Instrumented Analysis of the Sit-to-Stand Movement for Geriatric Screening: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
- Older people: Old* OR elder* OR geriatric* OR senior* adj5 (people OR adult* OR person*)
- Sit-to-Stand: Sit-to-stand OR stand-to-sit OR chair stand OR STS OR 5STS OR 30STS OR CST
- Technology: sensor* OR instrument* OR accelerometer* OR gyroscope* OR magnetom* OR ICT OR device OR smartphone OR motion capture OR video OR Kinect OR camera
2.1. Types of Studies
2.2. Types of Participants
2.3. Primary Outcomes
2.4. Inclusion and Exclusion Criteria
2.5. Data Extraction
2.6. Quality Appraisal
3. Results
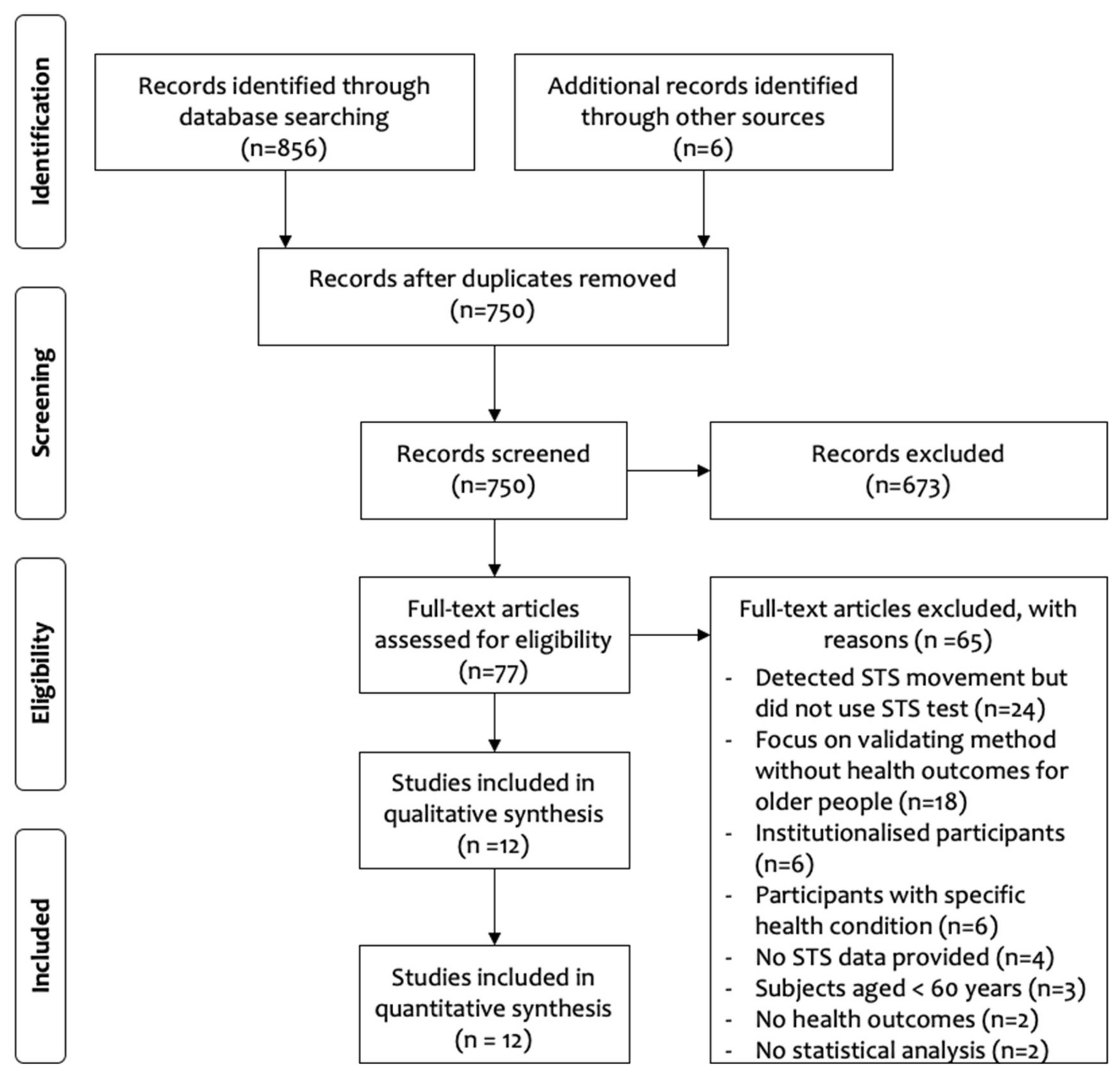
3.1. Article Selection
3.2. Study Characteristics
3.3. Evaluation of Fallers and Non-Fallers
3.4. Evaluation of Frailty Sub-Groups
4. Discussion
4.1. Overview
4.2. iSTS and Fallers
4.3. iSTS and Frailty
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- United Nations Department of Economic and Social Affairs Population Division. World Population Prospects: The 2017 Revision; United Nations: New York, NY, USA, 2017. [Google Scholar]
- Angulo, J.; El Assar, M.; Rodríguez-Mañas, L. Frailty and sarcopenia as the basis for the phenotypic manifestation of chronic diseases in older adults. Mol. Asp. Med. 2016, 50, 1–32. [Google Scholar] [CrossRef]
- Tyrovolas, S.; Koyanagi, A.; Olaya, B.; Ayuso-Mateos, J.L.; Miret, M.; Chatterji, S.; Tobiasz-Adamczyk, B.; Koskinen, S.; Leonardi, M.; Haro, J.M. Factors associated with skeletal muscle mass, sarcopenia, and sarcopenic obesity in older adults: A multi-continent study. J. Cachexia Sarcopenia Muscle 2016, 7, 312–321. [Google Scholar] [CrossRef]
- Morley, J.E. Sarcopenia: Diagnosis and treatment. J. Nutr. Health Aging 2008, 12, 452. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Anker, S.D.; Haehling, S. Prevalence, incidence and clinical impact of sarcopenia: Facts, numbers and epidemiology—Update 2014. J. Cachexia Sarcopenia Muscle 2014, 5, 253–259. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Ciol, M.A.; Hoffman, J.; Dudgeon, B.J.; Yorkston, K.; Chan, L. Falls in the medicare population: Incidence, associated factors, and impact on health care. Phys. Ther. 2009, 89, 324–332. [Google Scholar] [CrossRef] [Green Version]
- Grundstrom, A.C.; Guse, C.E.; Layde, P.M. Risk factors for falls and fall-related injuries in adults 85 years of age and older. Arch. Gerontol. Geriatr. 2012, 54, 421–428. [Google Scholar] [CrossRef] [Green Version]
- De Buyser, S.L.; Petrovic, M.; Taes, Y.E.; Toye, K.R.C.; Kaufman, J.M.; Lapauw, B.; Goemaere, S. Validation of the FNIH sarcopenia criteria and SOF frailty index as predictors of long-term mortality in ambulatory older men. Age Ageing 2016, 45, 603–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 4. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Nakakubo, S.; Hotta, R.; Suzuki, T. Predictive cutoff values of the five-times sit-to-stand test and the timed “Up & Go” test for disability incidence in older people dwelling in the community. Phys. Ther. 2017, 97, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Applebaum, E.V.; Breton, D.; Feng, Z.W.; Ta, A.T.; Walsh, K.; Chasse, K.; Robbins, S.M. Modified 30-second Sit to Stand test predicts falls in a cohort of institutionalized older veterans. PLoS ONE 2017, 12, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European working group on sarcopenia in older people. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.; Walsh, L.; Doyle, J.; Greene, B.; Blake, C. The reliability of the quantitative timed up and go test (QTUG) measured over five consecutive days under single and dual-task conditions in community dwelling older adults. Gait Posture 2016, 43, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Van Lummel, R.C.; Ainsworth, E.; Lindemann, U.; Zijlstra, W.; Chiari, L.; Van Campen, P.; Hausdorff, J.M. Automated approach for quantifying the repeated sit-to-stand using one body fixed sensor in young and older adults. Gait Posture 2013, 38, 153–156. [Google Scholar] [CrossRef] [Green Version]
- Millor, N.; Lecumberri, P.; Gomez, M.; Martinez-Ramirez, A.; Izquierdo, M. Kinematic parameters to evaluate functional performance of sit-to-stand and stand-to-sit transitions using motion sensor devices: A systematic review. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 926–936. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [Green Version]
- Silver, N.C.; Dunlap, W.P. Averaging correlation coefficients: Should Fisher’s z transformation be used? J. Appl. Psychol. 1987, 72, 146. [Google Scholar] [CrossRef]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipsey, M.W.; Wilson, D.B. Practical Meta-Analysis; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; deBeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Loney, P.L.; Chambers, L.W.; Bennett, K.J.; Roberts, J.G.; Stratford, P.W. Critical appraisal of the health research literature prevalence or incidence of a health problem. Chronic Dis. Can. 1998, 19, 170. [Google Scholar]
- Sanderson, S.; Tatt, I.D.; Higgins, J. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: A systematic review and annotated bibliography. Int. J. Epidemiol. 2007, 36, 666–676. [Google Scholar] [CrossRef] [Green Version]
- Payette, M.-C.; Bélanger, C.; Léveillé, V.; Grenier, S. Fall-Related Psychological Concerns and Anxiety among Community-Dwelling Older Adults: Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0152848. [Google Scholar] [CrossRef] [Green Version]
- Millor, N.; Lecumberri, P.; Gomez, M.; Martinez, A.; Martinikorena, J.; Rodriguez-Manas, L.; Garcia-Garcia, F.J.; Izquierdo, M. Gait Velocity and Chair Sit-Stand-Sit Performance Improves Current Frailty-Status Identification. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 2018–2025. [Google Scholar] [CrossRef] [PubMed]
- Millor, N.; Lecumberri, P.; Gomez, M.; Martinez-Ramirez, A.; Izquierdo, M. An evaluation of the 30-s chair stand test in older adults: Frailty detection based on kinematic parameters from a single inertial unit. J. Neuroeng. Rehabil. 2013, 10. [Google Scholar] [CrossRef] [Green Version]
- Millor, N.; Lecumberri, P.; Gomez, M.; Martinez-Ramirez, A.; Izquierdo, M. Frailty detection using the instrumented version of the 30-s chair stand test. In Replace, Repair, Restore, Relieve—Bridging Clinical and Engineering Solutions in Neurorehabilition; Springer: Cham, Switzerland, 2014; Volume 7, pp. 553–561. [Google Scholar] [CrossRef]
- Greene, B.R.; Doheny, E.P.; Kenny, R.A.; Caulfield, B. Classification of frailty and falls history using a combination of sensor-based mobility assessments. Physiol. Meas. 2014, 35, 2053–2066. [Google Scholar] [CrossRef]
- Doheny, E.P.; Fan, C.W.; Foran, T.; Greene, B.R.; Cunningham, C.; Kenny, R.A. An instrumented sit-to-stand test used to examine differences between older fallers and non-fallers. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 3063–3066. [Google Scholar]
- Doheny, E.P.; Walsh, C.; Foran, T.; Greene, B.R.; Fan, C.W.; Cunningham, C.; Kenny, R.A. Falls classification using tri-axial accelerometers during the five-times-sit-to-stand test. Gait Posture 2013, 38, 1021–1025. [Google Scholar] [CrossRef]
- Zhang, W.; Regterschot, G.R.H.; Geraedts, H.; Baldus, H.; Zijlstra, W. Chair rise peak power in daily life measured with a pendant sensor associates with mobility, limitation in activities and frailty in old people. IEEE J. Biomed. Health Inf. 2017, 21, 211–217. [Google Scholar] [CrossRef]
- Coni, A.; Mellone, S.; Colpo, M.; Guralnik, J.M.; Patel, K.V.; Bandinelli, S.; Chiari, L. An exploratory factor analysis of sensor-based physical capability assessment. Sensors 2019, 19, 2227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincenzo, J.L.; Gray, M.; Glenn, J.M. Validity of a novel, clinically relevant measure to differentiate functional power and movement velocity and discriminate fall history among older adults: A pilot investigation. Innov. Aging 2018, 2, igy028. [Google Scholar] [CrossRef] [Green Version]
- Ejupi, A.; Brodie, M.; Gschwind, Y.J.; Lord, S.R.; Zagler, W.L.; Delbaere, K. Kinect-based five-times-sit-to-stand test for clinical and in-home assessment of fall risk in older people. Gerontology 2016, 61, 118–124. [Google Scholar] [CrossRef]
- Houck, J.; Kneiss, J.; Bukata, S.V.; Puzas, J.E. Analysis of vertical ground reaction force variables during a Sit to Stand task in participants recovering from a hip fracture. Clin. Biomech. 2011, 26, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Peters, L.L.; Boter, H.; Buskens, E.; Slaets, J.P.J. Measurement Properties of the Groningen Frailty Indicator in Home-Dwelling; Institutionalized Elderly People. J. Am. Med. Dir. Assoc. 2012, 13, 546–551. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E.; Malmstrom, T.K.; Miller, D.K. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J. Nutr. Health Aging 2012, 16, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.W.; Roh, H.; Cho, Y.; Jeong, J.; Shin, Y.S.; Lim, J.Y.; Guralnik, J.M.; Park, J. Validation of a multi–sensor-based kiosk for short physical performance battery. J Am. Geriatr. Soc. 2019, 67, 2605–2609. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Smith, W.N.; Del Rossi, G.; Adams, J.B.; Abderlarahman, K.Z.; Asfour, S.A.; Roos, B.A.; Signorile, J.F. Simple equations to predict concentric lower-body muscle power in older adults using the 30-second chair-rise test: A pilot study. Clin. Interv. Aging 2010, 5, 173–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takai, Y.; Ohta, M.; Akagi, R.; Kanehisa, H.; Kawakami, Y.; Fukunaga, T. Sit-to-stand test to evaluate knee extensor muscle size and strength in the elderly: A novel approach. J. Physiol. Anthr. 2009, 28, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Nnamoko, N.; Korkontzelos, I. Efficient treatment of outliers and class imbalance for diabetes prediction. Artif. Intell. Med. 2020, 104, 101815. [Google Scholar] [CrossRef]
- Fushiki, T. Estimation of prediction error by using K-fold cross-validation. Stat. Comput. 2011, 21, 137–146. [Google Scholar] [CrossRef]
- Shany, T.; Wang, K.; Liu, Y.; Lovell, N.H.; Redmond, S.J. Review: Are we stumbling in our quest to find the best predictor? Over-optimism in sensor-based models for predicting falls in older adults. Healthc. Technol. Lett. 2015, 2, 79–88. [Google Scholar] [CrossRef] [Green Version]
- Cho, J. Current status and prospects of health-related sensing technology in wearable devices. J. Healthc. Eng. 2019, 2019, 8. [Google Scholar] [CrossRef]
- Matsuyama, H.; Hiroi, K.; Kaji, K.; Yonezawa, T.; Kawaguchi, N. Hybrid activity recognition for ballroom dance exercise using video and wearable sensor. In Proceedings of the 2019 Joint 8th International Conference on Informatics, Electronics & Vision (ICIEV) and 2019 3rd International Conference on Imaging, Vision & Pattern Recognition (icIVPR), Spokane, WA, USA, 30 May–2 June 2019; pp. 112–117. [Google Scholar]


{kind=link}
| Authors | Technology | Version | Subjects 1 | Age (Years) | Condition | Quality |
|---|---|---|---|---|---|---|
| Coni et al. (2019) | Triaxial accelerometers | 5STS | 304 (53.6%) | 80.9 ± 6.4 | Fallers | 6 |
| Doheny et al. (2011) | Triaxial accelerometers | 5STS | 40 (60%) | 71.4 ± 7.3 | Fallers | 6 |
| Doheny et al. (2013) | Triaxial accelerometers | 5STS | 39 (59%) | Fallers: 74.9 ± 7.0 | Fallers | 7 |
| Non-fallers: 68.4 ± 6.2 | ||||||
| Ejupi et al. (2016) | Kinect sensor | 5STS | 94 (70.2%) | 79.7 ± 6.4 | Fallers | 9 |
| Greene et al. (2014) | IMU | 5STS | 124 (73.4%) | Non-frail: 73.7 ± 6.0 | Frailty, Fallers | 8 |
| Frail: 77.8 ± 6.4 | ||||||
| Fallers: 76.0 ± 6.2 | ||||||
| Non-fallers: 75.8 ± 6.8 | ||||||
| Houck et al. (2011) | Force plates in a chair | 3STS | 28 (71.4%) | Control: 69.4 ± 10.9 | Fallers | 9 |
| Hip fracture: 76.4 ± 7.1 | ||||||
| Jung et al. (2019) | Load cells in a chair and laser | 5STS | 40 (62.5%) | 74.3 ± 5.4 | Frailty | 9 |
| Millor et al. (2013) | IMU | 30STS | 47 (44.7%) | Frail: 85 ± 5 | Frailty | 6 |
| Prefrail: 78 ± 3 | ||||||
| Robust: 54 ± 6 | ||||||
| Millor et al. (2014) | IMU | 30STS | 431 (N/S) | Frail: 79 ± 6 | Frailty | 5 |
| Pre-frail: 73 ± 5 | ||||||
| Robust: 74 ± 5 | ||||||
| Millor et al. (2017) | IMU | 30STS | 431 (N/S) | Frail: 79 ± 6 | Frailty | 6 |
| Pre-frail: 73 ± 5 | ||||||
| Robust: 74 ± 5 | ||||||
| Vincenzo et al. (2018) | Linear position transducer | 5STS | 98 (62.2%) | 77.5 ± 7.3 | Fallers | 9 |
| Zhang et al. (2017) | Triaxial accelerometer, pressure sensor | 5STS | 25 (80.0%) | 79.7 ± 5.7 | Frailty | 7 |
| Authors | Definition Used for Falling and Frailty |
|---|---|
| Coni et al. (2019) | Faller: ≥2 falls in previous 12 months |
| Doheny et al. (2011) | Faller: ≥2 falls in previous 5 years, or previous fall requiring medical attention, or fear of falling, or cardiovascular risk factor for falls |
| Doheny et al. (2013) | Faller: ≥2 falls in previous 12 months or fall requiring medical attention |
| Ejupi et al. (2016) | Faller: fall in previous 12 months |
| Greene et al. (2014) | Faller: ≥2 falls in previous 12 months or fall requiring medical attention Frailty: Fried phenotype used to classify participant as robust, pre-frail, or frail |
| Houck et al. (2011) | Faller: hip fracture from fall within previous 12 months, no longer receiving physical therapy |
| Jung et al. (2019) | Frailty: score on the Korean version of the FRAIL scale |
| Millor et al. (2013) | Frailty: Fried phenotype used to classify participant as robust, pre-frail, or frail |
| Millor et al. (2014) | Frailty: Fried phenotype used to classify participant as robust, pre-frail, or frail |
| Millor et al. (2017) | Frailty: Fried phenotype used to classify participant as robust, pre-frail, or frail |
| Vincenzo et al. (2018) | Faller: fall in previous 12 months |
| Zhang et al. (2017) | Frailty: Groningen Frailty Indicator |
| Population: Anyone Classified as A Faller | |||||
|---|---|---|---|---|---|
| Settings: Clinical or Laboratory | |||||
| Evaluation: Instrumented Sit-to-Stand Test | |||||
| Comparison: Non-Fallers | |||||
| Outcomes | Illustrative Example | Effect Size (95% CI) | Number of Participants (Studies) | Evidence Quality (GRADE) | |
| Fallers | Non-Fallers | ||||
| iSTS total time | 16.8 s | 14.3 s [37] | 0.42 1 (0.10, 0.74) | 172 (3 studies) | Low |
| iSTS stand-to-sit time | 0.45 s | 0.45 s [32] | 0.03 1 (−0.33, 0.39) | 172 (3 studies) | Low |
| iSTS sit-to-stand time | 0.49 s | 0.41 s [32] | 0.38 1 (0.10, 0.66) | 172 (3 studies) | Low |
| iSTS force/power | 6.2 W/Kg | 7.3 W/kg [36] | 0.56 1 (0.36, 0.76) | 126 (2 studies) | Low |
| iSTS frequency | 13.1 Hz | 11.3 Hz [32] | 0.45 1 (0.16, 0.73) | 39 (1 study) | Low |
| iSTS velocity | 0.41 m/s | 0.50 m/s [36] | 0.56 1 (0.35, 0.77) | 192 (2 studies) | Low |
| Physical function vs. iSTS force/power | r = 0.499 [38] peak GRF 3 vs. gait speed | 0.46 2 (0.35, 0.51) | 27 (1 study) | Low | |
| Physical function vs. iSTS velocity | r = 0.533 [37] STS velocity vs. knee extension | 0.43 2 (0.33, 0.53) | 94 (1 study) | Low | |
| Physical function vs. iSTS time | r = 0.316 [37] STS time vs. knee extension | 0.31 2 (0.21, 0.42) | 94 (1 study) | Low | |
| Classification using iSTS parameters | 72.6% accuracy in classifying fallers [31] | Not estimable | 261 (3 studies) | Low | |
| Population: Anyone Classified as Frail | ||||||
|---|---|---|---|---|---|---|
| Settings: Clinical or Laboratory | ||||||
| Evaluation: Instrumented Sit-to-Stand Test | ||||||
| Comparison: Frail vs. Pre-Frail and Pre-Frail vs. Robust | ||||||
| Outcomes | Illustrative Example | Effect Size (95% CI) | Number of Participants (Studies) | Evidence Quality (GRADE) | ||
| Frail | Pre-Frail | Robust | ||||
| STS cycles | 6.24 | 8.16 | 9.86 [28] | 0.79 2 (0.40, 1.17) | 431 (2 studies) | Low |
| 0.63 3 (0.43, 0.83) | ||||||
| iSTS phase time 1 | 1.67 s | 1.30 s | 1.10 s [30] | 0.81 2 (0.61, 1.00) | 237 (2 studies) | Low |
| 0.53 3 (0.43, 0.63) | ||||||
| iSTS force/power | 38.1 W | 65.4 W | 88.7 W [28] | 0.73 2 (0.51, 0.95) | 237 (2 studies) | Low |
| 0.72 3 (0.56, 0.88) | ||||||
| iSTS acceleration | 1.01 m/s2 | 1.28 m/s2 | 1.36 m/s2 [28] | 0.72 2 (0.56, 0.88) | 237 (2 studies) | Low |
| 0.44 3 (0.28, 0.59) | ||||||
| iSTS velocity | 0.48 m/s | 0.61 m/s | 0.68 m/s [30] | 0.83 2 (0.64, 1.02) | 237 (2 studies) | Low |
| 0.46 3 (0.27, 0.65) | ||||||
| Classification of groups using iSTS parameters | AUC = 0.934 for classification of frail participants using decision tree model [28] | 0.83 4 (0.82, 0.85) | 361 (2 studies) | Low | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shukla, B.; Bassement, J.; Vijay, V.; Yadav, S.; Hewson, D. Instrumented Analysis of the Sit-to-Stand Movement for Geriatric Screening: A Systematic Review. Bioengineering 2020, 7, 139. https://doi.org/10.3390/bioengineering7040139
Shukla B, Bassement J, Vijay V, Yadav S, Hewson D. Instrumented Analysis of the Sit-to-Stand Movement for Geriatric Screening: A Systematic Review. Bioengineering. 2020; 7(4):139. https://doi.org/10.3390/bioengineering7040139
Chicago/Turabian StyleShukla, Brajesh, Jennifer Bassement, Vivek Vijay, Sandeep Yadav, and David Hewson. 2020. "Instrumented Analysis of the Sit-to-Stand Movement for Geriatric Screening: A Systematic Review" Bioengineering 7, no. 4: 139. https://doi.org/10.3390/bioengineering7040139