
Heart Rate Variability Analysis for Seizure Detection in Neonatal Intensive Care Units

 , , ,
, , ,
Abstract
:1. Introduction
2. Dataset
3. Methods
3.1. ECG Windowing and RR Time Series Extraction
3.2. Features Extraction
3.3. Feature Selection, Classification and Validation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gaussian SVM | |
|---|---|
| Hyperparameters | Short Description |
| Box Constraints | Regularization term that controls the number of misclassifications [68]. |
| Kernel Scale | Scaling parameter for the input data preventing some features that have a wider range than others from becoming dominant in the kernel calculation. |
| Costs | Misclassification costs introduced to mitigate the class imbalance that occurs when one class has a smaller number of examples compared to the other. |
4. Performance Metrics
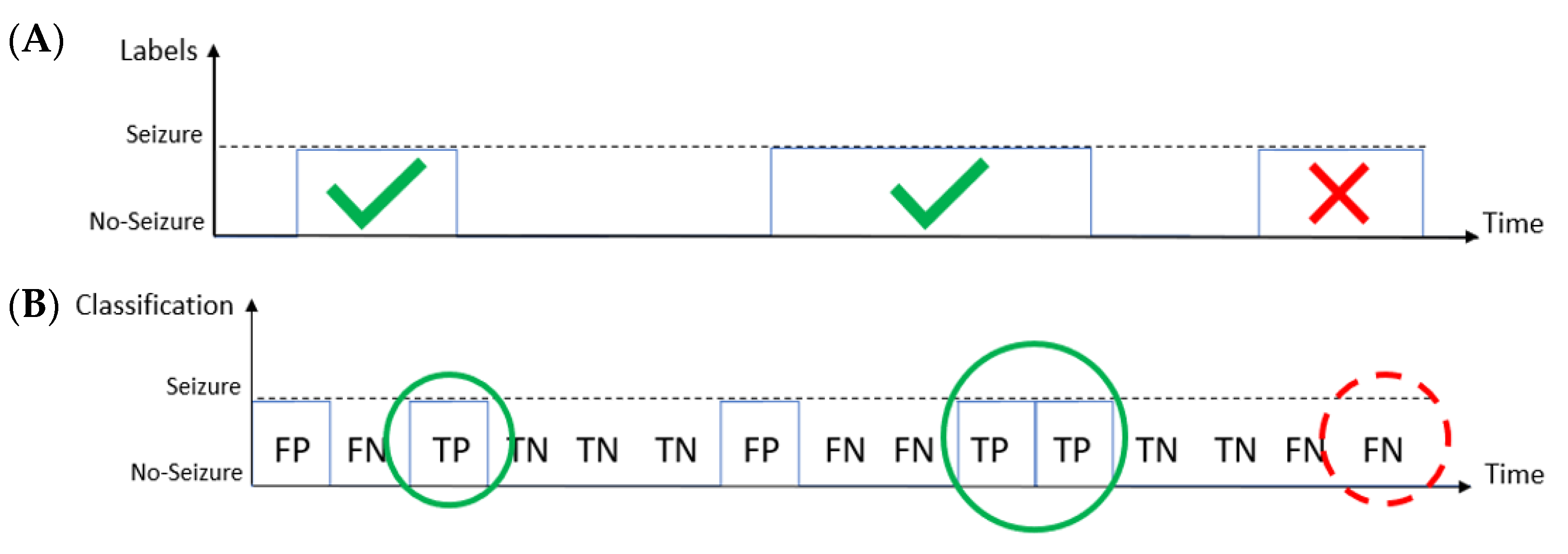
- Good Detection Rate (GDR): the overall percentage of the seizure events correctly identified by the system [44]. A seizure event is correctly identified if the system detects at least one epoch during the event.
- False Discovery Rate (FDR): the overall percentage of the seizure events incorrectly identified by the system [44].
- False Detection per Hour (FDH): the number of seizure events identified by the system in 1 h that have no overlap with the events labeled by the expert [44].
5. Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pisani, F.; Spagnoli, C.; Falsaperla, R.; Nagarajan, L.; Ramantani, G. Seizures in the neonate: A review of etiologies and outcomes. Seizure 2021, 85, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Ramantani, G. Neonatal epilepsy and underlying aetiology: To what extent do seizures and EEG abnormalities influence outcome? Epileptic Disord 2013, 15, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Apers, W.M.J.; de Vries, L.S.; Groenendaal, F.; Toet, M.C.; Weeke, L.C. Delay in treatment of neonatal seizures: A retrospective cohort study. Neonatology 2020, 117, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Pressler, R.M.; Lagae, L. Why we urgently improved seizure and epilepsy therapies for children and neonates. Neuropharmacology 2020, 170, 107854. [Google Scholar] [CrossRef] [PubMed]
- Shellhaas, R.A.; Chang, T.; Tsuchida, T.; Scher, M.S.; Riviello, J.J.; Abend, N.S.; Nguyen, S.; Wusthoff, C.J.; Clancy, R.R. The American Clinical Neurophysiology Society’s Guideline on Continuous Electroencephalography Monitoring in Neonates. J. Clin. Neurophysiol. Off. Publ. Am. Electroencephalogr. Soc. 2011, 28, 611–617. [Google Scholar] [CrossRef] [Green Version]
- Pisani, F.; Pavlidis, E. The role of electroencephalogram in neonatal seizure detection. Expert Rev. Neurother. 2017, 18, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Olmi, B.; Frassineti, L.; Lanatà, A.; Manfredi, C. Automatic Detection of Epileptic Seizures in Neonatal Intensive Care Units Through EEG, ECG and Video Recordings: A Survey. IEEE Access 2021, 9, 138174–138191. [Google Scholar] [CrossRef]
- Malarvili, M.B.; Mesbah, M.; Boashash, B. Time-Frequency Analysis of Heart Rate Variability for Neonatal Seizure Detection. EURASIP J. Adv. Signal Process. 2007, 2007, 050396. [Google Scholar] [CrossRef] [Green Version]
- Greene, B.R.; de Chazal, P.; Boylan, G.B.; Connolly, S.; Reilly, R. Electrocardiogram Based Neonatal Seizure Detection. IEEE Trans. Biomed. Eng. 2007, 54, 673–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, O.M.; Temko, A.; Marnane, W.; Lightbody, G. Heart rate based automatic seizure detection in the newborn. Med. Eng. Phys. 2010, 32, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Ntonfo, G.K.; Ferrari, G.; Lofino, F.; Raheli, R.; Pisani, F. Extraction of video features for real-time detection of neonatal seizures. In Proceedings of the 2011 IEEE International Symposium on a World of Wireless, Mobile and Multimedia Networks, Lucca, Italy, 20–24 June 2011; pp. 1–6. [Google Scholar] [CrossRef]
- Statello, R.; Carnevali, L.; Sgoifo, A.; Miragoli, M.; Pisani, F. Heart rate variability in neonatal seizures: Investigation and implications for management. Neurophysiol. Clin. 2021, 51, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Ntonfo, G.; Lofino, F.; Ferrari, G.; Raheli, R.; Pisani, F. Video processing-based detection of neonatal seizures by trajectory features clustering. In Proceedings of the IEEE International Conference on Communications, Ottawa, ON, Canada, 10–15 June 2012; pp. 3456–3460. [Google Scholar] [CrossRef]
- Pisani, F.; Spagnoli, C.; Pavlidis, E.; Facini, C.; Ntonfo, G.K.; Ferrari, G.; Raheli, R. Real-time automated detection of clonic seizures in newborns. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2014, 125, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Cattani, L.; Alinovi, D.; Ferrari, G.; Raheli, R.; Pavlidis, E.; Spagnoli, C.; Pisani, F. Monitoring infants by automatic video processing: A unified approach to motion analysis. Comput. Biol. Med. 2017, 80, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Karayiannis, N.B.; Srinivasan, S.; Bhattacharya, R.; Wise, M.; Frost, J.D., Jr.; Mizrahi, E.M. Extraction of motion strength and motor activity signals from video recordings of neonatal seizures. IEEE Trans. Med. Imaging 2011, 20, 965–980. [Google Scholar] [CrossRef] [PubMed]
- Karayiannis, N.B.; Tao, G. Improving the extraction of temporal motion strength signals from video recording of neonatal seizures. In Proceedings of the IEEE Conference on Advanced Video and Signal Based Surveillance (AVSS03), Miami, FL, USA, 22–22 July 2003. [Google Scholar] [CrossRef] [Green Version]
- Karayiannis, N.B.; Tao, G. An improved procedure for the extraction of temporal motion strength signals from video recordings of neonatal seizures. Image Vis. Comput. 2006, 24, 27–40. [Google Scholar] [CrossRef]
- Karayiannis, N.B.; Tao, G.; Xiong, Y.; Sami, A.; Varughese, B.; Frost, J.D., Jr.; Wise, M.S.; Mizrahi, E.M. Computerized Motion Analysis of Videotaped Neonatal Seizures of Epileptic Origin. Epilepsia 2005, 46, 901–917. [Google Scholar] [CrossRef]
- Li, L.M.; Roche, J.; Sander, J.W. Ictal ECG changes in temporal lobe epilepsy. Arq. Neuro-Psiquiatr. 1995, 53, 619–624. [Google Scholar] [CrossRef] [Green Version]
- Moridani, M.K.; Farhadi, H. Heart rate variability as a biomarker for epilepsy seizure prediction. Bratisl. Lek. Listy 2017, 118, 3–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponnusamy, A.; Marques, J.L.; Reuber, M. Comparison of heart rate variability parameters during complex partial seizures and psychogenic nonepileptic seizures. Epilepsia 2012, 53, 1314–1321. [Google Scholar] [CrossRef]
- Bersani, I.; Piersigilli, F.; Gazzolo, D.; Campi, F.; Savarese, I.; Dotta, A.; Tamborrino, P.P.; Auriti, C.; Di Mambro, C. Heart rate variability as possible marker of brain damage in neonates with hypoxic ischemic encephalopathy: A systematic review. Eur. J. Nucl. Med. Mol. Imaging 2021, 180, 1335–1345. [Google Scholar] [CrossRef]
- Lucchini, M.; Fifer, W.P.; Sahni, R.; Signorini, M.G. Novel heart rate parameters for the assessment of autonomic nervous system function in premature infants. Physiol. Meas. 2016, 37, 1436–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statello, R.; Carnevali, L.; Alinovi, D.; Pisani, F.; Sgoifo, A. Heart rate variability in neonatal patients with seizures. Clin. Neurophysiol. 2018, 129, 2534–2540. [Google Scholar] [CrossRef]
- Goldberg, R.N.; Goldman, S.L.; Ramsay, R.E.; Feller, R. Detection of seizure activity in the paralyzed neonate using continuous monitoring. Pediatrics 1982, 69, 583586. [Google Scholar] [CrossRef]
- Watanabe, K.; Hara, K.; Miyazaki, S.; Kuroyanagi, M.; Asano, S.; Kondo, K.; Kuno, K.; Jose, H.; Iwase, K. Electroclinical studies of seizures in the newborn. Folia Psychiatr. Neurol. Jpn. 1977, 31, 383392. [Google Scholar] [CrossRef] [PubMed]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Voss, A.; Schulz, S.; Schroeder, R.; Baumert, M.; Caminal, P. Methods derived from nonlinear dynamics for analysing heart rate variability. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2009, 367, 277–296. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peltola, M.A. Role of editing of R-R intervals in the analysis of heart rate variability. Front. Physiol. 2012, 3, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frassineti, L.; Lanatà, A.; Olmi, B.; Manfredi, C. Multiscale Entropy Analysis of Heart Rate Variability in Neonatal Patients with and without Seizures. Bioengineering 2021, 8, 122. [Google Scholar] [CrossRef] [PubMed]
- De Cooman, T.; Varon, C.; Hunyadi, B.; Van Paesschen, W.; Lagae, L.; Van Huffel, S. Online Automated Seizure Detection in Temporal Lobe Epilepsy Patients Using Single-lead ECG. Int. J. Neural Syst. 2017, 27, 1750022. [Google Scholar] [CrossRef] [PubMed]
- Behbahani, S.; Dabanloo, N.J.; Nasrabadi, A.M.; Teixeira, C.A.; Dourado, A. A new algorithm for detection of epileptic seizures based on HRV signal. J. Exp. Theor. Artif. Intell. 2014, 26, 251–265. [Google Scholar] [CrossRef]
- Jeppesen, J.; Fuglsang-Frederiksen, A.; Johansen, P.; Christensen, J.; Wüstenhagen, S.; Tankisi, H.; Qerama, E.; Beniczky, S. Seizure detection using heart rate variability: A prospective validation study. Epilepsia 2020, 61, S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Frassineti, L.; Lanatà, A.; Manfredi, C. HRV analysis: A non-invasive approach to discriminate between newborns with and without seizures. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 52–55. [Google Scholar] [CrossRef]
- Pavel, A.M.; Rennie, J.M.; de Vries, L.S.; Blennow, M.; Foran, A.; Shah, D.K.; Pressler, R.M.; Kapellou, O.; Dempsey, E.M.; Mathieson, S.R.; et al. A machine-learning algorithm for neonatal seizure recognition: A multicentre, randomised, controlled trial. Lancet Child Adolesc. Health 2020, 4, 740–749. [Google Scholar] [CrossRef]
- Frassineti, L.; Manfredi, C.; Olmi, B.; Lanatà, A. A Generalized Linear Model for an ECG-based Neonatal Seizure Detector. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 471–474. [Google Scholar] [CrossRef]
- Panayiotopoulos, C.P. The Epilepsies: Seizures, Syndromes and Management; Bladon Medical Publishing: Oxfordshire, UK, 2005; Chapter 5. [Google Scholar]
- Pressler, R.M. Neonatal Seizures; Lecture notes of “The Fifteenth epilepsy teaching weekend on September 2015, Chapter 6; Epilepsy Society: Buckinghamshire, UK, 2015. [Google Scholar]
- Rennie, J.M. Neonatal seizures. Eur. J. Pediatrics 1997, 156, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Pressler, R.M.; Cilio, M.R.; Mizrahi, E.M.; Moshé, S.L.; Nunes, M.L.; Plouin, P.; Vanhatalo, S.; Yozawitz, E.; de Vries, L.S.; Puthenveettil Vinayan, K.; et al. The ILAE classification of seizures and the epilepsies: Modification for seizures in the neonate. Position paper by the ILAE Task Force on Neonatal Seizures. Epilepsia 2021, 62, 615–628. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://it.mathworks.com/products/new_products/release2020b.html (accessed on 28 March 2022).
- Temko, A.; Thomas, E.; Marnane, W.; Lightbody, G.; Boylan, G.B. Performance assessment for EEG-based neonatal seizure detectors. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2011, 122, 474–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bock, C.; Kovacs, P.; Laguna, P.; Meier, J.; Huemer, M. ECG Beat Representation and Delineation by means of Variable Projection. IEEE Trans. Biomed. Eng. 2021, 68, 2997–3008. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://it.mathworks.com/matlabcentral/fileexchange/45840-complete-pan-tompkins-implementation-ecg-qrs-detector (accessed on 28 March 2022).
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Pini, N.; Lucchini, M.; Fifer, W.; Burtchen, N.; Signorini, M.G. Lagged Transfer Entropy Analysis to Investigate Cardiorespiratory Regulation in Newborns during Sleep. In Proceedings of the 12th International Joint Conference on Biomedical Engineering Systems and Technologies, 12th International Conference on Bio-Inspired Systems and Signal Processing (BIOSTEC-BIOSIGNALS), Prague, Czech Republic, 22–24 February 2019; Volume 4, pp. 139–146. Available online: https://www.scitepress.org/ProceedingsDetails.aspx?ID=juQVHZgir3E=&t=1 (accessed on 28 March 2022). [CrossRef]
- Vollmer, M. A Robust, Simple and Reliable Measure of Heart Rate Variability using Relative RR Intervals. 2015. Comput. Cardiol. 2015, 42, 609–612. [Google Scholar]
- Costa, M.; Goldberger, A.; Peng, C.K. Multiscale entropy of biological signals. Phys. Review. E Stat. Nonlinear Soft Matter Phys. 2005, 71, 021906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.Y.; Choi, Y.S. Multiscale Distribution Entropy Analysis of Heart Rate Variability Using Differential Inter-Beat Intervals. IEEE Access 2020, 8, 48761–48773. [Google Scholar] [CrossRef]
- Humeau-Heurtier, A. Entropy Analysis in Health Informatics. In Signal Processing Techniques for Computational Health Informatics; Ahad, M.A.R., Ahmed, M.U., Eds.; Springer: Cham, Switzerland, 2020; Volume 192, pp. 123–143. [Google Scholar] [CrossRef]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [Green Version]
- Li, P.; Liu, C.; Li, K.; Zheng, D.; Liu, C.; Hou, Y. Assessing the complexity of short-term heartbeat interval series by distribution entropy. Med. Biol. Eng. Comput. 2015, 53, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Karmakar, C.; Udhayakumar, R.K.; Palaniswami, M. Distribution Entropy (DistEn): A complexity measure to detect arrhythmia from short length RR interval time series. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 5207–5210. [Google Scholar] [CrossRef]
- Karmakar, C.; Udhayakumar, R.; Li, P.; Venkatesh, S.; Palaniswami, M. Stability, Consistency and Performance of Distribution Entropy in Analysing Short Length Heart Rate Variability (HRV) Signal. Front. Physiol. 2017, 8, 720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yentes, J.M.; Hunt, N.; Schmid, K.K.; Kaipust, J.P.; McGrath, D.; Stergiou, N. The appropriate use of approximate entropy and sample entropy with short data sets. Ann. Biomed. Eng. 2013, 41, 349–365. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.D.; Wu, C.W.; Lee, K.Y.; Lin, S.G. Modified multiscale entropy for short-term time series analysis. Phys. A Stat. Mech. Its Appl. 2013, 392, 5865–5873. [Google Scholar] [CrossRef]
- Açıkoğlu, M.; Tuncer, S.A. Incorporating feature selection methods into a machine learning-based neonatal seizure diagnosis. Med. Hypotheses 2019, 135, 109464. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Long, F.; Ding, C. Feature selection based on mutual information criteria of max-dependency, max-relevance, and min-redundancy. IEEE Trans. Pattern Anal. Mach. Intell. August 2005, 27, 1226–1238. Available online: https://ranger.uta.edu/~chqding/papers/mRMR_PAMI.pdf (accessed on 28 March 2022). [CrossRef] [PubMed]
- Scherf, U.; Ross, D.T.; Waltham, M.; Smith, L.H.; Lee, J.K.; Tanabe, L.; Kohn, K.W.; Reinhold, W.C.; Myers, T.G.; Andrews, D.T.; et al. A gene expression database for the molecular pharmacology of cancer. Nat. Genet. 2000, 24, 236–244. [Google Scholar] [CrossRef]
- Memarian, N.; Kim, S.; Dewar, S.; Engel, J.; Staba, R. Multimodal data and machine learning for surgery outcome prediction in complicated cases of mesial temporal lobe epilepsy. Comput. Biol. Med. 2015, 64, 67–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, S.; Koller, D. Support vector machine active learning with applications to text classification. J. Mach. Learn. Res. 2001, 2, 45–66. [Google Scholar] [CrossRef]
- Available online: https://it.mathworks.com/help/stats/fitcsvm.html (accessed on 28 March 2022).
- Available online: https://it.mathworks.com/help/stats/fitclinear.html (accessed on 28 March 2022).
- Amin, S.; Kamboh, A.M. A robust approach towards epileptic seizure detection. In Proceedings of the 2016 IEEE International Workshop on Machine Learning for Signal Processing, Vietri sul Mare, Italy, 13–16 September 2016. [Google Scholar] [CrossRef]
- Awad, M.; Khanna, R. Support Vector Machines for Classification. In Efficient Learning Machines; Apress: Berkeley, CA, USA, 2015. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://it.mathworks.com/help/stats/classification-with-unequal-misclassification-costs.html (accessed on 28 March 2022).
- Temko, A.; Thomas, E.; Marnane, W.; Lightbody, G.; Boylan, G. EEG-based neonatal seizure detection with Support Vector Machines. Clin. Neurophysiol. 2011, 122, 464–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, E.M.; Temko, A.; Lightbody, G.; Marnane, W.P.; Boylan, G.B. Gaussian mixture models for classification of neonatal seizures using EEG. Physiol. Meas. 2010, 31, 1047–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansari, A.H.; Cherian, P.; Caicedo, A.; Jansen, K.; Dereymaeker, A.; Wispelaere, L.; Dielman, C.; Vervisch, J.; Govaert, P.; Vos, M.; et al. Weighted Performance Metrics for Automatic Neonatal Seizure Detection Using Multiscored EEG Data. IEEE J. Biomed. Health Inform. 2017, 22, 1114–1123. [Google Scholar] [CrossRef] [PubMed]
- Tapani, K.T.; Vanhatalo, S.; Stevenson, N.J. Time-Varying EEG Correlations Improve Automated Neonatal Seizure Detection. Int. J. Neural Syst. 2019, 29, 1850030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akyüz, E.; Üner, A.K.; Köklü, B.; Arulsamy, A.; Shaikh, M.F. Cardiorespiratory findings in epilepsy: A recent review on outcomes and pathophysiology. J. Neurosci. Res. 2021, 99, 2059–2073. [Google Scholar] [CrossRef] [PubMed]
- Hämmerle, P.; Eick, C.; Blum, S.; Schlageter, V.; Bauer, A.; Rizas, K.D.; Eken, C.; Coslovsky, M.; Aeschbacher, S.; Krisai, P.; et al. Heart Rate Variability Triangular Index as a Predictor of Cardiovascular Mortality in Patients with Atrial Fibrillation. J. Am. Heart Assoc. Cardiovasc. Cerebrovasc. Dis. 2020, 9, e016075. [Google Scholar] [CrossRef] [PubMed]
- Rajendra Acharya, U.; Paul Joseph, K.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, G.U.; Dogan, E.A.; Dogan, U.; Tokgoz, O.S.; Ozdemir, K.; Genc, B.O.; Ilhan, N. Analysis of 24-h heart rate variations in patients with epilepsy receiving antiepileptic drugs. Epilepsy Behav. EB 2011, 20, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Kolsal, E.; Serdaroğlu, A.; Cilsal, E.; Kula, S.; Soysal, A.Ş.; Kurt, A.N.; Arhan, E. Can heart rate variability in children with epilepsy be used to predict seizures? Seizure 2014, 23, 357–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volpe, J.J. Neonatal seizures. In Neurology of the Newborn, 4th ed.; Saunders: Philadelphia, PA, USA, 2001; pp. 178–214. [Google Scholar]
- O’regan, M.E.; Brown, J.K. Abnormalities in cardiac and respiratory function observed during seizures in childhood. Dev. Med. Child. Neurol. 2005, 47, 4–9. [Google Scholar] [CrossRef]
- Quint, S.R.; Messenheimer, J.A.; Tennison, M.B.; Nagle, H.T. Assessing autonomic activity from the EKG related to seizure onset detection and localization. In Proceedings of the Second Annual IEEE Symposium on Computer-Based Medical Systems, Minneapolis, MN, USA, 26–27 June 1989; pp. 2–9. Available online: https://ieeexplore.ieee.org/abstract/document/47350 (accessed on 28 March 2022). [CrossRef]
- Zijlmans, M.; Flanagan, D.; Gotman, J. Heart rate changes and ecg abnormalities during epileptic seizures: Prevalence and definition of an objective clinical sign. Epilepsia 2022, 43, 847–854. [Google Scholar] [CrossRef] [Green Version]
- Greene, B.R.; de Chazal, P.; Boylan, G.; Reilly, R.B.; O’Brien, C.; Connolly, S. Heart and respiration rate changes in the neonate during electroencephalographic seizure. Med. Biol. Eng. Comput. 2006, 44, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Valenza, G.; Greco, A.; Gentili, C.; Lanata, A.; Sebastiani, L.; Menicucci, D.; Gemignani, A.; Scilingo, E.P. Combining electroencephalographic activity and instantaneous heart rate for assessing brain–heart dynamics during visual emotional elicitation in healthy subjects. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2016, 374, 20150176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiecke, K.; Pester, B.; Piper, D.; Benninger, F.; Feucht, M.; Leistritz, L.; Witte, H. Nonlinear directed interactions between HRV and EEG activity in children with TLE. IEEE Trans. Biomed. Eng. 2016, 63, 2497–2504. [Google Scholar] [CrossRef] [PubMed]
- Hendrikx, D.; Thewissen, L.; Smits, A.; Naulaers, G.; Allegaert, K.; Van Huffel, S.; Caicedo, A. Using graph theory to assess the interaction between cerebral function, brain hemodynamics, and systemic variables in premature infants. Complexity 2018, 2018, 6504039. [Google Scholar] [CrossRef] [Green Version]









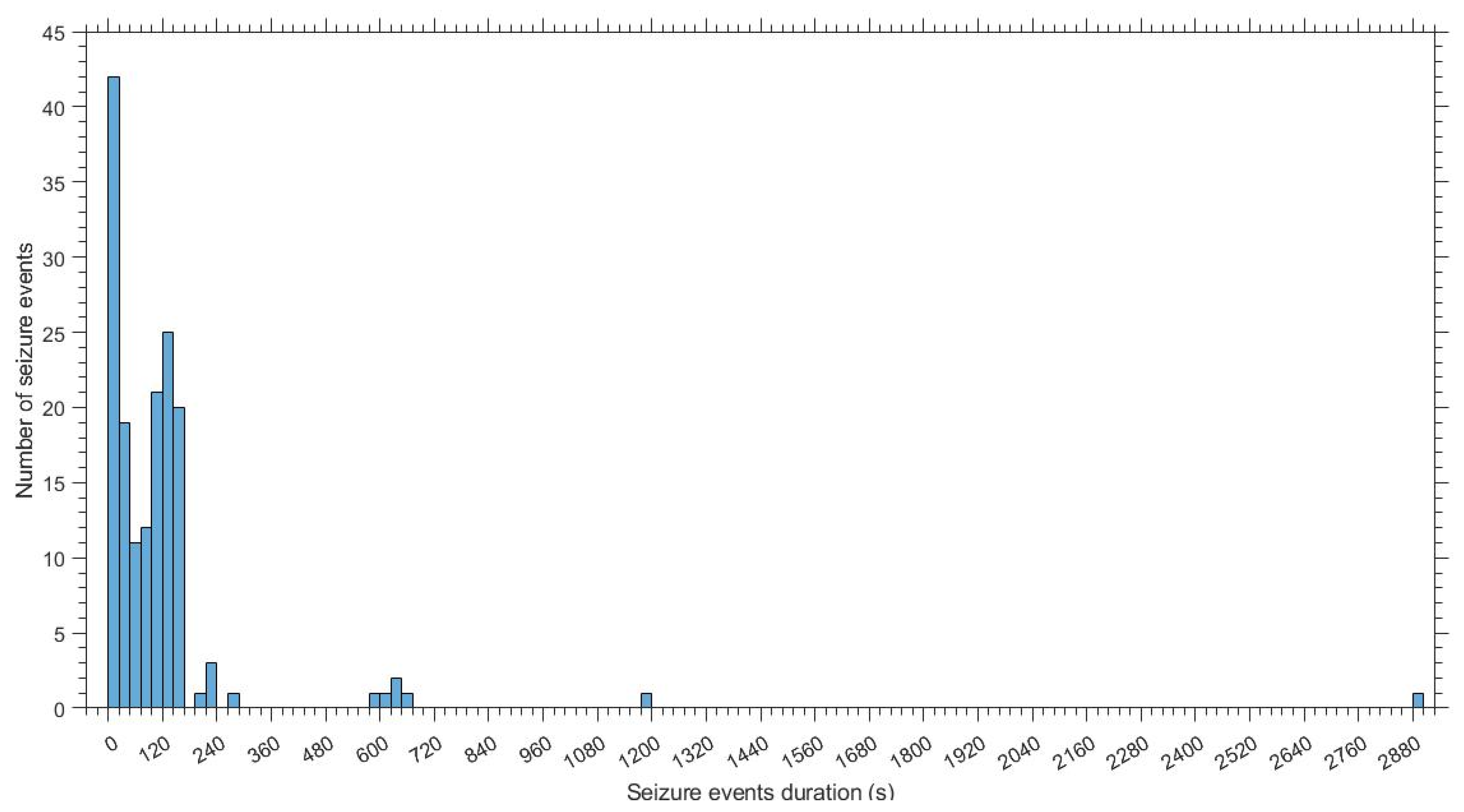
| Patients | Record Length (h) | Number of Seizure Events | Seizure Events Duration | Etiology | ||
|---|---|---|---|---|---|---|
| Average | Min | Max | ||||
| EGP1 | 01:08:29 | 1 | 00:03:40 | 00:03:40 | 00:03:40 | Metabolic |
| EGP2 | 01:09:34 | 8 | 00:00:24 | 00:00:12 | 00:00:43 | HIE |
| EGP3 | 01:10:15 | 1 | 00:00:31 | 00:00:31 | 00:00:31 | Other |
| EGP4 | 00:56:28 | 4 | 00:00:16 | 00:00:07 | 00:00:22 | HIE |
| EGP5 | 01:02:30 | 3 | 00:01:45 | 00:01:18 | 00:02:00 | HIE |
| EGP6 | 01:17:02 | 4 | 00:00:12 | 00:00:08 | 00:00:16 | HIE |
| EGP7 | 01:05:53 | 1 | 00:00:50 | 00:00:50 | 00:00:50 | HIE |
| EGP8 | 00:45:40 | 3 | 00:01:28 | 00:01:19 | 00:01:40 | HIE |
| EGP9 | 01:20:39 | 1 | 00:00:29 | 00:00:29 | 00:00:29 | Other |
| EGP10 | 00:58:22 | 1 | 00:01:40 | 00:01:40 | 00:01:40 | Other |
| ECP1 | 00:48:12 | 1 | 00:48:12 | 00:48:12 | 00:48:12 | Genetic |
| ECP2 | 00:54:31 | 13 | 00:01:48 | 00:00:27 | 00:09:49 | Metabolic |
| ECP3 | 01:04:14 | 6 | 00:02:49 | 00:01:20 | 00:04:40 | Stroke |
| ECP4 | 01:18:36 | 5 | 00:00:33 | 00:00:16 | 00:00:50 | Genetic |
| ECP5 | 01:00:10 | 3 | 00:07:54 | 00:01:56 | 00:19:45 | Other |
| ECP6 | 01:10:02 | 7 | 00:01:05 | 00:00:33 | 00:02:23 | HIE |
| ECP7 | 00:54:06 | 1 | 00:10:26 | 00:10:26 | 00:10:26 | Stroke |
| ECP8 | 01:00:43 | 10 | 00:02:53 | 00:01:19 | 00:11:04 | Other |
| ECP9 | 01:30:08 | 5 | 00:00:48 | 00:00:22 | 00:01:16 | HIE |
| ECP10 | 00:41:16 | 3 | 00:03:52 | 00:00:20 | 00:10:10 | Stroke |
| ECP11 | 01:01:02 | 8 | 00:00:52 | 00:00:26 | 00:02:01 | HIE |
| ECP12 | 01:20:06 | 3 | 00:01:58 | 00:01:19 | 00:02:31 | HIE |
| Total | 23:37:58 | 92 | ||||
| Feature | Unit of Measure | Short Description | |
|---|---|---|---|
| Time domain | SDSD | (ms) | Standard deviation of successive R-R interval differences |
| SDNN | (ms) | Standard deviation of R-R intervals | |
| RMSDD | (ms) | Root mean square of successive differences | |
| pNN50 | (%) | Probability of R-R intervals > 50 ms e < −50 ms | |
| TRI | - | Area of the histogram of R-R intervals divided by its maximum height | |
| TINN | (ms) | Width of the R-R intervals histogram evaluated trough triangular interpolation | |
| CD | - | Correlation dimension | |
| SD2 | (ms) | Standard deviation of Poincarè plot along the line-of-identity | |
| SD1SD2ratio | - | Ratio of standard deviation of Poincarè plot perpendicular to the line-of-identity to standard deviation of Poincarè plot along the line-of-identity | |
| HR | (beats/min) | Average heart rate | |
| Frequency domain | VLF | (ms2) | Spectral density (computed through FFT) of the linear interpolated R-R tachogram up to 0.04 Hz (very low frequency) [25] |
| LF | (ms2) | Spectral density (computed through FFT) of the linear interpolated R-R tachogram between 0.04 and 0.3 Hz (low frequency) [25] | |
| HF | (ms2) | Spectral density (computed through FFT) of the linear interpolated R-R tachogram between 0.3 and 1.3 Hz (high frequency) [25] | |
| LFHFratio | - | Ratio between spectral density of low frequency parts and high frequency parts | |
| TP | (ms2) | Total spectral density | |
| pLF | (%) | Percentage of spectral density of low frequency parts to total spectral density minus the spectral density of very low frequency parts | |
| pHF | (%) | Percentage of spectral density of high frequency parts to total spectral density minus the spectral density of very low frequency parts | |
| Information theory domain | ApEn | - | Approximate Entropy |
| Multiscale DistEn Scale (1–4) | - | Multiscale Distribution Entropy from scale 1 to scale 4 for the 180 s epochs; at scale 1 for the 60 s epochs | |
| Multiscale SampEn Scale (1–4) | - | Multiscale Sample Entropy from scale 1 to scale 4 for the 180 s epochs; at scale 1 for the 60 s epochs | |
| Total | 20 (60 s epochs)/26 (180 s epochs) |
| Linear SVM | |
|---|---|
| Hyperparameters | Short Description |
| λ | Regularization penalty term introduced to search for the hyperplane that maximizes the margin and minimizes the misclassifications. |
| Costs | Misclassification costs introduced to mitigate the class imbalance that occurs when one class has a smaller number of examples compared to the other. |
| Model | N° Features | Hyperparameters | AUC (%) | SEN (%) | SPE (%) | GDR (%) | FDH (h−1) | FDR (%) | F1 (%) | Time Delay (s) |
|---|---|---|---|---|---|---|---|---|---|---|
| (Mean ± Standard Error) | ||||||||||
| Linear SVM | Full feature set (20) | λ = 10−5 Solver: dual C1 = 1; C2 = 2 | 52 ± 4 | 24 ± 7 | 89 ± 3 | 27 ± 8 | 2 ±1 | 4 ± 1 | 12 ± 4 | 56 ± 3.5 |
| Features selected through mRMR (20) | λ = 10−8 Solver: dual C1 = 1; C2 = 7 | 54 ± 3 | 26 ± 8 | 87 ± 3 | 36 ± 8 | 3 ± 0.4 | 5 ± 1 | 15 ± 4 | 116 ± 10 | |
| Gaussian SVM | Full feature set (20) | Box Constraint: 1 Kernel Scale: 5 C1 = 1; C2 = 7 | 52 ± 3 | 29 ± 8 | 84 ± 4 | 34 ± 9 | 4 ± 1 | 6 ± 1 | 16 ± 5 | 42 ± 0.6 |
| Features selected with mRMR (5) | Box Constraint: 0.5 Kernel Scale: 1 C1 = 1; C2 = 7 | 54 ± 3 | 24 ± 8 | 85 ± 2 | 27 ± 9 | 3 ± 1 | 6 ± 1 | 16 ± 5 | 55 ± 3 | |
| Model | N° Features | Hyperparameters | AUC (%) | SEN (%) | SPE (%) | GDR (%) | FDH (h−1) | FDR (%) | F1 (%) | Time Delay (s) |
|---|---|---|---|---|---|---|---|---|---|---|
| (Mean ± Standard Error) | ||||||||||
| Linear SVM | Full feature set (26) | λ = 10−7 Solver: dual C1 = 3; C2 = 1 | 56 ± 5 | 22 ± 7 | 87 ± 3 | 31 ± 8 | 1 ± 0.2 | 6 ± 1 | 20 ± 6 | 141 ± 4 |
| Features selected with mRMR (2) | λ = 10−7 Solver: dual C1 = 1; C2 = 40 | 58 ± 5 | 22 ± 9 | 77 ± 5 | 25 ± 9 | 1 ± 0.2 | 4 ± 1 | 13 ± 1 | 138 ± 15 | |
| Gaussian SVM | Full feature set (26) | Box Constraint: 0.5 Kernel Scale: 25 C1 = 1; C2 = 5 | 50 ± 4 | 51 ± 1 | 61 ± 5 | 58 ± 10 | 2 ± 0.3 | 10 ± 1 | 27 ± 6 | 117 ± 13 |
| Features selected through mRMR (2) | Box Constraint: 5 Kernel Scale: 0.1 C1 = 1; C2 = 200 | 62 ± 5 | 47 ± 8 | 67 ± 3 | 62 ± 9 | 3 ± 0.3 | 16 ± 1 | 29 ± 5 | 123 ± 3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olmi, B.; Manfredi, C.; Frassineti, L.; Dani, C.; Lori, S.; Bertini, G.; Cossu, C.; Bastianelli, M.; Gabbanini, S.; Lanatà, A. Heart Rate Variability Analysis for Seizure Detection in Neonatal Intensive Care Units. Bioengineering 2022, 9, 165. https://doi.org/10.3390/bioengineering9040165
Olmi B, Manfredi C, Frassineti L, Dani C, Lori S, Bertini G, Cossu C, Bastianelli M, Gabbanini S, Lanatà A. Heart Rate Variability Analysis for Seizure Detection in Neonatal Intensive Care Units. Bioengineering. 2022; 9(4):165. https://doi.org/10.3390/bioengineering9040165
Chicago/Turabian StyleOlmi, Benedetta, Claudia Manfredi, Lorenzo Frassineti, Carlo Dani, Silvia Lori, Giovanna Bertini, Cesarina Cossu, Maria Bastianelli, Simonetta Gabbanini, and Antonio Lanatà. 2022. "Heart Rate Variability Analysis for Seizure Detection in Neonatal Intensive Care Units" Bioengineering 9, no. 4: 165. https://doi.org/10.3390/bioengineering9040165