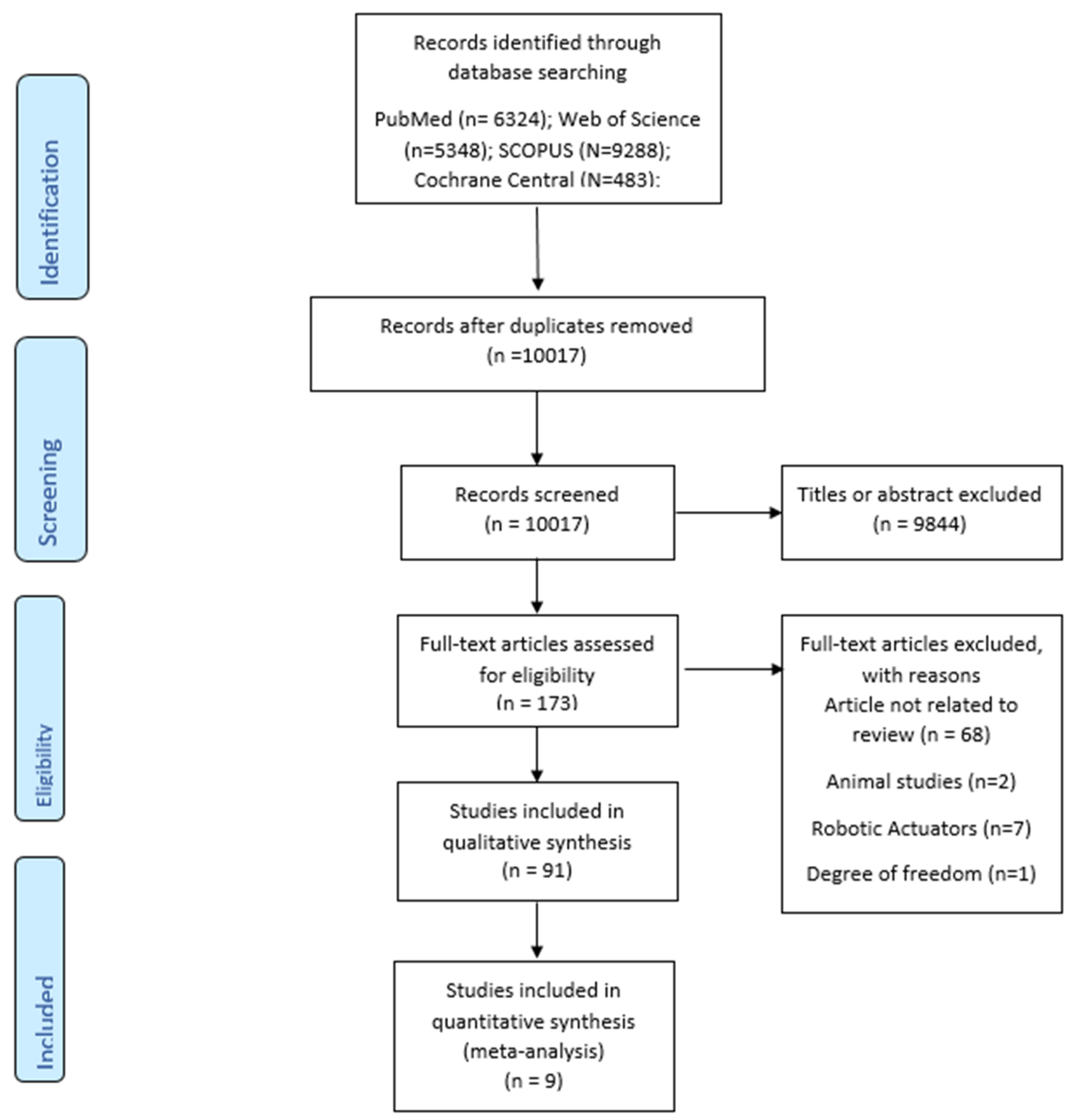
3.1. Study Selection and Description
3.2. Bias Risk Assessment
3.2.1. Qualitative Synthesis
3.2.2. Quantitative Synthesis
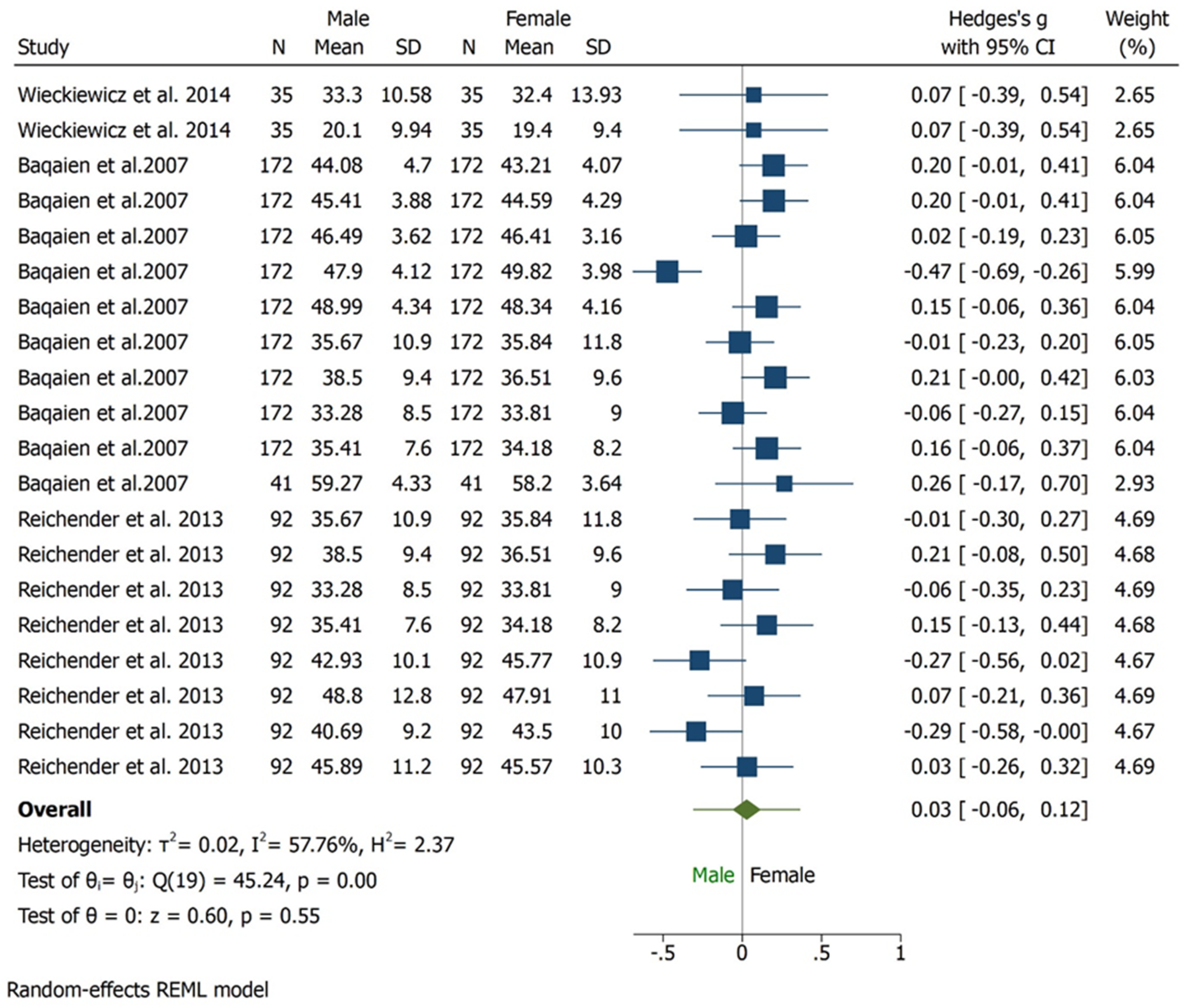
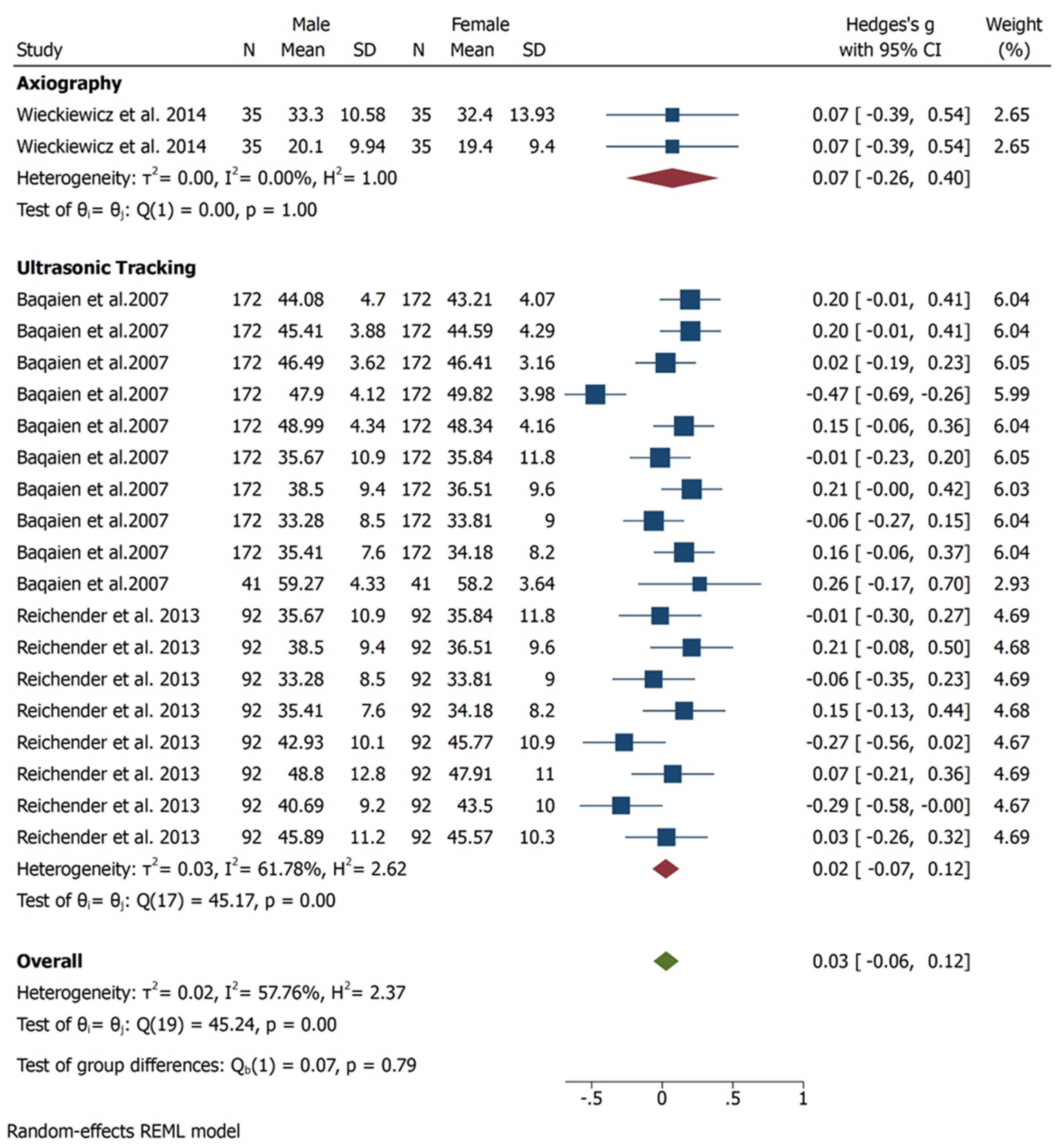
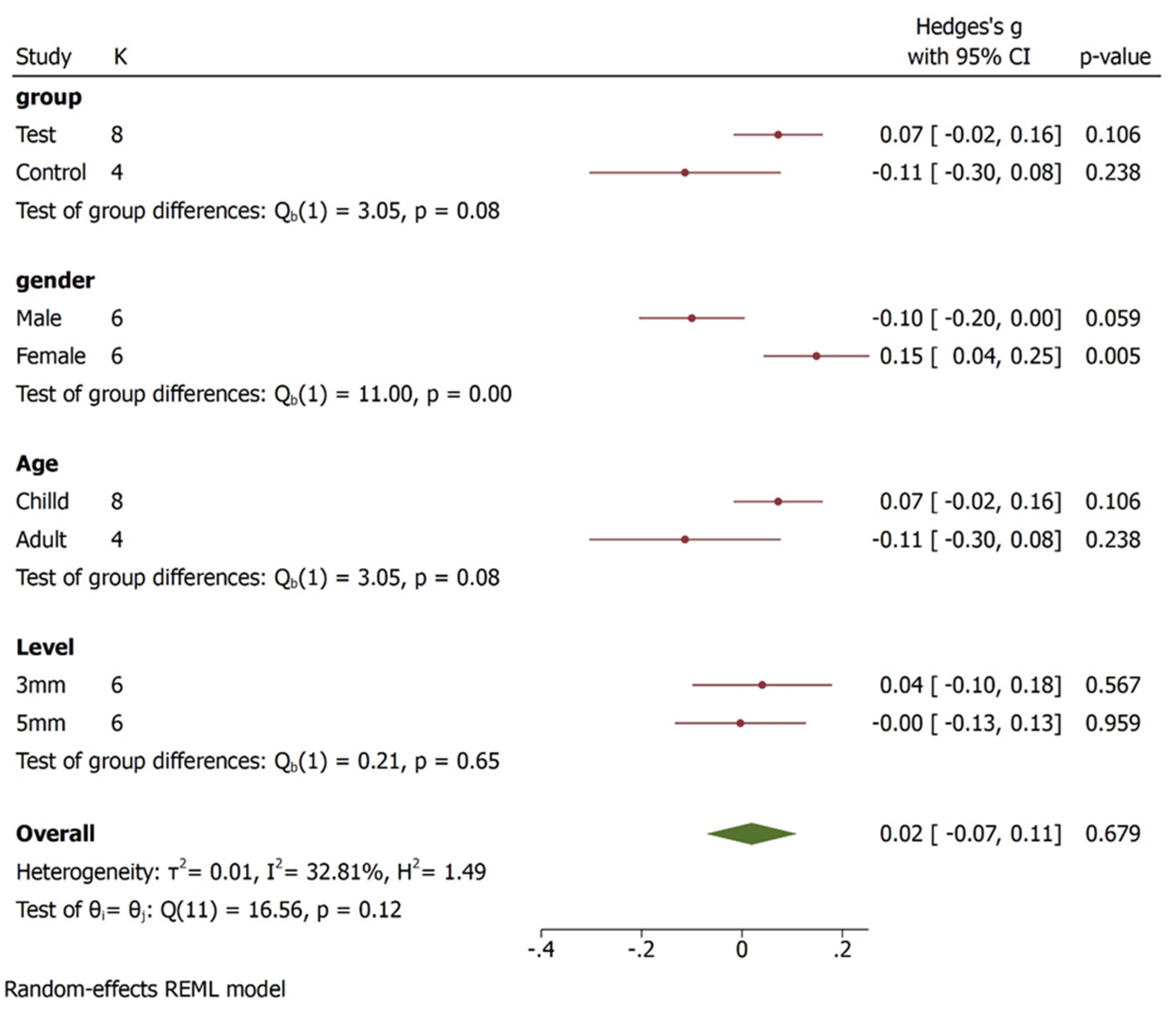
3.3. Condylar Inclination
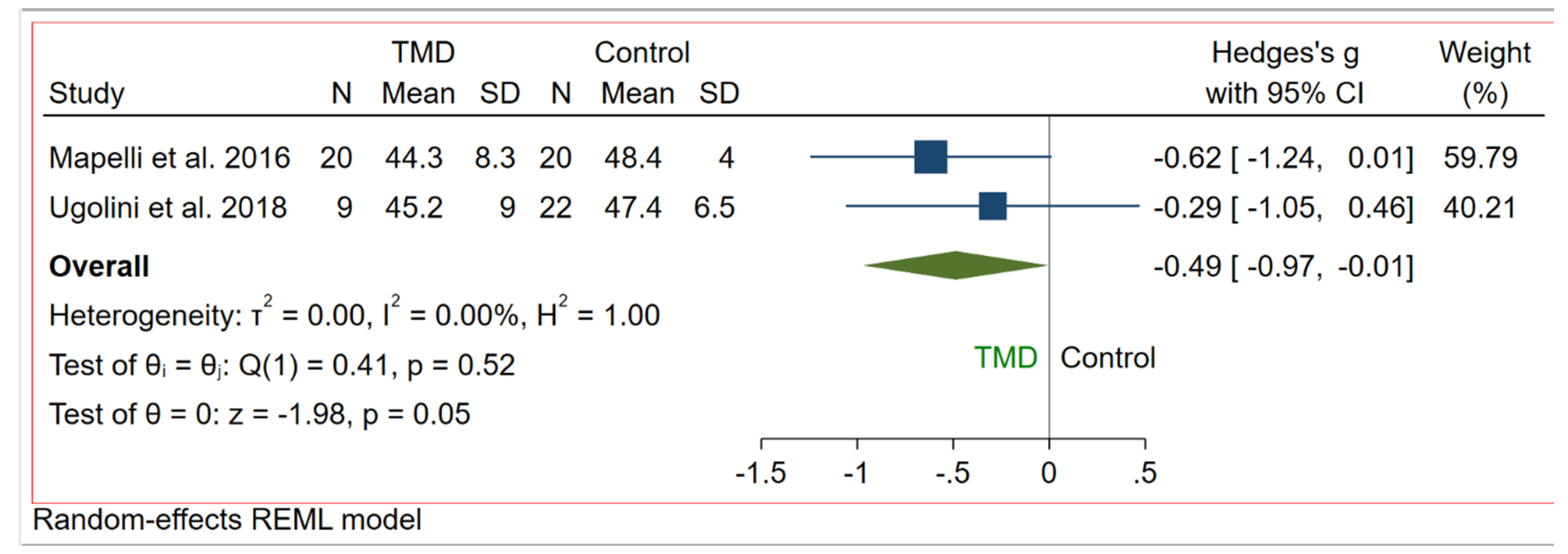
3.4. Maximum Mouth Opening
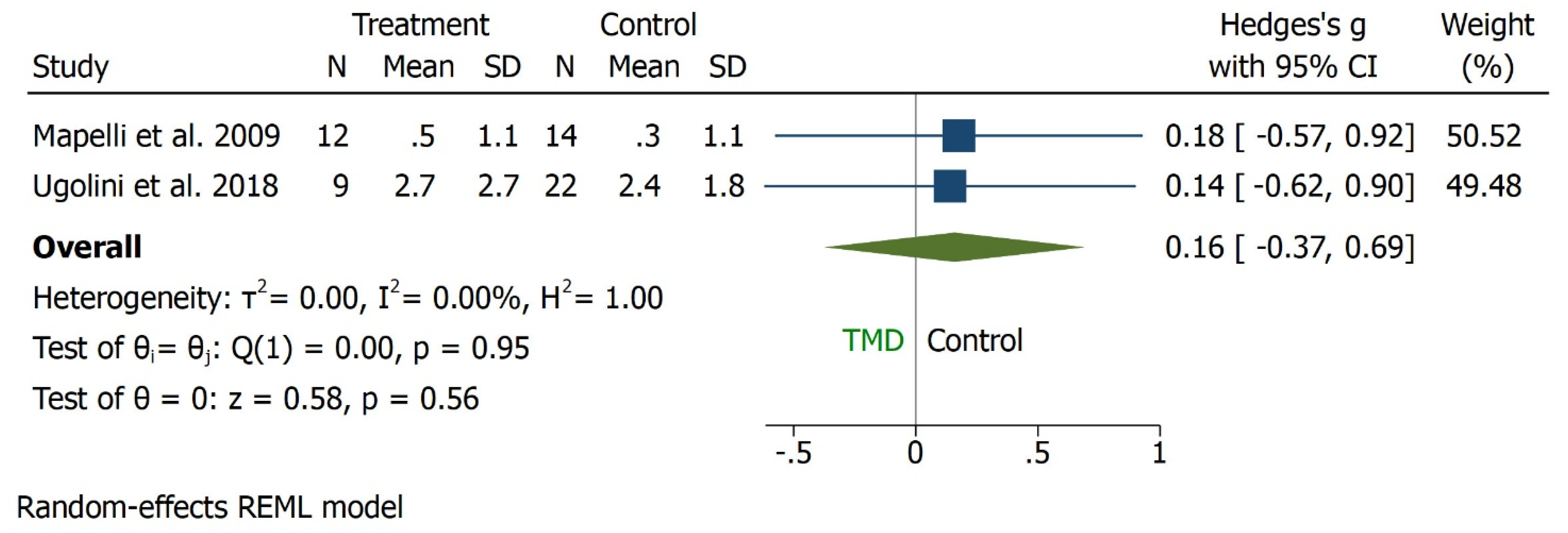
3.5. IP-MMO
3.6. Horizontal Angle
3.7. Sagittal Angle
4. Discussion
5. Conclusions
6. Recommendations
- A well-designed case-control studies would be beneficial in order to increase the level of evidence on the clinical significance of kinematics;
- The literature in the present review demonstrated varying diagnostic tools and measurements for different outcomes. It would be beneficial if the different diagnostic tools are used along with a standard of care;
- The present review highlighted different outcome measures and it would benefit if the case-control studies with MMO outcome as standard method would be measured along with the different outcomes which can have similar dimensions or unit of measurement;
- There are varying groups compared in the studies highlighted within this review. Comparing the groups that include, the TMD and the pre-surgical, post-surgical would bridge the gap in the evidence;
- Majority of studies included in this review lack sample size calculations. Therefore, it is highly recommended to use appropriate sample size calculations for respective studies.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Okeson, J.P. Management of Temporomandibular Disorders and Occlusion, 7th ed.; Elsevier: Mosby, MO, USA; Louis, MO, USA, 2012. [Google Scholar]
- Reisine, S.T.; Weber, J. The effects of temporomandibular joint disorders on patients’ quality of life. Community Dent. Health 1989, 6, 257–270. [Google Scholar] [PubMed]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: Recommendations of the international RDC/TMD consortium network and orofacial pain special interest group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Steinkeler, A. Epidemiology, diagnosis, and treatment of temporomandibular disorders. Dent. Clin. N. Am. 2013, 57, 465–479. [Google Scholar] [CrossRef] [PubMed]
- Peck, C.C.; Goulet, J.-P.; Lobbezoo, F.; Schiffman, E.L.; Alstergren, P.; Anderson, G.C.; de Leeuw, R.; Jensen, R.; Michelotti, A.; Ohrbach, R.; et al. Expanding the taxonomy of the diagnostic criteria for temporomandibular disorders. J. Oral Rehabil. 2014, 41, 2e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koolstra, J.H. Dynamics of the human masticatory system. Crit. Rev. Oral Biol. Med. 2002, 13, 366e76. [Google Scholar] [CrossRef] [Green Version]
- Soboleva, U.; Laurina, L.; Slaidina, A. Jaw tracking devices-historical review of methods development, Part II. Stomatologija 2005, 7, 72–76. [Google Scholar]
- De Bont, L.G.; Stegenga, B. Pathology of temporomandibular joint internal derangement and osteoarthritis. Int. J. Oral Maxillofac. Surg. 1993, 22, 71–74. [Google Scholar] [CrossRef]
- Ferrillo, M.; Ammendolia, A.; Paduano, S.; Calafiore, D.; Marotta, N.; Migliario, M.; Fortunato, L.; Giudice, A.; Michelotti, A.; De Sire, A. Efficacy of rehabilitation on reducing pain in muscle-related temporomandibular disorders: A systematic review and meta-analysis of randomized controlled trials. J. Back Musculoskelet. Rehabil. in press. 2022, 1–16. [Google Scholar] [CrossRef]
- Deregibus, A.; Ferrillo, M.; Piancino, M.; Domini, M.; De Sire, A.; Castroflorio, T. Are occlusal splints effective in reducing myofascial pain in patients with muscle-related temporomandibular disorders? A randomized-controlled trial. Turk. J. Phys. Med. Rehabil. 2021, 67, 32–40. [Google Scholar] [CrossRef]
- De Sire, A.; Marotta, M.; Ferrillo, M.; Agostini, F.; Sconza, C.; Lippi, L.; Respizzi, S.; Giudice, A.; Invernizzi, M.; Ammendolia, A. Oxygen-Ozone Therapy for Reducing Pro-Inflammatory Cytokines Serum Levels in Musculoskeletal and Temporomandibular Disorders: A Comprehensive Review. Int. J. Mol. Sci. 2022, 23, 2528. [Google Scholar] [CrossRef]
- Bando, E.; Nishigawa, K.; Nakano, M.; Takeuchi, H.; Shigemoto, S.; Okura, K.; Satsuma, T.; Yamamoto, T. Currentstatus of researches on jaw movement and occlusion for clinical applications. Jpn. Dent. Sci. Rev. 2009, 45, 83–97. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.-C.; Lin, C.-C.; Hsieh, H.-P.; Fu, Y.-C.; Chen, Y.-J.; Lu, T.-W. In vivo three-dimensional mandibular kinematics and functional point trajectories during temporomandibular activities using 3d fluoroscopy. Dentomaxillofacial Radiol. 2021, 50, 20190464. [Google Scholar] [CrossRef] [PubMed]
- Woodford, S.C.; Robinson, D.L.; Mehl, A.; Lee, P.V.S.; Ackland, D.C. Measurement of normal and pathological mandibular and temporomandibular joint kinematics: A systematic review. J. Biomech. 2020, 111, 109994. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematics review and meta-analyses: The PRISMA statement. BMJ Br. Med. J. 2009, 339, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.; Cochrane Consumers and Communication Review Group. Cochrane Consumers and Communication Group: Meta-analysis. Available online: http://cccrg.cochrane.org (accessed on 10 December 2016).
- Pearson, A.; Wiechula, R.; Court, A.; Lockwood, C. The JBI model of evidence-based healthcare. Int. J. Evid. Based Healthc. 2005, 3, 207–215. [Google Scholar]
- Placko, G.; Bellot-Samson, V.; Brunet, S.; Guyot, L.; Richard, O.; Cheynet, F.; Chossegros, C.; Ouaknine, M. Normal mouth opening in the adult French population. Rev. Stomatol. Chir. Maxillofac. 2005, 106, 267–271. [Google Scholar] [CrossRef]
- Travell, J. Temporomandibular joint dysfunction. Temporomandibular joint pain referred from muscles of the head and neck. J. Prosthet. Dent. 1960, 10, 745–763. [Google Scholar] [CrossRef]
- Visscher, C.M.; Huddleston Slater, J.J.R.; Lobbezoo, F.; Naeije, M. Kinematics of the human mandible for different head postures. J. Oral Rehabil. 2000, 27, 299–305. [Google Scholar] [CrossRef]
- Rieder, C.E. Maximum mandibular opening in patients with and without a history of temporomandibular dysfunction. J. Prosthet. Dent. 1978, 39, 441–446. [Google Scholar] [CrossRef]
- Ferrario, V.F.; Sforza, C.; Miani, A.; D’Addona, A.; Tartaglia, G. Statistical evaluation of some mandibular reference positions in normal young people. Int. J. Prosthodont. 1992, 5, 158–165. [Google Scholar]
- Tsolka, P.; Fenlon, M.R.; McCullock, A.J.; Preiskel, H.W. A controlled clinical, electromyographic, and kinesiographic assessment of craniomandibular disorders in women. J. Orofac. Pain 1994, 8, 80–89. [Google Scholar] [PubMed]
- Wieckiewicz, M.; Zietek, M.; Nowakowska, D.; Wieckiewicz, W. Comparison of selected kinematic facebows applied to mandibular tracing. Biomed. Res. Int. 2014, 2014, 818694. [Google Scholar] [CrossRef] [PubMed]
- Baqaien, M.A.; Al-Salti, F.M.; Muessig, D. Changes in condylar path inclination during maximum protrusion between the ages of 6 and 12 years. J. Oral Rehabil. 2007, 34, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Reicheneder, C.; Kardari, Z.; Proff, P.; Fanghaenel, J.; Faltermeier, A.; Römer, P. Correlation of condylar kinematics in children with gender, facial type and weight. Ann. Anat. 2013, 195, 243–247. [Google Scholar] [CrossRef]
- Ferrario, V.F.; Sforza, C.; Lovecchio, N.; Mian, F. Quantification of translational and gliding components in human temporomandibular joint during mouth opening. Arch. Oral Biol. 2005, 50, 507–515. [Google Scholar] [CrossRef]
- Gallo, L.M.; Airoldi, G.B.; Airoldi, R.L.; Palla, S. Description of mandibular finite helical axis pathways in asymptomatic subjects. J. Dent. Res. 1997, 76, 704–713. [Google Scholar] [CrossRef]
- Mapelli, A.; Machado, B.C.Z.; Garcia, D.M.; Rodrigues Da Silva, M.A.M.; Sforza, C.; DeFelicio, C.M. Three-dimensional analysis of jaw kinematic alterations in patients with chronic TMD—Disc displacement with reduction. J. Oral Rehabil. 2016, 43, 824–832. [Google Scholar] [CrossRef]
- Ugolini, A.; Mapelli, A.; Segu, M.; Zago, M.; Codari, M.; Sforza, C. Three dimensional mandibular motion in skeletal Class III patients. CRANIO J. Craniomandib. Sleep Pract. 2018, 36, 113–120. [Google Scholar] [CrossRef]
- Mapelli, A.; Galante, D.; Lovecchio, N.; Sforza, C.; Ferrario, V.F. Translation and rotation movements of the mandible during mouth opening and closing. Clin. Anat. 2009, 22, 311–318. [Google Scholar] [CrossRef]
- Tamaki, K.; Celar, A.G.; Beyrer, S.; Aoki, H. Reproduction of excursive tooth contact in an articulator with computerized axiography data. J. Prosthet. Dent. 1997, 78, 373–378. [Google Scholar] [CrossRef]
- Leissner, O.; Maulén-Yáñez, M.; Meeder-Bella, W.; León-Morales, C.; Vergara-Bruna, E.; González-Arriagada, W.A. Assessment of mandibular kinematics values and its relevance for the diagnosis of temporomandibular joint disorders. J. Dent. Sci. 2021, 16, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Jordan, Z.; Lockwood, C.; Munn, Z.; Aromataris, E. The updated Joanna Briggs Institute model of evidence-based healthcare. JBI Evid. Implement. 2019, 17, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Leader, J.K.; Boston, J.R.; Rudy, T.E.; Greco, C.M.; Zaki, H.S. Relation of jaw sounds and kinematics visualized and quantified using 3-D computer animation. Med. Eng. Phys. 2003, 25, 191–200. [Google Scholar] [CrossRef]
- De Felicio, C.M.; Mapelli, A.; Sidequersky, F.V.; Tartaglia, G.M.; Sforza, C. Mandibular kinematics and masticatory muscles EMG in patients with short lasting TMD of mild-moderate severity. J. Electromyogr. Kinesiol. 2013, 23, 627–633. [Google Scholar] [CrossRef]
- Sforza, C.; Ugolini, A.; Rocchetta, D.; Galante, D.; Mapelli, A.; Giannì, A.B. Mandibular kinematics after orthognathic surgical treatment. A pilot study. Br. J. Oral Maxillofac. Surg. 2010, 48, 110–114. [Google Scholar] [CrossRef]
- Ugolini, A.; Mapelli, A.; Segu, M.; Galante, D.; Sidequersky, F.V.; Sforza, C. Kinematic analysis of mandibular motion before and after orthognathic surgery for skeletal Class III malocclusion: A pilot study. CRANIO J. Craniomandib. Sleep Pract. 2017, 35, 94–100. [Google Scholar] [CrossRef]
- Linsen, S.S.; Schön, A.; Mercuri, L.G.; Teschke, M. Unilateral, Alloplastic Temporomandibular Joint Reconstruction, Biomechanically What Happens to the Contralateral Joint? A Prospective Cohort Study. J. Oral Maxillofac. Surg. 2021, 79, 2016–2029. [Google Scholar] [CrossRef]
- Hüe, O. Condylar paths during protrusion in edentulous patients: Analysis with electronic axiography. J. Prosthodont. 2011, 20, 294–298. [Google Scholar] [CrossRef]
- Ko, E.W.-C.; Huang, C.S.; Lo, L.-J.; Chen, Y.-R. Longitudinal observation of mandibular motion pattern in patients with skeletal class III malocclusion subsequent to orthognathic surgery. J. Oral Maxillofac. Surg. 2012, 70, e158–e168. [Google Scholar]
- Linsen, S.S.; Wolf, M.; Mussig, D. Long-term outcomes of mandibular kinematics following class II malocclusion therapy with removable functional appliance therapy. CRANIO J. Craniomandib. Sleep Pract. 2016, 34, 363–370. [Google Scholar] [CrossRef]
- Coutant, J.-C.; Mesnard, M.; Morlier, J.; Ballu, A.; Cid, M. Discrimination of objective kinematic characters in temporomandibular joint displacements. Arch. Oral Biol. 2008, 53, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Lemoine, J.J.; Xia, J.J.; Gateno, J.; Liebschner, M.A.K. Radiographic analysis for jaw motion normalization. J. Oral Maxillofac. Surg. 2005, 63, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Sforza, C.; Ugolini, A.; Sozzi, D.; Galante, D.; Mapelli, A.; Bozzetti, A. Threedimensional mandibular motion after closed and open reduction of unilateral mandibular condylar process fractures. J. Cranio-Maxillofacial Surg. 2011, 39, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, O.; Küppers, N.; Rosin, M.; Meyer, G. Comparative tests of arbitrary and kinematic transverse horizontal axis recordings of mandibular movements, J. Prosthet. Dent. 2003, 89, 175–179. [Google Scholar] [CrossRef]
- Ghodsi, S.; Rasaeipour, S. Revising average condylar inclinations using electronic pantograph assessment: A cross-sectional study. Dent. Hypotheses. 2018, 9, 84–89. [Google Scholar]
- Hirai, S.; Ogawa, T.; Shigeta, Y.; Ando, E.; Hirabayashi, R.; Ikawa, T.; Kasama, S.; Fukushima, S.; Matsuka, Y. Characteristics of mandibular movements in patients with square mandible. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, e75–e81. [Google Scholar] [CrossRef]
- Sadat-Khonsari, R.; Fenske, C.; Kahl-Nieke, B.; Kirsch, I.; Jüde, H.D. Mandibular instantaneous centers of rotation in patients with and without temporomandibular dysfunction. J. Orofac. Orthop. 2003, 64, 256–264. [Google Scholar] [CrossRef]
- Sadat-Khonsari, R.; Fenske, C.; Kahl-Nieke, B.; Kirsch, I.; Jüde, H.D. The helical axis of the mandible during the opening and closing movement of the mouth. J. Orofac. Orthop. 2003, 64, 178–185. [Google Scholar] [CrossRef]
- Kiseri, B.; Dayan, Ç.; Yildiz, M.; Sülün, T. The correlation between direction and amount of retrusive movement and condyle position and joint space. CRANIO J. Craniomandib. Sleep Pract. 2018, 36, 250–256. [Google Scholar] [CrossRef]
- Ko, E.W.-C.; Alazizi, A.I.; Lin, C.-H. Three-dimensional surgical changes of mandibular proximal segments affect outcome of jaw motion analysis. J. Oral Maxillofac. Surg. 2015, 73, 971–984. [Google Scholar]
- Kordaß, B.; Bernhardt, O.; Ratzmann, A.; Hugger, S.; Hugger, A. Standard and limit values of mandibular condylar and incisal movement capacity. Int. J. Comput. Dent. 2014, 17, 9–20. [Google Scholar] [PubMed]
- Ratzmann, A.; Mundt, T.; Schwahn, C.; Langforth, G.; Hützen, D.; Gedrange, T.; Kordaß, B. Comparative clinical investigation of horizontal condylar inclination using the JMA electronic recording system and a protrusive wax record for setting articulators. Int. J. Comput. Dent. 2007, 10, 265–284. [Google Scholar] [PubMed]
- Schwestka-Polly, R.; Kubein-Meesenburg, D.; Nagerl, H.; Fanghanel, J.; Miehe, B. Alteration of the functional condition of the mandible during clinical treatment. Ann. Anat. 1999, 181, 45–50. [Google Scholar] [CrossRef]
- Stiesch-Scholz, M.; Demling, A.; Rossbach, A. Reproducibility of jaw movements in patients with craniomandibular disorders. J. Oral Rehabil. 2006, 33, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Teng, T.T.-Y.; Ko, E.W.-C.; Huang, C.S.; Chen, Y.-R. The Effect of early physiotherapy on the recovery of mandibular function after orthognathic surgery for Class III correction: Part I - Jaw-motion analysis. J. Cranio-Maxillofacial Surg. 2015, 43, 131–137. [Google Scholar] [CrossRef]
- Wang, D.; Fu, H.; Zeng, R.; Yang, X. Changes of mandibular movement tracings after the correction of mandibular protrusion by bilateral sagittal split ramus osteotomy. J. Oral Maxillofac. Surg. 2009, 67, 2238–2244. [Google Scholar] [CrossRef]
- Yen, C.-I.; Chou, P.-Y.; Chen, C.-H.; Chen, T.-Y.; Chen, C.-T.; Lin, W.-Y.; Lee, M.-Y. Kinematic, Kinetic and surface electromyography analysis following zygomatic fracture reconstruction. J. Med. Biol. Eng. 2017, 37, 468–473. [Google Scholar] [CrossRef]
- Baeyens, J.P.; Gilomen, H.; Erdmann, B.; Clijsen, R.; Cabri, J.; Vissers, D. In vivo measurement of the 3D kinematics of the temporomandibular joint using miniaturized electromagnetic trackers: Technical report. Med. Biol. Eng. Comput. 2013, 51, 479–484. [Google Scholar] [CrossRef]
- Baltali, E.; Zhao, K.D.; Koff, M.F.; Durmus, E.; An, K.-N.; Keller, E.E. A method for quantifying condylar motion in patients with osteoarthritis using an electromagnetic tracking device and computed tomography imaging. J. Oral Maxillofac. Surg. 2008, 66, 848–857. [Google Scholar] [CrossRef]
- Keller, E.E.; Baltali, E.; Liang, X.; Zhao, K.; Huebner, M.; An, K.-N. Temporomandibular custom hemijoint replacement prosthesis: Prospective clinical and kinematic study. J. Oral Maxillofac. Surg. 2012, 70, 276–288. [Google Scholar] [CrossRef]
- Minami, I.; Wirianski, A.; Harakawa, R.; Wakabayashi, N.; Murray, G.M. The three-axial gyroscope sensor detects the turning point between opening and closing phases of chewing. Clin. Exp. Dent. Res. 2018, 4, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, T.; Nishigawa, K.; Bando, E.; Hosoki, M. Effect of different head positions on the jaw closing point during tapping movements. J. Oral Rehabil. 2009, 36, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.R.; Han, J.J.; Kim, D.-S.; Yi, W.-J.; Hwang, S.J. Evaluation of intraarticular distance narrowing during tem-poromandibular joint movement in patients with facial asymmetry using 3-dimensional computed tomography image and tracking camera system. J. Cranio-Maxillofacial Surg. 2015, 43, 342–348. [Google Scholar] [CrossRef]
- Ettlin, D.A.; Mang, H.; Colombo, V.; Palla, S.; Gallo, L.M. Stereometric assessment of TMJ space variation by occlusal splints. J. Dent. Res. 2008, 87, 877–881. [Google Scholar] [CrossRef] [PubMed]
- Fushima, K.; Gallo, L.M.; Krebs, M.; Palla, S. Analysis of the TMJ intraarticular space variation: A non-invasive insight during mastication. Med. Eng. Phys. 2003, 25, 181–190. [Google Scholar] [CrossRef]
- Gallo, L.M.; Gössi, D.B.; Colombo, V.; Palla, S. Relationship between kinematic center and TMJ anatomy and function. J. Dent. Res. 2008, 87, 726–730. [Google Scholar] [CrossRef]
- Goto, T.K.; Langenbach, G.E.J.; Hannam, A.G. Length changes in the human masseter muscle after jaw movement. Anat. Rec. 2001, 262, 293–300. [Google Scholar] [CrossRef]
- Hayasaki, H.; Saitoh, I.; Iwase, Y.; Inada, E.; Hasegawa, H.; Tokutomi, J.; Matsumoto, Y.; Yamasaki, Y. Movement of the instantaneous center of rotation and the position of the lateral excursion center during lateral excursion. CRANIO J. Craniomandib. Sleep Pract. 2008, 26, 253–262. [Google Scholar]
- Kim, D.-S.; Choi, S.-C.; Lee, S.-S.; Heo, M.-S.; Huh, K.-H.; Hwang, S.-J.; Kim, S.-H.; Yi, W.-J. Principal direction of inertia for 3D trajectories from patientspecific TMJ movement. Comput. Biol. Med. 2013, 43, 169–175. [Google Scholar] [CrossRef]
- Kim, S.-G.; Kim, D.-S.; Choi, S.-C.; Lee, S.-S.; Heo, M.-S.; Huh, K.-H.; Hwang, S.-J.; Yi, W.-J. The relationship between three-dimensional principal rotations and mandibular deviation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 110, 52–60. [Google Scholar] [CrossRef]
- Kubota, N.; Hayasaki, H.; Saitoh, I.; Iwase, Y.; Maruyama, T.; Inada, E.; Hasegawa, H.; Yamada, C.; Takemoto, Y.; Matsumoto, Y.; et al. Jaw motion during gum-chewing in children with primary dentition. CRANIO J. Craniomandib. Sleep Pract. 2010, 28, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Wojczynska, A.; Gallo, L.M.; Bredell, M.; Leiggener, C.S. Alterations of mandibular movement patterns after total joint replacement: A case series of long-term outcomes in patients with total alloplastic temporomandibular joint reconstructions. Int. J. Oral Maxillofac. Surg. 2019, 48, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Yashiro, K.; Iwata, A.; Takada, K.; Murakami, S.; Uchiyama, Y.; Furukawa, S. Temporomandibular joint articulations on working side during chewing in adult females with cross-bite and mandibular asymmetry. J. Oral Rehabil. 2015, 42, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Yashiro, K.; Yamamoto, K.; Takada, K.; Murakami, S.; Uchiyama, Y.; Furukawa, S. Influence of balancing-side occlusal interference on smoothness of working-side condylar movement and intra-articular space in chewing efforts. J. Oral Rehabil. 2015, 42, 10–17. [Google Scholar] [CrossRef]
- Zaugg, B.; Hämmerle, C.H.F.; Palla, S.; Gallo, L.M. Implant-supported mandibular splinting affects temporomandibular joint biomechanics. Clin. Oral Implants Res. 2012, 23, 897–901. [Google Scholar] [CrossRef]
- Abbink, J.H.; Van Der Bilt, A.; Bosman, F.; Van Der Glas, H.W. Speed-dependent control of cyclic open-close movements of the human jaw with an externalforce counteracting closing. J. Dent. Res. 1999, 78, 878–886. [Google Scholar] [CrossRef]
- Amhamed, M.; Whittle, T.; Maulina, T.; Gal, J.; Akhter, R.; Murray, G.M. Effect of experimental anterior temporalis muscle pain on jaw movements. J. Oral Rehabil. 2016, 43, 889–899. [Google Scholar] [CrossRef]
- Bhaskaracharya, M.; Memon, S.M.; Whittle, T.; Murray, G.M. Jaw movements in patients with a history of pain: An exploratory study. J. Oral Rehabil. 2015, 42, 18–26. [Google Scholar] [CrossRef]
- Buschang, P.H.; Throckmorton, G.S.; Travers, K.H.; Hayasaki, H. Incisor and mandibular condylar movements of young adult females during maximum protrusion and lateratrusion of the jaw. Arch. Oral Biol. 2001, 46, 39–48. [Google Scholar] [CrossRef]
- Buschang, P.H.; Hayasaki, H.; Throckmorton, G.S. Quantification of human chewing-cycle kinematics. Arch. Oral Biol. 2000, 45, 461–474. [Google Scholar] [CrossRef]
- Calixtre, L.B.; Nakagawa, T.H.; Alburquerque-Sendin, F.; da Silva Gruninger, B.L.; de Sena Rosa, L.R.; Oliveira, A.B. Inter- and intra-rater reliability of 3D kinematics during maximum mouth opening of asymptomatic subjects. J. Biomech. 2017, 64, 245–252. [Google Scholar] [CrossRef] [PubMed]
- C´atic, A.; Naeije, M. Location of the hinge axis and the kinematic centre in asymptomatic and clicking temporo-mandibular joints. J. Oral Rehabil. 1999, 26, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Crane, E.A.; Rothman, E.D.; Childers, D.; Gerstner, G.E. Analysis of temporal variation in human masticatory cycles during gum chewing. Arch. Oral Biol. 2013, 58, 1464–1474. [Google Scholar] [CrossRef] [PubMed]
- Gallo, L.M.; Fushima, K.; Palla, S. Mandibular helical axis pathways during mastication. J. Dent. Res. 2000, 79, 1566–1572. [Google Scholar] [CrossRef] [PubMed]
- Gallo, L.M.; Brasi, M.; Ernst, B.; Palla, S. Relevance of mandibular helical axis analysis in functional and dysfunctional TMJs. J. Biomech. 2006, 39, 1716–1725. [Google Scholar] [CrossRef]
- Gerstner, G.E.; Lafia, C.; Lin, D. Predicting masticatory jaw movements from chin movements using multivariate linear methods. J. Biomech. 2005, 38, 1991–1999. [Google Scholar] [CrossRef]
- Hayashi, K.; Reich, B.; Delong, R.; Lee, S.-P.; Mizoguchi, I. A novel statistical model for mandibular helical axis analysis. J. Oral Rehabil. 2009, 36, 102–109. [Google Scholar] [CrossRef]
- Hayashi, K.; Hayashi, M.; Reich, B.; Lee, S.-P.; Sachdeva, A.U.C.; Mizoguchi, I. Functional data analysis of mandibular movement using third-degree b-spline basis functions and self-modeling regression. Orthod. Waves. 2012, 71, 17–25. [Google Scholar] [CrossRef]
- Leader, J.K.; Boston, J.R.; Rudy, T.E.; Greco, C.M.; Zaki, H.S. Use of sound and jaw movement patterns to characterize patients with temporomandibulardisorders. Annu. Int. Conf IEEE Eng. Med. Biol. Proc. 1997, 4, 1729–1732. [Google Scholar]
- Lewis, R.P.; Buschang, P.H.; Throckmorton, G.S. Sex differences in mandibular movements during opening and closing. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 294–303. [Google Scholar] [CrossRef]
- Lobbezoo, F.; Zwijnenburg, A.J.; Naeije, M. Functional subdivision of the human masseter and temporalis muscles as shown by the condylar movement response to electrical muscle stimulation. J. Oral Rehabil. 2000, 27, 887–892. [Google Scholar] [CrossRef]
- Naeije, M. Local kinematic and anthropometric factors related to the maximum mouth opening in healthy individuals. J. Oral Rehabil. 2002, 29, 534–539. [Google Scholar] [CrossRef]
- Naeije, M.; Hofman, N. Biomechanics of the human temporomandibular joint during chewing. J. Dent. Res. 2003, 82, 528–531. [Google Scholar] [CrossRef] [PubMed]
- Ostry, D.J.; Vatikiotis-Bateson, E.; Gribble, P.L. An examination of the degrees of freedom of human jaw motion in speech and mastication. J. Speech Lang. Hear. Res. 1997, 40, 1341–1351. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T.; Koyano, K.; Umemoto, G. Inclination of the occlusal plane and occlusal guidance as contributing factors in mastication. J. Dent. 1998, 26, 641–647. [Google Scholar] [CrossRef]
- Remijn, L.; Groen, B.E.; Speyer, R.; van Limbeek, J.; Vermaire, J.A.; van den Engel-Hoek, L.; Nijhuis-van der Sanden, M.W.G. Can mastication in children with cerebral palsy be analyzed by clinical observation, dynamic ultrasound and 3D kinematics? J. Electromyogr. Kinesiol. 2017, 32, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Sforza, C.; Tartaglia, G.M.; Lovecchio, N.; Ugolini, A.; Monteverdi, R.; Giannì, A.B.; Ferrario, V.F. Mandibular movements at maximum mouth opening and EMG activity of masticatory and neck muscles in patients rehabilitated after a mandibular condyle fracture. J. Cranio-Maxillofacial Surg. 2009, 37, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Shiller, D.M.; Ostry, D.J.; Gribble, P.L. Effects of gravitational load on jaw movements in speech. J. Neurosci. 1999, 19, 9073–9080. [Google Scholar] [CrossRef]
- Shiller, D.M.; Ostry, D.J.; Gribble, P.L.; Laboissière, R. Compensation for the effects of head acceleration on jaw movement in speech. J. Neurosci. 2001, 21, 6447–6456. [Google Scholar] [CrossRef] [Green Version]
- Siegler, S.; Hayes, R.; Nicolella, D.; Fielding, A. A technique to investigate the three-dimensional kinesiology of the human temporomandibular joint. J. Prosthet. Dent. 1991, 65, 833–839. [Google Scholar] [CrossRef]
- Slater, J.; Visscher, C.M.; Lobbezoo, F.; Naeije, M. The intra-articular distance within the TMJ during free and loaded closing movements. J. Dent. Res. 1999, 78, 1815–1820. [Google Scholar] [CrossRef] [PubMed]
- Tomonari, H.; Kwon, S.; Kuninori, T.; Miyawaki, S. Differences between the chewing and non-chewing sides of the mandibular first molars and condyles in the closing phase during chewing in normal subjects. Arch. Oral Biol. 2017, 81, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Travers, K.H.; Buschang, P.H.; Hayasaki, H.; Throckmorton, G.S. Associations between incisor and mandibular condylar movements during maximum mouth opening in humans. Arch. Oral Biol. 2000, 45, 267–275. [Google Scholar] [CrossRef]
- Zhao, N.N.; Whittle, T.; Murray, G.M.; Peck, C.C. The effects of capsaicin induced intraoral mucosal pain on jaw movements in humans. J. Oral Facial Pain Headache. 2012, 26, 277–287. [Google Scholar]
- Dos Santos, D.M.; Lucareli, P.R.; Borges Barbosa, B.R.; Alves de Azevedo, L.M.; Leonardis, M.N.; Fonseca, F.F.; de Carvalho, L.S.; Gonzalez, T.D.O.; Politti, F.; Biasotto-Gonzalez, D.A. Reproducibility of a three-dimensional jaw model during opening and lateral excursion tests. Gait Posture. 2019, 73, 529–530. [Google Scholar]
- Dos Santos, D.M.; Politti, F.; de Azevedo, L.M.A.; de Cassia das Neves Martins, R.; Ricci, F.C.; Masuda, K.S.Y.; Muramoto do Nascimento, E.M.; Spinato, I.L.; de Paula Gomes, C.A.F.; Biasotto-Gonzalez, D.A. Association between convergence insufficiency and temporomandibular disorder cross-sectional study. Clin. Oral Investigations. 2021, 25, 851–858. [Google Scholar] [CrossRef]
- Ernst, M.; Schenkenberger, A.E.; Domin, M.; Kordass, B.; Lotze, M. Effects of centric mandibular splint therapy on orofacial pain and cerebral activation patterns. Clin. Oral Investigations. 2020, 24, 2005–2013. [Google Scholar] [CrossRef]
- Choi, D.D.; Vandenberg, K.; Smith, D.; Davis, C.; McCain, J.P. Is Temporomandibular Joint Arthroscopy Effective in Managing Pediatric Temporomandibular Joint Disorders in the Short- and Long-Term? J. Oral Maxillofac Surg. 2020, 78, 44–51. [Google Scholar] [CrossRef]
- Feng, Y.; Shu, J.; Liu, Y.; Zheng, T.; Shao, B.; Liu, Z. Biomechanical analysis of temporomandibular joints during mandibular pro-trusion and retraction motions: A 3d finite element simulation. Comput. Methods Programs Biomed. 2021, 208, 106299. [Google Scholar] [CrossRef]
- Shu, J.; Ma, H.; Jia, L.; Fang, H.; Chong, D.Y.R.; Zheng, T.; Yao, J.; Liu, Z. Biomechanical behaviour of temporomandibular joints during opening and closing of the mouth: A 3D finite element analysis. Int. J. Numer. Methods Biomed. Eng. 2020, 8, e3373. [Google Scholar] [CrossRef]
- Shu, J.; Ma, H.; Xiong, X.; Shao, B.; Zheng, T.; Liu, Y.; Liu, Z. Mathematical analysis of the condylar trajectories in asymptomatic subjects during mandibular motions. Med. Biol. Eng. Comput. 2021, 59, 901–911. [Google Scholar] [CrossRef] [PubMed]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population/Participant | Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications, in Particular Myofascial Pain, Anterior Disk Displacement with or without Joint Noises, Arthralgia, Osteoarthritis, and Osteoarthrosis for at Least 3 Months. |
|---|---|
| Intervention | TMD conservative treatment and non-surgical intervention. |
| Comparison/Control | Asymptomatic subjects with different types of occlusion. |
| Outcome | Maximum mouth opening (MMO), Incisor displacement at MMO (IP-MMO), Condylar inclination, Horizontal and Sagittal angles. |
| Main finding | Heterogeneous variables and outcomes found to assess the TMJ kinematics. No gold standard outcome was found. No standardised control was found. Maximum mouth opening was commonly compared outcomes Different diagnostic methods were used for assessing TMD kinematics and among these methods could not be used as gold standard. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scolaro, A.; Khijmatgar, S.; Rai, P.M.; Falsarone, F.; Alicchio, F.; Mosca, A.; Greco, C.; Del Fabbro, M.; Tartaglia, G.M. Efficacy of Kinematic Parameters for Assessment of Temporomandibular Joint Function and Disfunction: A Systematic Review and Meta-Analysis. Bioengineering 2022, 9, 269. https://doi.org/10.3390/bioengineering9070269
Scolaro A, Khijmatgar S, Rai PM, Falsarone F, Alicchio F, Mosca A, Greco C, Del Fabbro M, Tartaglia GM. Efficacy of Kinematic Parameters for Assessment of Temporomandibular Joint Function and Disfunction: A Systematic Review and Meta-Analysis. Bioengineering. 2022; 9(7):269. https://doi.org/10.3390/bioengineering9070269
Chicago/Turabian StyleScolaro, Alessandra, Shahnawaz Khijmatgar, Pooja Mali Rai, Francesca Falsarone, Francesca Alicchio, Arianna Mosca, Christian Greco, Massimo Del Fabbro, and Gianluca Martino Tartaglia. 2022. "Efficacy of Kinematic Parameters for Assessment of Temporomandibular Joint Function and Disfunction: A Systematic Review and Meta-Analysis" Bioengineering 9, no. 7: 269. https://doi.org/10.3390/bioengineering9070269