1. Introduction
There are many factors that have repercussions on ageing. During life, social and physical environment, as well as behavioural attitudes have a major impact on human ageing process. Nowadays, as a result of medical improvements, people are living longer—both an increase in the average life expectancy and a drop in the fertility rate has been observed. The World Health Organization (WHO) states that there are 125 million of people 80 years old or more, which is expected to increase to 434 million by 2050 [
1].
Over the years, it is predictable that more ageing health problems will arise. Thus, it is crucial to consider not only the physical deterioration (the visible one), but also the nervous system deterioration. Concerning elderly people, it is proved that they have a greater propensity to develop neurodegenerative diseases such as dementia. Neurodegenerative disease is a serious clinical condition since it truly affects the nervous system functioning and progresses irreversibly. Epidemiological data state that 1 in 3 seniors dies with dementia [
2,
3].
Every 3 seconds, a new case of dementia is diagnosed. The WHO estimates that there are around 50 million people suffering from dementia worldwide. It is estimated that this value may reach about 82 million and 152 million in 2030 and 2050, respectively. In terms of geographic distribution, there is an expected higher rate of incidence in low- and middle-income countries compared with high-income countries [
4].
Alzheimer Disease is known as the most common form of dementia, representing 65% of all dementia cases. It is characterised by the deterioration of human cognitive functions, affecting behaviour, language, memory and reasoning, among others. Alzheimer is a neurodegenerative disease in which the accumulation of certain toxic substances in the brain leads to the progressive death of neuronal cells. The major brain changes that AD causes are the accumulation of an atypical form of the tau protein within neurons, as well as the accumulation of the
-amyloid fragments outside neurons [
5,
6].
The AD progress can be described over four development stages: Pre-clinical, Mild Cognitive Impairment (MCI), Moderate AD and Severe AD. In the first stage, there are no associated symptoms (asymptomatic period). It is believed that AD arises at least 20 years before symptoms appear, hence the patient could stay in this initial phase for a long period of time. During the second phase, MCI, symptoms like memory lapses begins. The concept of MCI was created with the aim of including individuals with mild symptoms who might eventually progress to AD. It is stated that 6% to 25% of MCI patients later develop AD. The moderate stage is typically the longest one—frequent memory lapses and difficulty in performing daily routine tasks are faced, as well as other psychological symptoms. Lastly, the severe stage is the moment that patient loses the ability to interact with those who are around, having cognitive and motor functions extremely altered [
5,
7,
8].
There are several factors that increase the risk of developing AD. Genetics, age, sex, lifestyle and other diseases are considered the main ones. Concerning family history, having one and two first-degree relatives with AD increases the risk of developing the disease by four and eight times, respectively. As it can be expected, dementia is scarce before the age of 65. Concerning sex, statistical data shows that AD is more common in women. As far as lifestyle habits are concerned, smokers and inactive people develop a propensity for this disease. The level of education also has impact since more years of education means a constant brain stimulation. There is also a strong evidence that having a healthy diet may reduce the probability of developing dementia. People diagnosed with depression and cardiovascular diseases are considered equally susceptible [
5,
9,
10,
11,
12].
To date, there is no cure for this disease. However, there are several medical exams that support the diagnostic when someone reveals signs of dementia during life—Magnetic Resonance Imaging (MRI), Positron Emission Tomography (PET), Cerebrospinal Fluid (CFS) Analysis and Electroencephalogram (EEG). Besides that, Neurologists consider the medical history and perform several neurological and cognitive tests. It is important to note the true diagnosis of Alzheimer is only achieved with autopsy exam, after patient’s death [
13].
EEG is a non-invasive and painless medical exam that aims to record and evaluate brain electrical activity. EEG signal is acquired by placing electrodes on the scalp and its frequency and amplitude values are contained in the range of 1 to 100 Hz and 10 to 100 µV, respectively. EEG enables to identify potential abnormalities in brain wave patterns [
14]. Those abnormalities may be linked with brain illnesses such as dementia [
15].
In the clinical branch, it is possible to evaluate brain abnormalities in a patient’s brain activity by analysing the EEG signal frequency. In this way, it is considered five conventional frequency bands—delta, theta, alpha, beta and gamma. Delta waves (
) are the slowest and highest amplitude waves, belonging to the frequency range of 0.5 to 4 Hz. These waves are related to events such as deep sleep and wakefulness. Theta waves (
) have an amplitude greater than 20 µV and are contained within the frequency range of 4 to 8 Hz. The presence of these waves is associated with moments of emotional stress, deep meditation and creative inspiration. Alpha waves (
) belong to the frequency and amplitude range of 8 to 13 Hz and 30 to 50 µV, respectively. When a person is with the eyes closed or in a relaxed state, these waves appear mostly in the occipital lobe. Beta waves (
) refer to rhythms in the frequency range of 13 to 30 Hz, having amplitude values less than 30 µV. This wave type is commonly observed in the brain of a healthy adult and it is associated with active brain activity, active thinking and problem solving. Finally, gamma waves (
) are the fastest and lowest amplitude waves, lying above the frequency of 30 Hz (normally the upper limit is 100 Hz). The activity of these waves are of rare occurrence—a brain disease can be confirmed by an abnormal presence of this rhythm [
16,
17].
An AD patient reveals changes in the EEG signal compared to the normal patterns observed in a healthy individual. The main phenomenon is named slowing effect. As the disease progresses, there is an increase in power in the lower frequency bands (
and
), as well as a decrease in power in the higher frequency bands (
,
and
). Additionally, shift-to-the-left phenomenon is also observed. A shift of the power spectrum peak at the alpha band to the lower frequency bands occurs. The surface distribution of these rhythms becomes emphatic in anterior regions, instead of in the occipital region (healthy subject). Briefly, these signal power modifications are essentially due to the lack of acetylcholine in the AD brain. Insufficient amounts of acetylcholine result in failures in the synchronisation of synaptic potentials [
8,
18,
19].
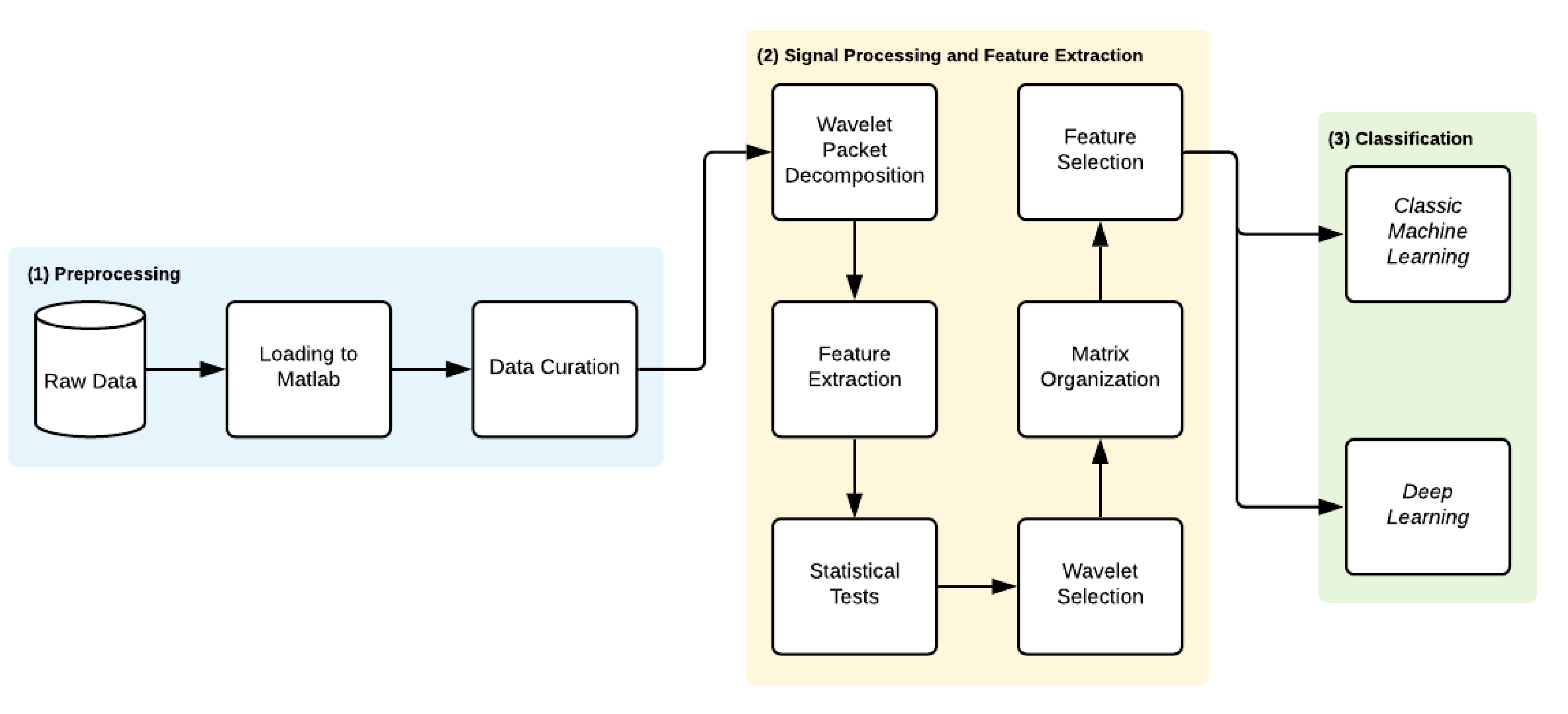
Given the large number of people affected and the inherent severity, it is urgent to find a method capable of assisting in the AD early stages diagnosis. For this reason, the main goal of the present work is to create an intelligent system that can be useful for that purpose—a tool that could detect anomalies in the EEG signal of an Alzheimer carrier during the asymptomatic period so that the disease evolution can be delayed. This paper proposes a new method based on a nonlinear multiband analysis of the EEG signals. By the extraction of relevant features, it was feasible to perform the data classification per electrode by means of Classic ML and DL.
In terms of structure, this paper is organized in five main sections: In
Section 2, the EEG database is described. Thereafter, the methodology concerning the signal processing and the classification procedure is explained in
Section 3. The obtained results and the inherent discussion were covered in
Section 4. Lastly,
Section 5 makes remarks about conclusions.
2. Materials
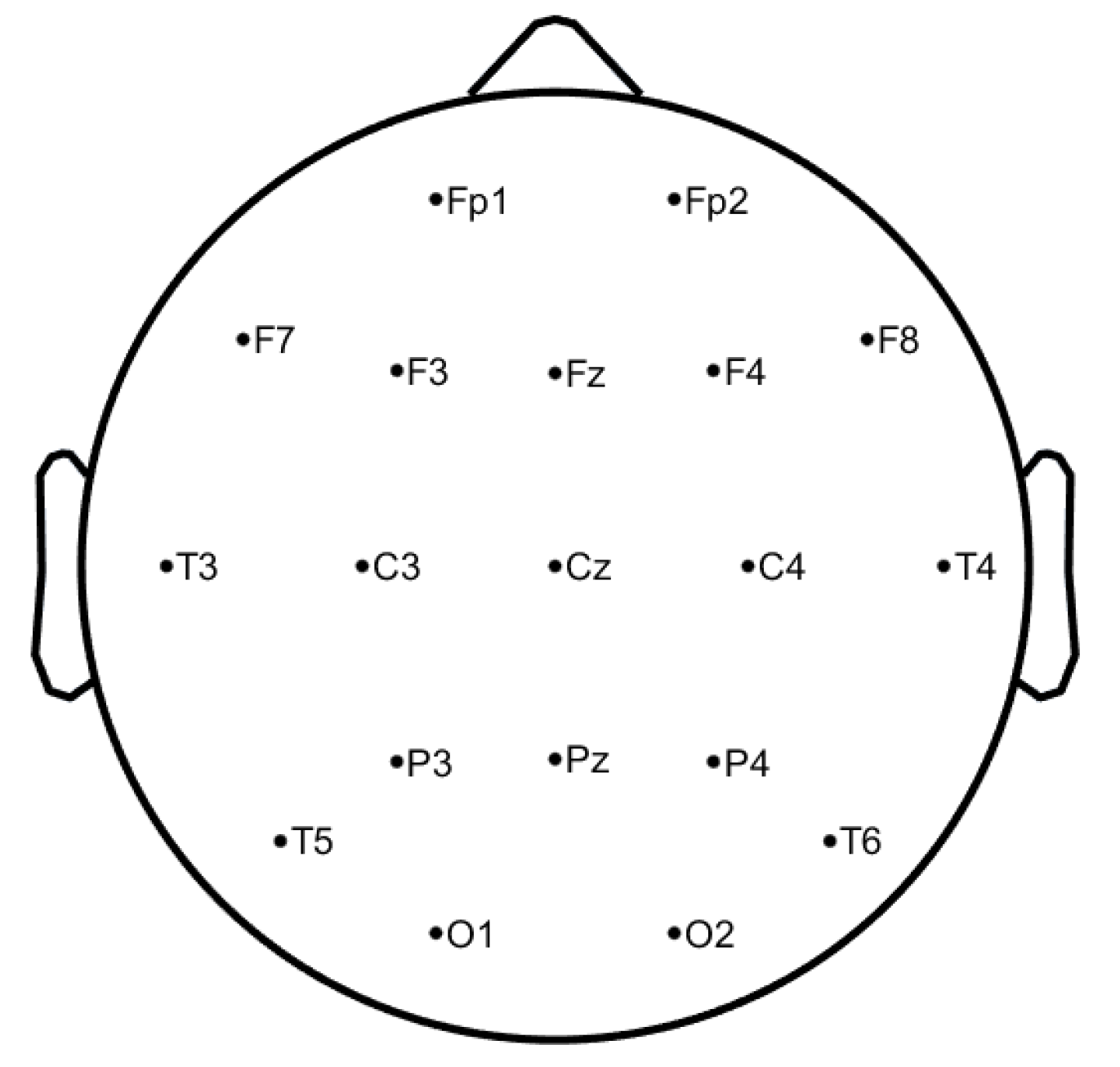
The EEG signals have been collected at Hospital de São João in Porto, Portugal, with the approval of the local ethics committee and the hospital’s administration board within the project CES198-14. The data were acquired at a sampling rate of 256 Hz through 19 electrodes placed on the scalp, using the common reference electrode at CPz, according to the 10–20 system (see
Figure 1, image generated by authors in Matlab using EEGLab [
20]), covering the frontal (Fz, FP1, FP2, F3, F7), temporal (T7, T8), parietal (Pz, P3, P4, P7, P8, PO7, PO8), occipital (O1, O2), and central (Cz, C3, C4) regions, resulting in 19 waveforms per exam. During the acquisition, it was ensured that all the study subjects were relaxed and with the eyes closed. The DC component was removed. It is important to note that only signals without any kind of artefacts are selected.
This database includes 38 subjects split into 4 distinct groups—11 healthy subjects called healthy controls (C), 8 MCI, 11 AD mild and moderate (ADM) patients and 8 AD advanced (ADA) patients. The average Mini Mental State Examination (MMSE) and age average of each group are presented in
Table 1. MMSE is the most common exam used in clinics and hospitals to assess patients’ major cognitive domains, such as visuospatial abilities, attention, memory and language. Its scores range from 0 to 30. Scores on the higher end indicate a higher cognitive function, while lower scores mean more severe cases of dementia [
21].
4. Results and Discussion
The final results of the classification for each comparison case are shown in
Table 4, where the best classifier, the maximum accuracy and the electrode scalp position are indicated per classifier modality (Classic ML and Deep Learning).
Analysing the results presented
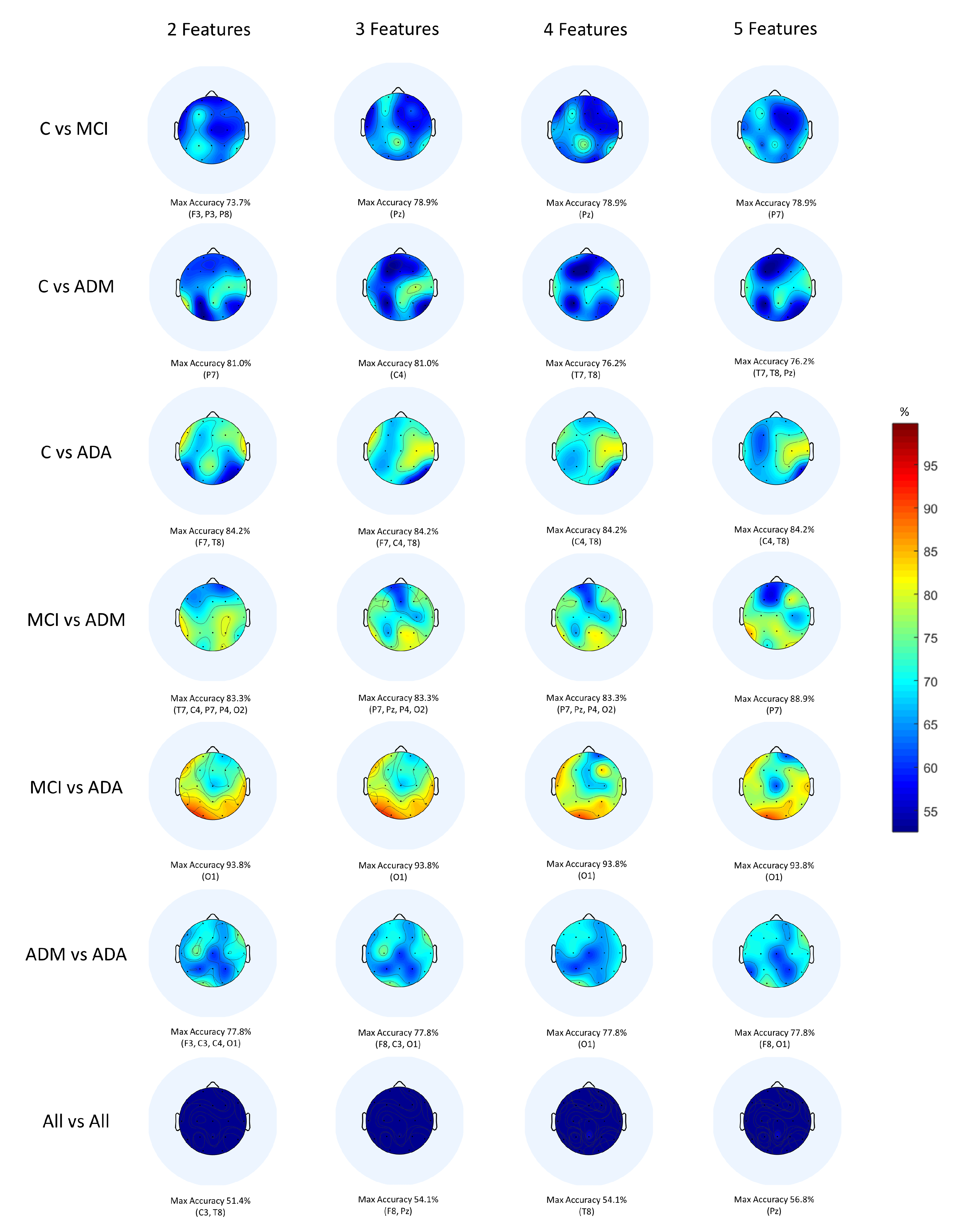
Table 4, the binary classification of C vs. MCI exhibits a maximum accuracy of 78.9% on P7 and Pz electrodes, being noticeable that those are the ones with the greatest discriminate power. Regarding this comparison, the classifier which presented this best performance was Decision Tree (Fine, Medium and Coarse Tree). In turn, DL selected the P8 electrode as the one which present more significant differences between groups, reaching 78.9% as maximum accuracy.
Regarding Classic ML, and when comparing C vs. ADM, it is observed that the C4 and P7 electrodes present a maximum accuracy of 81.0%, being the ones that reveal more significant differences. The classifiers Cubic SVM and Fine Gaussian SVM were the ones who correspond to the highest accuracy result. In contrast, through DL, a maximum accuracy of 76.2% was achieved in the Pz electrode, this being the one that corresponds to the scalp region with the highest discriminative power between subjects.
Concerning Classic ML, the binary classification of C vs. ADA exhibits a maximum accuracy of 84.2% visible in the F7, C4 and T8 electrodes, being noticeable that those are the ones with the greatest discriminative power. Regarding this comparison, the classifiers which presented this best performance were Linear SVM and Gaussian Naive Bayes. In turn, DL selected the F7 and F8 electrodes as the scalp regions which present more significant differences between groups, reaching 78.9% as maximum accuracy.
Regarding Classic ML, and when comparing MCI vs. ADM, it is observed that the P7 electrode present a maximum accuracy of 88.9%, being the one that reveals more significant differences. The classifier Cosine KNN was the one who correspond to the highest accuracy result. In contrast, through DL, a maximum accuracy of 83.3% was achieved in the Pz electrode, this being the one that corresponds to the scalp region with the highest discriminative power between subjects.
Concerning Classic ML, the binary classification of MCI vs. ADA exhibits a maximum accuracy of 93.8% visible in the O1 electrode; it is noticeable that this is the one with the greatest discriminative power. Regarding this comparison, the classifier which presented this best performance was Decision Tree (Fine, Medium and Coarse Tree). In turn, DL selected the P4 electrode as the scalp region which present more significant differences between groups, reaching 93.8% as maximum accuracy.
Regarding Classic ML, and when comparing ADM vs. ADA, it is observed that the F3, F8, C3, C4, O1 electrodes present a maximum accuracy of 77.8%, being the ones that reveal more significant differences. The classifiers Ensemble Subspace Discriminant and Fine KNN were the ones who correspond to the highest accuracy result. In contrast, through DL, a maximum accuracy of 72.2% was achieved in the Fz, F4 and C4 electrodes, these being the ones that correspond to the scalp regions with the highest discriminative power between subjects.
Concerning Classic ML, the multiclass classification of All vs. All exhibits a maximum accuracy of 56.8% visible in the Pz electrode, being noticeable that this is the one with the greatest discriminative power. Regarding this comparison, the classifier which presented this best performance was Medium Gaussian SVM. In turn, DL selected the Pz electrode as the scalp region which present more significant differences between groups, reaching 51.4% as the maximum accuracy.
In fact, Classic ML shows better results than DL with the exception of 2 out of 7 comparisons. This being the best technique, it is relevant to deepen the results obtained. To this end, the topographic maps were elaborated (
Figure 5) with the Classic ML results in order to visualise the scalp regions that present the best values of accuracy.
When observing the topographic maps, it is possible to conclude that C4 and P7 are the electrodes which best distinguish the differences between subjects. Those electrodes correspond to the brain central region and to the parietal lobe, respectively. Depending on the disease stage and which stages are being compared, the area which is considered to be the most affected may vary. Although the temporal lobe is typically responsible for memory functions, it does not mean that the other scalp regions are not equally affected by the disease. According to Siuly and Zhang [
16], the parietal area is very important in recognition and orientation. Actually, AD patients tend to lose these abilities, for example, at the moments when they do not recognise their family or when they feel lost in a physical space they previously knew. This conclusion sustains the results obtained.
Additionally, it is crucial to reflect on the work considered closest to this one in order to draw some further conclusions. To this end,
Table 5 and
Table 6 present a direct comparison between the developed work and others—same EEG database and different EEG database:
- 1
Compared to other methods of diagnosing AD through EEG signals from the same database (
Table 5), the proposed method outperformed the study developed by Rodrigues et al. [
19] by 2% in the binary comparison MCI vs. ADM. It can be seen that CNNs have never been applied to this dataset, so this work is the first and the only one that follows this approach. Indeed, this works presents added value to the scientific community, as it has the potential to be improved and become a powerful tool for AD diagnosis in all its stages.
- 2
Compared to other techniques of diagnosing AD through EEG signals from different databases (
Table 6), it is observed that the present study outperformed the work carried out by Fiscon et al. [
36] by 13% in the pair MCI vs. AD. It is noteworthy that the present study has the peculiarity of being the only one that applied the F-score technique, so it may have highly contributed to the good classification results.
In general, Classic ML proved to have more capacity to identify AD activity along its progression than DL. One of the reasons for this happening is that DL is commonly used for analysing large amounts of data. According to Esteva et al. [
38], and particularly regarding the medical field, DL methods are benefic because of the capacity to generate sheer volume of data. In fact, this database only contains 38 participants, so the simpler methods (such as Classic ML) were sufficient to get better results than CNN.
5. Conclusions
AD is a neurodegenerative disease marked by a rapid progression, leading to total loss of cognitive functions. As with other types of dementia, the prevalence is increasing and forecasts show no improvements. During the early stages, patients do not have symptoms—the disease is silent. As soon as the symptomatic phase begins, there is a worsening of the clinical condition. Since AD is considered one of the most severe diseases and there is still no cure, the main goal of this work was to develop a strong system proficient of assisting in the AD diagnosis.
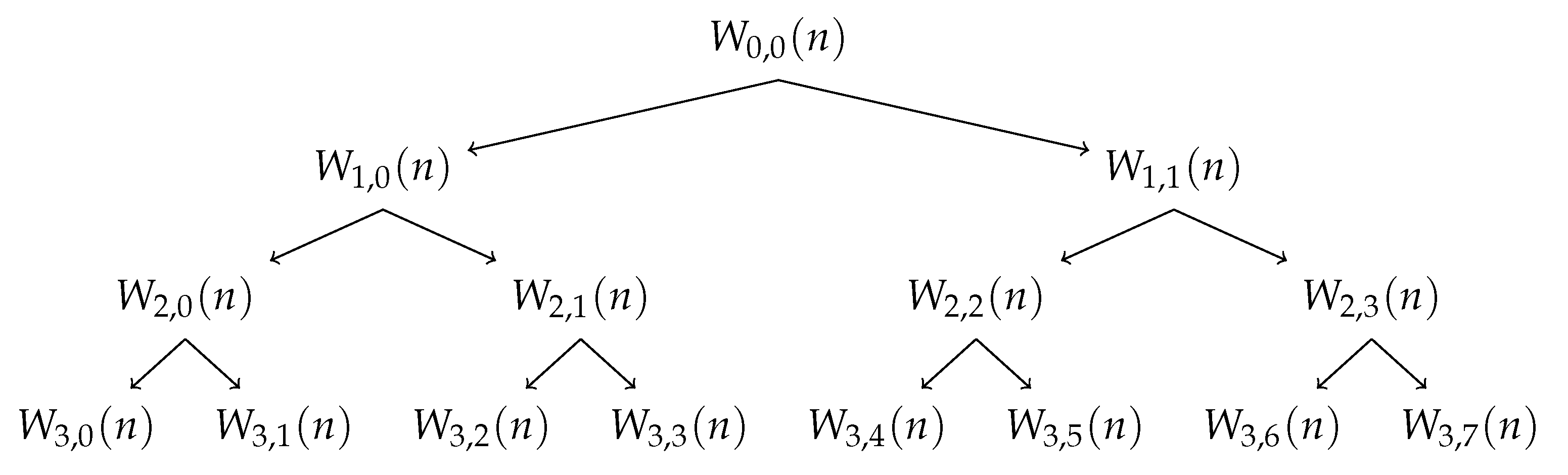
Hence, and taking benefit from Wavelet Packet Transform for multi-band analysis, several statistics and nonlinear features were extracted from EEG signals. The most interesting features were used to evaluate the significant differences between the study groups through Classic ML and DL classification methods. The main results indicate that Classic ML algorithms showed a higher discriminant power to emphasize AD activity than DL, except in the binary comparisons C vs. MCI and MCI vs. ADA where they achieved exactly the same accuracy.
In conclusion, the aim of this work was accomplished according to what was expected, since it corroborated the state of the art, having exceeded some discriminant accuracies comparing to others studies. Regarding the state of the art with the same EEG database, the proposed method outperforms previous works by 2%, in the binary comparison MCI vs. ADM. It is relevant to highlight that the remaining comparisons performed (C vs. MCI, C vs. ADM, C vs. ADA, MCI vs. ADA, ADM vs. ADA and All vs. All) did not show better results. Indeed, this improvement reflects the impact that this tool can have, particularly in distinguishing these two consecutive stages of AD.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}