Medial Collateral Ligament Deficiency of the Elbow Joint: A Computational Approach

Abstract
:
1. Introduction
2. Materials and Methods
3. Results
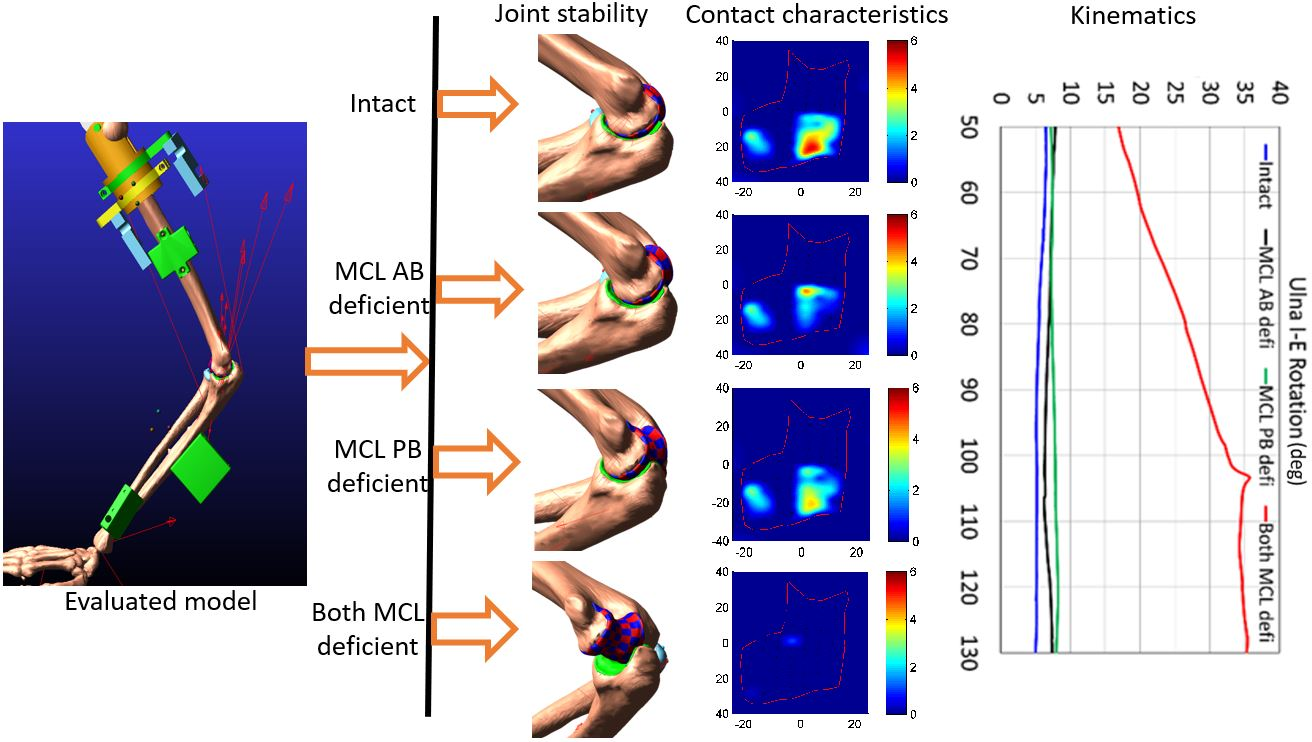
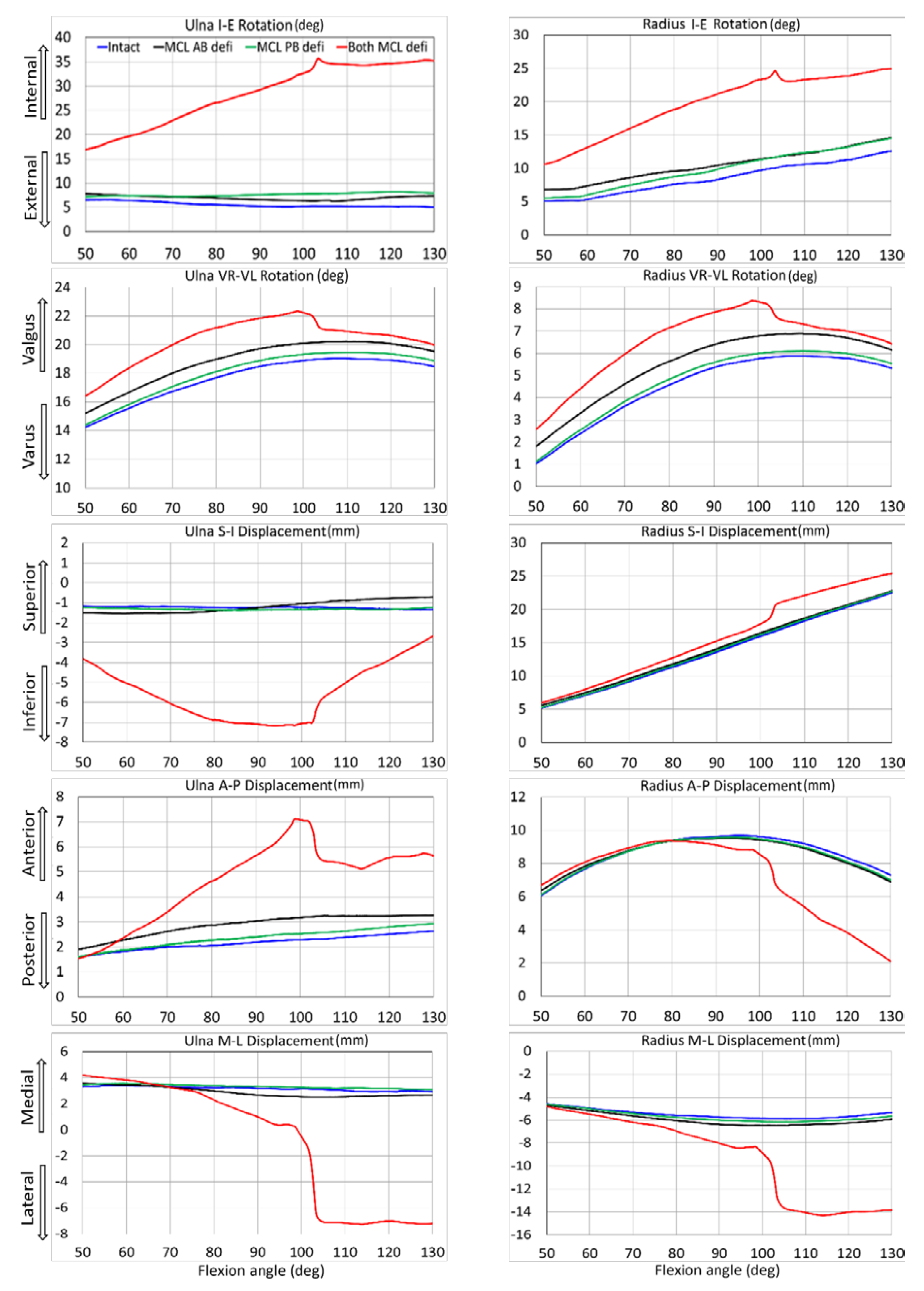
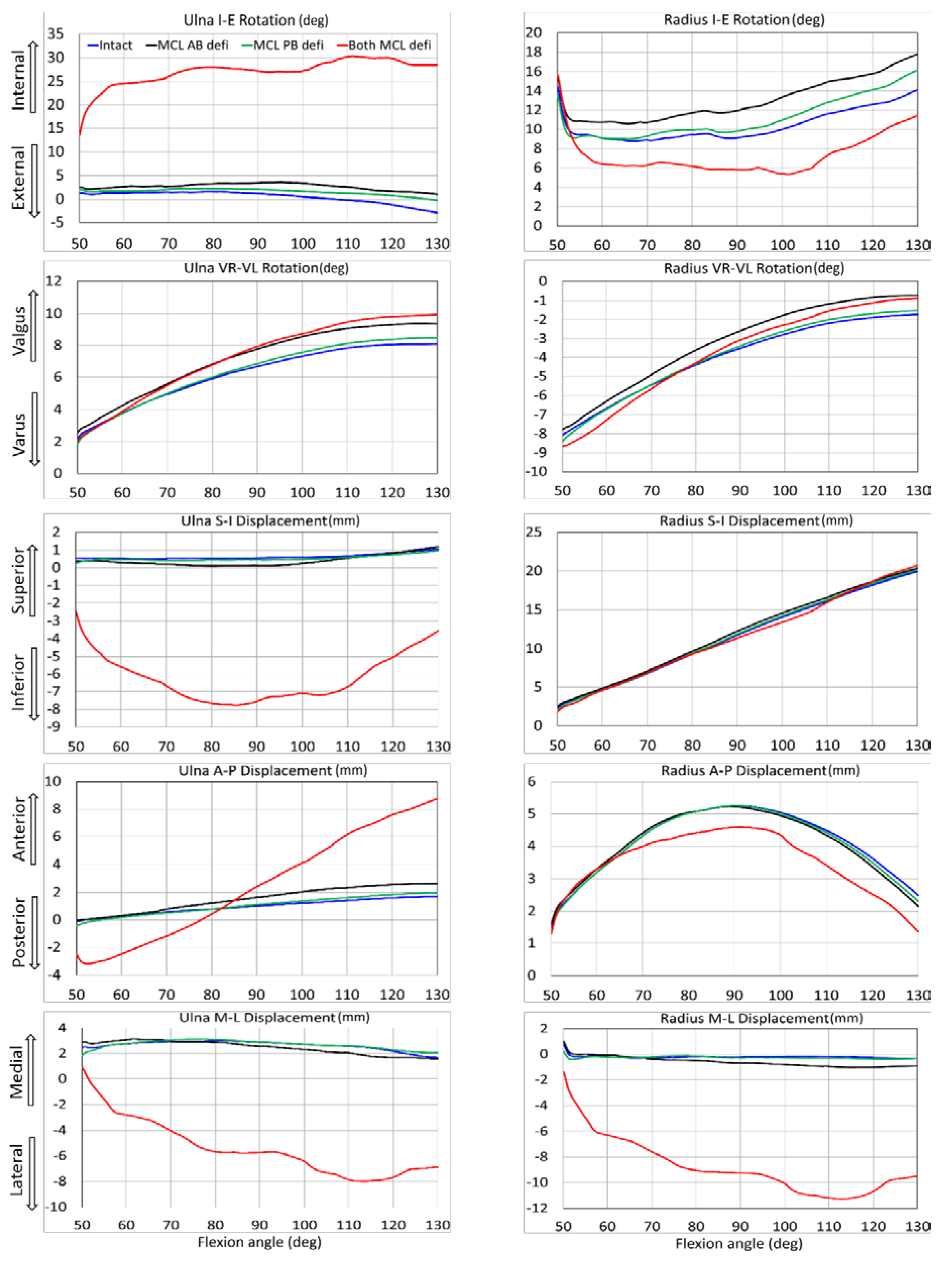
3.1. Kinematic Comparison
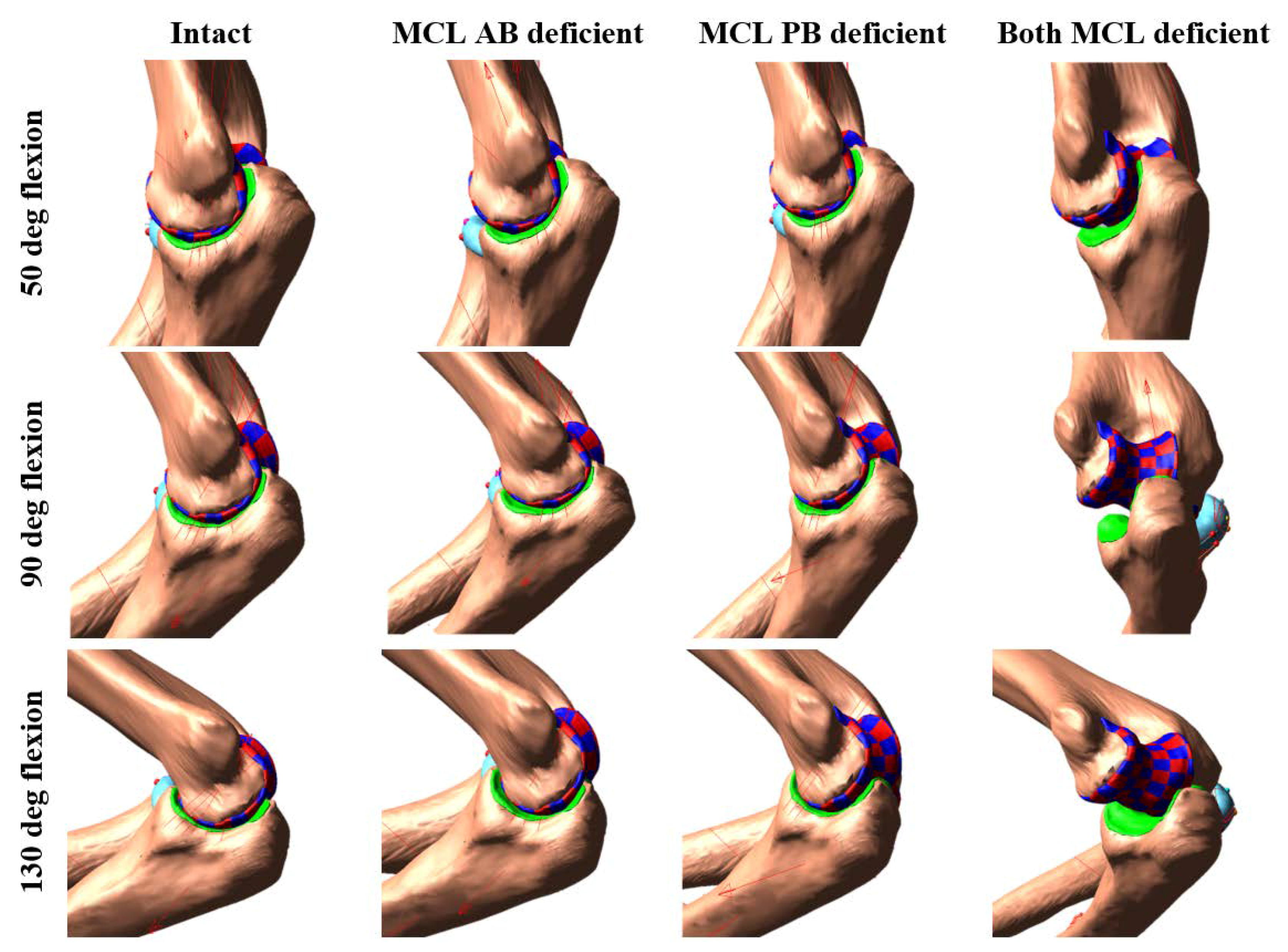
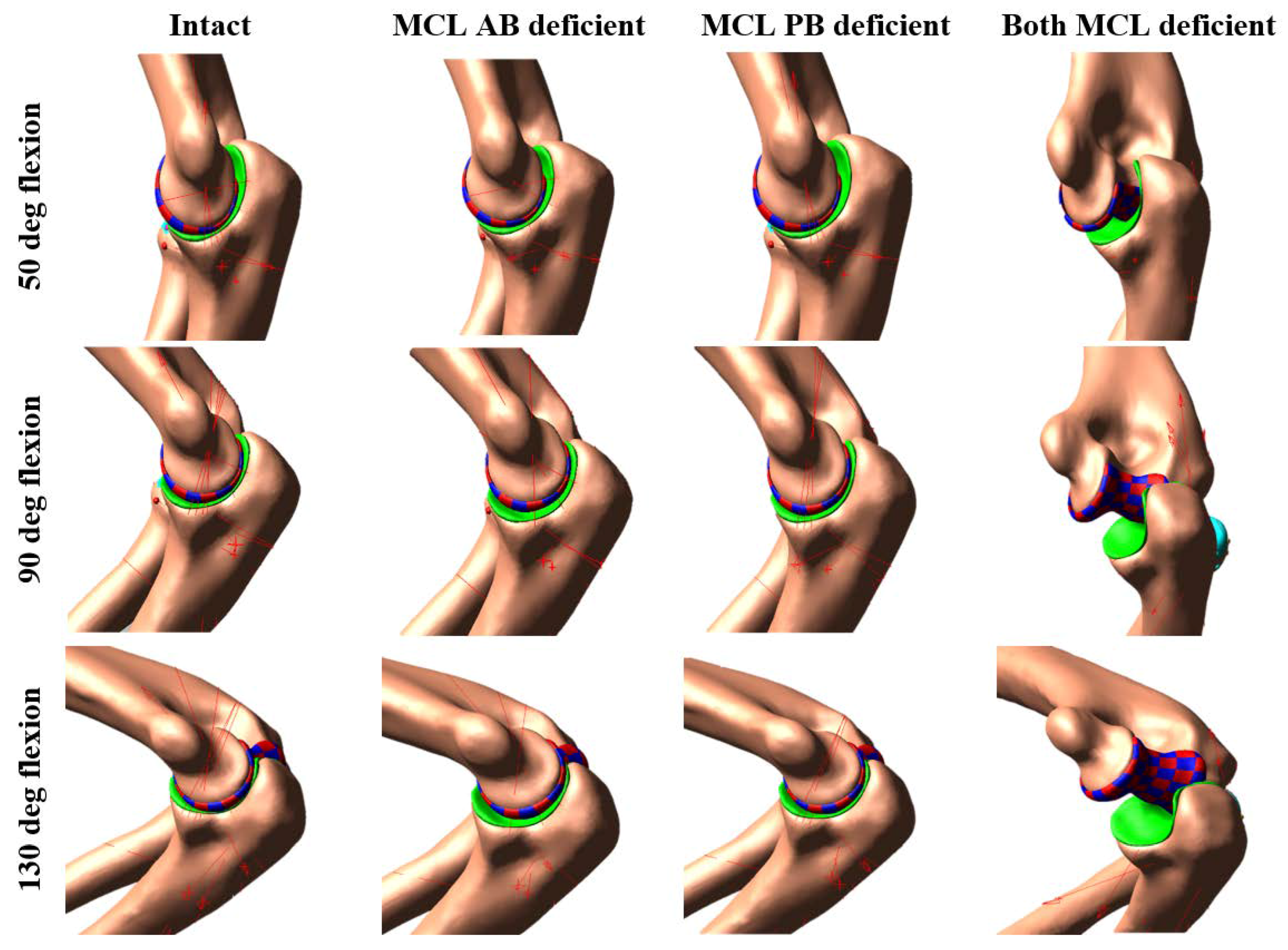
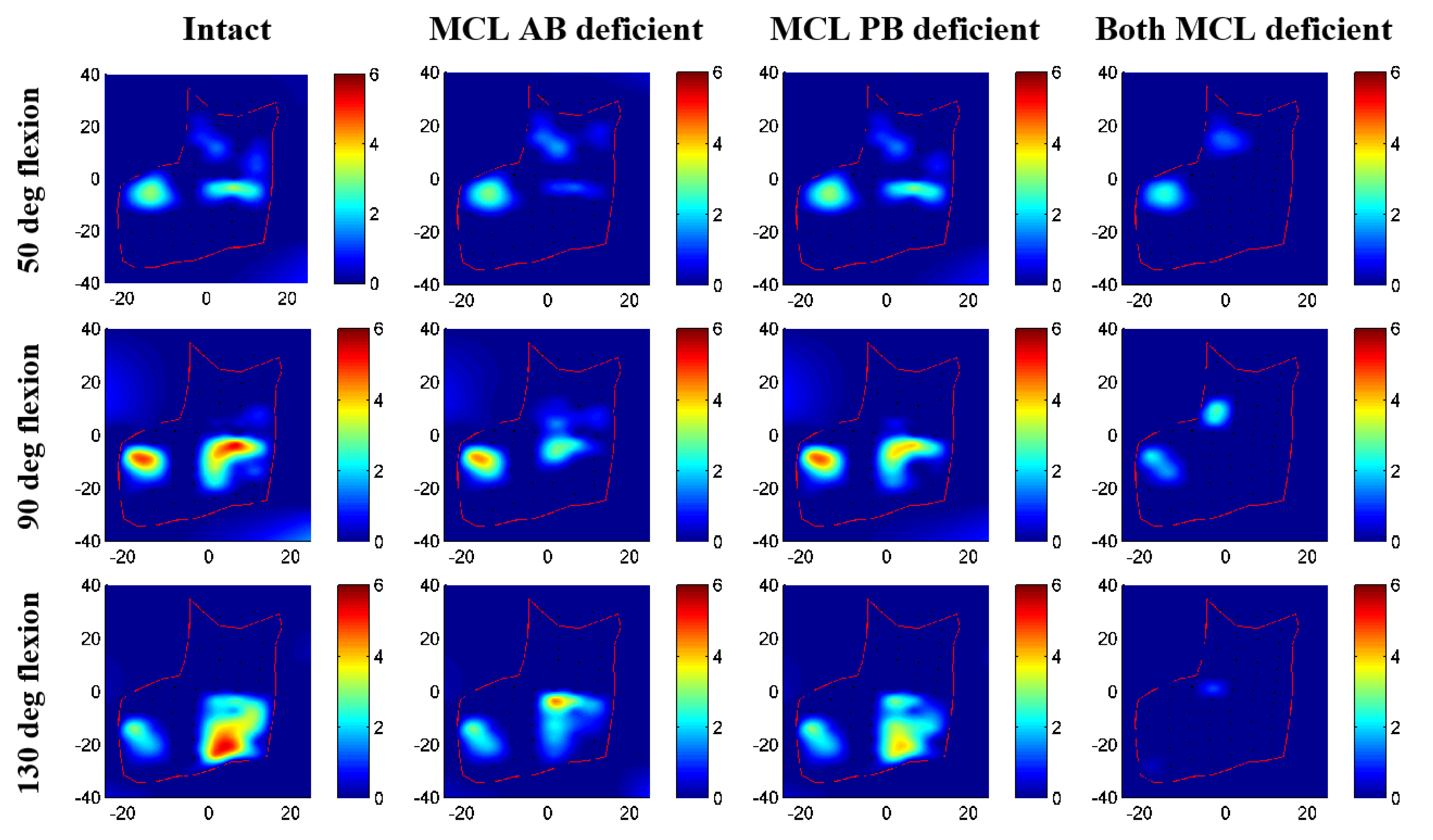
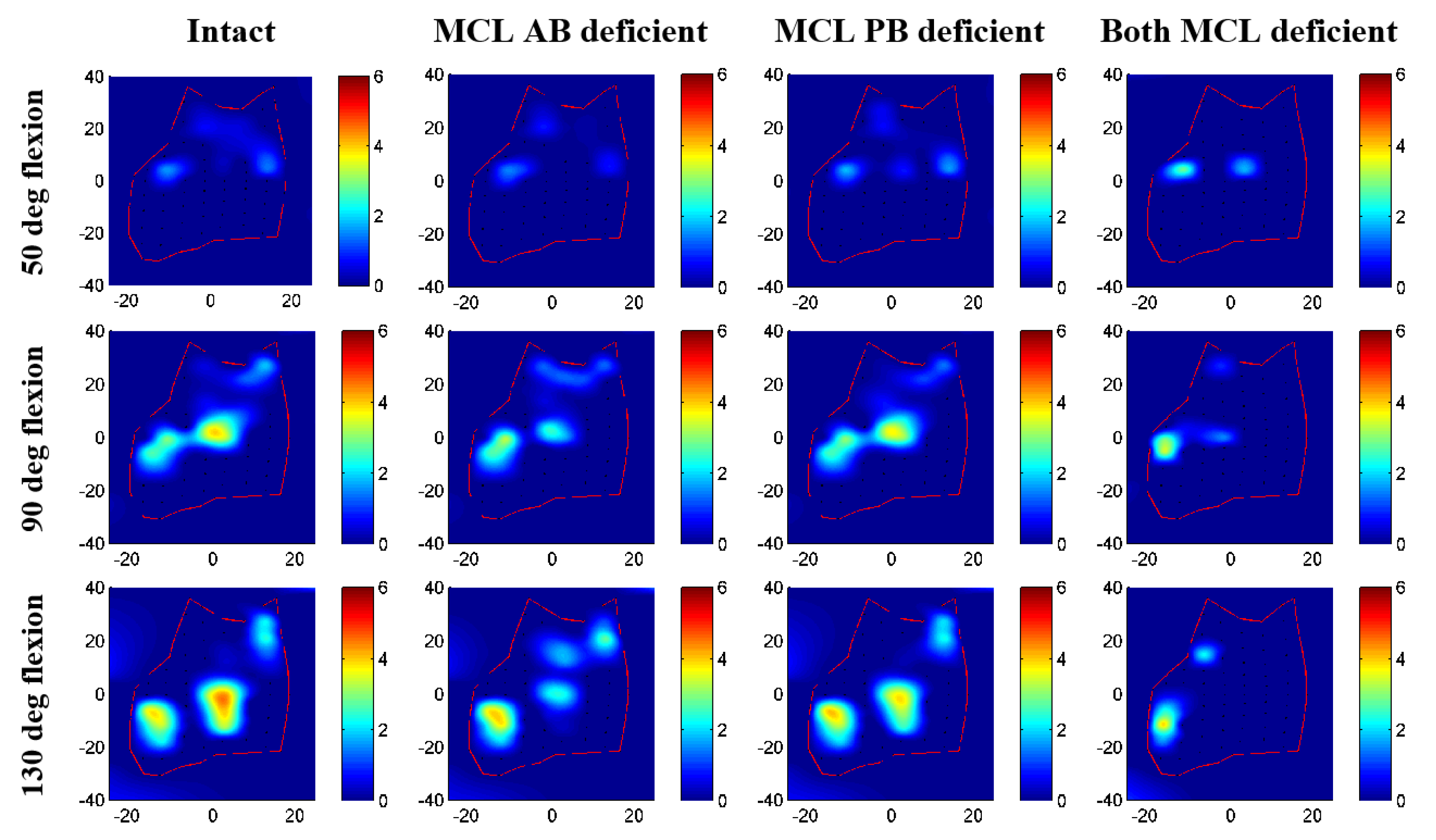
3.2. Contact Area and Pressure Comparison
3.3. Ligament Load Comparison
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Alolabi, B.; Gray, A.; Ferreira, L.M.; Johnson, J.A.; Athwal, G.S.; King, G.J. Rehabilitation of the medial- and lateral collateral ligament-deficient elbow: An in vitro biomechanical study. J. Hand Ther. 2012, 25, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Hildebrand, K.A.; Patterson, S.D.; King, G.J. Acute elbow dislocations: Simple and complex. Orthop. Clin. N. Am. 1999, 30, 63–79. [Google Scholar] [CrossRef]
- Josefsson, P.O.; Gentz, C.F.; Johnell, O.; Wendeberg, B. Surgical versus non-surgical treatment of ligamentous injuries following dislocation of the elbow joint. A prospective randomized study. J. Bone Joint Surg. Am. 1987, 69, 605–608. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.D.; Dunning, C.E.; Faber, K.J.; Duck, T.R.; Johnson, J.A.; King, G.J. Rehabilitation of the medial collateral ligament-deficient elbow: An in vitro biomechanical study. J. Hand Surg. Am. 2000, 25, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Safran, M.; Ahmad, C.S.; Elattrache, N.S. Ulnar collateral ligament of the elbow. Arthroscopy 2005, 21, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Bei, Y.; Fregly, B.J. Multibody dynamic simulation of knee contact mechanics. Med. Eng. Phys. 2004, 26, 777–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisk, J.P.; Wayne, J.S. Development and validation of a computational musculoskeletal model of the elbow and forearm. Ann. Biomed. Eng. 2009, 37, 803–812. [Google Scholar] [CrossRef] [PubMed]
- Garner, B.A.; Pandy, M.G. Musculoskeletal model of the upper limb based on the visible human male dataset. Comput. Methods Biomechan. Biomed. Eng. 2001, 4, 93–126. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, R.V.; Hutchins, E.L.; Barr, R.E.; Abraham, L.D. Development and evaluation of a musculoskeletal model of the elbow joint complex. J. Biomech. Eng. 1996, 118, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Guess, T.M.; Thiagarajan, G.; Kia, M.; Mishra, M. A subject specific multibody model of the knee with menisci. Med. Eng. Phys. 2010, 32, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Holzbaur, K.R.; Murray, W.M.; Delp, S.L. A model of the upper extremity for simulating musculoskeletal surgery and analyzing neuromuscular control. Ann. Biomed. Eng. 2005, 33, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Liacouras, P.C.; Wayne, J.S. Computational modeling to predict mechanical function of joints: Application to the lower leg with simulation of two cadaver studies. J. Biomech. Eng. 2007, 129, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Cil, A.; Bogener, J.W.; Stylianou, A.P. Lateral collateral ligament deficiency of the elbow joint: A modeling approach. J. Orthop. Res. 2016, 34, 1645–1655. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Cil, A.; Stylianou, A.P. Prediction of elbow joint contact mechanics in the multibody framework. Med. Eng. Phys. 2016, 38, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Stylianou, A.P.; Guess, T.M.; Cook, J.L. Development and validation of a multi-body model of the canine stifle joint. Comput. Methods Biomechan. Biomed. Eng. 2014, 17, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Willing, R.T.; Lalone, E.A.; Shannon, H.; Johnson, J.A.; King, G.J. Validation of a finite element model of the human elbow for determining cartilage contact mechanics. J. Biomech. 2013, 46, 1767–1771. [Google Scholar] [CrossRef] [PubMed]
- Willing, R.T.; Lapner, M.; Lalone, E.A.; King, G.J.; Johnson, J.A. Development of a computational technique to measure cartilage contact area. J. Biomech. 2014, 47, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Sharifi Renani, M.; Cil, A.; Stylianou, A.P. Musculoskeletal model development of the elbow joint with an experimental evaluation. Bioengineering 2018, 5, 31. [Google Scholar] [CrossRef] [PubMed]
- Morrey, B.F. The Elbow and Its Disorders; W.B. Saunders: Philadelphia, PA, USA, 2000. [Google Scholar]
- Machado, M.; Moreira, P.; Flores, P.; Lankarani, H.M. Compliant contact force models in multibody dynamics: Evolution of the hertz contact theory. Mechan. Mach. Theory 2012, 53, 99–121. [Google Scholar] [CrossRef] [Green Version]
- Hunt, K.H.; Crossley, F.R.E. Coefficient of restitution interpreted as damping in vibroimpact. J. Appl. Mechan. 1975, 42, 440–445. [Google Scholar] [CrossRef]
- Blankevoort, L.; Kuiper, J.H.; Huiskes, R.; Grootenboer, H.J. Articular contact in a three-dimensional model of the knee. J. Biomech. 1991, 24, 1019–1031. [Google Scholar] [CrossRef] [Green Version]
- Athanasiou, K.A.; Rosenwasser, M.P.; Buckwalter, J.A.; Malinin, T.I.; Mow, V.C. Interspecies comparisons of in situ intrinsic mechanical properties of distal femoral cartilage. J. Orthop. Res. 1991, 9, 330–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Gil, J.; Kanamori, A.; Woo, S.L. A validated three-dimensional computational model of a human knee joint. J. Biomech. Eng. 1999, 121, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Regan, W.D.; Korinek, S.L.; Morrey, B.F.; An, K.N. Biomechanical study of ligaments around the elbow joint. Clin. Orthop. Relat. Res. 1991, 271, 170–179. [Google Scholar] [CrossRef]
- Rahman, M.; Cil, A.; Johnson, M.; Lu, Y.; Guess, T.M. Development and validation of a computational multibody model of the elbow joint. Adv. Biomech. Appl. 2014, 1, 169–185. [Google Scholar] [CrossRef] [Green Version]
- Morrey, B.F.; Tanaka, S.; An, K.N. Valgus stability of the elbow. A definition of primary and secondary constraints. Clin. Orthop. Relat. Res. 1991, 265, 187–195. [Google Scholar]
- Ferreira, L.M.; King, G.J.; Johnson, J.A. Motion-derived coordinate systems reduce inter-subject variability of elbow flexion kinematics. J. Orthop. Res. 2011, 29, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Morrey, B.F.; Chao, E.Y. Passive motion of the elbow joint. J. Bone Joint Surg. Am. 1976, 58, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Pichora, J.E.; Fraser, G.S.; Ferreira, L.F.; Brownhill, J.R.; Johnson, J.A.; King, G.J. The effect of medial collateral ligament repair tension on elbow joint kinematics and stability. J. Hand Surg. Am. 2007, 32, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- An, K.N.; Hui, F.C.; Morrey, B.F.; Linscheid, R.L.; Chao, E.Y. Muscles across the elbow joint: A biomechanical analysis. J. Biomech. 1981, 14, 659–669. [Google Scholar] [CrossRef]
- King, G.J.; Morrey, B.F.; An, K.N. Stabilizers of the elbow. J. Shoulder Elbow Surg. 1993, 2, 165–174. [Google Scholar] [CrossRef]
- Morrey, B.F.; An, K.N. Articular and ligamentous contributions to the stability of the elbow joint. Am. J. Sports Med. 1983, 11, 315–319. [Google Scholar] [CrossRef] [PubMed]
- De Haan, J.; Schep, N.W.; Eygendaal, D.; Kleinrensink, G.J.; Tuinebreijer, W.E.; den Hartog, D. Stability of the elbow joint: Relevant anatomy and clinical implications of in vitro biomechanical studies. Open Orthop. J. 2011, 5, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Renani, M.S.; Rahman, M.; Cil, A.; Stylianou, A.P. Ulna-humerus contact mechanics: Finite element analysis and experimental measurements using a tactile pressure sensor. Med. Eng. Phys. 2017, 50, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Renani, M.S.; Rahman, M.; Cil, A.; Stylianou, A.P. Calibrating multibody ulno-humeral joint cartilage using a validated finite element model. Multibody Syst. Dyn. 2018, 44, 81–91. [Google Scholar] [CrossRef]
- Brand, R.A. Joint contact stress: A reasonable surrogate for biological processes? Iowa Orthop. J. 2005, 25, 82–94. [Google Scholar] [PubMed]
- Eckstein, F.; Merz, B.; Muller-Gerbl, M.; Holzknecht, N.; Pleier, M.; Putz, R. Morphomechanics of the humero-ulnar joint: Ii. Concave incongruity determines the distribution of load and subchondral mineralization. Anat. Rec. 1995, 243, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Andrews, J.R.; Jelsma, R.D.; Joyce, M.E.; Timmerman, L.A. Open surgical procedures for injuriesto the elbow in throwers. Oper. Tech. Sports Med. 1996, 4, 109–113. [Google Scholar] [CrossRef]
- Fleisig, G.S.; Leddon, C.E.; Laughlin, W.A.; Ciccotti, M.G.; Mandelbaum, B.R.; Aune, K.T.; Escamilla, R.F.; MacLeod, T.D.; Andrews, J.R. Biomechanical performance of baseball pitchers with a history of ulnar collateral ligament reconstruction. Am. J. Sports Med. 2015, 43, 1045–1050. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ligament Conditions | I-E (deg) | VR-VL (deg) | S-I (mm) | A-P (mm) | M-L (mm) | |
|---|---|---|---|---|---|---|
| Ulna Kinematics | MCL AB Deficient | 1.44 ± 0.36 | 1.18 ± 0.08 | 0.10 ± 0.35 | 0.73 ± 0.17 | −0.28 ± 0.23 |
| (0.19) | (<0.01 *) | (0.93) | (<0.01 *) | (0.94) | ||
| MCL PB Deficient | 2.24 ± 0.73 | 0.40 ± 0.08 | −0.08 ± 0.06 | 0.20 ± 0.09 | 0.15 ± 0.04 | |
| (0.02) | (<0.01 *) | (0.96) | (0.49) | (0.99) | ||
| Both MCL Deficient | 23.72 ± 6.50 | 2.61 ± 0.76 | −4.19 ± 1.46 | 2.61 ± 1.26 | −4.71 ± 4.62 | |
| (<0.01 *) | (<0.01 *) | (<0.01 *) | (<0.01 *) | (< 0.01 *) | ||
| Radius Kinematics | MCL AB Deficient | 1.91 ± 0.16 | 0.97 ± 0.07 | 0.43 ± 0.07 | −0.13 ± 0.19 | −0.47 ± 0.15 |
| (<0.01 *) | (<0.01 *) | (<0.01 *) | (0.95) | (0.61) | ||
| MCL PB Deficient | 1.41 ± 0.47 | 0.22 ± 0.03 | 0.20 ± 0.05 | −0.11 ± 0.11 | −0.21 ± 0.90 | |
| (<0.01 *) | (<0.01 *) | (0.41) | (0.97) | (0.94) | ||
| Both MCL Deficient | 11.42 ± 2.25 | 1.93 ± 0.57 | 2.24 ± 1.14 | −1.78 ± 2.13 | −4.21 ± 3.44 | |
| (<0.01 *) | (<0.01 *) | (<0.01 *) | (<0.01 *) | (<0.01 *) |
| Ligament Conditions | I-E (deg) | VR-VL (deg) | S-I (mm) | A-P (mm) | M-L (mm) | |
|---|---|---|---|---|---|---|
| Ulna Kinematics | MCL AB Deficient | 2.29 ± 0.79 | 0.99 ± 0.32 | −0.23 ± 0.17 | 0.61 ± 0.35 | −0.21 ± 0.31 |
| (<0.01 *) | (<0.01 *) | (0.38) | (0.35) | (0.78) | ||
| MCL PB Deficient | 1.17 ± 0.64 | 0.17 ± 0.16 | −0.10 ± 0.03 | 0.09 ± 0.14 | 0.05 ± 0.14 | |
| (0.03) | (0.13) | (0.89) | (0.99) | (0.99) | ||
| Both MCL Deficient | 26.89 ± 3.78 | 4.14 ± 0.62 | −6.87 ± 1.27 | 1.97 ± 3.33 | −8.31 ± 2.01 | |
| (<0.01 *) | (<0.01 *) | (<0.01 *) | (<0.01 *) | (<0.01 *) | ||
| Radius Kinematics | MCL AB Deficient | 2.73 ± 0.77 | 0.82 ± 0.26 | 0.41 ± 0.10 | −0.07 ± 0.14 | −0.43 ± 0.34 |
| (<0.01 *) | (<0.01 *) | (<0.01 *) | (0.47) | (0.24) | ||
| MCL PB Deficient | 0.84 ± 0.66 | 0.10 ± 0.12 | 0.12 ± 0.10 | −0.05 ± 0.06 | −0.07 ± 0.11 | |
| (<0.01 *) | (0.06) | (0.41) | (0.73) | (0.99) | ||
| Both MCL Deficient | −3.22 ± 1.17 | 0.28 ± 0.49 | −0.05 ± 42 | −0.68 ± 0.41 | −8.83 ± 2.06 | |
| (<0.01 *) | (<0.01 *) | (0.70) | (<0.01 *) | (<0.01 *) |
| Ligament Band | Intact | MCL AB Deficient | MCL PB Deficient | Both MCL Deficient | ||||
|---|---|---|---|---|---|---|---|---|
| Peak Load (N) | Max. Strain | Peak Load (N) | Max. Strain | Peak Load (N) | Max. Strain | Peak Load (N) | Max. Strain | |
| Lateral ulnar collateral ligament | 62 | 0.13 | 59 | 0.13 | 54 | 0.12 | 44 | 0.10 |
| Radial collateral ligament | 24 | 0.11 | 20 | 0.10 | 19 | 0.10 | 23 | 0.11 |
| MCL anterior band | 211 | 0.50 | - | - | 224 | 0.53 | - | - |
| MCL posterior Band | 118 | 0.44 | 140 | 0.52 | - | - | - | - |
| Ligament Band | Intact | MCL AB Deficient | MCL PB Deficient | Both MCL Deficient | ||||
|---|---|---|---|---|---|---|---|---|
| Peak Load (N) | Max. Strain | Peak Load (N) | Max. Strain | Peak Load (N) | Max. Strain | Peak Load (N) | Max. Strain | |
| Lateral ulnar collateral ligament | 53 | 0.11 | 45 | 0.10 | 49 | 0.11 | 31 | 0.08 |
| Radial collateral ligament | 20 | 0.10 | 16 | 0.09 | 18 | 0.09 | 43 | 0.18 |
| MCL anterior band | 170 | 0.40 | - | - | 181 | 0.43 | - | - |
| MCL posterior band | 65 | 0.26 | 95 | 0.36 | - | - | - | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahman, M.; Cil, A.; Stylianou, A.P. Medial Collateral Ligament Deficiency of the Elbow Joint: A Computational Approach. Bioengineering 2018, 5, 84. https://doi.org/10.3390/bioengineering5040084
Rahman M, Cil A, Stylianou AP. Medial Collateral Ligament Deficiency of the Elbow Joint: A Computational Approach. Bioengineering. 2018; 5(4):84. https://doi.org/10.3390/bioengineering5040084
Chicago/Turabian StyleRahman, Munsur, Akin Cil, and Antonis P. Stylianou. 2018. "Medial Collateral Ligament Deficiency of the Elbow Joint: A Computational Approach" Bioengineering 5, no. 4: 84. https://doi.org/10.3390/bioengineering5040084