
Metal Oxide Nanoparticles and Nanotubes: Ultrasmall Nanostructures to Engineer Antibacterial and Improved Dental Adhesives and Composites

 , , and
, , and 
Abstract
:
1. Introduction
2. How Long Do Composite Restorations Last?
3. Nanotechnology in Dentistry
4. The Use of Metallic Oxide Particles in Restorative Dentistry
4.1. Titanium Dioxide (TiO2)
4.2. Zinc Oxide (ZnO)
4.3. Copper Oxide Nanoparticles
4.4. Iron Oxide (Fe2O3)
4.5. Cerium Oxide (CeO2)
4.6. Tantalum Oxide (Ta2O5)
4.7. Niobium Pentoxide (Nb2O5)
4.8. Zirconium Oxide (ZrO2)
5. The Use of Nanotubes in Restorative Dentistry
5.1. Titanium Dioxide Nanotubes
5.2. Halloysite Nanotubes
- (1)
- The H+ exchange and modification of silica network, creating a layer highly doped with SiO2;
- (2)
- The layer of SiO2 stimulates the precipitation of calcium and phosphate ions from the artificial saliva or SBF;
- (3)
- Differences in electronegativity between HNTs and the environment, which is rich in calcium and magnesium cations, induce the mineral nucleation and formation of apatite-like particles on the surface of the polymer doped with HNTs.
5.3. Boron Nitride Nanotubes
6. Future Perspectives and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Edelstein, B.L. The Dental Caries Pandemic and Disparities Problem. BMC Oral Health 2006, 6 (Suppl. 1), S2. [Google Scholar] [CrossRef] [Green Version]
- Martins, M.T.; Sardenberg, F.; Bendo, C.B.; Abreu, M.H.; Vale, M.P.; Paiva, S.M.; Pordeus, I.A. Dental Caries Remains as the Main Oral Condition with the Greatest Impact on Children’s Quality of Life. PLoS ONE 2017, 12, e0185365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitwalli, H.; Alsahafi, R.; Balhaddad, A.A.; Weir, M.D.; Xu, H.H.K.; Melo, M.A.S. Emerging Contact-Killing Antibacterial Strategies for Developing Anti-Biofilm Dental Polymeric Restorative Materials. Bioengineering 2020, 7, 83. [Google Scholar] [CrossRef]
- Balhaddad, A.A.; Kansara, A.A.; Hidan, D.; Weir, M.D.; Xu, H.H.K.; Melo, M.A.S. Toward Dental Caries: Exploring Nanoparticle-Based Platforms and Calcium Phosphate Compounds for Dental Restorative Materials. Bioact. Mater. 2019, 4, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Balhaddad, A.A.; Garcia, I.M.; Mokeem, L.; Ibrahim, M.S.; Collares, F.M.; Weir, M.D.; Xu, H.H.K.; Melo, M.A.S. Bifunctional Composites for Biofilms Modulation on Cervical Restorations. J. Dent. Res. 2021, 100, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Alhareky, M.; Tavares, M. Amalgam vs Composite Restoration, Survival, and Secondary Caries. J. Evid. Based Dent. Pract. 2016, 16, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, R.L. Review of the Current Status and Challenges for Dental Posterior Restorative Composites: Clinical, Chemistry, and Physical Behavior Considerations. Summary of Discussion from the Portland Composites Symposium (POCOS) June 17–19, 2004, Oregon Health and Science University, Portland, Oregon. Dent. Mater. 2005, 21, 3–6. [Google Scholar] [CrossRef]
- Mjör, I.A.; Toffenetti, F. Secondary Caries: A Literature Review with Case Reports. Quintessence Int. 2000, 31, 165–179. [Google Scholar]
- Ferracane, J.L. Resin Composite—State of the Art. Dent. Mater. 2011, 27, 29–38. [Google Scholar] [CrossRef]
- Frost, P.M. An Audit on the Placement and Replacement of Restorations in a General Dental Practice. Prim. Dent. Care 2002, 9, 31–36. [Google Scholar] [CrossRef]
- Featherstone, J.D.B. The Continuum of Dental Caries—Evidence for a Dynamic Disease Process. J. Dent. Res. 2004, 83, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Shen, H.; Suh, B.I. Antibacterial Dental Restorative Materials: A State-of-the-Art Review. Am. J. Dent. 2012, 25, 337–346. [Google Scholar] [PubMed]
- Imazato, S. Antibacterial Properties of Resin Composites and Dentin Bonding Systems. Dent. Mater. 2003, 19, 449–457. [Google Scholar] [CrossRef]
- Kurata, S.; Hamada, N.; Kanazawa, A.; Endo, T. Study on Antibacterial Dental Resin Using Tri-n-Butyl(4-Vinylbenzyl)Phosphonium Chloride. Dent. Mater. J. 2011, 30, 960–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buonocore, M.G. A Simple Method of Increasing the Adhesion of Acrylic Filling Materials to Enamel Surfaces. J. Dent. Res. 1955, 34, 849–853. [Google Scholar] [CrossRef] [PubMed]
- Demarco, F.F.; Corrêa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J.M. Longevity of Posterior Composite Restorations: Not Only a Matter of Materials. Dent. Mater. 2012, 28, 87–101. [Google Scholar] [CrossRef]
- Opdam, N.J.M.; van de Sande, F.H.; Bronkhorst, E.; Cenci, M.S.; Bottenberg, P.; Pallesen, U.; Gaengler, P.; Lindberg, A.; Huysmans, M.C.D.N.J.M.; van Dijken, J.W. Longevity of Posterior Composite Restorations: A Systematic Review and Meta-Analysis. J. Dent. Res. 2014, 93, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Montag, R.; Dietz, W.; Nietzsche, S.; Lang, T.; Weich, K.; Sigusch, B.W.; Gaengler, P. Clinical and Micromorphologic 29-Year Results of Posterior Composite Restorations. J. Dent. Res. 2018, 97, 1431–1437. [Google Scholar] [CrossRef]
- Pallesen, U.; van Dijken, J.W.V. A Randomized Controlled 27 Years Follow up of Three Resin Composites in Class II Restorations. J. Dent. 2015, 43, 1547–1558. [Google Scholar] [CrossRef]
- Collares, K.; Opdam, N.J.M.; Laske, M.; Bronkhorst, E.M.; Demarco, F.F.; Correa, M.B.; Huysmans, M.C.D.N.J.M. Longevity of Anterior Composite Restorations in a General Dental Practice-Based Network. J. Dent. Res. 2017, 96, 1092–1099. [Google Scholar] [CrossRef]
- Balhaddad, A.A.; Ibrahim, M.S.; Weir, M.D.; Xu, H.H.K.; Melo, M.A.S. Concentration Dependence of Quaternary Ammonium Monomer on the Design of High-Performance Bioactive Composite for Root Caries Restorations. Dent. Mater. 2020, 36, e266–e278. [Google Scholar] [CrossRef] [PubMed]
- Mitwalli, H.; Balhaddad, A.A.; AlSahafi, R.; Oates, T.W.; Melo, M.A.S.; Xu, H.H.K.; Weir, M.D. Novel CaF2 Nanocomposites with Antibacterial Function and Fluoride and Calcium Ion Release to Inhibit Oral Biofilm and Protect Teeth. J. Funct. Biomater. 2020, 11, 56. [Google Scholar] [CrossRef] [PubMed]
- AlSahafi, R.; Balhaddad, A.A.; Mitwalli, H.; Ibrahim, M.S.; Melo, M.A.S.; Oates, T.W.; Xu, H.H.K.; Weir, M.D. Novel Crown Cement Containing Antibacterial Monomer and Calcium Phosphate Nanoparticles. Nanomaterials 2020, 10, 2001. [Google Scholar] [CrossRef]
- Imazato, S.; Kinomoto, Y.; Tarumi, H.; Torii, M.; Russell, R.R.; McCabe, J.F. Incorporation of Antibacterial Monomer MDPB into Dentin Primer. J. Dent. Res. 1997, 76, 768–772. [Google Scholar] [CrossRef]
- Xu, X.; Wang, Y.; Liao, S.; Wen, Z.T.; Fan, Y. Synthesis and Characterization of Antibacterial Dental Monomers and Composites. J. Biomed. Mater. Res. B Appl. Biomater. 2012, 100, 1151–1162. [Google Scholar] [CrossRef] [Green Version]
- Lendenmann, U.; Grogan, J.; Oppenheim, F.G. Saliva and Dental Pellicle—A Review. Adv. Dent. Res. 2000, 14, 22–28. [Google Scholar] [CrossRef]
- Busscher, H.J.; Rinastiti, M.; Siswomihardjo, W.; van der Mei, H.C. Biofilm Formation on Dental Restorative and Implant Materials. J. Dent. Res. 2010, 89, 657–665. [Google Scholar] [CrossRef]
- Ishihara, K.; Nomura, H.; Mihara, T.; Kurita, K.; Iwasaki, Y.; Nakabayashi, N. Why Do Phospholipid Polymers Reduce Protein Adsorption? J. Biomed. Mater. Res. 1998, 39, 323–330. [Google Scholar] [CrossRef]
- Ishihara, K.; Ziats, N.P.; Tierney, B.P.; Nakabayashi, N.; Anderson, J.M. Protein Adsorption from Human Plasma Is Reduced on Phospholipid Polymers. J. Biomed. Mater. Res. 1991, 25, 1397–1407. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Melo, M.A.S.; Bai, Y.; Xu, H.H.K. Novel Protein-Repellent Dental Adhesive Containing 2-Methacryloyloxyethyl Phosphorylcholine. J. Dent. 2014, 42, 1284–1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, N.; Ma, J.; Melo, M.A.S.; Weir, M.D.; Bai, Y.; Xu, H.H.K. Protein-Repellent and Antibacterial Dental Composite to Inhibit Biofilms and Caries. J. Dent. 2015, 43, 225–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allaker, R.P. The Use of Nanoparticles to Control Oral Biofilm Formation. J. Dent. Res. 2010, 89, 1175–1186. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, D.R.; Gorup, L.F.; Takamiya, A.S.; Ruvollo-Filho, A.C.; de Camargo, E.R.; Barbosa, D.B. The Growing Importance of Materials That Prevent Microbial Adhesion: Antimicrobial Effect of Medical Devices Containing Silver. Int. J. Antimicrob. Agents 2009, 34, 103–110. [Google Scholar] [CrossRef]
- Percival, S.L.; Bowler, P.G.; Russell, D. Bacterial Resistance to Silver in Wound Care. J. Hosp. Infect. 2005, 60, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Weir, M.D.; Xu, H.H.K.; Antonucci, J.M.; Lin, N.J.; Lin-Gibson, S.; Xu, S.M.; Zhou, X. Effect of Amorphous Calcium Phosphate and Silver Nanocomposites on Dental Plaque Microcosm Biofilms. J. Biomed. Mater. Res. B Appl. Biomater. 2012, 100, 1378–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, J.L.; Sun, L.; Chow, L.C.; Xu, H.H.K. Mechanical and Acid Neutralizing Properties and Bacteria Inhibition of Amorphous Calcium Phosphate Dental Nanocomposite. J. Biomed. Mater. Res. B Appl. Biomater. 2011, 98, 80–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.H.K.; Moreau, J.L.; Sun, L.; Chow, L.C. Nanocomposite Containing Amorphous Calcium Phosphate Nanoparticles for Caries Inhibition. Dent. Mater. 2011, 27, 762–769. [Google Scholar] [CrossRef] [Green Version]
- Liang, K.; Xiao, S.; Wu, J.; Li, J.; Weir, M.D.; Cheng, L.; Reynolds, M.A.; Zhou, X.; Xu, H.H.K. Long-Term Dentin Remineralization by Poly(Amido Amine) and Rechargeable Calcium Phosphate Nanocomposite after Fluid Challenges. Dent. Mater. 2018, 34, 607–618. [Google Scholar] [CrossRef] [PubMed]
- Peumans, M.; De Munck, J.; Mine, A.; Van Meerbeek, B. Clinical Effectiveness of Contemporary Adhesives for the Restoration of Non-Carious Cervical Lesions. A Systematic Review. Dent. Mater. 2014, 30, 1089–1103. [Google Scholar] [CrossRef]
- de Paris Matos, T.; Perdigão, J.; de Paula, E.; Coppla, F.; Hass, V.; Scheffer, R.F.; Reis, A.; Loguercio, A.D. Five-Year Clinical Evaluation of a Universal Adhesive: A Randomized Double-Blind Trial. Dent. Mater. 2020, 36, 1474–1485. [Google Scholar] [CrossRef]
- 14:00–17:00 ISO/TR 10993-22:2017. Available online: https://www.iso.org/cms/render/live/en/sites/isoorg/contents/data/standard/06/59/65918.html (accessed on 22 September 2021).
- ETPN | Nanomedicine European Technology Platform. Available online: https://etp-nanomedicine.eu/ (accessed on 22 September 2021).
- Besinis, A.; De Peralta, T.; Tredwin, C.J.; Handy, R.D. Review of Nanomaterials in Dentistry: Interactions with the Oral Microenvironment, Clinical Applications, Hazards, and Benefits. ACS Nano 2015, 9, 2255–2289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Priyadarsini, S.; Mukherjee, S.; Mishra, M. Nanoparticles Used in Dentistry: A Review. J. Oral Biol. Craniofac. Res. 2018, 8, 58–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Definition-Nanomaterials-Environment-European Commission. Available online: https://ec.europa.eu/environment/chemicals/nanotech/faq/definition_en.htm (accessed on 22 September 2021).
- Saafan, A.; Zaazou, M.H.; Sallam, M.K.; Mosallam, O.; El Danaf, H.A. Assessment of Photodynamic Therapy and Nanoparticles Effects on Caries Models. Open Access Maced. J. Med. Sci. 2018, 6, 1289–1295. [Google Scholar] [CrossRef] [Green Version]
- Cao, W.; Zhang, Y.; Wang, X.; Li, Q.; Xiao, Y.; Li, P.; Wang, L.; Ye, Z.; Xing, X. Novel Resin-Based Dental Material with Anti-Biofilm Activity and Improved Mechanical Property by Incorporating Hydrophilic Cationic Copolymer Functionalized Nanodiamond. J. Mater. Sci. Mater. Med. 2018, 29, 162. [Google Scholar] [CrossRef] [PubMed]
- Magalhães, A.-P.-R.; Moreira, F.-C.-L.; Alves, D.-R.-S.; Estrela, C.-R.-A.; Estrela, C.; Carrião, M.-S.; Bakuzis, A.-F.; Lopes, L.-G. Silver Nanoparticles in Resin Luting Cements: Antibacterial and Physiochemical Properties. J. Clin. Exp. Dent. 2016, 8, e415–e422. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Han, Z.; Huang, Z.; Karki, J.; Wang, C.; Zhu, B.; Zhang, X. Antibacterial Activity, Cytotoxicity and Mechanical Behavior of Nano-Enhanced Denture Base Resin with Different Kinds of Inorganic Antibacterial Agents. Dent. Mater. J. 2017, 36, 693–699. [Google Scholar] [CrossRef] [Green Version]
- Moreira, D.M.; Oei, J.; Rawls, H.R.; Wagner, J.; Chu, L.; Li, Y.; Zhang, W.; Whang, K. A Novel Antimicrobial Orthodontic Band Cement with in Situ-Generated Silver Nanoparticles. Angle Orthod. 2015, 85, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Cao, W.; Zhang, Y.; Wang, X.; Chen, Y.; Li, Q.; Xing, X.; Xiao, Y.; Peng, X.; Ye, Z. Development of a Novel Resin-Based Dental Material with Dual Biocidal Modes and Sustained Release of Ag+ Ions Based on Photocurable Core-Shell AgBr/Cationic Polymer Nanocomposites. J. Mater. Sci. Mater. Med. 2017, 28, 103. [Google Scholar] [CrossRef]
- Akin, S.; Sonmezoglu, S. Chapter 2—Metal Oxide Nanoparticles as Electron Transport Layer for Highly Efficient Dye-Sensitized Solar Cells. In Emerging Materials for Energy Conversion and Storage; Cheong, K.Y., Impellizzeri, G., Fraga, M.A., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 39–79. ISBN 978-0-12-813794-9. [Google Scholar]
- Chavali, M.S.; Nikolova, M.P. Metal Oxide Nanoparticles and Their Applications in Nanotechnology. SN Appl. Sci. 2019, 1, 607. [Google Scholar] [CrossRef] [Green Version]
- Sodagar, A.; Akhoundi, M.S.A.; Bahador, A.; Jalali, Y.F.; Behzadi, Z.; Elhaminejad, F.; Mirhashemi, A.H. Effect of TiO2 Nanoparticles Incorporation on Antibacterial Properties and Shear Bond Strength of Dental Composite Used in Orthodontics. Dent. Press J. Orthod. 2017, 22, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Xia, Y.; Zhang, F.; Xie, H.; Gu, N. Nanoparticle-Reinforced Resin-Based Dental Composites. J. Dent. 2008, 36, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Forster, A.M.; Johnson, P.M.; Eidelman, N.; Quinn, G.; Schumacher, G.; Zhang, X.; Wu, W. Improving Performance of Dental Resins by Adding Titanium Dioxide Nanoparticles. Dent. Mater. 2011, 27, 972–982. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Watson, S.S.; Allsopp, D.A.; Stanley, D.; Skrtic, D. Tuning Photo-Catalytic Activities of TiO2 Nanoparticles Using Dimethacrylate Resins. Dent. Mater. 2016, 32, 363–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavassoli Hojati, S.; Alaghemand, H.; Hamze, F.; Ahmadian Babaki, F.; Rajab-Nia, R.; Rezvani, M.B.; Kaviani, M.; Atai, M. Antibacterial, Physical and Mechanical Properties of Flowable Resin Composites Containing Zinc Oxide Nanoparticles. Dent. Mater. 2013, 29, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Garcia, I.M.; Balhaddad, A.A.; Ibrahim, M.S.; Weir, M.D.; Xu, H.H.K.; Collares, F.M.; Melo, M.A.S. Antibacterial Response of Oral Microcosm Biofilm to Nano-Zinc Oxide in Adhesive Resin. Dent. Mater. 2021, 37, e182–e193. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Deng, M.; Kaps, S.; Zhu, X.; Hölken, I.; Mess, K.; Adelung, R.; Mishra, Y.K. Study of Tetrapodal ZnO-PDMS Composites: A Comparison of Fillers Shapes in Stiffness and Hydrophobicity Improvements. PLoS ONE 2014, 9, e106991. [Google Scholar] [CrossRef]
- Zajdowicz, S.; Song, H.B.; Baranek, A.; Bowman, C.N. Evaluation of Biofilm Formation on Novel Copper-Catalyzed Azide-Alkyne Cycloaddition (CuAAC)-Based Resins for Dental Restoratives. Dent. Mater. 2018, 34, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Song, H.B.; Sowan, N.; Shah, P.K.; Baranek, A.; Flores, A.; Stansbury, J.W.; Bowman, C.N. Reduced Shrinkage Stress via Photo-Initiated Copper(I)-Catalyzed Cycloaddition Polymerizations of Azide-Alkyne Resins. Dent. Mater. 2016, 32, 1332–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, I.M.; Balhaddad, A.A.; Lan, Y.; Simionato, A.; Ibrahim, M.S.; Weir, M.D.; Masri, R.; Xu, H.H.K.; Collares, F.M.; Melo, M.A.S. Magnetic Motion of Superparamagnetic Iron Oxide Nanoparticles- Loaded Dental Adhesives: Physicochemical/Biological Properties, and Dentin Bonding Performance Studied through the Tooth Pulpal Pressure Model. Acta Biomater 2021. [Google Scholar] [CrossRef]
- Li, Y.; Hu, X.; Xia, Y.; Ji, Y.; Ruan, J.; Weir, M.D.; Lin, X.; Nie, Z.; Gu, N.; Masri, R.; et al. Novel Magnetic Nanoparticle-Containing Adhesive with Greater Dentin Bond Strength and Antibacterial and Remineralizing Capabilities. Dent. Mater. 2018, 34, 1310–1322. [Google Scholar] [CrossRef] [PubMed]
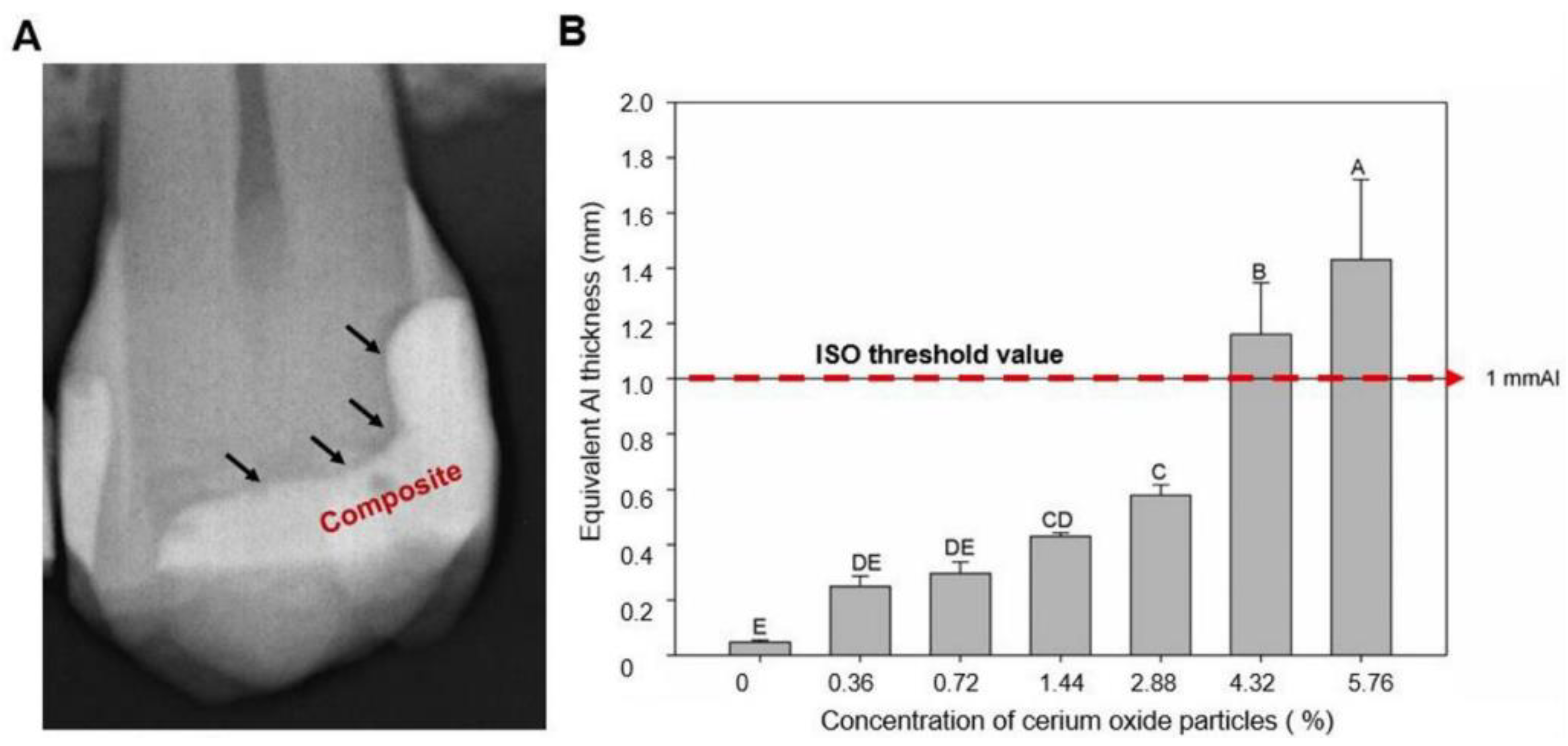
- Garcia, I.M.; Leitune, V.C.B.; Takimi, A.S.; Bergmann, C.P.; Samuel, S.M.W.; Melo, M.A.; Collares, F.M. Cerium Dioxide Particles to Tune Radiopacity of Dental Adhesives: Microstructural and Physico-Chemical Evaluation. J. Funct. Biomater. 2020, 11, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pypen, C.M.; Plenk, H.; Ebel, M.F.; Svagera, R.; Wernisch, J. Characterization of Microblasted and Reactive Ion Etched Surfaces on the Commercially Pure Metals Niobium, Tantalum and Titanium. J. Mater. Sci. Mater. Med. 1997, 8, 781–784. [Google Scholar] [CrossRef] [PubMed]
- Bencharit, S.; Byrd, W.C.; Altarawneh, S.; Hosseini, B.; Leong, A.; Reside, G.; Morelli, T.; Offenbacher, S. Development and Applications of Porous Tantalum Trabecular Metal-Enhanced Titanium Dental Implants. Clin. Implant Dent. Relat. Res. 2014, 16, 817–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, I.M.; Leitune, V.C.B.; Ferreira, C.J.; Collares, F.M. Tantalum Oxide as Filler for Dental Adhesive Resin. Dent. Mater. J. 2018, 37, 897–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, I.M.; Souza, V.S.; Scholten, J.D.; Collares, F.M. Quantum Dots of Tantalum Oxide with an Imidazolium Ionic Liquid as Antibacterial Agent for Adhesive Resin. J. Adhes. Dent. 2020, 22, 207–214. [Google Scholar] [CrossRef]
- Leitune, V.C.B.; Collares, F.M.; Takimi, A.; de Lima, G.B.; Petzhold, C.L.; Bergmann, C.P.; Samuel, S.M.W. Niobium Pentoxide as a Novel Filler for Dental Adhesive Resin. J. Dent. 2013, 41, 106–113. [Google Scholar] [CrossRef] [Green Version]
- Kolb, C.; Gumpert, K.; Wolter, H.; Sextl, G. Highly Translucent Dental Resin Composites through Refractive Index Adaption Using Zirconium Dioxide Nanoparticles and Organic Functionalization. Dent. Mater. 2020, 36, 1332–1342. [Google Scholar] [CrossRef] [PubMed]
- Lohbauer, U.; Wagner, A.; Belli, R.; Stoetzel, C.; Hilpert, A.; Kurland, H.-D.; Grabow, J.; Müller, F.A. Zirconia Nanoparticles Prepared by Laser Vaporization as Fillers for Dental Adhesives. Acta Biomater. 2010, 6, 4539–4546. [Google Scholar] [CrossRef] [PubMed]
- Jafari, S.; Mahyad, B.; Hashemzadeh, H.; Janfaza, S.; Gholikhani, T.; Tayebi, L. Biomedical Applications of TiO2 Nanostructures: Recent Advances. Int. J. Nanomed. 2020, 15, 3447–3470. [Google Scholar] [CrossRef]
- Garimella, R.; Eltorai, A.E.M. Nanotechnology in Orthopedics. J. Orthop. 2016, 14, 30–33. [Google Scholar] [CrossRef] [Green Version]
- Baan, R.; Straif, K.; Grosse, Y.; Secretan, B.; El Ghissassi, F.; Cogliano, V.; WHO International Agency for Research on Cancer Monograph Working Group. Carcinogenicity of Carbon Black, Titanium Dioxide, and Talc. Lancet Oncol. 2006, 7, 295–296. [Google Scholar] [CrossRef]
- Bavykin, D.V.; Friedrich, J.M.; Walsh, F.C. Protonated Titanates and TiO2 Nanostructured Materials: Synthesis, Properties, and Applications. Adv. Mater. 2006, 18, 2807–2824. [Google Scholar] [CrossRef]
- Bonetta, S.; Bonetta, S.; Motta, F.; Strini, A.; Carraro, E. Photocatalytic Bacterial Inactivation by TiO2-Coated Surfaces. AMB Express 2013, 3, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weintraub, J.; Burt, B. Oral Health Status in the United States: Tooth Loss and Edentulism. J. Dent. Educ. 1985, 49, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Contreras, R.; Scougall-Vilchis, R.J.; Contreras-Bulnes, R.; Sakagami, H.; Morales-Luckie, R.A.; Nakajima, H. Mechanical, Antibacterial and Bond Strength Properties of Nano-Titanium-Enriched Glass Ionomer Cement. J. Appl. Oral Sci. 2015, 23, 321–328. [Google Scholar] [CrossRef] [Green Version]
- Navío, J.A.; Colón, G.; Macías, M.; Real, C.; Litter, M.I. Iron-doped titania semiconductor powders prepared by a sol-gel method. Part I: Synthesis and characterization. Appl. Catal. A Gen. 1999, 177, 111–120. [Google Scholar] [CrossRef]
- Chen, X.; Liu, L.; Yu, P.Y.; Mao, S.S. Increasing Solar Absorption for Photocatalysis with Black Hydrogenated Titanium Dioxide Nanocrystals. Science 2011, 331, 746–750. [Google Scholar] [CrossRef]
- Fang, M.; Chen, J.-H.; Xu, X.-L.; Yang, P.-H.; Hildebrand, H.F. Antibacterial Activities of Inorganic Agents on Six Bacteria Associated with Oral Infections by Two Susceptibility Tests. Int. J. Antimicrob. Agents 2006, 27, 513–517. [Google Scholar] [CrossRef]
- Ordinola-Zapata, R.; Bramante, C.M.; GarcÍa-godoy, F.; Moldauer, B.I.; Minotti, P.G.; TercíLIA Grizzo, L.; Duarte, M.A.H. The Effect of Radiopacifiers Agents on PH, Calcium Release, Radiopacity, and Antimicrobial Properties of Different Calcium Hydroxide Dressings. Microsc. Res. Tech. 2015, 78, 620–625. [Google Scholar] [CrossRef]
- Adams, L.K.; Lyon, D.Y.; McIntosh, A.; Alvarez, P.J.J. Comparative Toxicity of Nano-Scale TiO2, SiO2 and ZnO Water Suspensions. Water Sci. Technol. 2006, 54, 327–334. [Google Scholar] [CrossRef]
- Garcia, I.M.; Leitune, V.C.B.; Visioli, F.; Samuel, S.M.W.; Collares, F.M. Influence of Zinc Oxide Quantum Dots in the Antibacterial Activity and Cytotoxicity of an Experimental Adhesive Resin. J. Dent. 2018, 73, 57–60. [Google Scholar] [CrossRef]
- Osorio, R.; Cabello, I.; Toledano, M. Bioactivity of Zinc-Doped Dental Adhesives. J. Dent. 2014, 42, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Divya, M.; Vaseeharan, B.; Abinaya, M.; Vijayakumar, S.; Govindarajan, M.; Alharbi, N.S.; Kadaikunnan, S.; Khaled, J.M.; Benelli, G. Biopolymer Gelatin-Coated Zinc Oxide Nanoparticles Showed High Antibacterial, Antibiofilm and Anti-Angiogenic Activity. J. Photochem. Photobiol. B Biol. 2018, 178, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Collares, F.M.; Garcia, I.M.; Klein, M.; Parolo, C.F.; Sánchez, F.A.L.; Takimi, A.; Bergmann, C.P.; Samuel, S.M.W.; Melo, M.A.; Leitune, V.C. Exploring Needle-Like Zinc Oxide Nanostructures for Improving Dental Resin Sealers: Design and Evaluation of Antibacterial, Physical and Chemical Properties. Polymers 2020, 12, 789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, G.; Hu, D.; Cheng, E.; Vargas-Reus, M.; Reip, P.; Allaker, R. Characterisation of Copper Oxide Nanoparticles for Antimicrobial Applications. Int. J. Antimicrob. Agents 2009, 33, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Song, H.B.; Wang, X.; Patton, J.R.; Stansbury, J.W.; Bowman, C.N. Kinetics and Mechanics of Photo-Polymerized Triazole-Containing Thermosetting Composites via the Copper(I)-Catalyzed Azide-Alkyne Cycloaddition. Dent. Mater. 2017, 33, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Chen, H.; Zhang, F.; Wang, L.; Chen, B.; Reynolds, M.A.; Ma, J.; Schneider, A.; Gu, N.; Xu, H.H.K. Injectable Calcium Phosphate Scaffold with Iron Oxide Nanoparticles to Enhance Osteogenesis via Dental Pulp Stem Cells. Artif. Cells Nanomed. Biotechnol. 2018, 46, 423–433. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.; Zhou, Z.; Mao, H.; Yang, L. Magnetic Nanoparticles for Precision Oncology: Theranostic Magnetic Iron Oxide Nanoparticles for Image-Guided and Targeted Cancer Therapy. Nanomedicine 2017, 12, 73–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iv, M.; Telischak, N.; Feng, D.; Holdsworth, S.J.; Yeom, K.W.; Daldrup-Link, H.E. Clinical Applications of Iron Oxide Nanoparticles for Magnetic Resonance Imaging of Brain Tumors. Nanomedicine 2015, 10, 993–1018. [Google Scholar] [CrossRef]
- Singh, K.R.; Nayak, V.; Sarkar, T.; Singh, R.P. Cerium Oxide Nanoparticles: Properties, Biosynthesis and Biomedical Application. RSC Adv. 2020, 10, 27194–27214. [Google Scholar] [CrossRef]
- Xia, T.; Kovochich, M.; Liong, M.; Mädler, L.; Gilbert, B.; Shi, H.; Yeh, J.I.; Zink, J.I.; Nel, A.E. Comparison of the Mechanism of Toxicity of Zinc Oxide and Cerium Oxide Nanoparticles Based on Dissolution and Oxidative Stress Properties. ACS Nano 2008, 2, 2121–2134. [Google Scholar] [CrossRef] [Green Version]
- Gojova, A.; Lee, J.-T.; Jung, H.S.; Guo, B.; Barakat, A.I.; Kennedy, I.M. Effect of Cerium Oxide Nanoparticles on Inflammation in Vascular Endothelial Cells. Inhal. Toxicol. 2009, 21 (Suppl. 1), 123–130. [Google Scholar] [CrossRef] [Green Version]
- Espelid, I.; Tveit, A.B.; Erickson, R.L.; Keck, S.C.; Glasspoole, E.A. Radiopacity of Restorations and Detection of Secondary Caries. Dent. Mater. 1991, 7, 114–117. [Google Scholar] [CrossRef]
- Akça, B.; Erzeneoğlu, S.Z. The Mass Attenuation Coefficients, Electronic, Atomic, and Molecular Cross Sections, Effective Atomic Numbers, and Electron Densities for Compounds of Some Biomedically Important Elements at 59.5 KeV. Sci. Technol. Nucl. Install. 2014, 2014, e901465. [Google Scholar] [CrossRef] [Green Version]
- Sagherian, B.H.; Claridge, R.J. The Use of Tantalum Metal in Foot and Ankle Surgery. Orthop. Clin. N. Am. 2019, 50, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Asadullah, S.; Mei, S.; Yang, K.; Hu, X.; Wang, F.; Yu, B.; Wu, Z.; Wei, J. Tantalum Oxide Submicro-Particles into Microporous Coating on Polyimide Possessing Antibacterial Property and Inducing Cellular Response for Orthopedic Application. J. Mech. Behav. Biomed. Mater. 2021, 124, 104800. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.S.; McCormick, J.R.; Ghasem, A.; Huntley, S.R.; Gjolaj, J.P. Tantalum: The next Biomaterial in Spine Surgery? J. Spine Surg. 2020, 6, 72–86. [Google Scholar] [CrossRef] [PubMed]
- Maho, A.; Detriche, S.; Delhalle, J.; Mekhalif, Z. Sol-Gel Synthesis of Tantalum Oxide and Phosphonic Acid-Modified Carbon Nanotubes Composite Coatings on Titanium Surfaces. Mater. Sci. Eng. C Mater. Biol. Appl. 2013, 33, 2686–2697. [Google Scholar] [CrossRef] [PubMed]
- Velten, D.; Eisenbarth, E.; Schanne, N.; Breme, J. Biocompatible Nb2O5 Thin Films Prepared by Means of the Sol-Gel Process. J. Mater. Sci. Mater. Med. 2004, 15, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Mazur, M.; Kalisz, M.; Wojcieszak, D.; Grobelny, M.; Mazur, P.; Kaczmarek, D.; Domaradzki, J. Determination of Structural, Mechanical and Corrosion Properties of Nb2O5 and (NbyCu1−y)Ox Thin Films Deposited on Ti6Al4V Alloy Substrates for Dental Implant Applications. Mater. Sci. Eng. C 2015, 47, 211–221. [Google Scholar] [CrossRef]
- Li, Y.; Munir, K.S.; Lin, J.; Wen, C. Titanium-Niobium Pentoxide Composites for Biomedical Applications. Bioact. Mater. 2016, 1, 127–131. [Google Scholar] [CrossRef] [Green Version]
- Garcia, I.M.; Leitune, V.C.B.; Balbinot, G.D.S.; Samuel, S.M.W.; Collares, F.M. Influence of Niobium Pentoxide Addition on the Properties of Glass Ionomer Cements. Acta Biomater. Odontol. Scand. 2016, 2, 138–143. [Google Scholar] [CrossRef] [Green Version]
- Jangra, S.L.; Stalin, K.; Dilbaghi, N.; Kumar, S.; Tawale, J.; Singh, S.P.; Pasricha, R. Antimicrobial Activity of Zirconia (ZrO2) Nanoparticles and Zirconium Complexes. J. Nanosci. Nanotechnol. 2012, 12, 7105–7112. [Google Scholar] [CrossRef] [PubMed]
- Gowri, S.; Rajiv Gandhi, R.; Sundrarajan, M. Structural, Optical, Antibacterial and Antifungal Properties of Zirconia Nanoparticles by Biobased Protocol. J. Mater. Sci. Technol. 2014, 30, 782–790. [Google Scholar] [CrossRef]
- Bona, A.D.; Pecho, O.E.; Alessandretti, R. Zirconia as a Dental Biomaterial. Materials 2015, 8, 4978–4991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fizir, M.; Dramou, P.; Dahiru, N.S.; Ruya, W.; Huang, T.; He, H. Halloysite Nanotubes in Analytical Sciences and in Drug Delivery: A Review. Mikrochim. Acta 2018, 185, 389. [Google Scholar] [CrossRef]
- Feng, W.; Geng, Z.; Li, Z.; Cui, Z.; Zhu, S.; Liang, Y.; Liu, Y.; Wang, R.; Yang, X. Controlled Release Behaviour and Antibacterial Effects of Antibiotic-Loaded Titania Nanotubes. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 62, 105–112. [Google Scholar] [CrossRef]
- Degrazia, F.W.; Leitune, V.C.B.; Takimi, A.S.; Collares, F.M.; Sauro, S. Physicochemical and Bioactive Properties of Innovative Resin-Based Materials Containing Functional Halloysite-Nanotubes Fillers. Dent. Mater. 2016, 32, 1133–1143. [Google Scholar] [CrossRef]
- Degrazia, F.W.; Genari, B.; Leitune, V.C.B.; Arthur, R.A.; Luxan, S.A.; Samuel, S.M.W.; Collares, F.M.; Sauro, S. Polymerisation, Antibacterial and Bioactivity Properties of Experimental Orthodontic Adhesives Containing Triclosan-Loaded Halloysite Nanotubes. J. Dent. 2018, 69, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Garcia, I.M.; Leitune, V.C.B.; Arthur, R.A.; Nunes, J.; Visioli, F.; Giovarruscio, M.; Sauro, S.; Collares, F.M. Chemical, Mechanical and Biological Properties of an Adhesive Resin with Alkyl Trimethyl Ammonium Bromide-Loaded Halloysite Nanotubes. J. Adhes. Dent. 2020, 22, 399–407. [Google Scholar] [CrossRef]
- Kalagi, S.; Feitosa, S.A.; Münchow, E.A.; Martins, V.M.; Karczewski, A.E.; Cook, N.B.; Diefenderfer, K.; Eckert, G.J.; Geraldeli, S.; Bottino, M.C. Chlorhexidine-Modified Nanotubes and Their Effects on the Polymerization and Bonding Performance of a Dental Adhesive. Dent. Mater. 2020, 36, 687–697. [Google Scholar] [CrossRef]
- Palasuk, J.; Windsor, L.J.; Platt, J.A.; Lvov, Y.; Geraldeli, S.; Bottino, M.C. Doxycycline-Loaded Nanotube-Modified Adhesives Inhibit MMP in a Dose-Dependent Fashion. Clin. Oral Investig. 2018, 22, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Degrazia, F.W.; Leitune, V.C.B.; Samuel, S.M.W.; Collares, F.M. Boron Nitride Nanotubes as Novel Fillers for Improving the Properties of Dental Adhesives. J. Dent. 2017, 62, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Degrazia, F.W.; Leitune, V.C.B.; Visioli, F.; Samuel, S.M.W.; Collares, F.M. Long-Term Stability of Dental Adhesive Incorporated by Boron Nitride Nanotubes. Dent. Mater. 2018, 34, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Kokubo, T.; Takadama, H. How Useful Is SBF in Predicting in Vivo Bone Bioactivity? Biomaterials 2006, 27, 2907–2915. [Google Scholar] [CrossRef] [PubMed]
- Gulati, K.; Maher, S.; Findlay, D.M.; Losic, D. Titania Nanotubes for Orchestrating Osteogenesis at the Bone-Implant Interface. Nanomedicine 2016, 11, 1847–1864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pozio, A.; Palmieri, A.; Girardi, A.; Cura, F.; Carinci, F. Titanium Nanotubes Stimulate Osteoblast Differentiation of Stem Cells from Pulp and Adipose Tissue. Dent. Res. J. 2012, 9, S169–S174. [Google Scholar] [CrossRef]
- Xia, L.; Feng, B.; Wang, P.; Ding, S.; Liu, Z.; Zhou, J.; Yu, R. In Vitro and in Vivo Studies of Surface-Structured Implants for Bone Formation. Int. J. Nanomed. 2012, 7, 4873–4881. [Google Scholar] [CrossRef] [Green Version]
- Jorge, J.R.P.; Barão, V.A.; Delben, J.A.; Faverani, L.P.; Queiroz, T.P.; Assunção, W.G. Titanium in Dentistry: Historical Development, State of the Art and Future Perspectives. J. Indian Prosthodont. Soc. 2013, 13, 71–77. [Google Scholar] [CrossRef]
- Dafar, M.O.; Grol, M.W.; Canham, P.B.; Dixon, S.J.; Rizkalla, A.S. Reinforcement of Flowable Dental Composites with Titanium Dioxide Nanotubes. Dent. Mater. 2016, 32, 817–826. [Google Scholar] [CrossRef] [Green Version]
- Ramos-Tonello, C.M.; Lisboa-Filho, P.N.; Arruda, L.B.; Tokuhara, C.K.; Oliveira, R.C.; Furuse, A.Y.; Rubo, J.H.; Borges, A.F.S. Titanium Dioxide Nanotubes Addition to Self-Adhesive Resin Cement: Effect on Physical and Biological Properties. Dent. Mater. 2017, 33, 866–875. [Google Scholar] [CrossRef] [Green Version]
- Stürmer, M.; Garcia, I.M.; Souza, V.S.; Visioli, F.; Scholten, J.D.; Samuel, S.M.W.; Leitune, V.C.B.; Collares, F.M. Titanium Dioxide Nanotubes with Triazine-Methacrylate Monomer to Improve Physicochemical and Biological Properties of Adhesives. Dent. Mater. 2021, 37, 223–235. [Google Scholar] [CrossRef]
- Garcia, I.M.; Souza, V.S.; Hellriegel, C.; Scholten, J.D.; Collares, F.M. Ionic Liquid-Stabilized Titania Quantum Dots Applied in Adhesive Resin. J. Dent. Res. 2019, 98, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Huang, J.-Y.; Li, H.-Q.; Chen, Z.; Zhao, A.Z.-J.; Wang, Y.; Zhang, K.-Q.; Sun, H.-T.; Al-Deyab, S.S.; Lai, Y.-K. TiO2 Nanotube Platforms for Smart Drug Delivery: A Review. Int. J. Nanomed. 2016, 11, 4819–4834. [Google Scholar] [CrossRef] [Green Version]
- Parveen, S.; Misra, R.; Sahoo, S.K. Nanoparticles: A Boon to Drug Delivery, Therapeutics, Diagnostics and Imaging. Nanomedicine 2012, 8, 147–166. [Google Scholar] [CrossRef] [PubMed]
- Hasanzadeh Kafshgari, M.; Kah, D.; Mazare, A.; Nguyen, N.T.; Distaso, M.; Peukert, W.; Goldmann, W.H.; Schmuki, P.; Fabry, B. Anodic Titanium Dioxide Nanotubes for Magnetically Guided Therapeutic Delivery. Sci. Rep. 2019, 9, 13439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tharmavaram, M.; Pandey, G.; Rawtani, D. Surface Modified Halloysite Nanotubes: A Flexible Interface for Biological, Environmental and Catalytic Applications. Adv. Colloid Interface Sci. 2018, 261, 82–101. [Google Scholar] [CrossRef]
- Hench, L.L.; Wilson, J.K. Bioceramics; Elsevier Ltd.: Oxford, UK, 1993. [Google Scholar]
- Lahiri, D.; Singh, V.; Keshri, A.K.; Seal, S.; Agarwal, A. Apatite Formability of Boron Nitride Nanotubes. Nanotechnology 2011, 22, 205601. [Google Scholar] [CrossRef] [PubMed]
- Li, L.H.; Chen, Y. Superhydrophobic Properties of Nonaligned Boron Nitride Nanotube Films. Langmuir 2010, 26, 5135–5140. [Google Scholar] [CrossRef]
- Zhi, C.; Bando, Y.; Tang, C.; Xie, R.; Sekiguchi, T.; Golberg, D. Perfectly Dissolved Boron Nitride Nanotubes Due to Polymer Wrapping. J. Am. Chem. Soc. 2005, 127, 15996–15997. [Google Scholar] [CrossRef]
- Ferreira, C.J.; Leitune, V.C.B.; de Souza Balbinot, G.; Degrazia, F.W.; Arakelyan, M.; Sauro, S.; Mezzomo Collares, F. Antibacterial and Remineralizing Fillers in Experimental Orthodontic Adhesives. Materials 2019, 12, 652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balhaddad, A.A.; Mokeem, L.S.; Weir, M.D.; Xu, H.; Melo, M.A.S. Sustained Antibacterial Effect and Wear Behavior of Quaternary Ammonium Contact-Killing Dental Polymers after One-Year of Hydrolytic Degradation. Appl. Sci. 2021, 11, 3718. [Google Scholar] [CrossRef]
- Schmalz, G.; Hickel, R.; van Landuyt, K.L.; Reichl, F.-X. Nanoparticles in Dentistry. Dent. Mater. 2017, 33, 1298–1314. [Google Scholar] [CrossRef] [PubMed]
- Bernhoft, R.A. Mercury Toxicity and Treatment: A Review of the Literature. J. Environ. Public Health 2012, 2012, 460508. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.S.; Garcia, I.M.; Kensara, A.; Balhaddad, A.A.; Collares, F.M.; Williams, M.A.; Ibrahim, A.S.; Lin, N.J.; Weir, M.D.; Xu, H.H.K.; et al. How We Are Assessing the Developing Antibacterial Resin-Based Dental Materials? A Scoping Review. J. Dent. 2020, 99, 103369. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metallic Oxide | Potential Applications |
|---|---|
| Titanium Dioxide (TiO2) | |
| Zinc Oxide (ZnO) |
|
| Copper Oxide (CuO) |
|
| Iron Oxide (Fe2O3) |
|
| Cerium Oxide (CeO2) |
|
| Tantalum Oxide (Ta2O5) | |
| Niobium Pentoxide (Nb2O5) |
|
| Zirconium Oxide (ZrO2) |
| Nanotubes | Potential Applications |
|---|---|
| Titanium dioxide nanotubes (nt-TiO2) | nt-TiO2 were found effective in carrying 1,3,5-Trimethylhexahydro-1,3,5-triazine in a dental adhesive to exert antibacterial properties and improve the µ-tensile bond strength |
| Halloysite nanotubes (HNT) | HNT may deliver bioactive components around the incorporated materials by depositing calcium phosphate compounds, which may contribute to remineralization [112]. HNT can act as a drug delivery system with triclosan [113], quaternary ammonium compound [114], chlorhexidine [115], and doxycycline [116] in different resin-based materials |
| Boron nitride nanotubes (BNNTs) | BNNTs were found to increase the contact angle, decrease the surface energy, improve the mechanical properties [117], and preserved the bonding interface in a dental adhesive [118] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balhaddad, A.A.; Garcia, I.M.; Mokeem, L.; Alsahafi, R.; Collares, F.M.; Sampaio de Melo, M.A. Metal Oxide Nanoparticles and Nanotubes: Ultrasmall Nanostructures to Engineer Antibacterial and Improved Dental Adhesives and Composites. Bioengineering 2021, 8, 146. https://doi.org/10.3390/bioengineering8100146
Balhaddad AA, Garcia IM, Mokeem L, Alsahafi R, Collares FM, Sampaio de Melo MA. Metal Oxide Nanoparticles and Nanotubes: Ultrasmall Nanostructures to Engineer Antibacterial and Improved Dental Adhesives and Composites. Bioengineering. 2021; 8(10):146. https://doi.org/10.3390/bioengineering8100146
Chicago/Turabian StyleBalhaddad, Abdulrahman A., Isadora M. Garcia, Lamia Mokeem, Rashed Alsahafi, Fabrício Mezzomo Collares, and Mary Anne Sampaio de Melo. 2021. "Metal Oxide Nanoparticles and Nanotubes: Ultrasmall Nanostructures to Engineer Antibacterial and Improved Dental Adhesives and Composites" Bioengineering 8, no. 10: 146. https://doi.org/10.3390/bioengineering8100146