
In-House, Fast FDM Prototyping of a Custom Cutting Guide for a Lower-Risk Pediatric Femoral Osteotomy

 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
1.1. Custom Cutting Guide (CCG)
1.2. CCGs in Maxillofacial Surgery (MFS)
1.3. CCGs in Total Knee Arthroplasty (TKA)
1.4. CCGs in Long Bones and Pediatric Surgery
2. Materials and Methods
2.1. Case Study
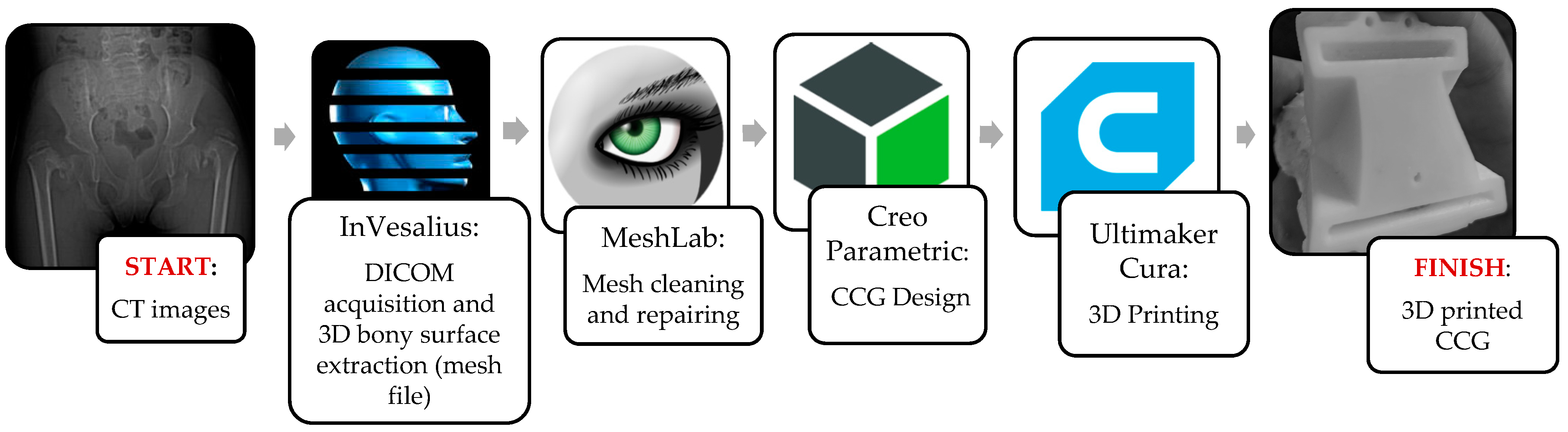
2.2. CAM and CAD-CAT
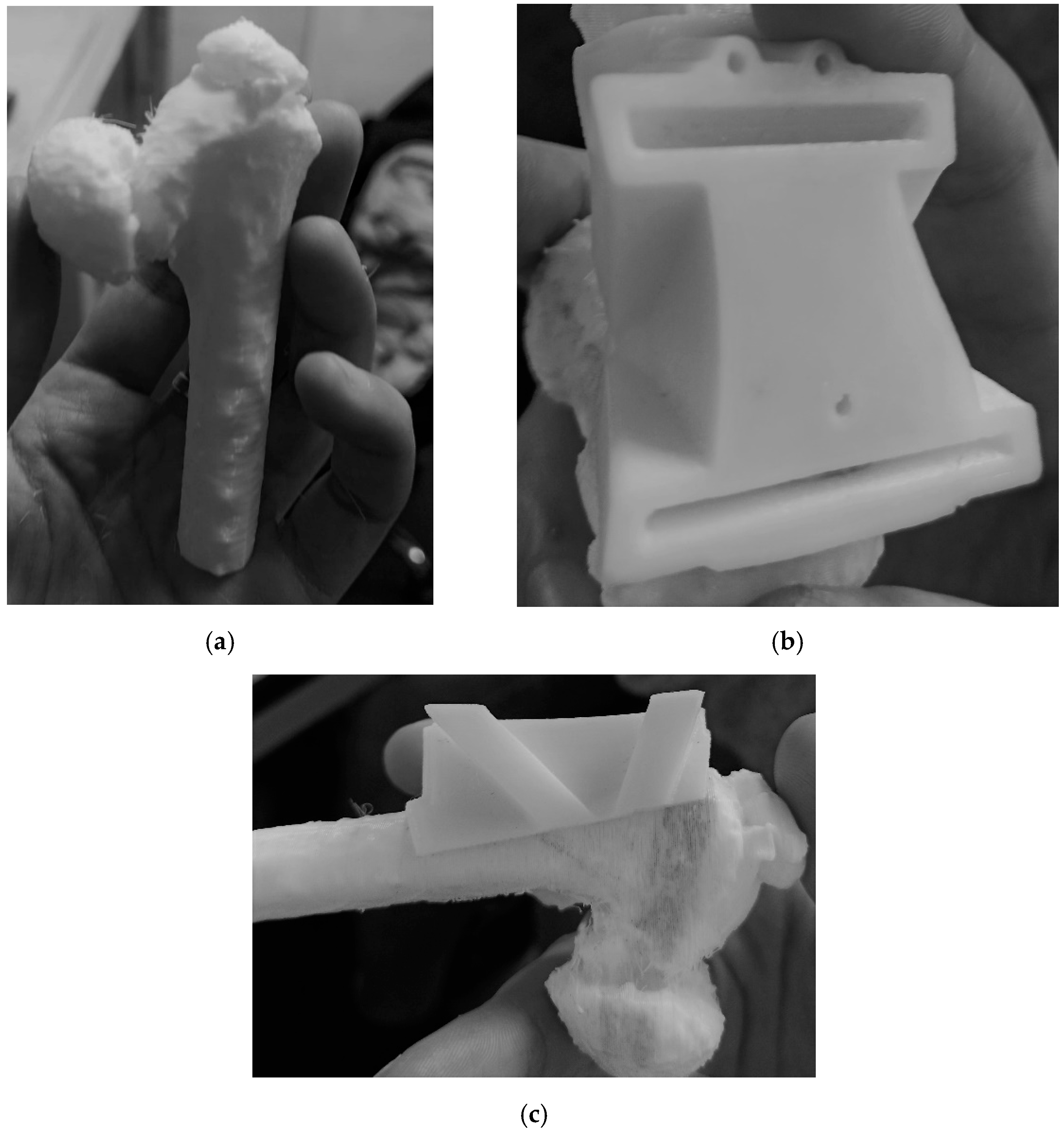
2.3. CASS and CCG Design
2.4. Sterilization of the Polymer-Based Medical Elements
2.5. Main Features of Low-End and High-End FDM 3D Printers
- −
- An hotend, which heats the filament and extrudes it outside the nozzle;
- −
- The printing bed, which can be static or mobile, heated or non-heated;
- −
- A cooling fan;
- −
- The frame, which has to absorb vibrations and guarantee stability during the process;
- −
- The material supply system, which is linked to the hotend through a polytetrafluoroethylene (PFTE) tube, giving the filament a precise path to follow (Bowden), or simply fixed directly on the x-axis (direct drive);
- −
- Rails and engines: rails are found in different constructive solutions. Low-end 3D printers usually use linear bar rails with vertical bearings, which is the most economical but inaccurate configuration because of the friction between the linear rail and the bearing. Another possible constructive solution is through a rubberized wheel on the extruded aluminum rail, which has silent disposition and has a good ratio between cost and efficiency. High-end FDM printers are equipped with linear rails, which represent the most expensive but most accurate solution.
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malik, H.H.; Darwood, A.R.J.; Shaunak, S.; Kulatilake, P.; El-Hilly, A.A.; Mulki, O.; Baskaradas, A. Three-dimensional printing in surgery: A review of current surgical applications. J. Surg. Res. 2015, 199, 512–522. [Google Scholar] [CrossRef]
- Napolitano, F.; Frizziero, L.; Santi, G.M.; Donnici, G.; Liverani, A.; Papaleo, P.; Giuseppetti, V. Description of the cad-am process for 3d bone printing: The case study of a flat foot. In Proceedings of the 5th NA International Conference on Industrial Engineering and Operations Management, Detroit, MI, USA, 10–14 August 2020. [Google Scholar]
- Bockhorn, L.; Gardner, S.S.; Dong, D.; Karmonik, C.; Elias, S.; Gwathmey, F.W.; Harris, J.D. Application of three-dimensional printing for pre-operative planning in hip preservation surgery. J. Hip Preserv. Surg. 2019, 6, 164–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frizziero, L.; Santi, G.M.; Liverani, A.; Napolitano, F.; Papaleo, P.; Maredi, E.; Di Gennaro, G.L.; Zarantonello, P.; Stallone, S.; Stilli, S.; et al. Computer-aided surgical simulation for correcting complex limb deformities in children. Appl. Sci. 2020, 10, 5181. [Google Scholar] [CrossRef]
- Frizziero, L.; Liverani, A.; Donnici, G.; Osti, F.; Neri, M.; Maredi, E.; Trisolino, G.; Stilli, S. New methodology for diagnosis of orthopedic diseases through additive manufacturing models. Symmetry 2019, 11, 542. [Google Scholar] [CrossRef] [Green Version]
- Osti, F.; Santi, G.M.; Neri, M.; Liverani, A.; Frizziero, L.; Stilli, S.; Maredi, E.; Zarantonello, P.; Gallone, G.; Stallone, S.; et al. CT conversion workflow for intraoperative usage of bony models: From DICOM data to 3D printed models. Appl. Sci. 2019, 9, 708. [Google Scholar] [CrossRef] [Green Version]
- Caligiana, P.; Liverani, A.; Ceruti, A.; Santi, G.M.; Donnici, G.; Osti, F. An Interactive Real-Time Cutting Technique for 3D Models in Mixed Reality. Technologies 2020, 8, 23. [Google Scholar] [CrossRef]
- Miyake, J.; Murase, T.; Oka, K.; Moritomo, H.; Sugamoto, K.; Yoshikawa, H. Computer-assisted corrective osteotomy for malunited diaphyseal forearm fractures. JBJS 2012, 94, e150. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.; Xing, W.; Wu, Z.; Huang, H.; Huang, W. A combination of three-dimensional printing and computer-assisted virtual surgical procedure for preoperative planning of acetabular fracture reduction. Injury 2016, 47, 2223–2227. [Google Scholar] [CrossRef]
- Shen, S.; Wang, P.Z.; Li, X.Y.; Han, X.; Tan, H.L. Pre-operative simulation using a three-dimensional printing model for surgical treatment of old and complex tibial plateau fractures. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Frizziero, L.; Santi, G.M.; Liverani, A.; Giuseppetti, V.; Trisolino, G.; Maredi, E.; Stilli, S. Paediatric orthopaedic surgery with 3D printing: Improvements and cost reduction. Symmetry 2019, 11, 1317. [Google Scholar] [CrossRef] [Green Version]
- Michalski, A.; Stopa, M.; Miśkowiak, B. Use of multimedia technology in the doctor- patient relationship for obtaining patient informed consent. Med. Sci. Monit. 2016, 22, 3994–3999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, D.S. Simulation in pediatric orthopaedic surgery. J. Pediatr. Orthop. 2015, 35, S26–S29. [Google Scholar] [CrossRef]
- Perica, E.; Sun, Z. Patient-specific three-dimensional printing for pre-surgical planning in hepatocellular carcinoma treatment. Quant. Imaging Med. Surg. 2017, 7, 668–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khandekar, S.; Tolessa, E.; Jones, S. Displaced distal end radius fractures in children treated with Kirschner wires—A systematic review. Acta Orthop. Belg. 2016, 82, 681–689. [Google Scholar] [PubMed]
- Nysjö, F.; Olsson, P.; Malmberg, F.; Carlbom, I.B.; Nyström, I. Using anti-aliased signed distance fields for generating surgical guides and plates from CT images. J. WSCG 2017, 25, 11–20. [Google Scholar]
- Hou, H.Y.; Li, C.H.; Chen, M.C.; Lin, P.Y.; Liu, W.C.; Cathy Tsai, Y.W.; Huang, R.Y. A novel 3D-printed computer-assisted piezocision guide for surgically facilitated orthodontics. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 584–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzoni, S.; Bianchi, A.; Schiariti, G.; Badiali, G.; Marchetti, C. Computer-aided design and computer-aided manufacturing cutting guides and customized titanium plates are useful in upper maxilla waferless repositioning. J. Oral Maxillofac. Surg. 2015, 73, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Louvrier, A.; Marty, P.; Barrabé, A.; Euvrard, E.; Chatelain, B.; Weber, E.; Meyer, C. How useful is 3D printing in maxillofacial surgery? J. Stomatol. Oral Maxillofac. Surg. 2017, 118, 206–212. [Google Scholar] [CrossRef]
- Haas Junior, O.L.; Fariña, R.; Hernández-Alfaro, F.; de Oliveira, R.B. Minimally invasive intraoral proportional condylectomy with a three-dimensionally printed cutting guide. Int. J. Oral Maxillofac. Surg. 2020, 49, 1435–1438. [Google Scholar] [CrossRef]
- Scolozzi, P. Computer-aided design and computer-aided modeling (CAD/CAM) generated surgical splints, cutting guides and custom-made implants: Which indications in orthognathic surgery? Rev. Stomatol. Chir. Maxillofac. Chir. Orale 2015, 116, 343–349. [Google Scholar] [CrossRef]
- Gateno, J.; Xia, J.J.; Teichgraeber, J.F.; Christensen, A.M.; Lemoine, J.J.; Liebschner, M.A.K.; Gliddon, M.J.; Briggs, M.E. Clinical Feasibility of Computer-Aided Surgical Simulation (CASS) in the Treatment of Complex Cranio-Maxillofacial Deformities. J. Oral Maxillofac. Surg. 2007, 65, 728–734. [Google Scholar] [CrossRef]
- Nam, D.; Williams, B.; Hirsh, J.; Johnson, S.R.; Nunley, R.M.; Barrack, R.L. Planned bone resections using an MRI-based custom cutting guide system versus 3-dimensional, weight-bearing images in total knee arthroplasty. J. Arthroplast. 2015, 30, 567–572. [Google Scholar] [CrossRef]
- Jacquet, C.; Sharma, A.; Fabre, M.; Ehlinger, M.; Argenson, J.N.; Parratte, S.; Ollivier, M. Patient-specific high-tibial osteotomy’s ‘cutting-guides’ decrease operating time and the number of fluoroscopic images taken after a Brief Learning Curve. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 2854–2862. [Google Scholar] [CrossRef] [PubMed]
- Pornrattanamaneewong, C.; Chareancholvanich, K.; Narkbunnam, R. A prospective randomised controlled study of patient-specific cutting guides compared with conventional instrumentation in total knee replacement. Bone Jonit J. 2013, 95, 354–359. [Google Scholar]
- Pérez-Mañanes, R.; Burró, J.A.; Manaute, J.R.; Rodriguez, F.C.; Martín, J.V. 3D Surgical Printing Cutting Guides for Open-Wedge High Tibial Osteotomy: Do It Yourself. J. Knee Surg. 2016, 29, 690–695. [Google Scholar] [CrossRef]
- Waters, P.M.; Bae, D.S. Pediatric Hand and Upper Limb Surgery: A Practical Guide; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; ISBN 1451178514. [Google Scholar]
- Maredi, E. IOR-IRCCS Direzione Generale IOR-IRCCS; IOR: Bologna, Italy, 2018; pp. 4–10. [Google Scholar]
- Louahem M’sabah, D.; Assi, C.; Cottalorda, J. Proximal femoral osteotomies in children. Orthop. Traumatol. Surg. Res. 2013, 99, S171–S186. [Google Scholar] [CrossRef] [PubMed]
- Rogers, W.J. Steam and dry heat sterilization of biomaterials and medical devices. In Sterilisation of Biomaterials and Medical Devices; Elsevier: Amsterdam, The Netherlands, 2012; pp. 20–55. [Google Scholar]
- Ferràs-Tarragó, J.; Sabalza-Baztán, O.; Sahuquillo-Arce, J.M.; Angulo-Sánchez, M.Á.; Amaya-Valero, J.; De-La-Calva Ceinos, C.; Baixauli-García, F. Security of 3D-printed polylactide acid piece sterilization in the operating room: A sterility test. Eur. J. Trauma Emerg. Surg. 2021, 1–6. [Google Scholar] [CrossRef]
- Arnal-Burró, J.; Pérez-Mañanes, R.; Gallo-del-Valle, E.; Igualada-Blazquez, C.; Cuervas-Mons, M.; Vaquero-Martín, J. Three dimensional-printed patient-specific cutting guides for femoral varization osteotomy: Do it yourself. Knee 2017, 24, 1359–1368. [Google Scholar] [CrossRef]
- Shi, J.H.; Lv, W.; Wang, Y.; Ma, B.; Cui, W.; Liu, Z.Z.; Han, K.C. Three dimensional patient-specific printed cutting guides for closing-wedge distal femoral osteotomy. Int. Orthop. 2019, 43, 619–624. [Google Scholar] [CrossRef]
- Nizam, I.; Batra, A.V. Accuracy of bone resection in total knee arthroplasty using CT assisted-3D printed patient specific cutting guides. Sicot-J. 2018, 4, 29. [Google Scholar] [CrossRef] [Green Version]
- Azimi, P.; Zhao, D.; Pouzet, C.; Crain, N.E.; Stephens, B. Emissions of Ultrafine Particles and Volatile Organic Compounds from Commercially Available Desktop Three-Dimensional Printers with Multiple Filaments. Environ. Sci. Technol. 2016, 50, 1260–1268. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Palomo, J.M.; Meschian-Coretti, S.; Esteban-Castillo, J.L.; García-Vera, J.J.; Montañez-Heredia, E. Double Level Osteotomy Assisted by 3D Printing Technology in a Patient with Blount Disease: A Case Report. JBJS Case Connect. 2020, 10, e0477. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhao, K.; Li, Y.; Chen, F. Mechanical characterization of biocompatible PEEK by FDM. J. Manuf. Process. 2020, 56, 28–42. [Google Scholar] [CrossRef]
- Cone, J.A.; Martin, T.M.; Marcellin-Little, D.J.; Harrysson, O.L.A.; Griffith, E.H. Accuracy and repeatability of long-bone replicas of small animals fabricated by use of low-end and high-end commercial three-dimensional printers. Am. J. Vet. Res. 2017, 78, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.V.; Dang, A.B.C.; Dang, A. Comparing cost and print time estimates for six commercially-available 3D printers obtained through slicing software for clinically relevant anatomical models. 3D Print. Med. 2021, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.V.; Tanaka, K.S.; Dang, A.B.C.; Dang, A. Identifying a commercially-available 3D printing process that minimizes model distortion after annealing and autoclaving and the effect of steam sterilization on mechanical strength. 3D Print. Med. 2020, 6, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Software | Availability |
|---|---|
| InVesalius | Open-source |
| MeshLab | Open-source |
| Creo Parametric | Student license// 30-day free trial |
| Ultimaker Cura | Open-source |
| Material | Autoclavability | 3D Printing Capability | Cost (EUR/kg) |
|---|---|---|---|
| HTPLA (ProtoPasta) | Yes | Low-end | 68 |
| Medical ABS (FiloAlfa) | No | Heated bed Closed chamber Gas emissions | 56 |
| Antibacterial PLA (FiberForce) | No | Low-end | 73 |
| nGen Flex (ColorFabb) | No | Heated bed Post-processing (cooling phase) | 62 |
| PLA Bioflex® (FiloAlfa) | No | Low-end | 60 |
| PEEK | Yes | Heated bed Post-processing (mechanical resistance enhancement) | 400 |
| Parameters | Values |
|---|---|
| Nozzle temperature (°C) | 210 |
| Printing speed (mm/s) | 25–45 |
| Nozzle diameter (mm) | 0.4 |
| Ref. | Production | Informatic Procedure | Material | Sterilization Method | 3D Printing Technology |
|---|---|---|---|---|---|
| This procedure | In-house | Invesalius + MeshLab (Meshmixer) + PTC Creo | HTPLA | Steam-heat | FDM |
| [29] | In-house | Orthoview + OsiriX + Meshmixer | ABS | Ethylene oxide | FDM |
| [32] | In-house | Orthoview + Meshmixer | Acrylate resin | * | FDM |
| [33] | In-house | Mimics | Nylon | Ethylene oxide | SLS |
| [34] | PROPHECY | * | Nylon | Steam heat | SLS |
| [35] | In-house | OsiriX + Netfabb + Fusion 360 | PETG | Hydrogen peroxide | FDM |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frizziero, L.; Santi, G.M.; Leon-Cardenas, C.; Donnici, G.; Liverani, A.; Papaleo, P.; Napolitano, F.; Pagliari, C.; Di Gennaro, G.L.; Stallone, S.; et al. In-House, Fast FDM Prototyping of a Custom Cutting Guide for a Lower-Risk Pediatric Femoral Osteotomy. Bioengineering 2021, 8, 71. https://doi.org/10.3390/bioengineering8060071
Frizziero L, Santi GM, Leon-Cardenas C, Donnici G, Liverani A, Papaleo P, Napolitano F, Pagliari C, Di Gennaro GL, Stallone S, et al. In-House, Fast FDM Prototyping of a Custom Cutting Guide for a Lower-Risk Pediatric Femoral Osteotomy. Bioengineering. 2021; 8(6):71. https://doi.org/10.3390/bioengineering8060071
Chicago/Turabian StyleFrizziero, Leonardo, Gian Maria Santi, Christian Leon-Cardenas, Giampiero Donnici, Alfredo Liverani, Paola Papaleo, Francesca Napolitano, Curzio Pagliari, Giovanni Luigi Di Gennaro, Stefano Stallone, and et al. 2021. "In-House, Fast FDM Prototyping of a Custom Cutting Guide for a Lower-Risk Pediatric Femoral Osteotomy" Bioengineering 8, no. 6: 71. https://doi.org/10.3390/bioengineering8060071